1
Phylum:
Nematoda
Strongyloides sterocoralis
nAim of the study: S.sterocoralis is important human parasite ,because of its
potential
fatal
hyperinfection
syndro me
in
immunocomp romised persons ,also recent study sho ws
that chronic alcoholism itself is an impo rtant facto r that
predispose factor to strongyloidiasis. In addition to certain
predisposing factors such as corticostero id therapy,
anticancer drugs, malnutrition among other factors.
nThe Obje ctive s:
1.
Define t he parasite S.sterocoralis .
2. Describe the Epidemiology: A. mode of transmission, B. risk for travelers.
3. Describe the morphology of S.sterocoralis.
4. Analyse the life cycle of S.sterocoralis.
5. List t he clinical feat ures of strongyloidiasis.
6. Determine the laboratory diagnosis.
7. Define t he hyperinfection syndrome.
8. Evalut e t he prevention and cont rol of st rongyloidiasis.
1.
Strongyloides stercoralis
:
Strongyloide s stercoralis is an intestinal
ne matode with
a comple x life cycle capable of a fre e living
cycle, a parasitic cycle and auto-infection. It is usually
asymptomatic in a he althy host but causes life thre ate ning
hyperinfe ction involving multiple organs in immunocompromise d
patients. S.ste rcoralis causing the disease of
strongyloidiasis
, is
the smalle st pathoge nic ne matode s , hardly visible to the nake d
eye measure 2.4-4.7mm. in length.
Habitat:
Adult female live e mbe dded in the mucosal epithelium of
upper small intestine (S.I.), especially the duode num and uppe r
je junum.
2.Epidemiology:
S. stercoralis has a very low pre vale nce in socie tie s whe re fecal
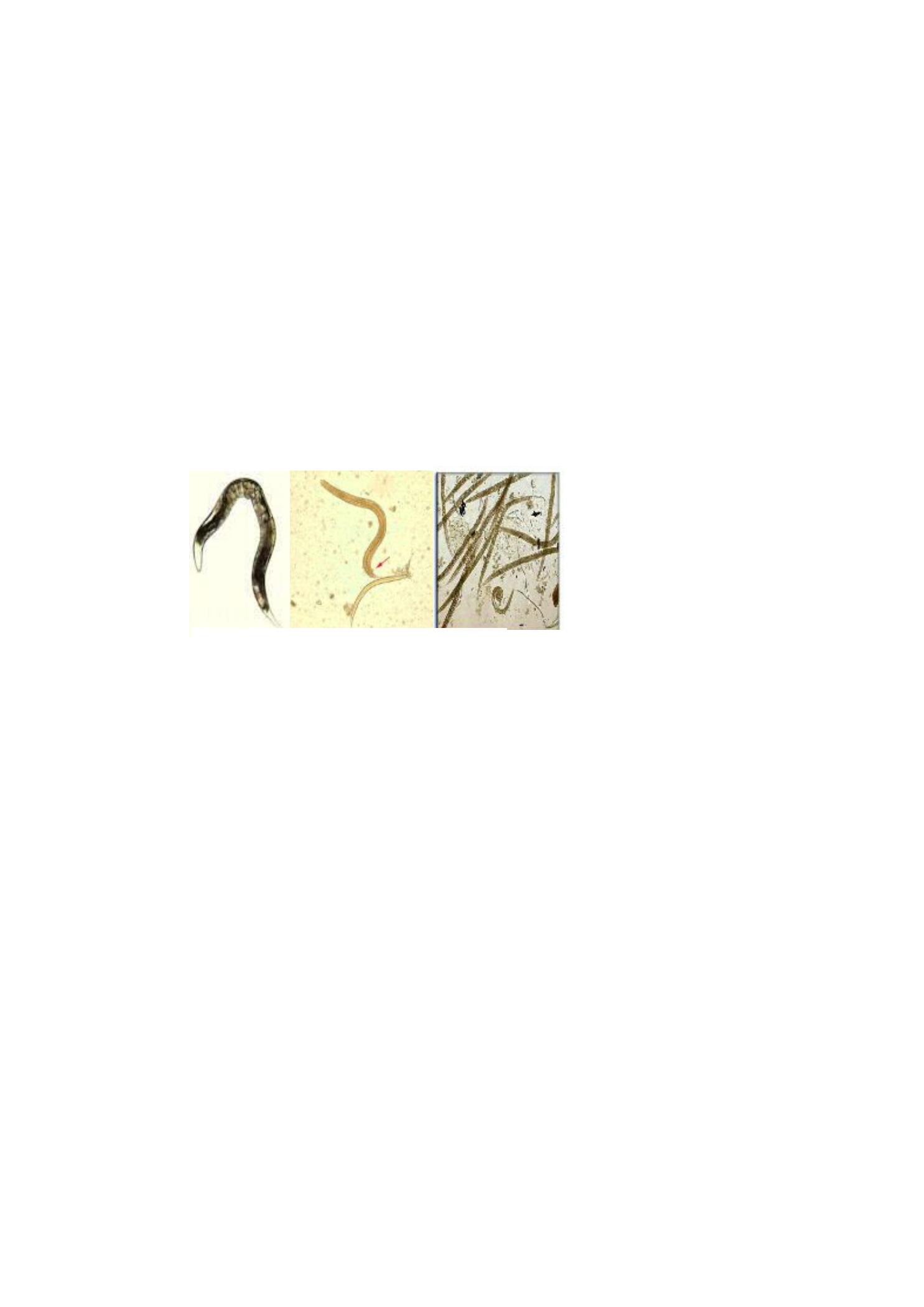
Adult female ,Rhabditiform,and filariform larv ae of

2
contamination of soil or water is rare . He nce, it is a very rare
infe ction
in de velope d economies. In the southe rn of Iraq during 1989 the
pre vale nce rate of infe ction was 64.2%. It was higher in rural
(74.2%) than in urban (57.5%) . In developing countries it is less
pre vale nt in urban areas than in rural areas (whe re sanitation
