
Cancer – Molecular basis
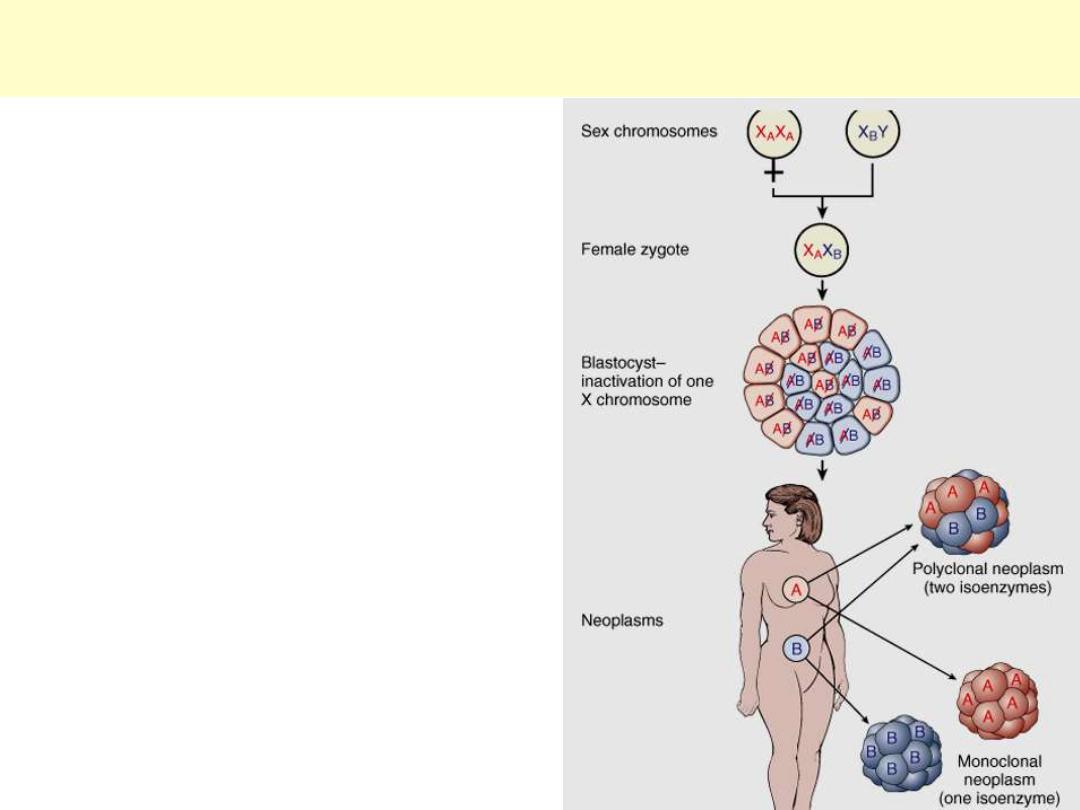
Because of random X inactivation, all females
are mosaics with two cell populations (with
glucose-6-phosphate dehydrogenase isoenzyme A
or B in this case). When neoplasms that arise in
women who are heterozygous for X-linked
markers are analyzed, they are made up of cells
that contain the active maternal (XA) or the
paternal (XB) X chromosome, but not both.
Currently, X-linked molecular markers are used
more commonly than isoenzyme variants.
Diagram depicting the use of X-linked isoenzyme cell markers as
evidence of the monoclonality of neoplasms.
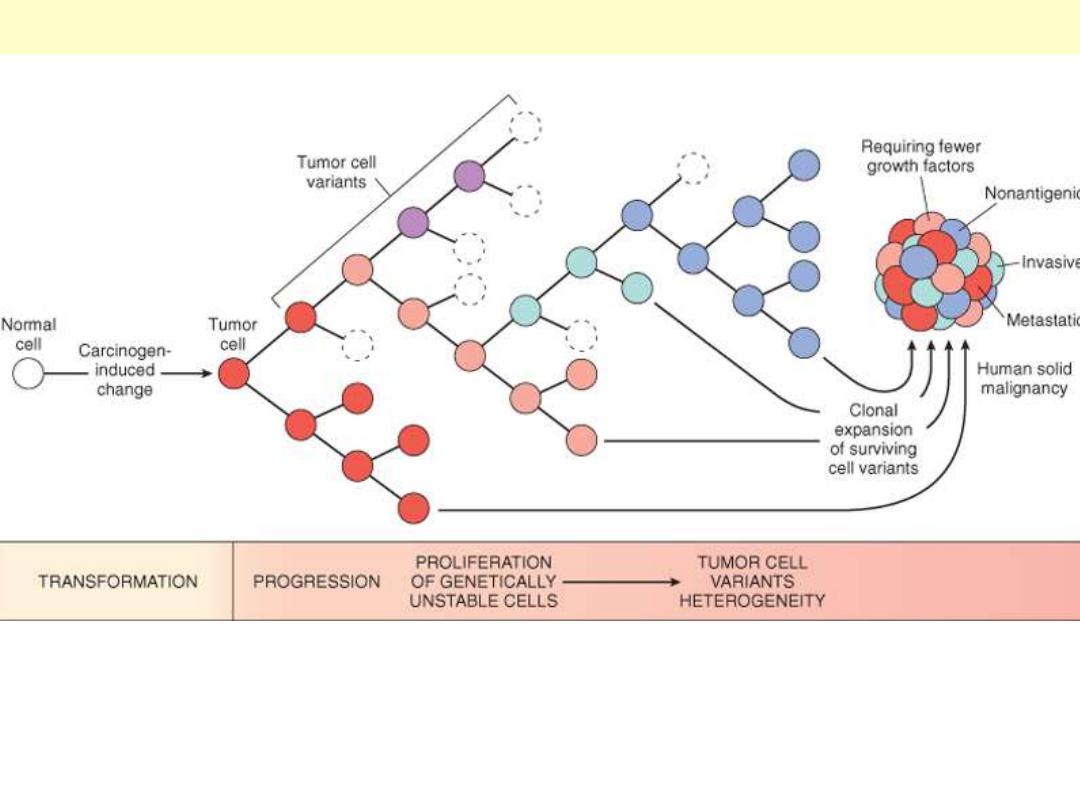
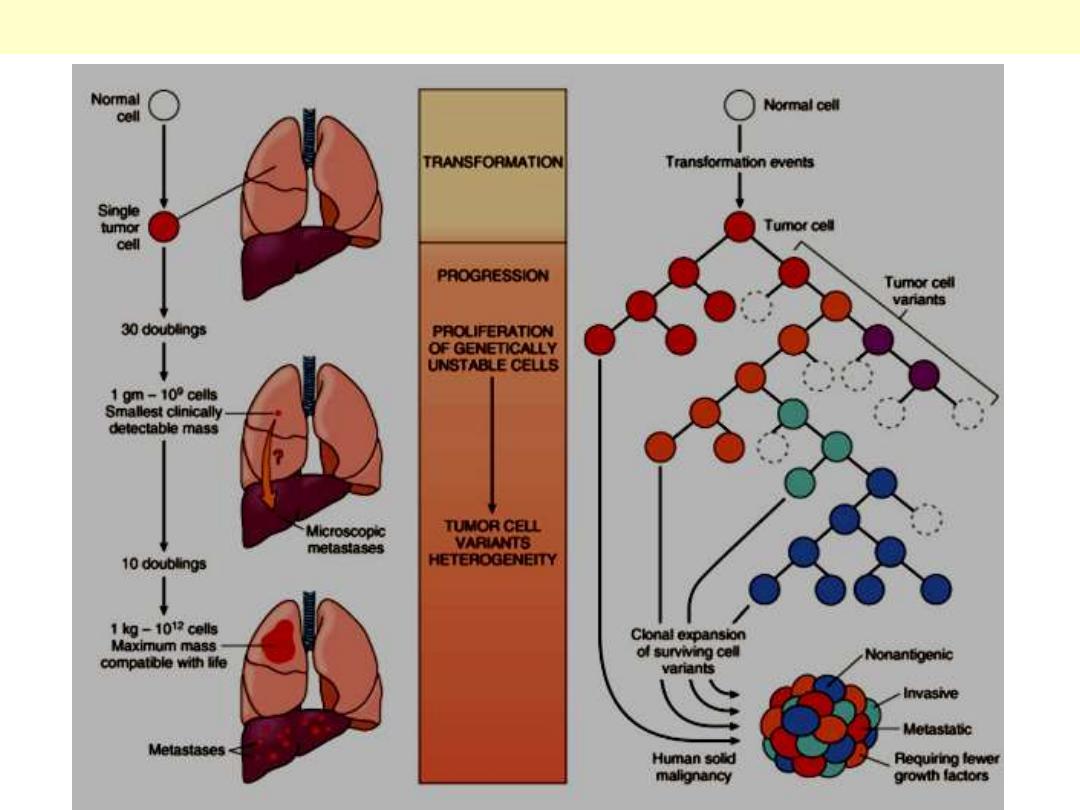
New subclones arise from the descendants of the original transformed cell by multiple mutations. With
progression the tumor mass becomes enriched for variants that are more adept at evading host
defenses and are likely to be more aggressive.
Tumor progression and generation of heterogeneity
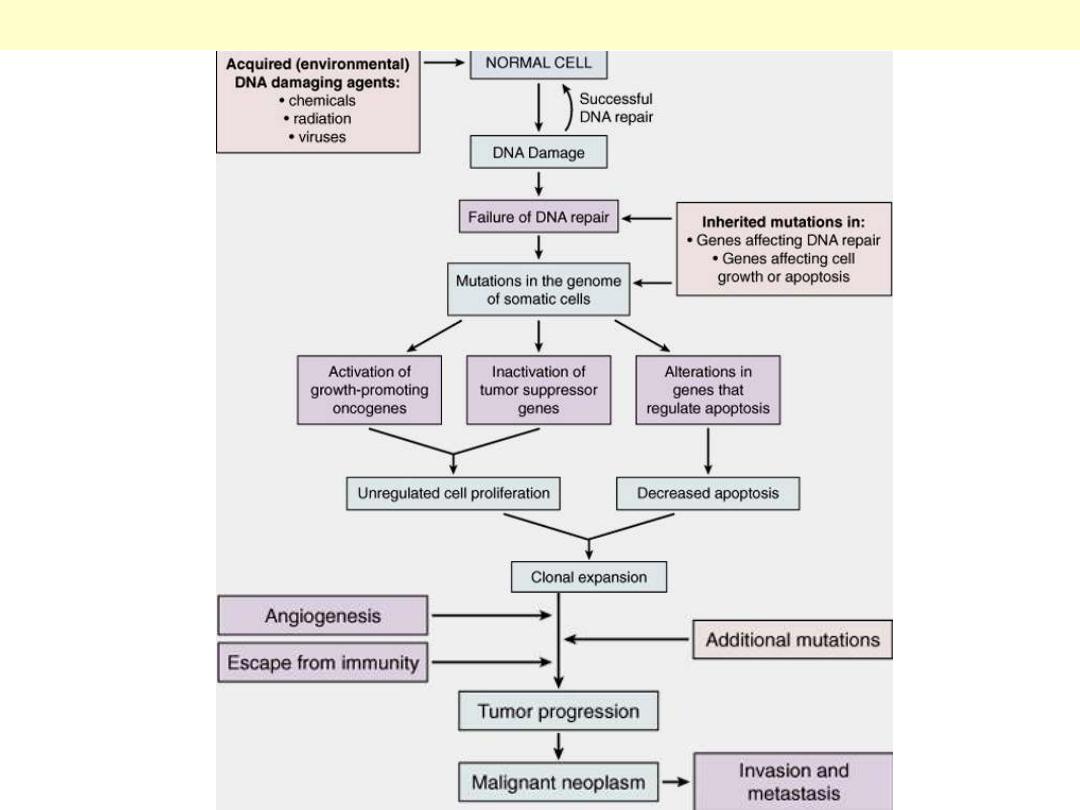
Flow chart depicting a simplified scheme of the molecular basis of cancer.
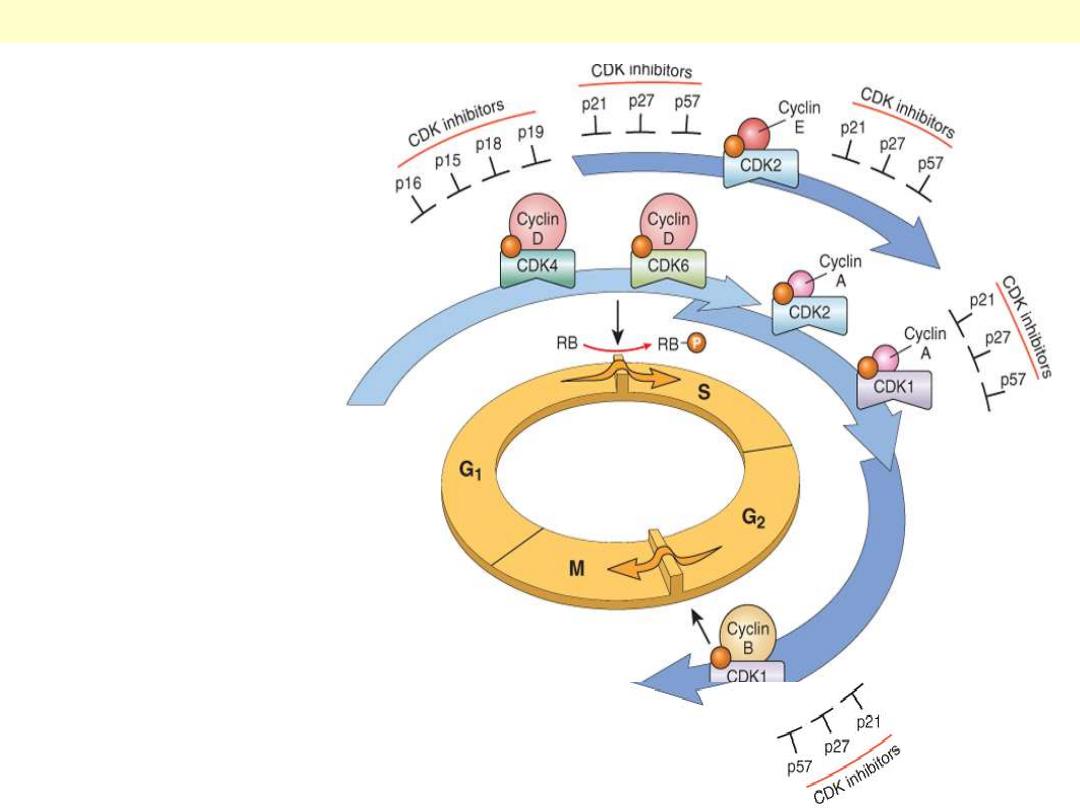
The shaded arrows
represent the phases of the
cell cycle during which
specific cyclin-CDK
complexes are active. As
illustrated, cyclin D-CDK4,
cyclin D-CDK6, and cyclin
E-CDK2 regulate the G1-to-
S transition by
phosphorylation of the RB
protein (pRB). Cyclin A-
CDK2 and cyclin A-CDK1
are active in the S phase.
Cyclin B-CDK1 is essential
for the G2-to-M transition.
Two families of CDK
inhibitors can block activity
of CDKs and progression
through the cell cycle. The
so-called INK4 inhibitors
composed of p16, p15, p18,
and p19, act on cyclin D-
CDK4 and cyclin D-CDK6.
The other family of three
inhibitors, p21, p27, and
p57, can inhibit all CDKs.
Schematic illustration of the role of cyclins, CDKs, and CDKIs in regulating the cell cycle
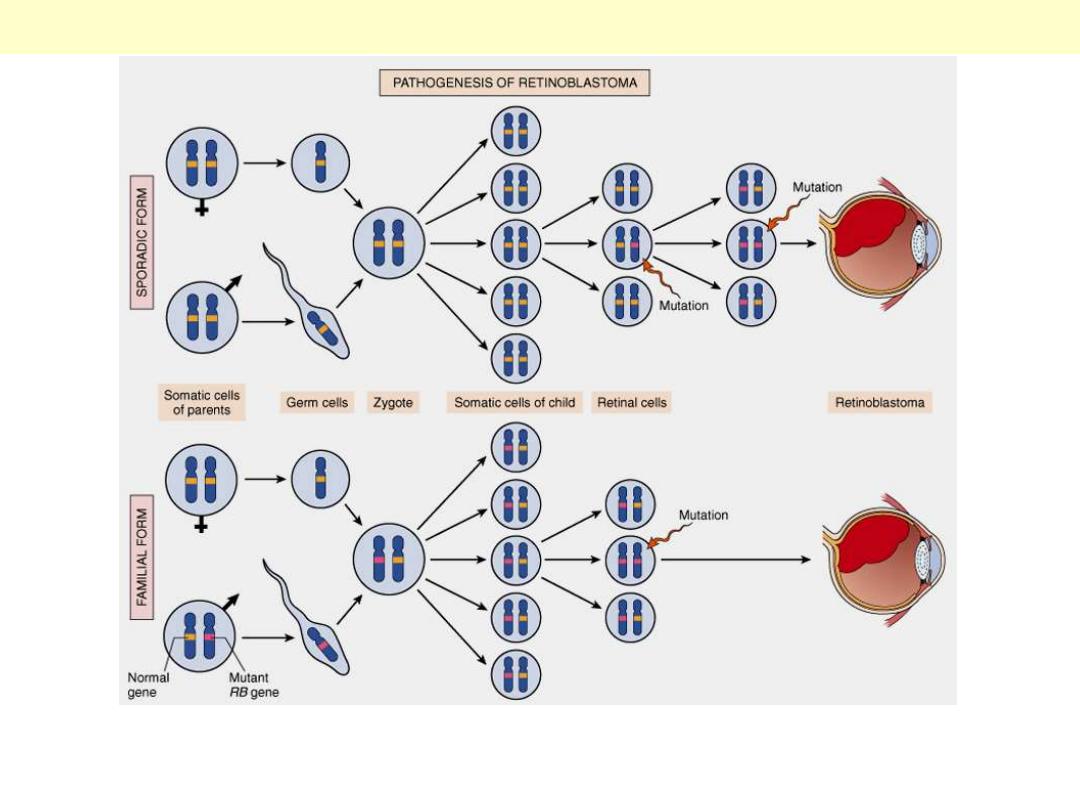
Two mutations of the RB locus on chromosome 13q14 lead to neoplastic proliferation of the retinal cells. In the
familial form, all somatic cells inherit one mutant RB gene from a carrier parent. The second mutation affects the RB
locus in one of the retinal cells after birth. In the sporadic form, both mutations at the RB locus are acquired by the
retinal cells after birth.
Pathogenesis of retinoblastoma.
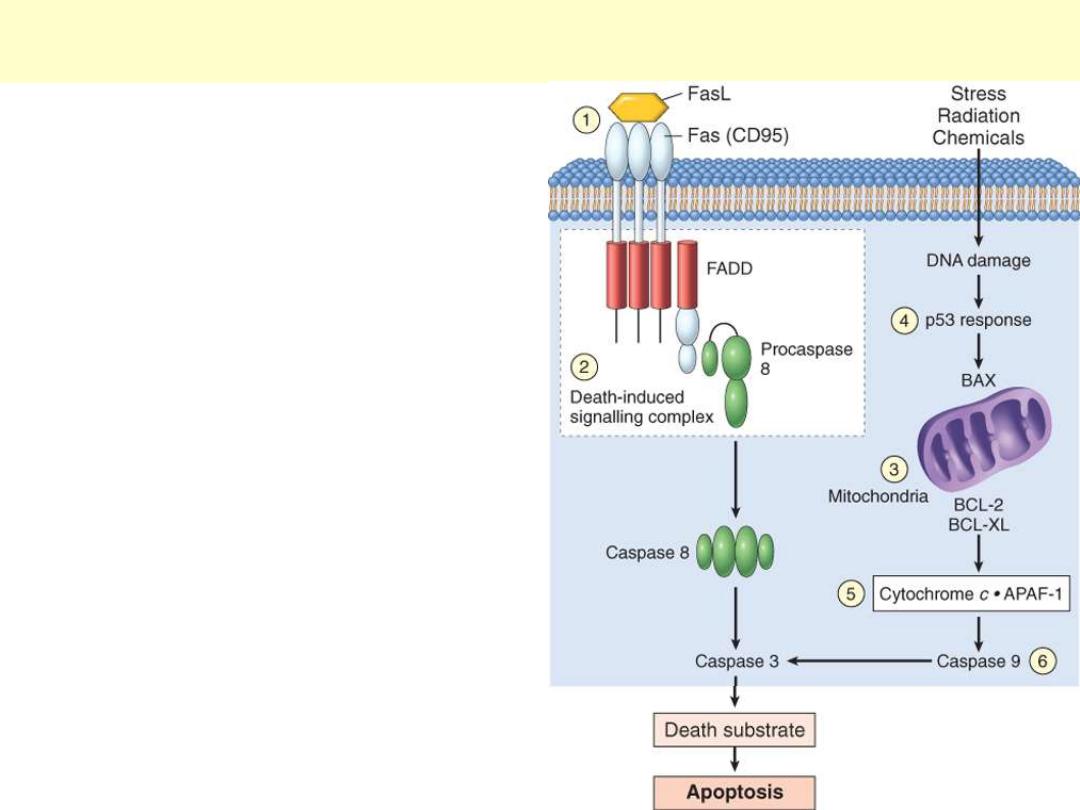
(1) Reduced CD95 level. (2) Inactivation of death-
induced signaling complex by FLICE protein. (3)
Reduced egress of cytochrome c from
mitochondrion as a result of up-regulation of
BCL2. (4) Reduced levels of pro-apoptotic BAX
resulting from loss of p53. (5) Loss of APAF-1. (6)
Up-regulation of inhibitors of apoptosis.
CD95 receptor-induced and DNA damage-triggered pathways of apoptosis and
mechanisms used by tumor cells to evade cell death

Differentiation –
Undifferentiated

Degrees of differentiation in various colonic tumors
Normal
adenoma
carcinoma
Poorly differentiated carcinoma
Very little evidence to suggest site of origin
Undifferentiated (Anaplastic) Cancer
Complete loss of differentiation (primitive
cells).
Frequent mitoses including abnormal ones
Cells/nuclei show marked
pleomorphism/sometimes
multinucleated tumor giant cells
Extreme nuclear hyperchromasia
Marked nuclear enlargement N:C may reach
1:1 (instead of 1:4 or 1:6)
The chromatin is coarsely clumped and
irregularly distributed
Usually large, prominent nucleoli
Undifferentiated (Anaplastic) Cancer
Complete loss of differentiation (primitive
cells).
Frequent mitoses including abnormal ones
Cells/nuclei show marked
pleomorphism/sometimes
multinucleated tumor giant cells
Extreme nuclear hyperchromasia
Marked nuclear enlargement N:C may reach
1:1 (instead of 1:4 or 1:6)
The chromatin is coarsely clumped and
irregularly distributed
Usually large, prominent nucleoli
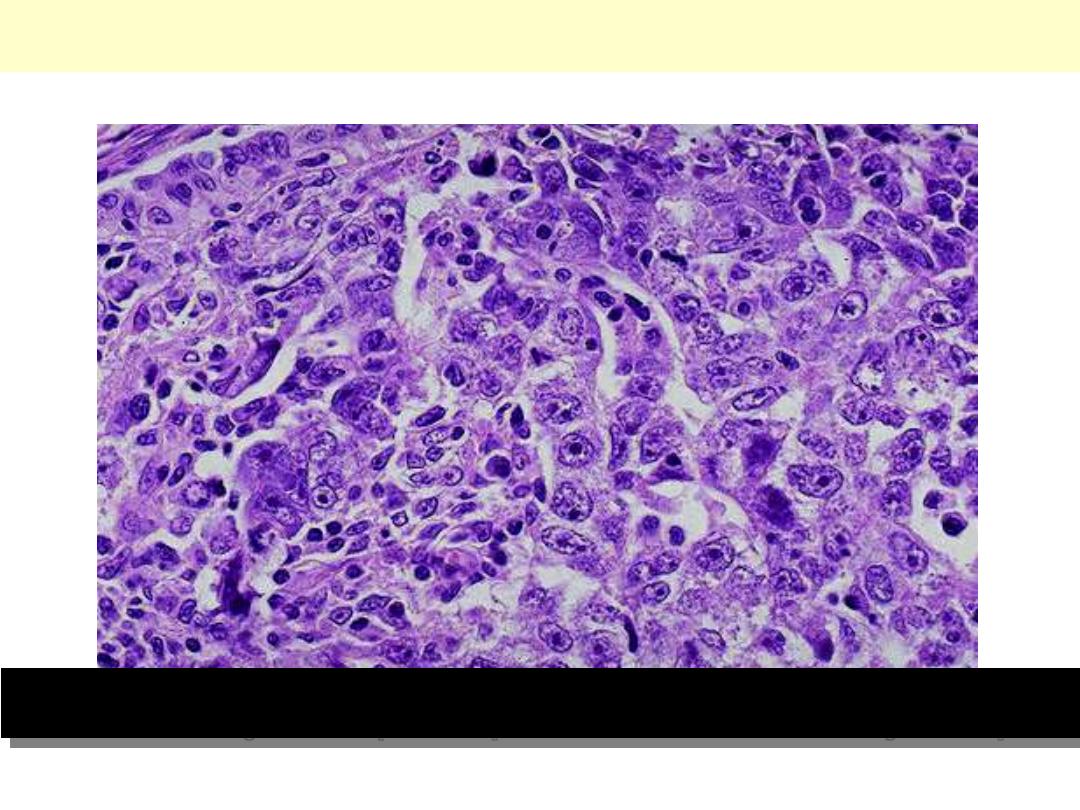
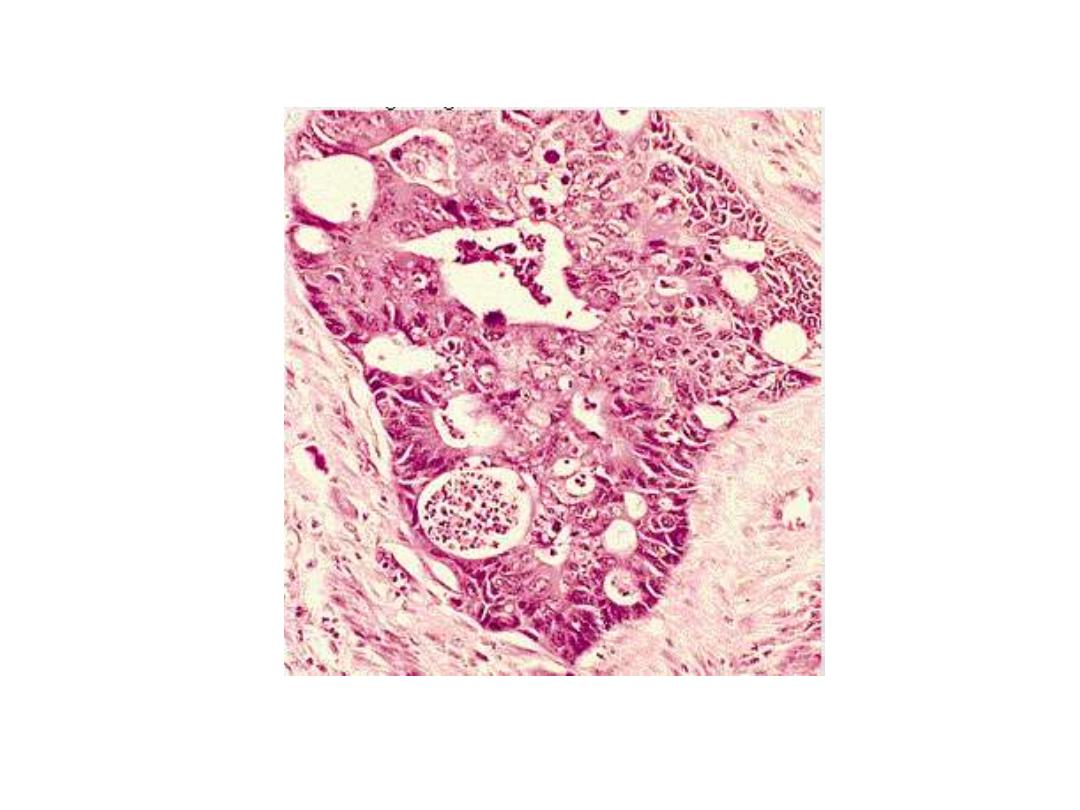
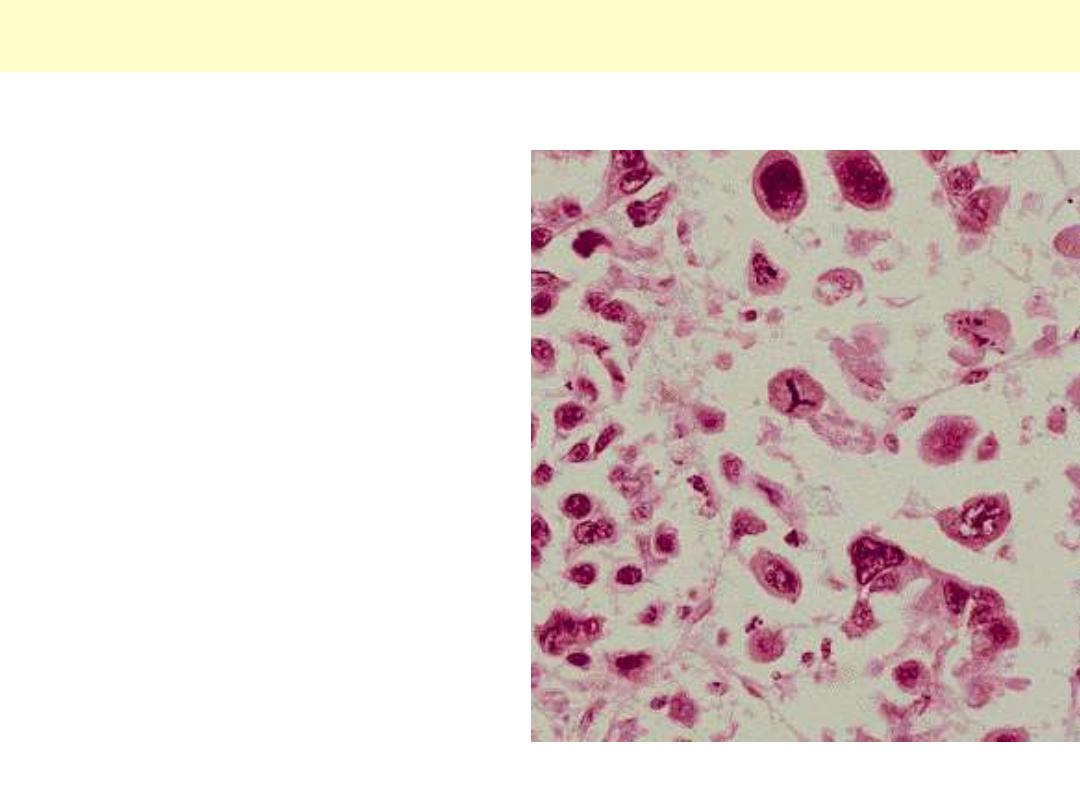
Undifferentiated/Anaplastic Carcinoma
This neoplasm is so poorly differentiated that it is difficult to tell the cell of origin. Note that nucleoli
are numerous and large in this neoplasm. Neoplasms with no differentiation are designated anaplastic.