standards are poor). S. stercoralis can be found in areas with
tropical and subtropical climates.
2.A. Mode of Transmission
:
n Filariform larvae found in infected soil in the tropics and
subtropics penetrate human skin, whe n man walks
barefoot on fae cally contaminate d soil .
Pe rson-to-person transmission is rare , but has be en
documente d.
2.B. Risk for Travelers :
n Knowledge of the geographic distribution of strongyloidiasis is
of
significance to trave lers who may acquire the parasite
during the ir stays in e ndemic are as. Also,travele rs who visit
ende mic areas and have contact with contaminated soil
through bare skin are at risk for infection. Most infe ctions
see n in the United States occur in immigrants, refugee s, and
military ve te rans who have live d in e ndemic are as for long
pe riods of time . Risk for short-te rm trave lers appears to be
very low, but can occur.
3.Morphology:
The different stages of S.sterocoralis are :
1
.adult worms,
2
.eggs,
3.
larvae(rhabditiform laravae,and filariform
larvae).
1.Adult worms : Only female are seen in the intestine .Majority of
the female worm are parthenogenetic(i.e. they can produce offspring
without being fertilized by the male).Contrary the male worms do
3
exist,which are shorter and boarder than the female, while males
grow to only about 0.9 mm in length, the females can be anywhere
from 2.0to 2.5 mm. While intestine is present in the posterior 2/3 of
the body, the posterior end is pointed .The eggs are arranged
anteroposteriorly in a single row of 5-10 eggs in a uterus, the female
is ovo-viviparous. The males are not seen in human infections
because they do not invade the intestinal wall and are eliminated
from the intestine. Both genders also possess a tiny buccal capsule,
the mouth possess 3-small lips and cylindrical esophagus (without a
posterior bulb) is present in anterior part of the body. In the free-
living stage, the esophagus of both sexes are rhabditiform. Males
can be distinguished from their female counterparts by two
structures: the spicules and gubernaculum.
Adult parasitic female and male of
S.sterocoralis
Free living male &female of S .sterocoralis
4
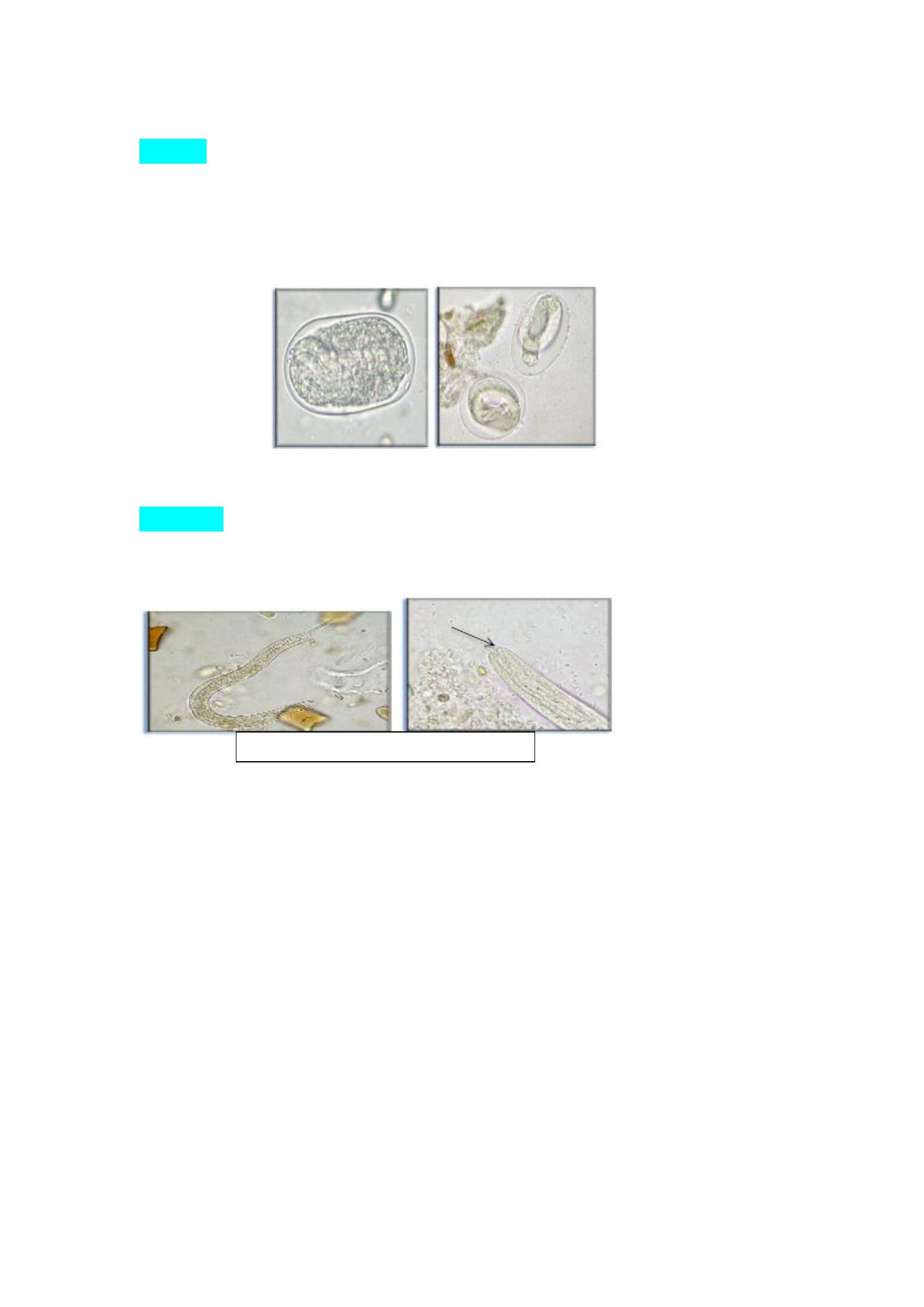
2. Eggs
: The ovum is oval, transparent, thin shelled, about 5-60μ
m*30-
35μm,partially embryonated when discharged in mucosal
epithelium. Eggs typically mature into rhabditiform larvae within
the intestine. Strongyloides is the only helminth to secrete
larvae (and not eggs) in feces.