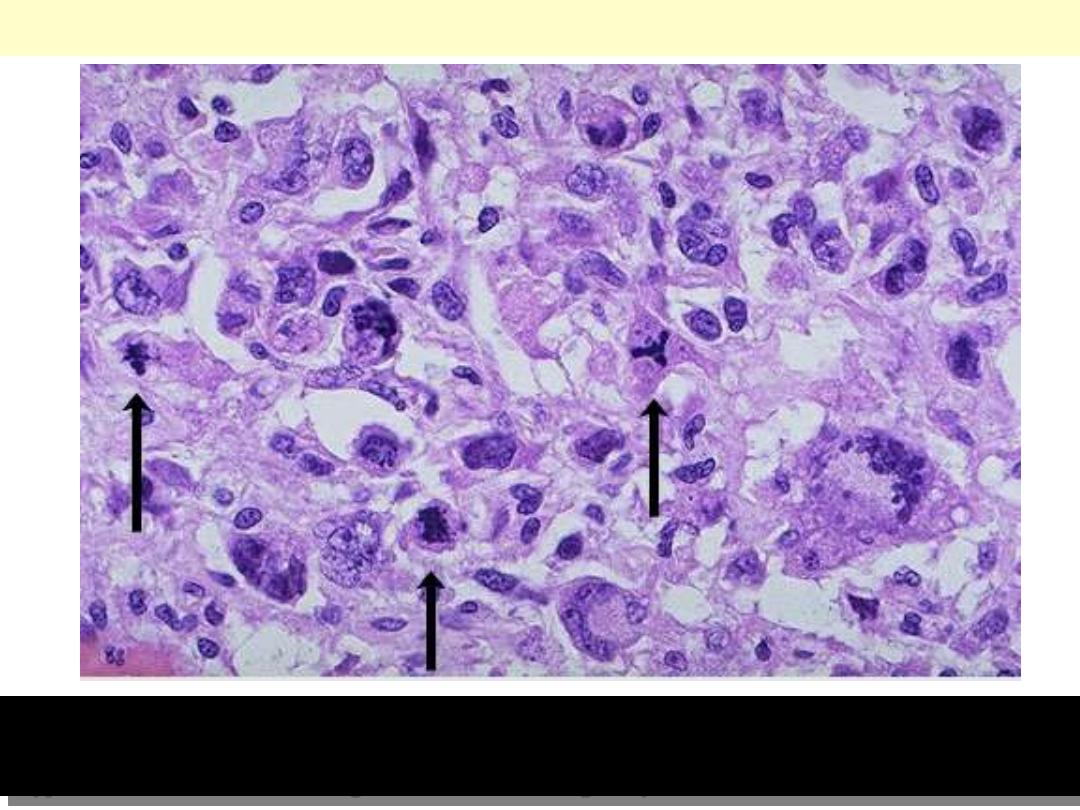
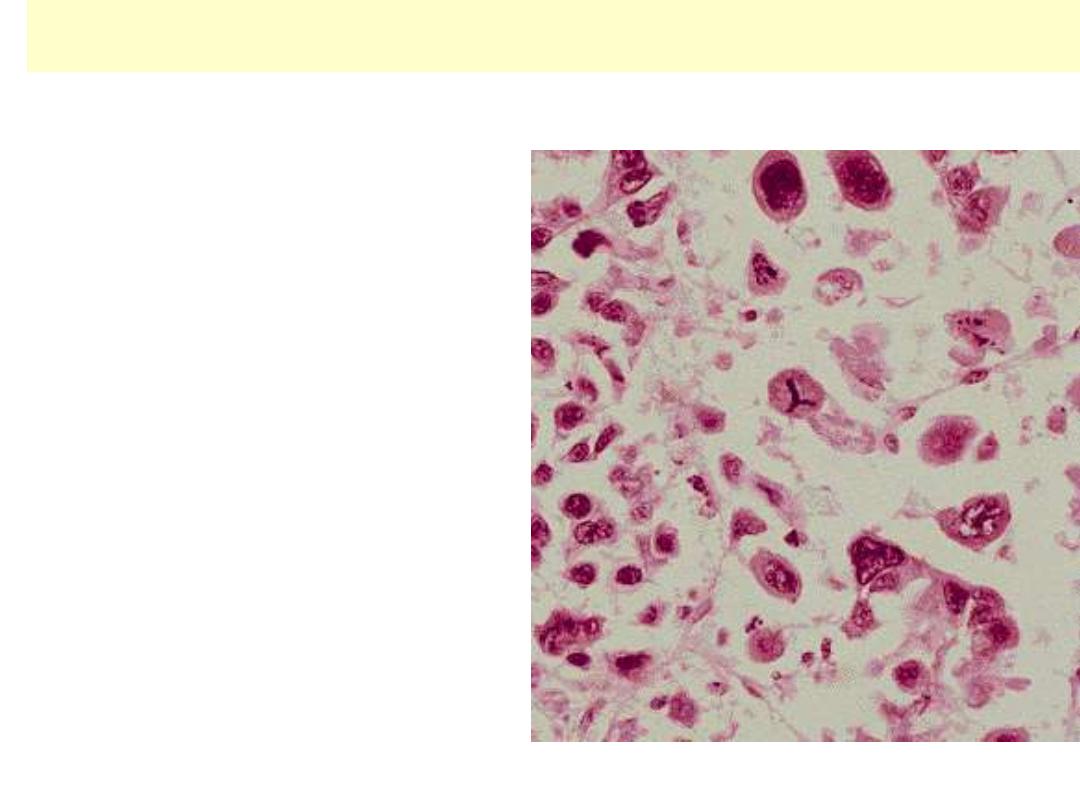
Abnormal Mitoses
Here are three abnormal mitoses. Mitoses by themselves are not indicators of malignancy. However,
abnormal mitoses are highly indicative of malignancy. The marked pleomorphism and
hyperchromatism of surrounding cells also favors malignancy.
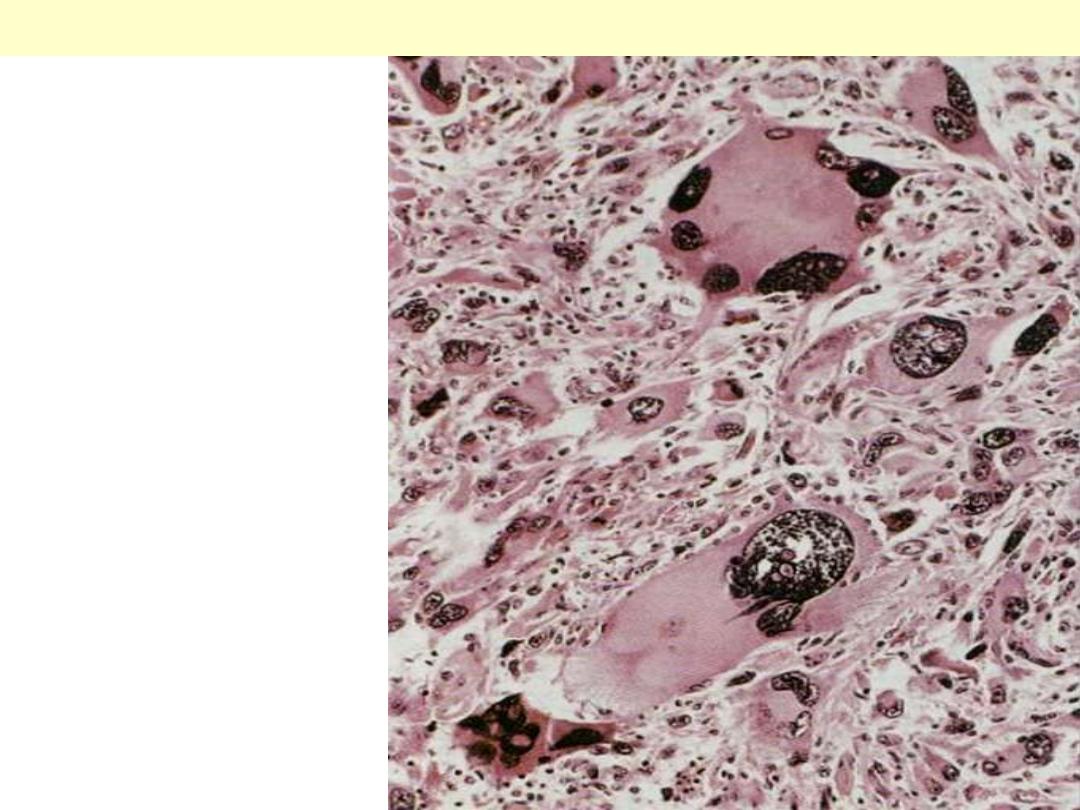
Rhabdomyosarcoma
Pleomorphic rhabdomyosarcoma
showing prominent pleomorphism,
frankly malignant nuclei &
malignant multinucleated giant
cells.

Differentiation – Very well
differentiated

Leiomyomas uteri
Multiple leiomyomas of the uterus. These common
smooth muscle tumors can occur within the
myometrium (intramural), subjacent to the serosa
(subserosal) or just below the endometrium
(submucosal). This example shows all the three
gross types.
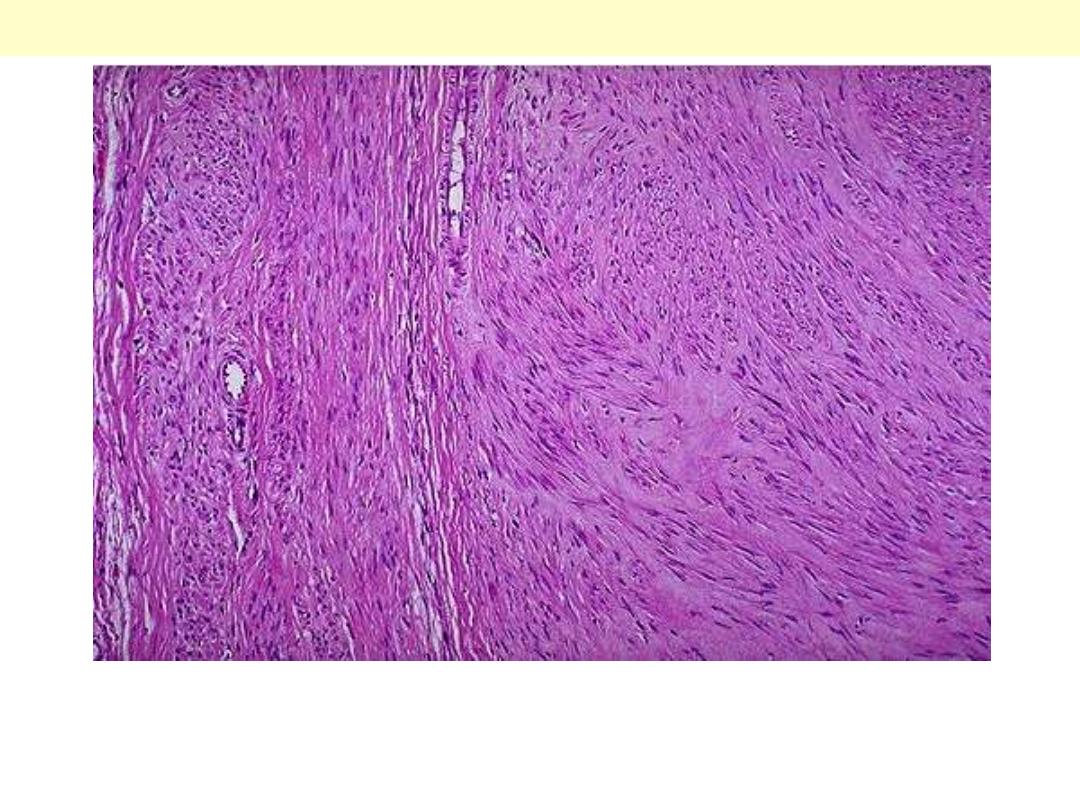
Leiomyoma
Sections from a leiomyoma show interlacing bundles of benign smooth muscle cells that simulate very
closely their native counterparts.
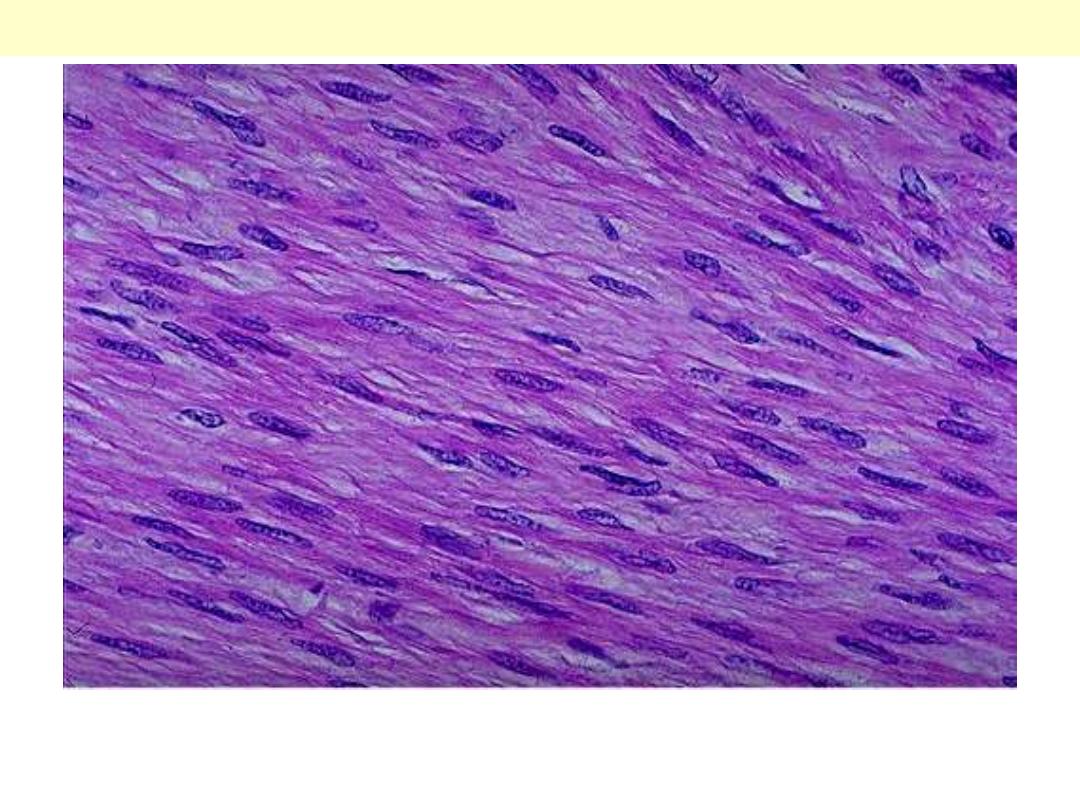
A higher magnification showing benign-looking spindle cells with cigar-shaped nuclei & fibrillary
pinkish cytoplasm.
Leiomyoma
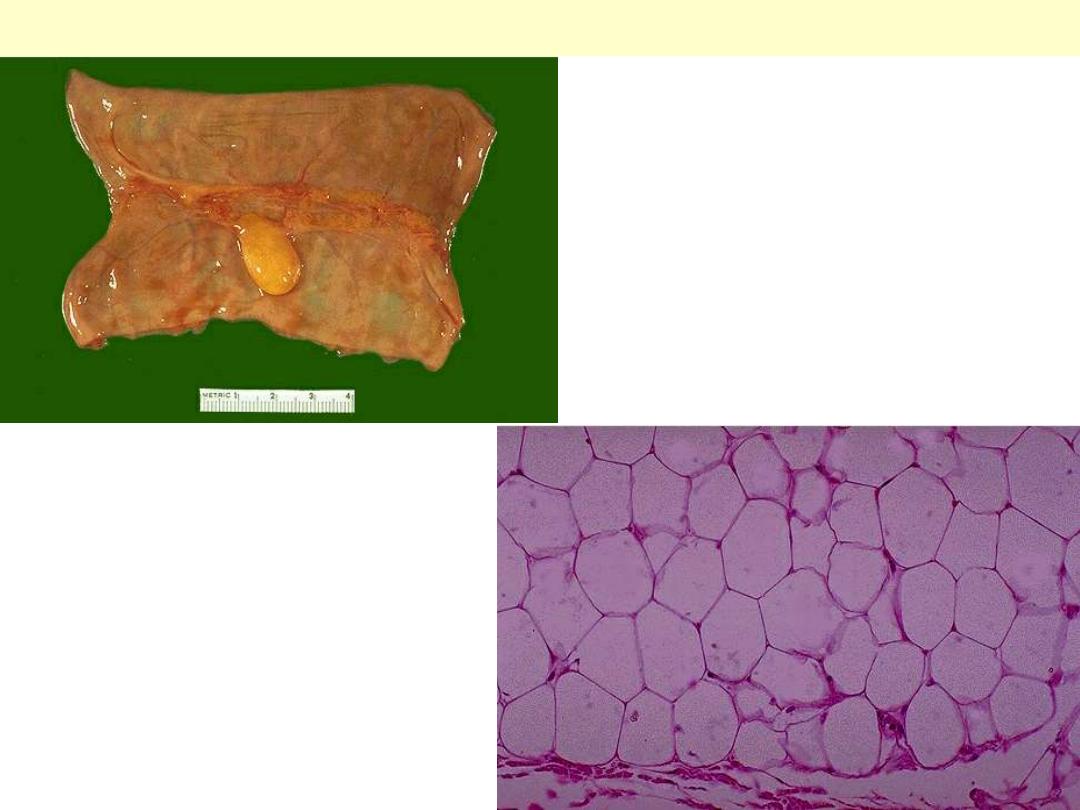
Lipoma small intestine
Lipoma arising from the serosal aspect of the
small intestine. It is ovoid with smooth outer
surface & has the typical bright yellow color.
Microscopic section shows closely packed
benign lipocytes. These are difficult to
differentiate from their normal counterparts.

Differentiation – Well
Differentiated
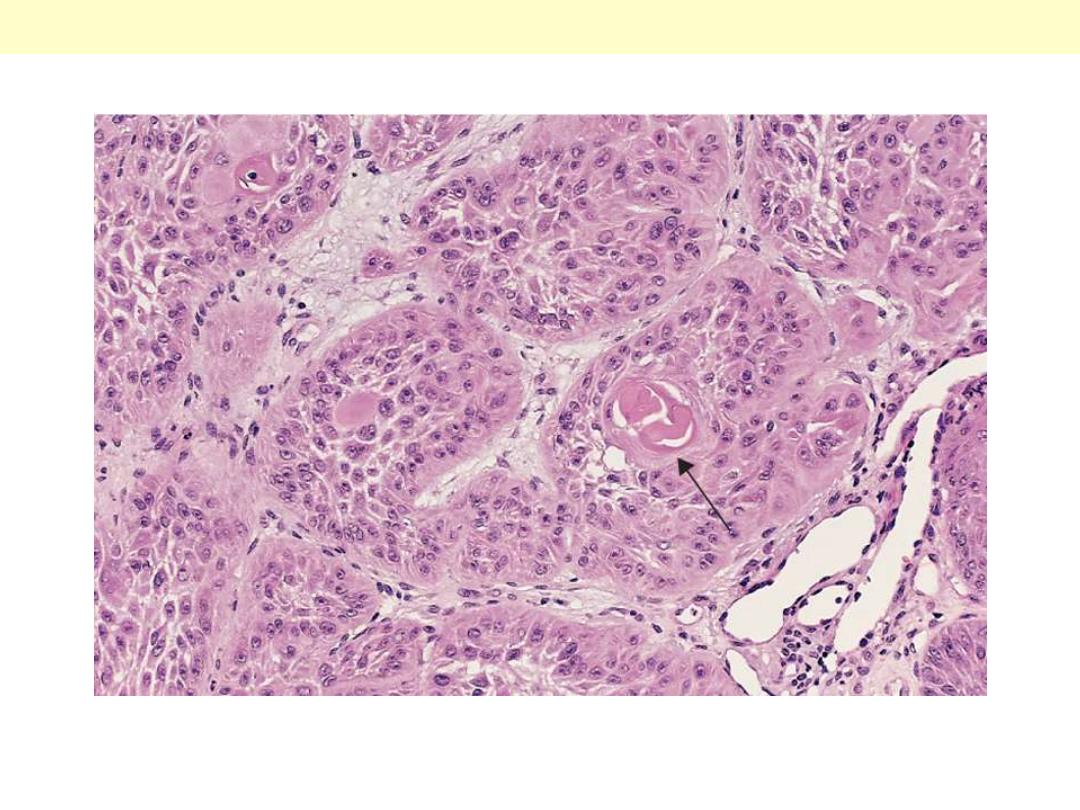
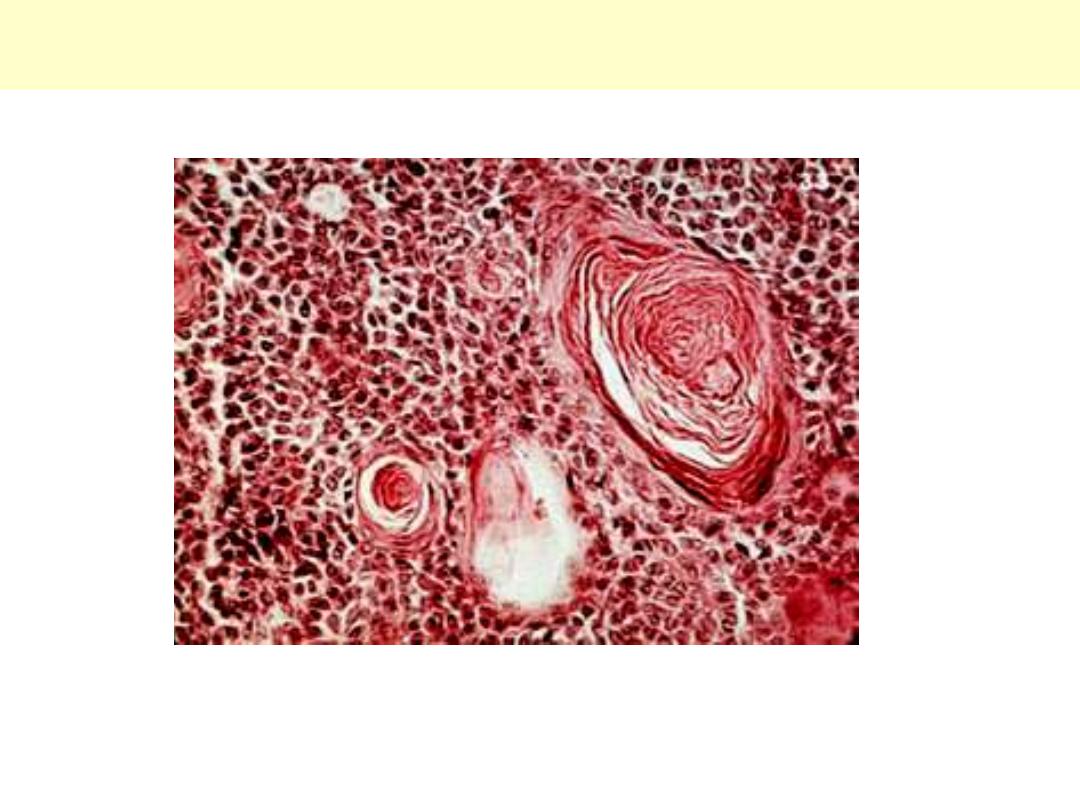
The tumor cells are strikingly similar to normal squamous epithelial cells, with intercellular bridges
and nests of keratin pearls (arrow).
Well-differentiated squamous cell carcinoma of the skin

Dysplasia – Carcinoma in situ
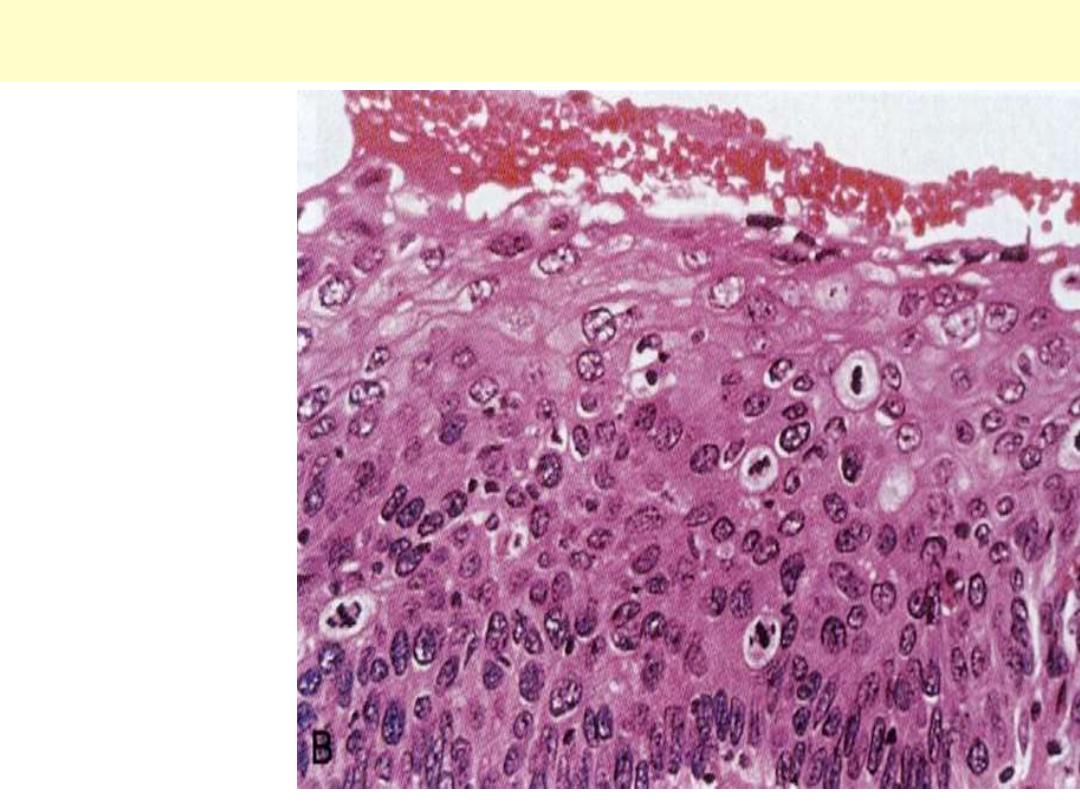
Cervix uteri severe dysplasia amounting to carcinoma in situ
There is failure of normal
differentiation, marked
nuclear and cellular
pleomorphism, and
numerous mitotic figures
extending toward the
surface. The intact
basement membrane
(below) is not seen in this
section.

Ectopia - Pancreas

Ectopic pancreas wall of jejunum (arrow)
Invasion - Local
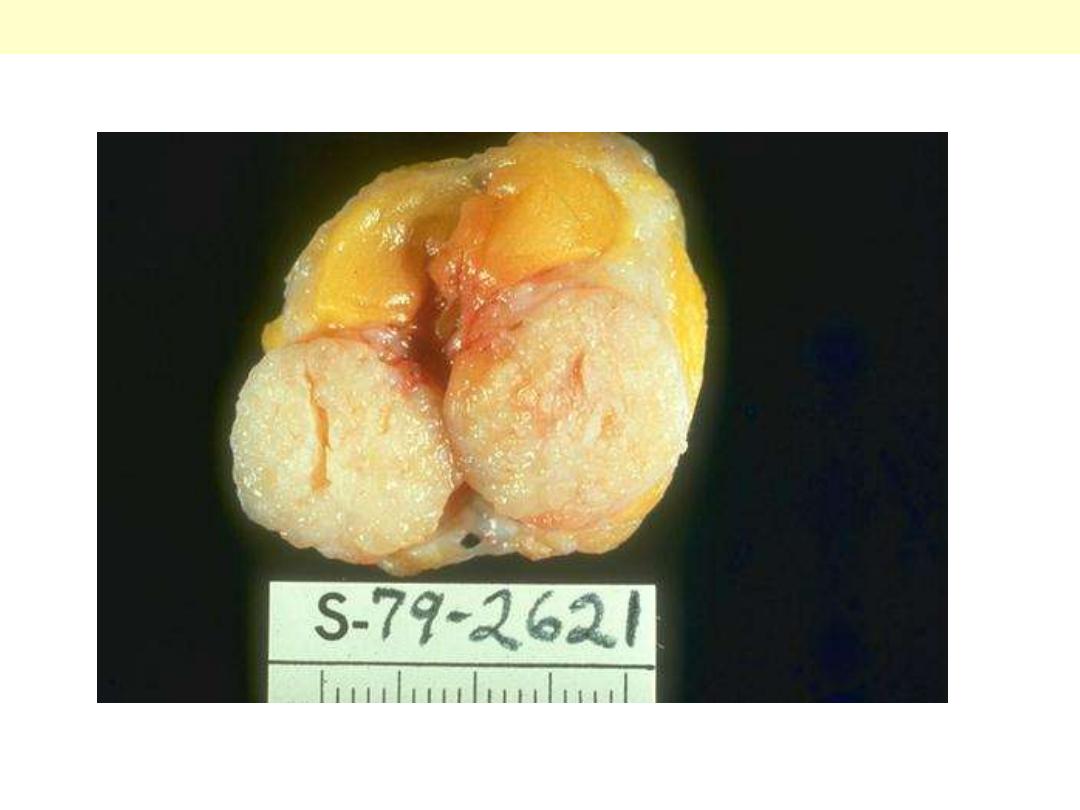
Sharply demarcated mass, about 3 cm in diameter. The cut surface is solid, grayish white. It is clearly
separated from surrounding native fibrofatty tissue of the breast.