3.Larvae :
Two types of larvae are found :rhabditiform and filariform
larvae. The embryonated eggs hatch almost immediately in the
mucosa of the intestine to the rhabditiform larvae.
A.Rhabditiform larvae: These are developed directly from gravid
females and are found in the lumen of the bowel, are 250-250µm
in length shorter than filariform larvae and sluggishly motile ,and
Embryonated ova of S.sterocoralis
Rhabditiform larva of S.sterocoralis
shor t mo uth
5
have short mouth and double bulb oesophagus, while that of
hookworm rhabditiform larvae contain long buccal cavity.
The further development could be as follows :
a. internal reinfection(in the bowel of the lumen they
metamorphose into
filariform larvae or by
b. external
reinfection or hyperinfection : through penetrate the perianal&
perineal skin without leaving the host, c. or by may be voided
with faeces and undergo development in the soil through direct
or indirect cycle .
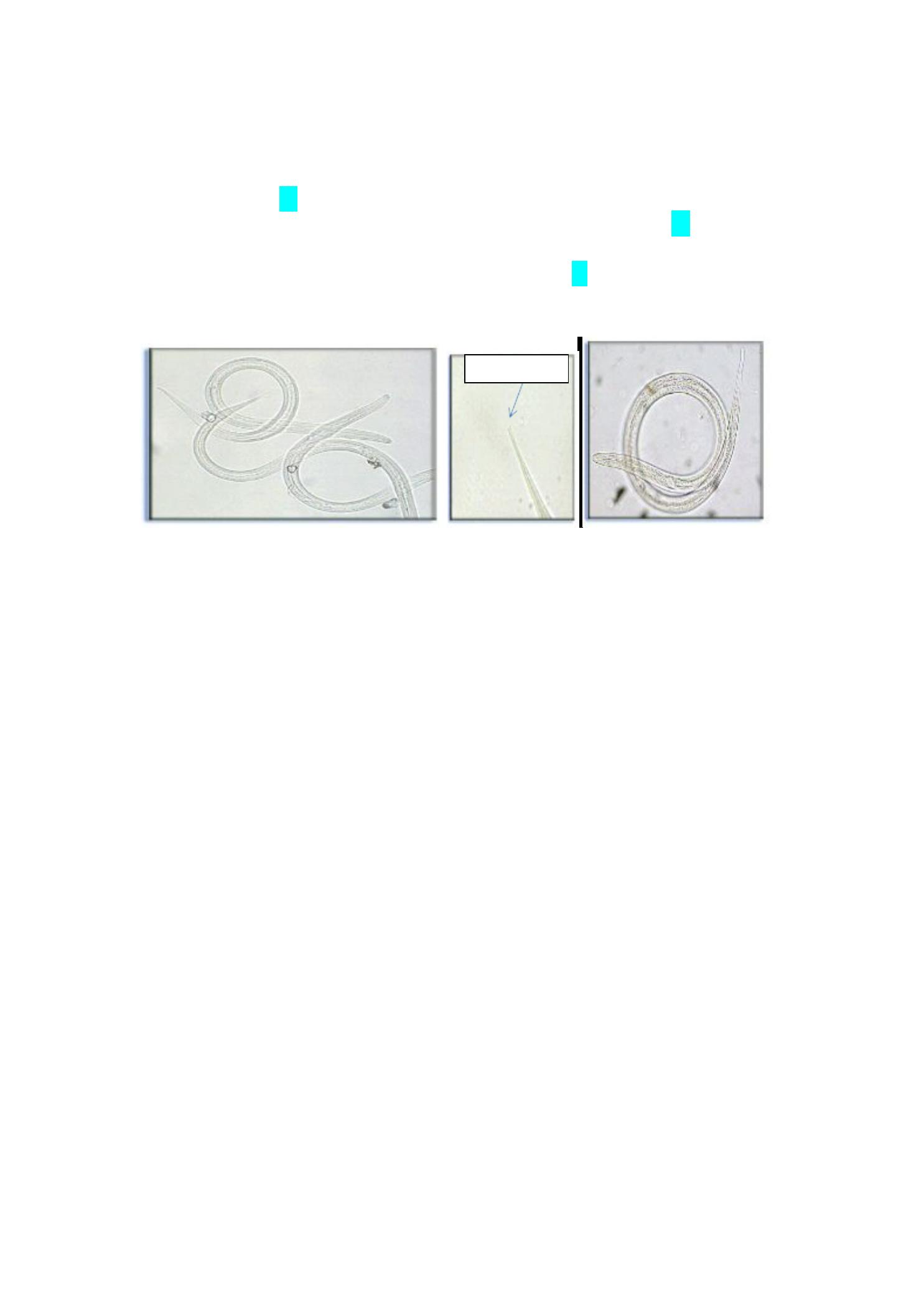
notched tail

6
B. Filariform larvae: These are skin penetrating infective forms of the
parasite ,which are longer and more slender than
the rhabditiform larvae, they have short mouths
and cylindrical esophagus,while that of hookworm