Fibroadenoma Breast
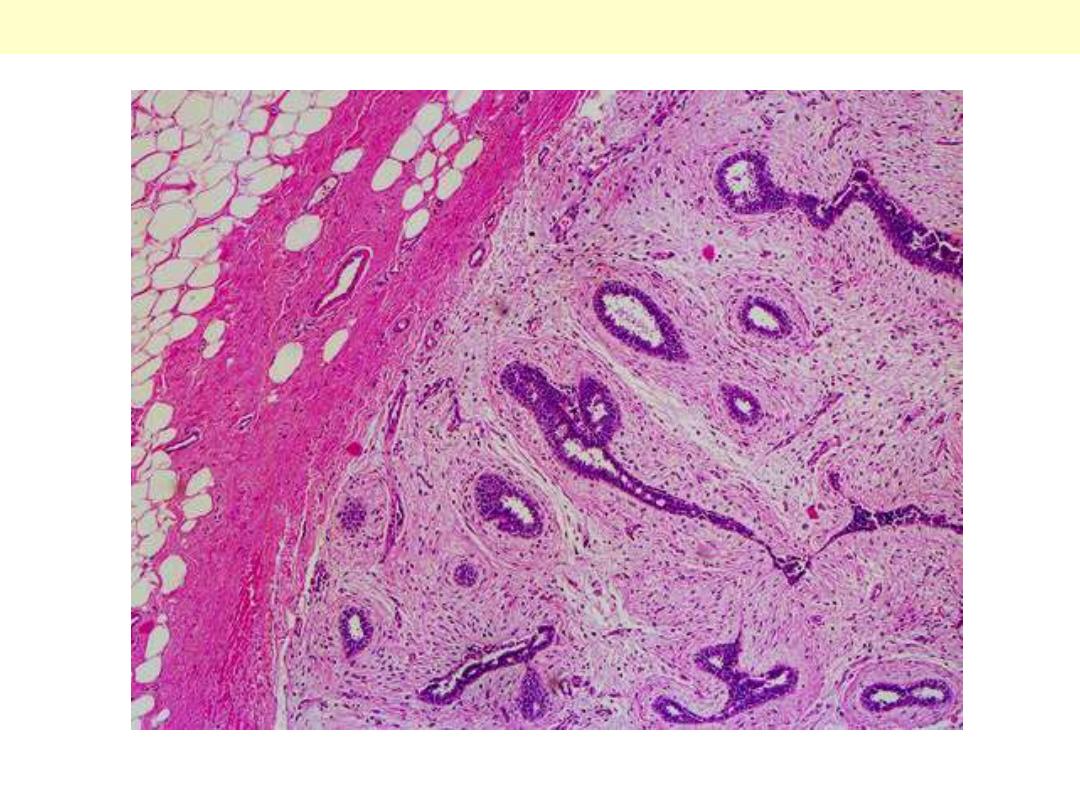
Well-defined fibrotic capsule surrounding the tumor. The latter consists of compressed ducts set within
fibroblastic stroma.
Fibroadenoma Breast

Carcinoma lung invasion
Malignant neoplasms are characterized by the tendency to invade surrounding tissues. Here, a lung
cancer is seen to be spreading along the bronchi into the surrounding lung tissues & pleura.
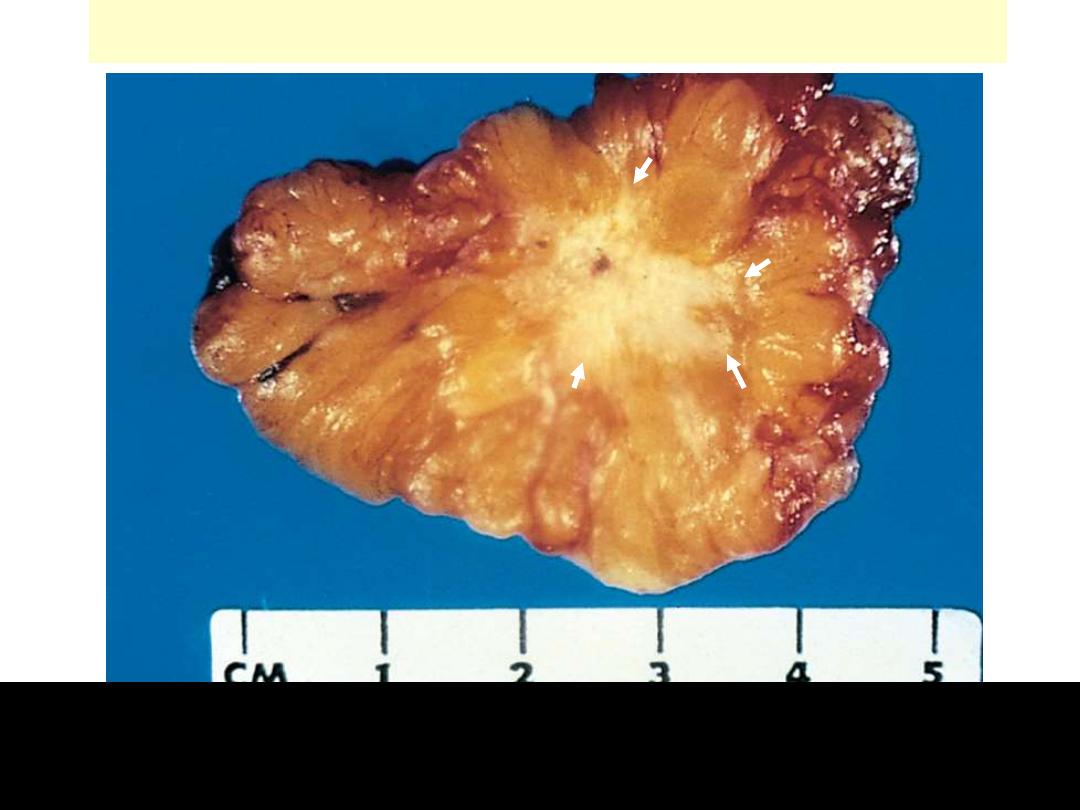
Ca breast invasion
This carcinoma of the breast is definitely infiltrating the surrounding breast. The central white area is
very hard in consistency and gritty on section, because the neoplasm is producing a desmoplastic
reaction with lots of collagen. This is often called a "scirrhous" appearance. There is also focal
dystrophic calcification leading to the gritty areas.
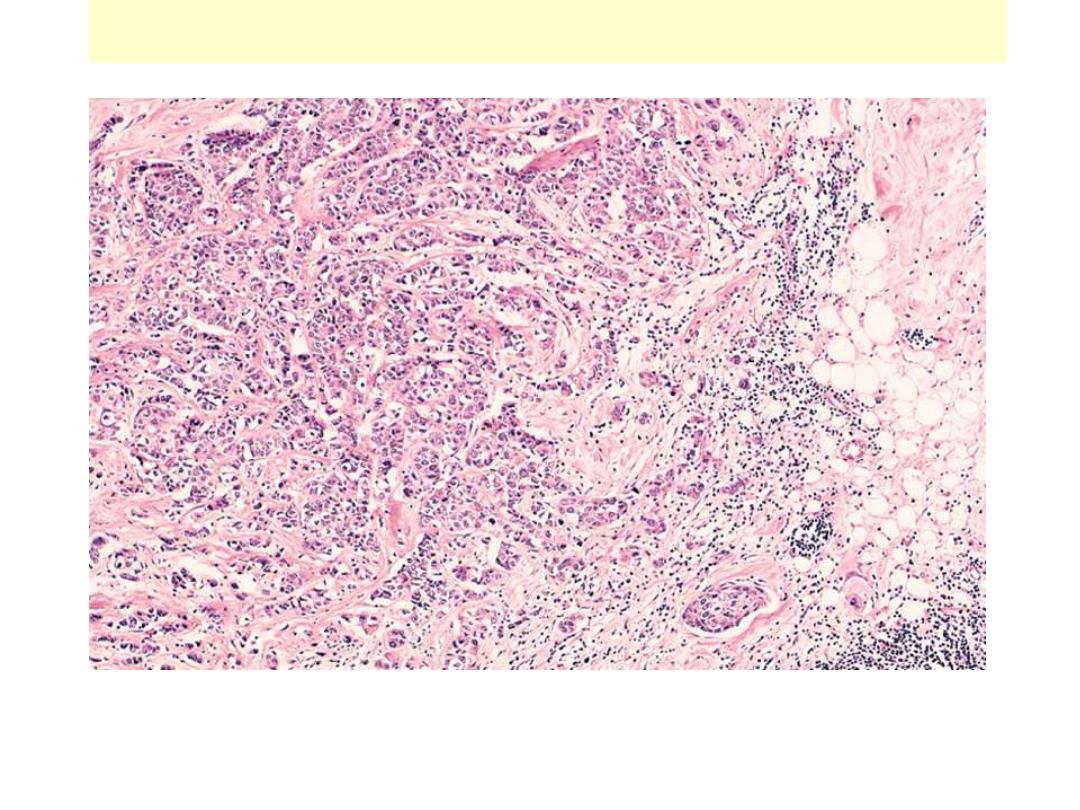
Ca breast invasion
On micrscopic examination, the infiltrating ductal carcinoma of the breast has pleomorphic cells
infiltrating through the stroma.
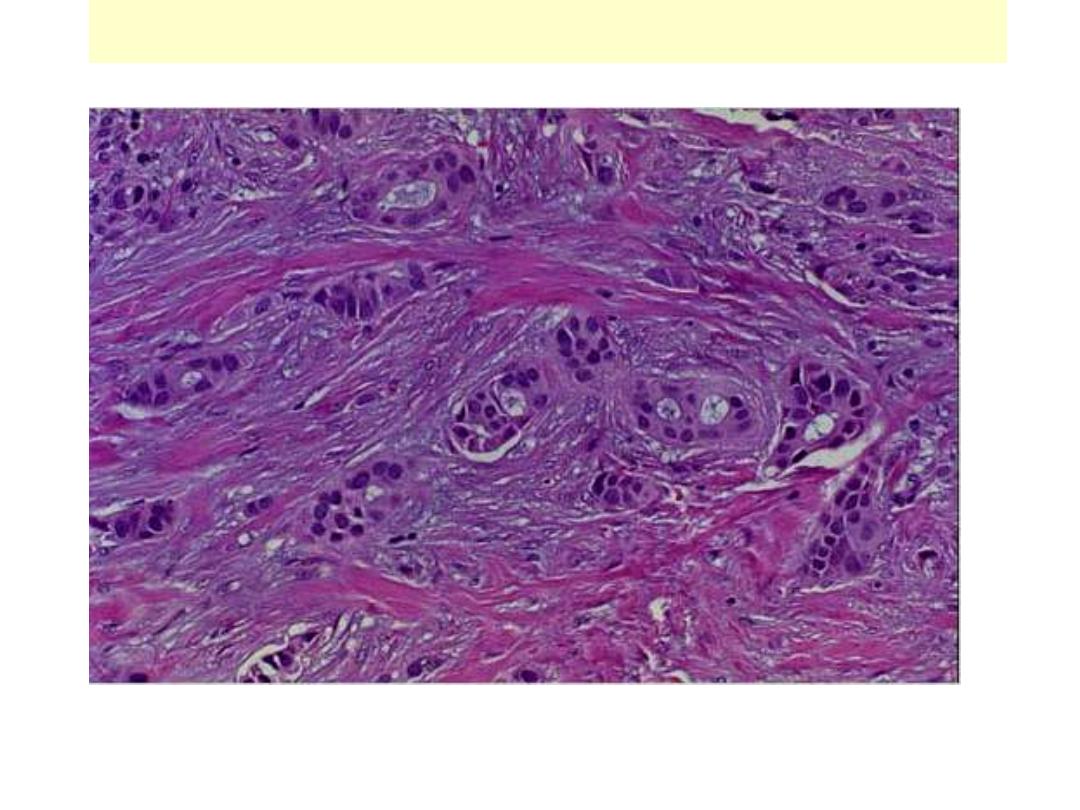
Ca breast invasion
On micrscopic examination, the infiltrating ductal carcinoma of the breast has pleomorphic cells
infiltrating through the stroma.
Metastasis
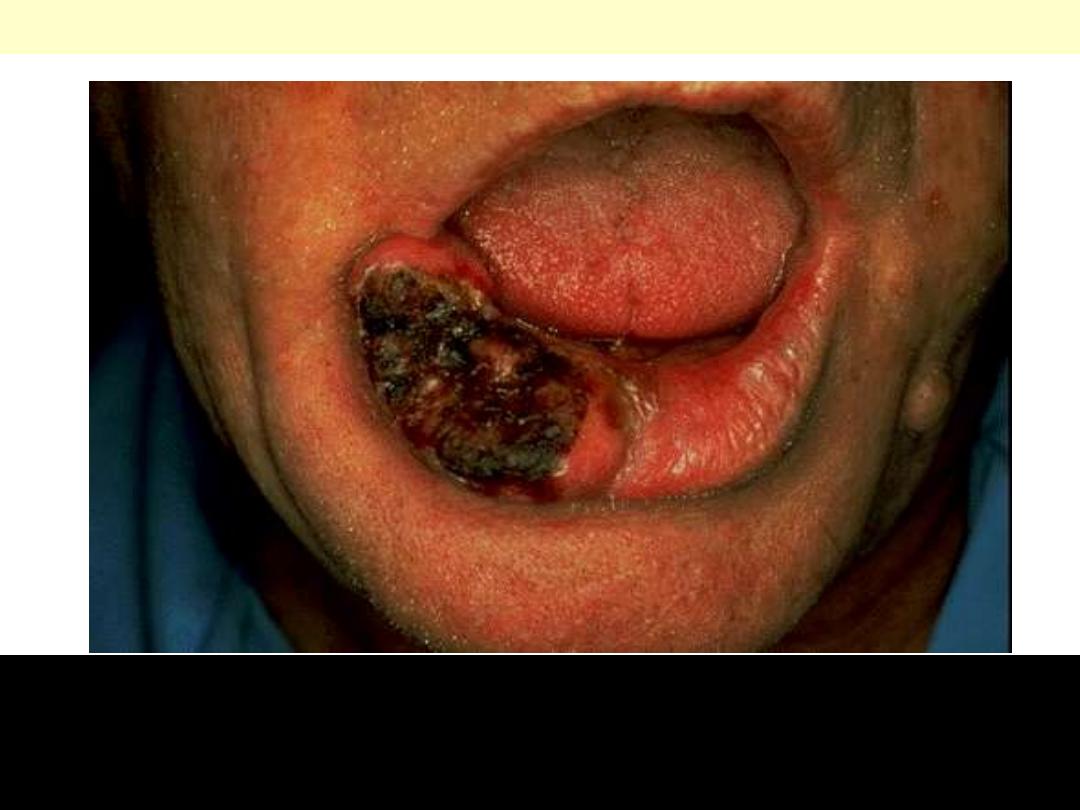
Basal cell carcinoma lower lip
These rarely metastasize, but are slow-growing and progressive over time. Leaving them to get larger
just makes the plastic surgeon's job much harder, with more disability to the patient, so early detection
and excision is a must. Most basal cell carcinomas occur in the head and neck area of adults with
prolonged sun exposure. Biopsy & microscopic examination are necessary steps to establish the
diagnosis.
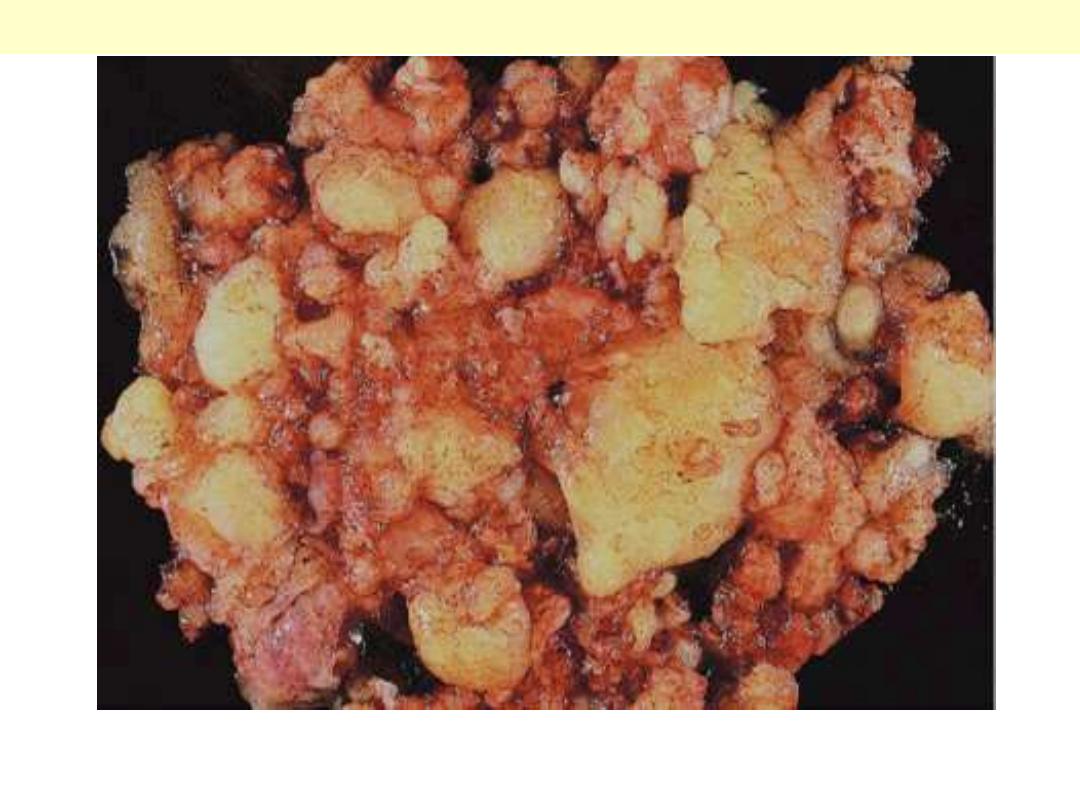
Pseudomyxoma peritonei
The entire peritoneal cavity is occupied by a multinodular mucinous mass
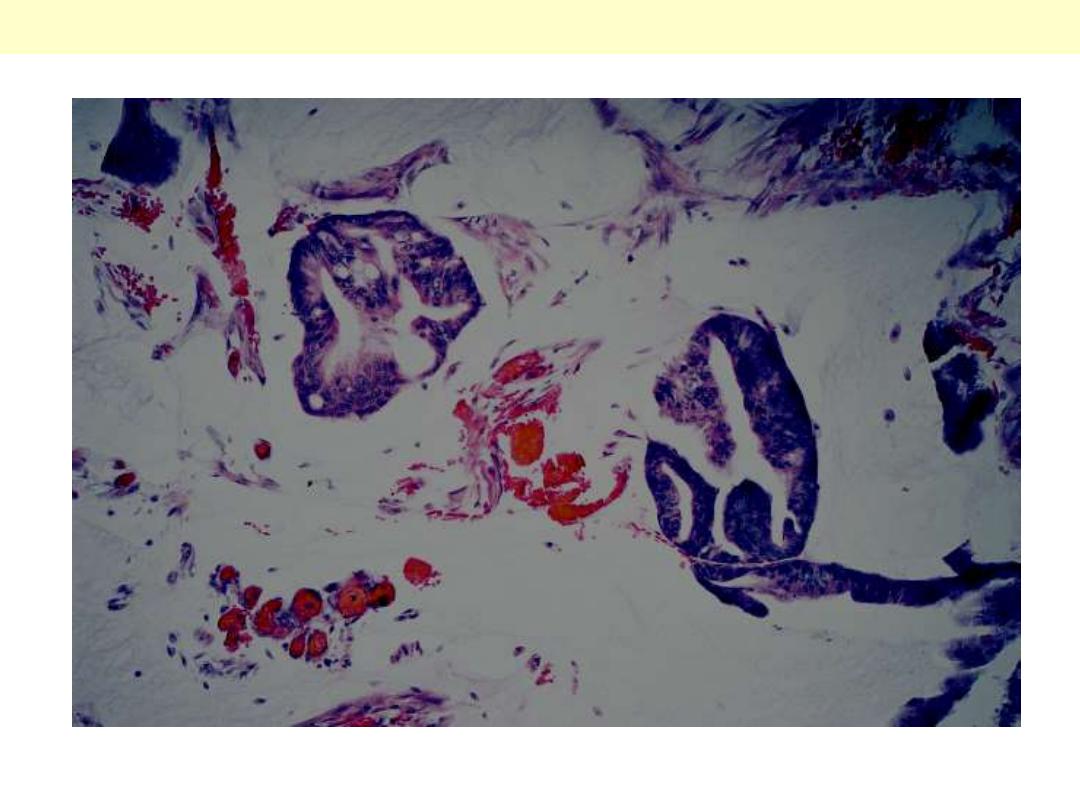
Pseudomyxoma peritonei
Clusters of well-differentiated mucin-producing glandular cells are seen floating in a sea of mucin.
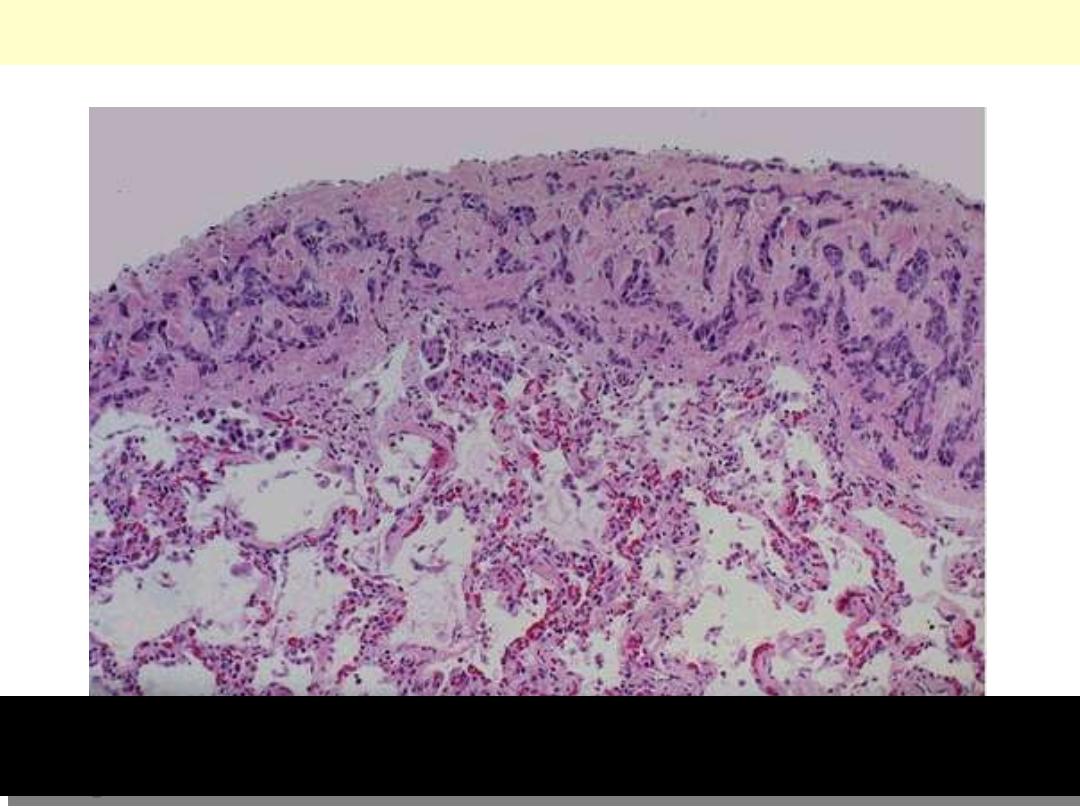
Metastatic breast carcinoma-pleura
Neoplasms can spread by seeding along body cavities, and this pattern is more typical for carcinomas
than other neoplasms. Here is a focus of metastatic breast carcinoma seen along the pleura overlying
the lung.
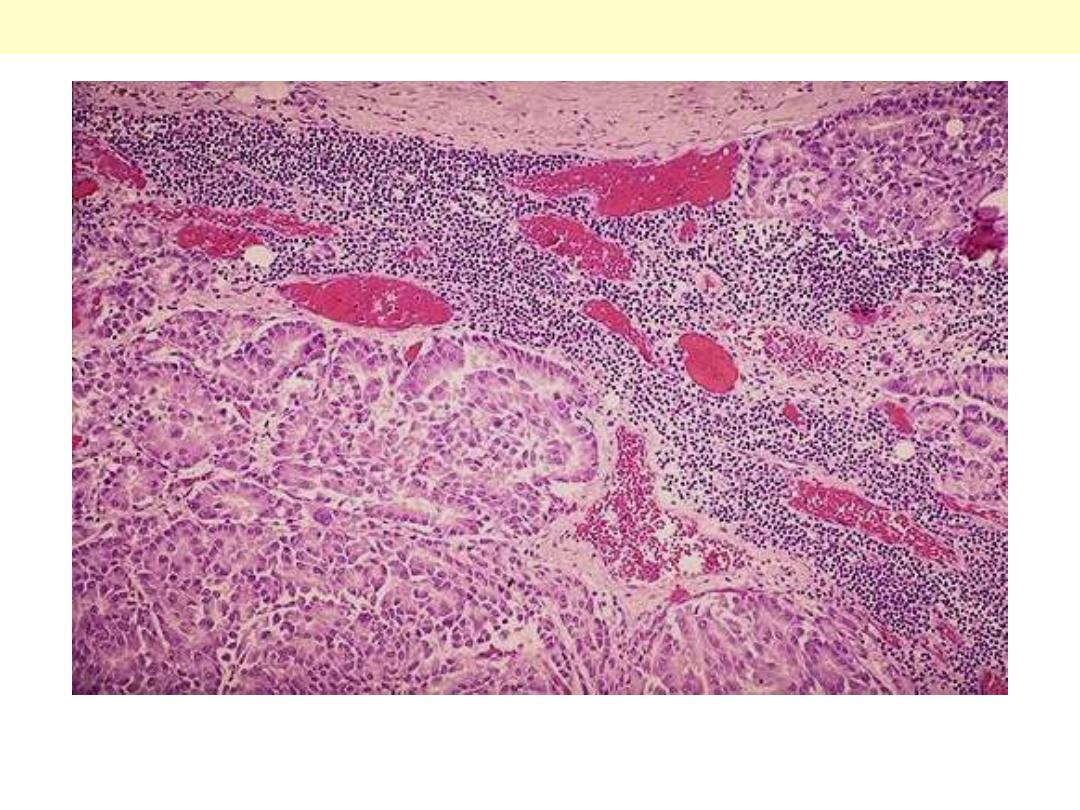
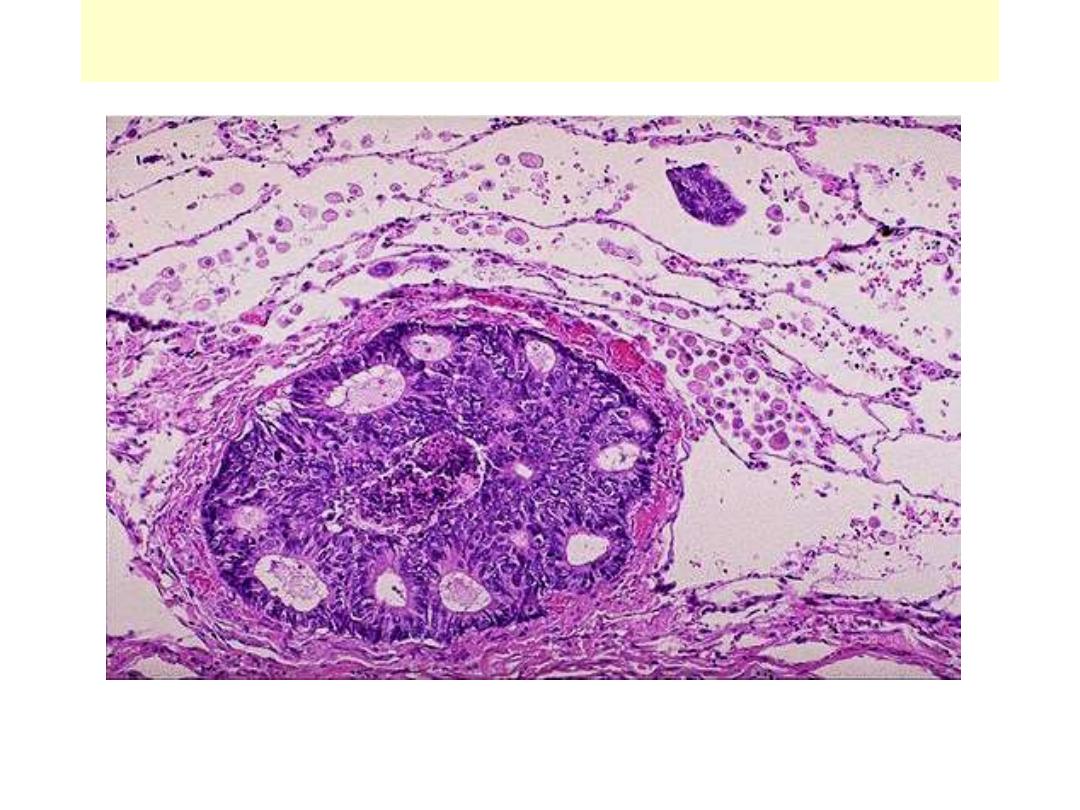
Microscopically, metastatic adenocarcinoma is seen in a lymph node here. It is common for carcinomas
to metastasize to lymph nodes. The first nodes involved are those draining the site of the primary.