have short esophagus and the tail Fl.larve of
S.sterocoralis is notched and pointed in hookworm.
These
are
develop
in
three
ways:a.
metamorphosed in human bowel from the first
batch
of
rhabditiform
larvae,b.
direct
development from rhabditiform larvae voided
with feces (in temperate climates),and c.from a
sexual phase of rhabditiform laravae in the soil
giving rise to second rhabditiform larvae and then
developed to filariform larvae(in tropical climates).
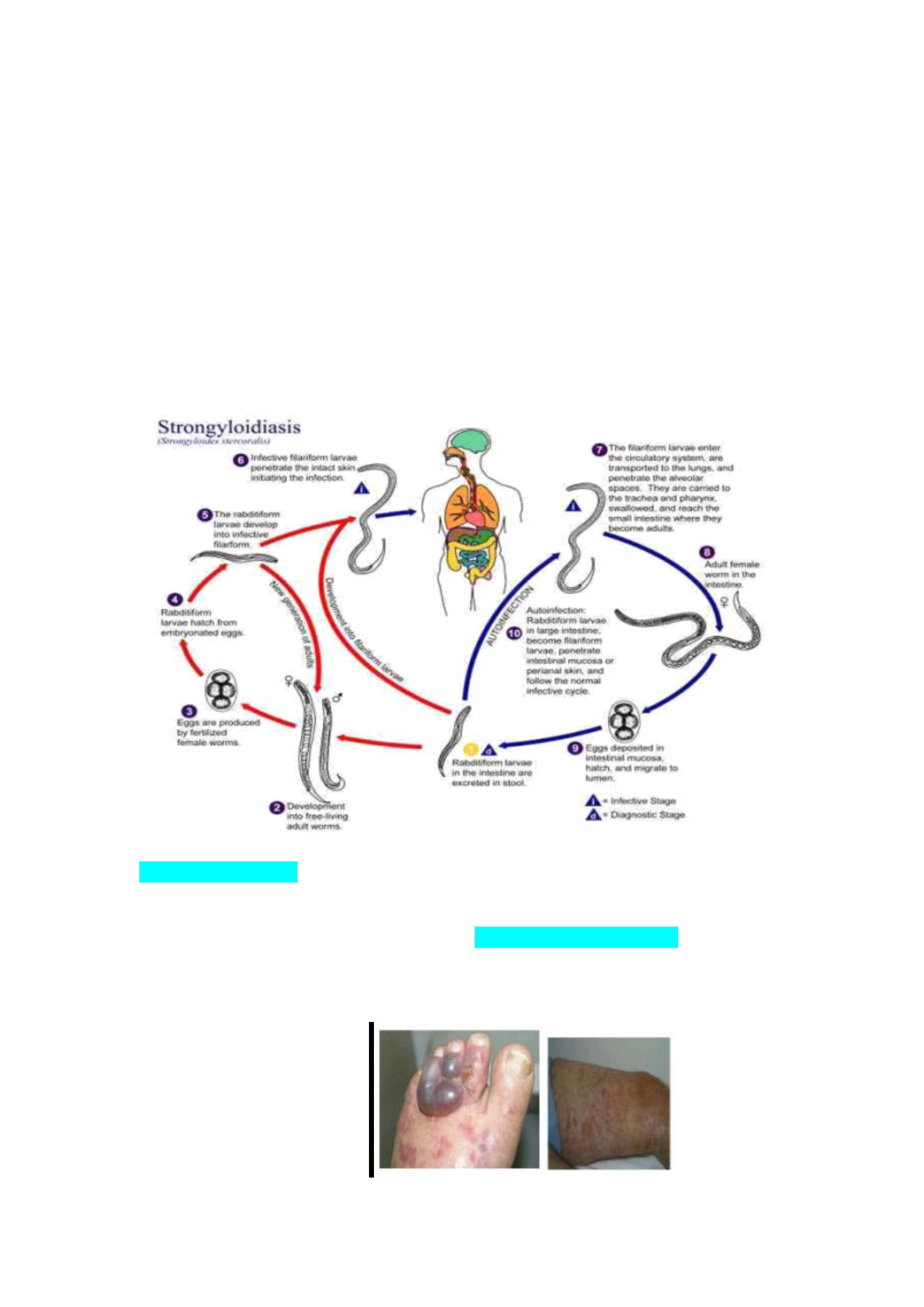
4.The Life Cycle of S.sterocoralis :
Man is the only host of S.sterocoralis , and no I.H. is required and the
change of the host is not essential.
nworms have a Heterogenetic life cycle which consists of :
1. (Heterogonic life cycle):A free -living ge ne rations have this life
cycle,the mating take place in the soil and fertilized female lays e ggs
,which hatch to re lease the next generation of rhabditiform larvae
that eithe r re pe at the life cycle or may de velop to into filariform
larvae which infe ct man and initiate the parasitic phase.
2. (Homogenic life cycle):
Aparasitic generation which is inte rnal and
e xte rnal autoinfe ction . Infection occurs when exp osed skin contacts
contaminated so il, following skin penetration they are carried by the bloo d to
the
lungs
, where they exit into the alveoli, travel up the
trachea
, are swallowed,
and mature in the
small intestine
. If ingested, migratio n thro ugh the lung s is not
necessary.
Filariform larvae rest in the smallintestine, mature into adult females. A parasitic
females anchor themselves with their mouths to the
mucosa
o f the
smallintestine
or burrow their anterior ends into the submucosa. Rep roduction in the host is b y
parthenog enetic females which lay several dozen eg gs each day. Eggs are released
into the lumen of the gut or the sub mucosa where they hatch and juveniles pass
7
into the lumen. These first stag es Rhabditiform larvae are 300-380μ
m long and are
usually passed with the feces, develop either to free-living adults or to infective
filarifo rm juveniles ,while passing down the small intestine. Third stage
juveniles(filariform larvae) are the infective stage. They are 4 90-630μ
m long . This is
a resting stag e which does no t develo p further until it penetrates throug h skin or is
ingested.Autoinfe ctio n occurs when the larvae reinfect the host by penetrating the
intestinalmuco sa o r the perianal or perineal skin. From initial infection to maturity
usually takes less than 4weeks.