Lymph node: metastatic adenocarcinoma
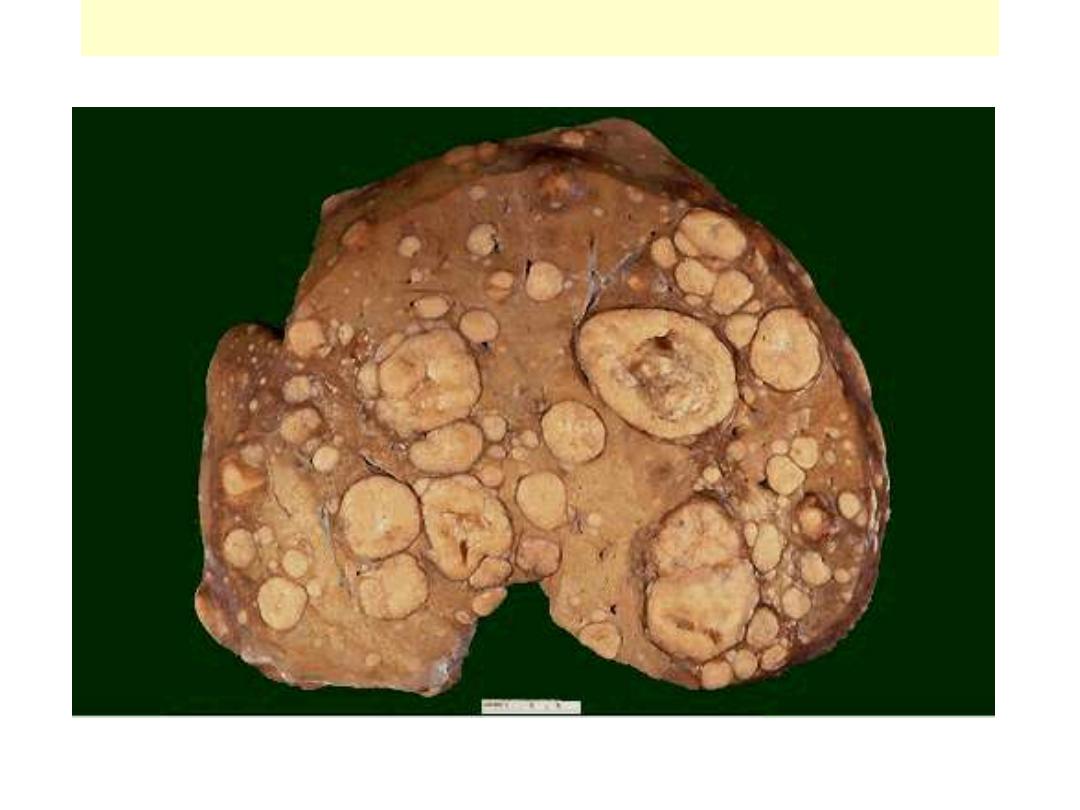
Liver metastases
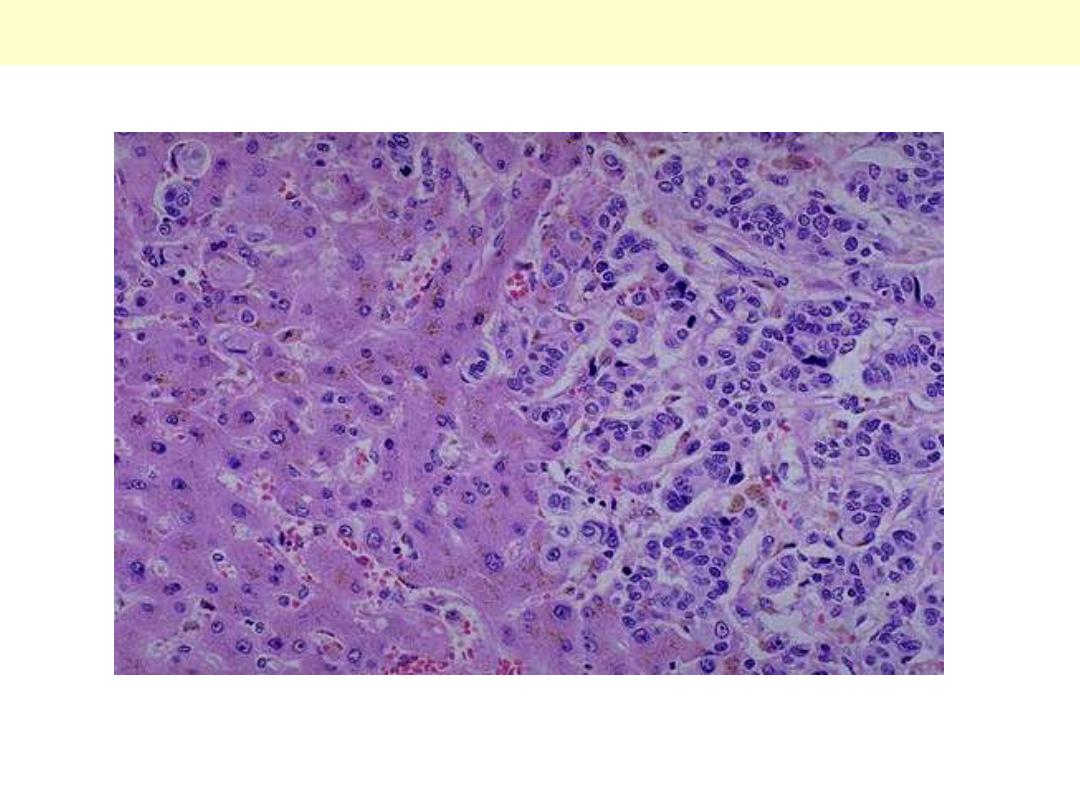
Liver metastasis by adenocarcinoma
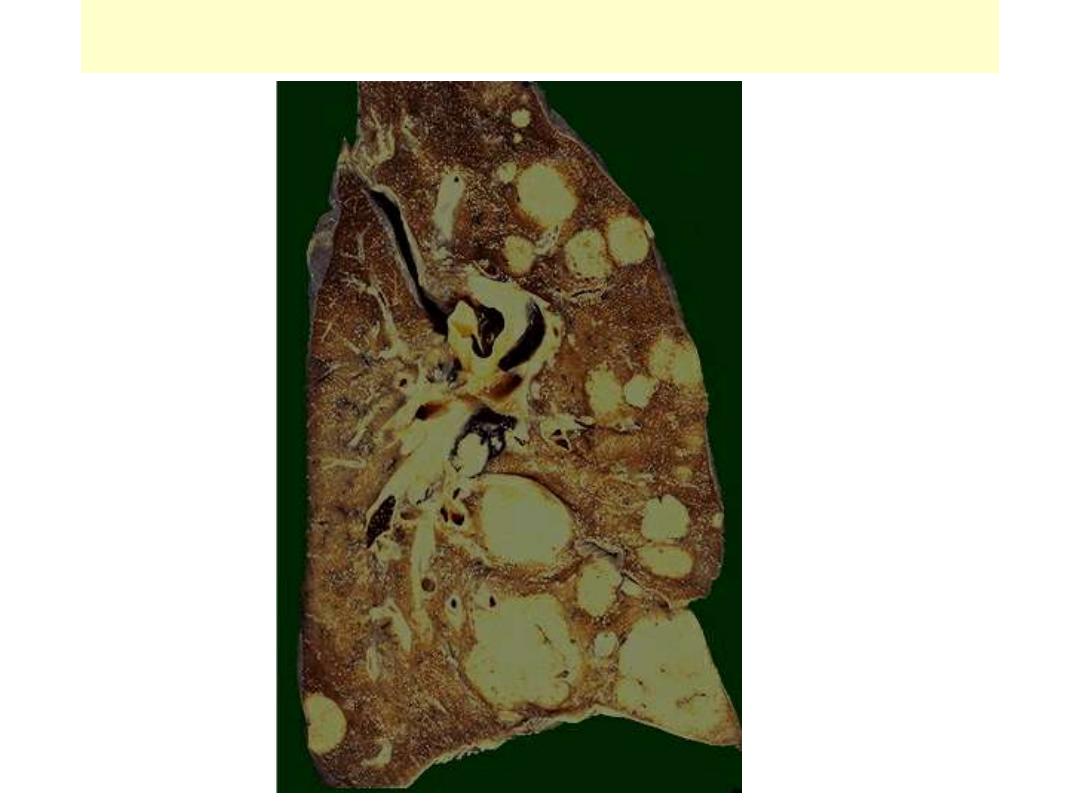
Pulmonary metastases
Metastatic adenocarcinoma lung
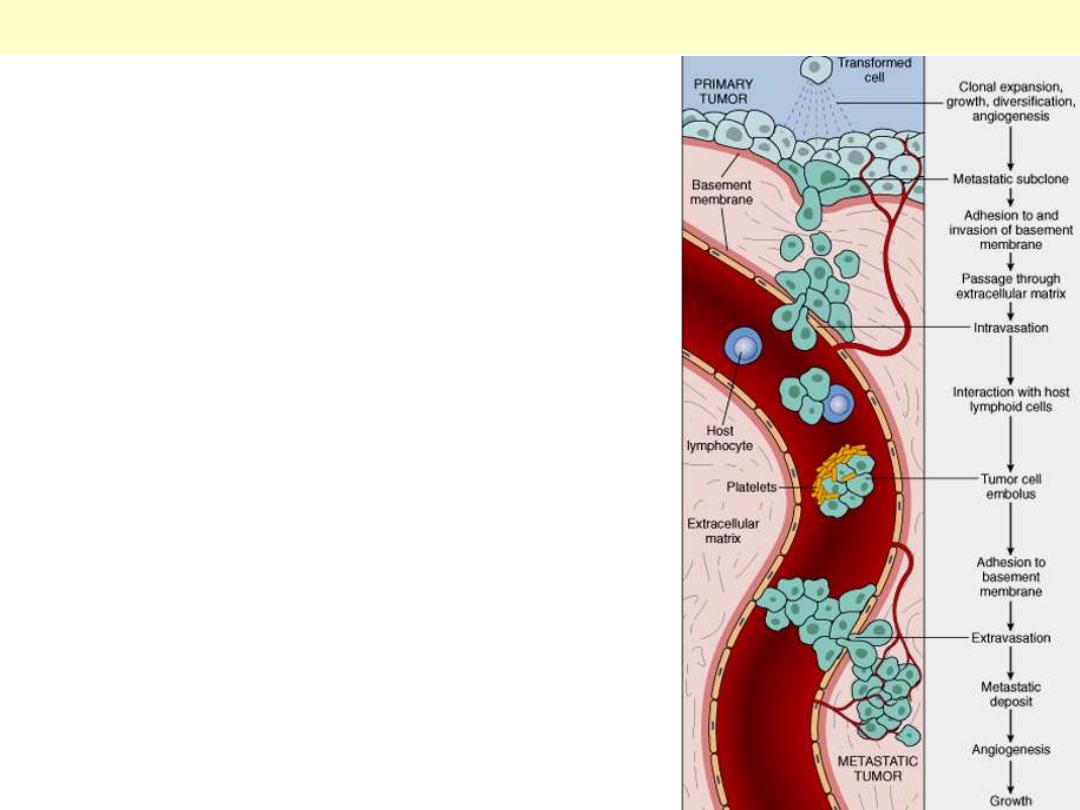
Schematic illustration of the sequential steps involved in
the hematogenous spread of a tumor.
The metastatic cascade

Nomenclature - Tumors

A 14-year-old male complained of pain of his Lt. knee joint. A radiograph was taken
to the joint. It showed an abnormality of upper metaphysis of the tibia. Describe.*
This is an osteochondroma of bone. This lesion appears as a bony projection (exostosis). Most are solitary,
incidental lesions that may be excised if they cause local pain. There is a rare condition of multiple
osteochondromatosis marked by bone deformity and by a greater propensity for development of chondrosarcoma.
This is another example of the
same tumor, but excised from a rib.
In what way it differs from the
previous lesion?*
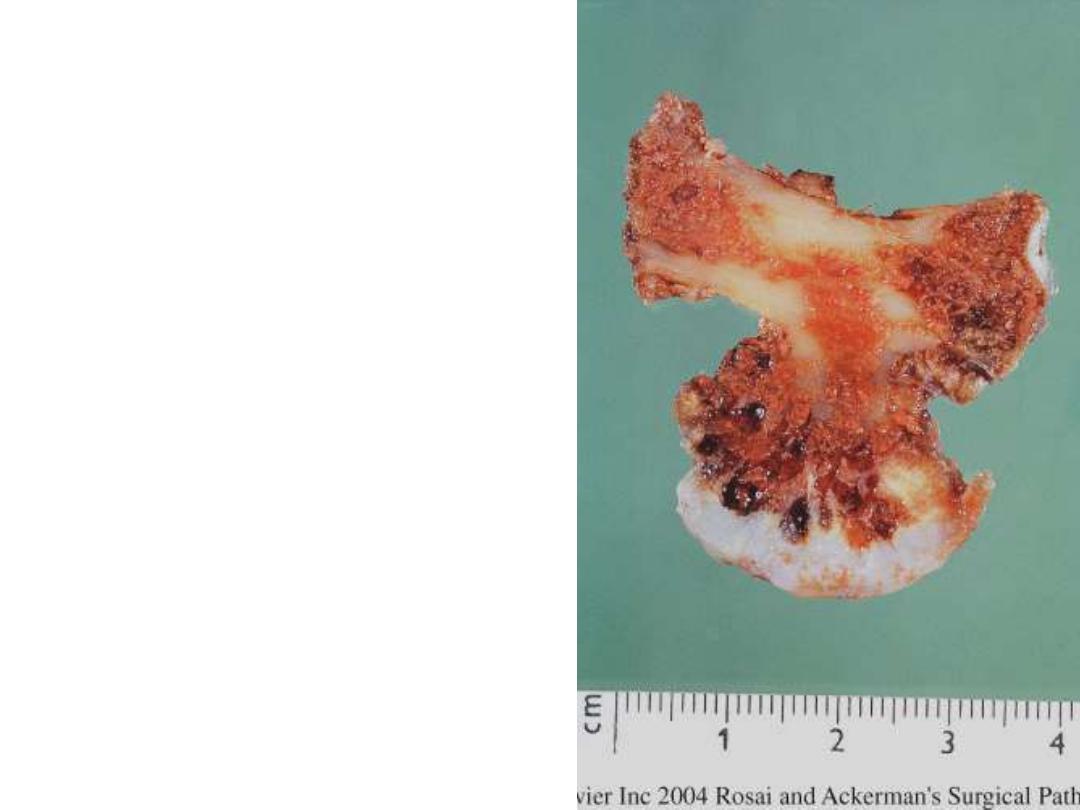
Cut surface of osteochondroma of rib. Note the thick
cartilaginous cup
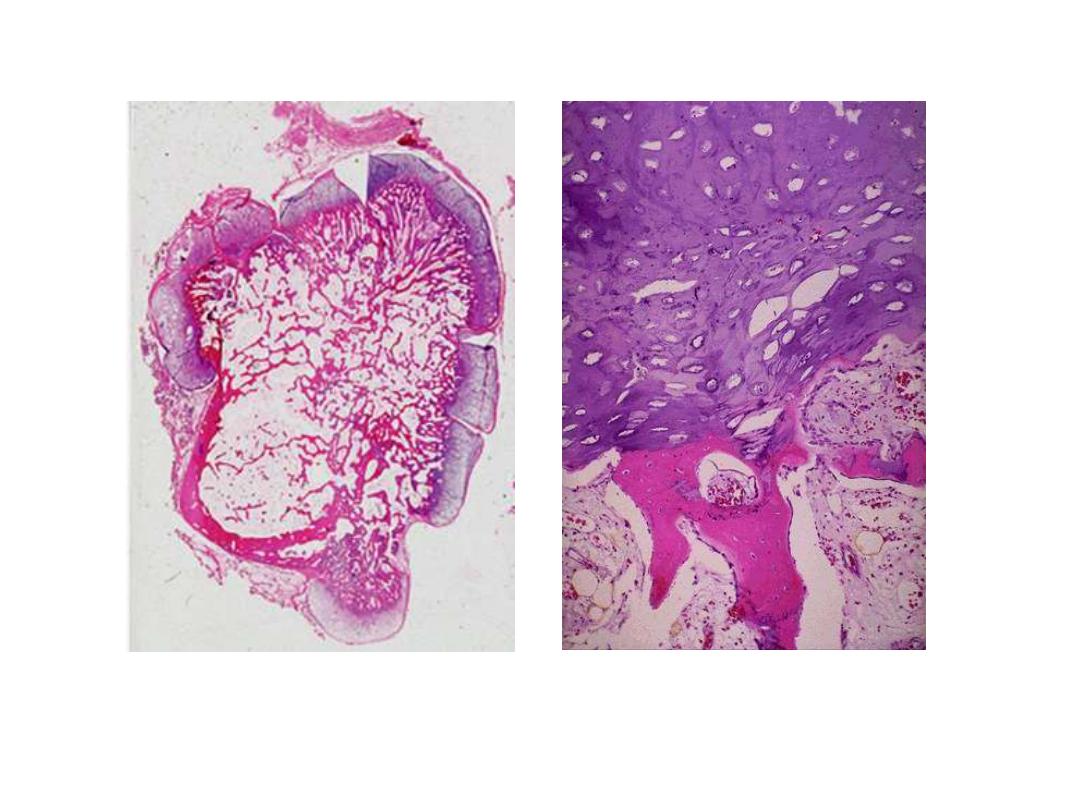
whole-mount appearance of the lesion on the Lt and HP view of the
surface on the Rt. Describe. What you call this lesion?