5.Clinical Features: Disease associated with infections due to S. stercoralisis varied,
rang ing from some patients b eing to tally asympto matic to the
hyperinfectio n syndro me. There are 3 areas o f invo lvement in
Strongyloides infections; skin, lung s and inte stine .
1.Dermatitis
(with acute infections) is p roduced by migration of the infective
juveniles thro ugh the skin (cutaneous infection) ,mig rating larvae in the skin
can cause larva curre ns.
8
2.The mild to severe symp tom o f
pneumonia
can occur during migration to air
sacs of
lungs
. The migratio n o f larvae through the lungs may stimulate an
immune response which can result in a cough, whe e zing and fe ve r.
3. Symp toms asso ciated with intestinalstrongyloidiasis may mimic pe ptic ulce r
due to ulceration of the intestinalmuco sa. In heavy infections the intestinal
mucosa maybe severely damaged resulting in malabsorp tion. There may also
be lo wer gastro intestinal bleeding. Eosinophilia may b e high
4 .Diarrhea
accompanied b y emaciatio n and exhaustion.
Immunocompromised individuals, especially tho se receiving systemic
co rticosteroids or patients with HTLV-1 infection, are at risk fo r
hype rinfe ction or disse minate d dise ase, characterized b y abdominal pain,
diffuse pulmonary infiltrates, and sep ticemia or mening itis from enteric gram
negative b acilli. Untreated disseminated stro ngyloidiasis has high mortality.
5. Under certain conditions (e.g. constipation, decreased bo wel motility,
diverticular disease), the larvae do no t exit the host in feces and
instead molt into the infective filariform .
6.Lab orato ry o f d iagn osis o f S.steroc oralis :
Lab oratory diagno sis depends o n finding larvae in stoo l, sputum or duodenal
aspirates.
1. Stoo lexamination ,only larvae of the parasite can be detected(either
rhab ditiform
or filariform larvae )willconfirm the presence of this parasite.
Rep eated stool
examinations may be necessary, given the lo w sensitivity o f a
sing le stoo l examinatio n.
a. Direct wet smear examination ,by using either (direct saline o r iodine smear)is
examined for the p resence o f larvae.
b. Formal –
ether concentration: this method is more sensitive than the direct
smear examinatio n .
c. Concentration of larvae b y Bae rmann's me thod ,this method depends on
the
p rincip le o f the tendency of stro ngyloides larvae to migrate fro m a co lder to
warmer area. This is the mo st sensitive method available for diagno sis.
2.Stool culture :using charco al culture me thod , filariform larvae develop in 5-
7days
in po sitive cases.
3.Duodenal asp iration :using entero test gelatin cap sule (repeated examination is
recommended) .This is also a very sensitive method.
4.Histo patholog ical examination :biopsy or autopsy sp ecimen.
5.Immunodiagno sis : like ELISA ,RAST( used fo r screening from individuals from
endemic area who are likely to p ut on immunosuppressive therapy.
L arval Strogy loides st ercoralis from a faecal
sample. Image tak en
by blogger Yuri

9
7.Hyperinfection syndrome
The autoinfective capability of larvae may be responsible for long term infections
which persist for many years. The parasite and host reach an equilibrium state where
neither host nor parasite suffers any adverse reactions. If this equilibrium is disturbed
e.g. immunosuppression, the infection proliferates with immense numbers of larva
emigrating to every tissue in the body, especially the lungs. This condition is referred
to as disseminated strongyloidiasis. This results in tissue damage, pneumonitis, brain
damage or respiratory failure.
Prevention and Control:
1.
imp roving sanitation and water infrastructure in reso urce poo r areas
2. Because stro ngyloidiasis is transmittable by textiles, such as b edclothes and
clo thing, care must be taken ne ve r to use hotel bed sheets in endemic areas.
Perso nal sleeping bag s and using plastic slippers when showering are very
important when travelling in trop ical reg io ns.