whole-mount appearance of osteochondroma. Mature bone is covered by a well-differentiated cartilaginous
cap
The tumor has lobules of benign-looking
chondrocytes
Chondroma
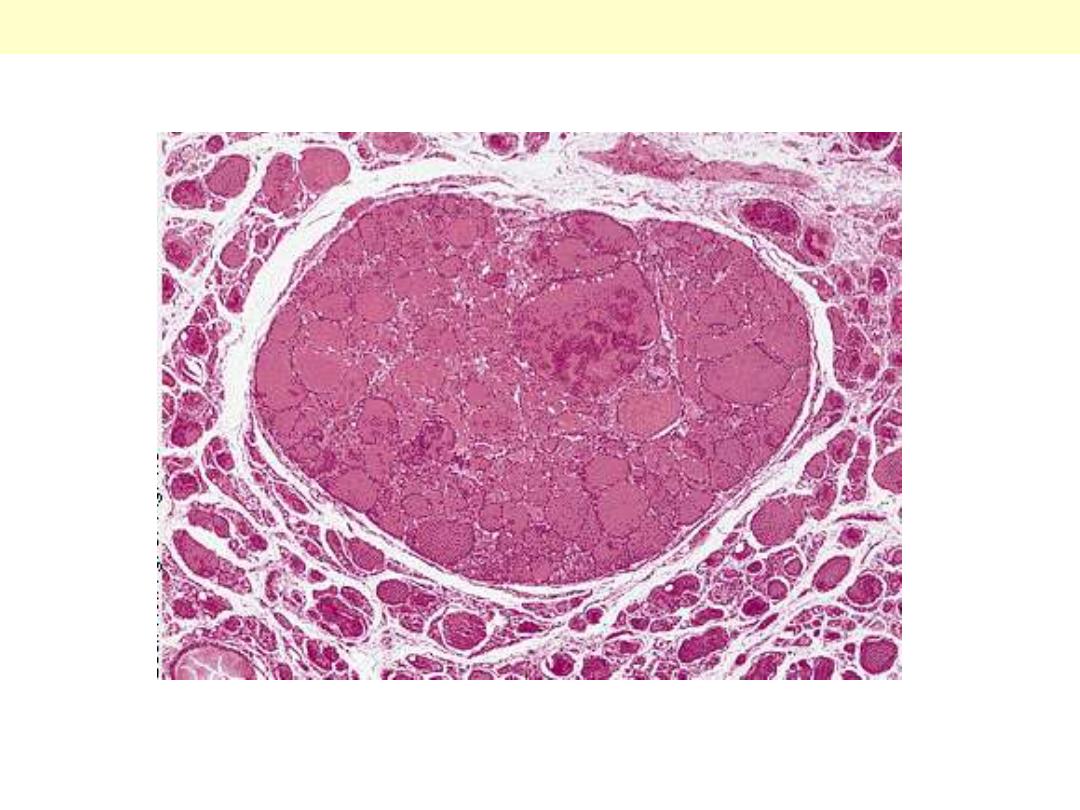
A small, well-defined proliferation of colloid-filled, thyroid-like follicles separated from the normal
tissue by a thin fibrotic capsule.
Follicular adenoma thyroid
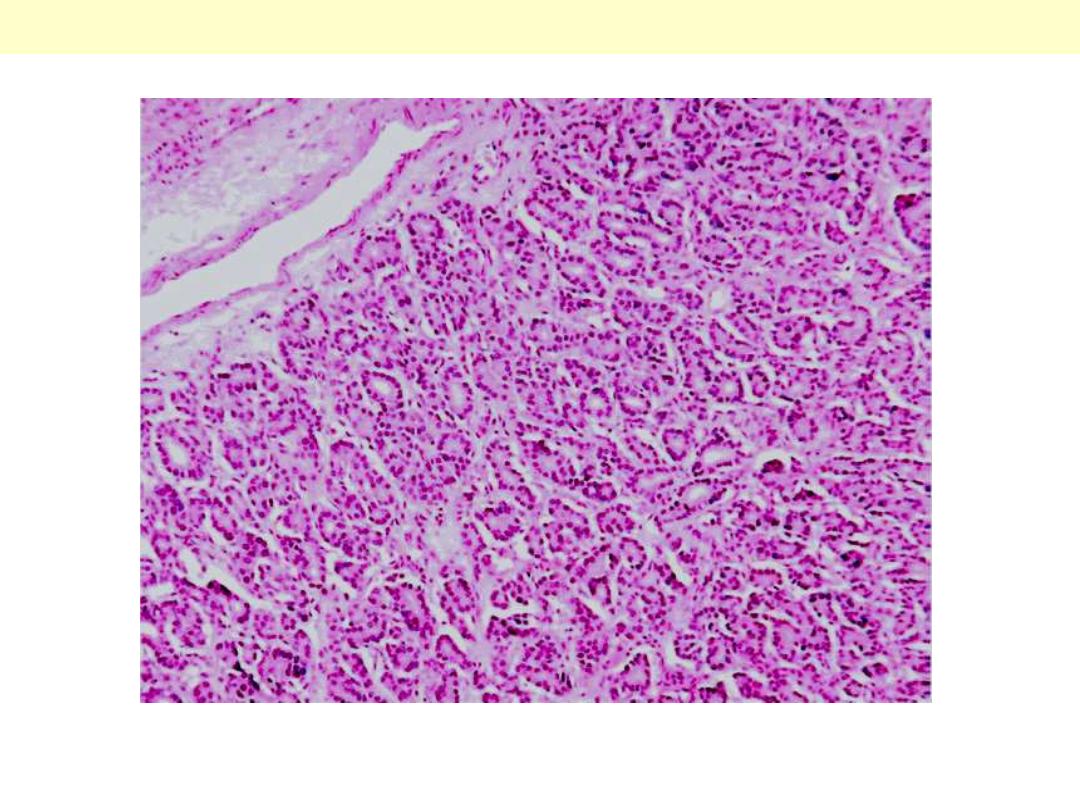
A portion of another follicular adenoma consisting of small (micro) follicles.
Follicular adenoma thyroid
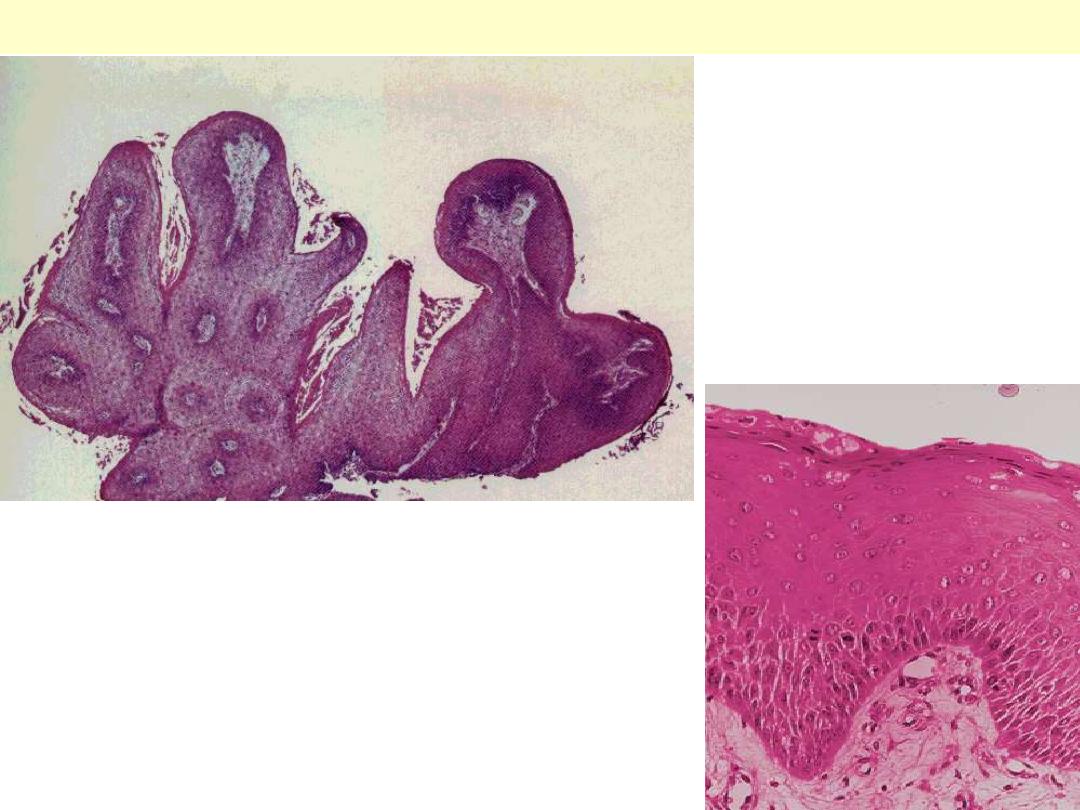
This multilayered benign-looking squamous epithelium is
arranged in a finger-like projections, each having a core of
vascularized connective tissue. The Rt. Photo is a higher power
showing the squamous epithelium cover of one of the papillae.
Squamous cell papilloma larynx
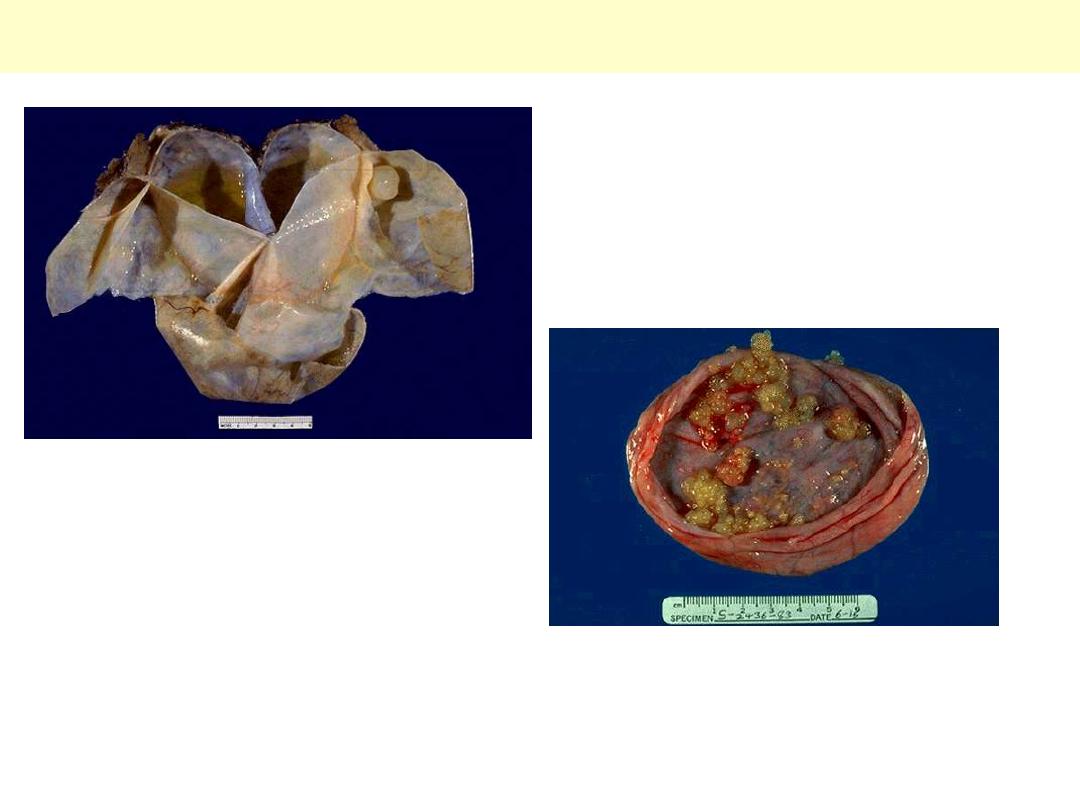
Ovarian cystadenoma and papillary cystadenoma
Lt, a cystadenoma seen as a unilocular, thin-
walled cyst with smooth inner & outer surfaces.
Rt, papillary cystadenoma having similar gross
features to cystadenoma except for the presence of
multiple yellowish, warty projections sprouting
from the inner surface.
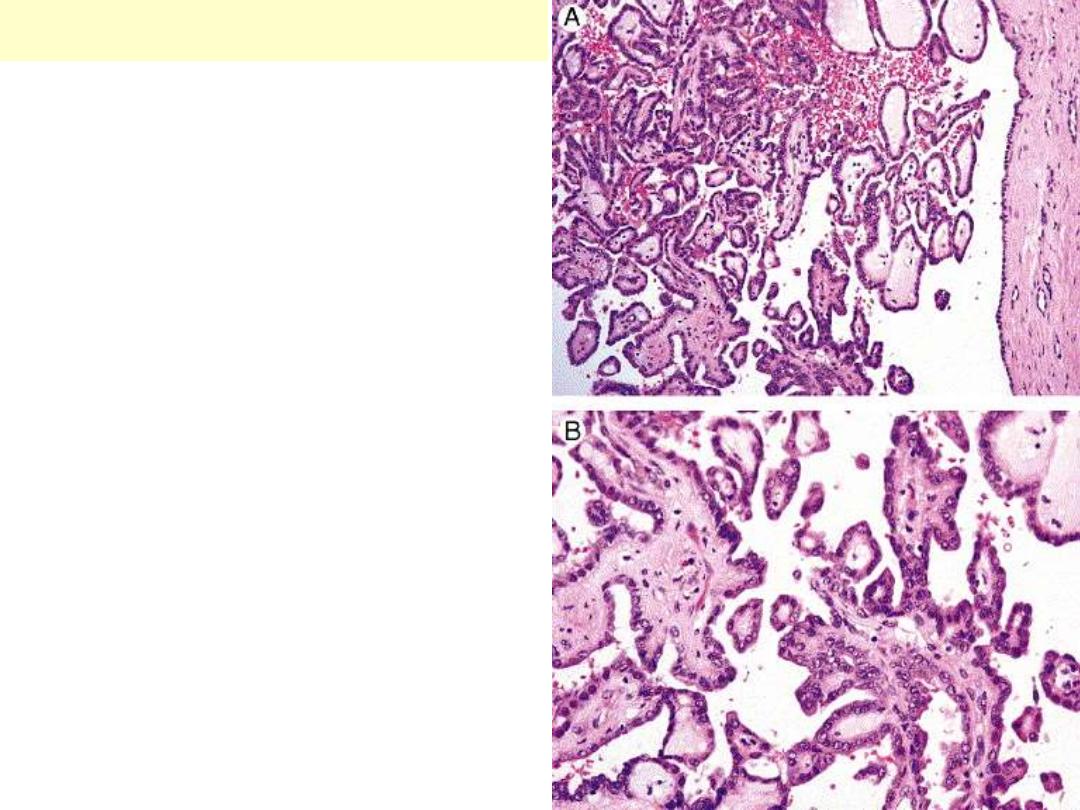
Papillary cystadenoma
A histological section taken from one of the warty
projections showing papillary (finger-like)
projections each composed of vascularized
connective tissue core covered by benign-looking
epithelial cells. The lower photo is a higher
magnification of the upper.
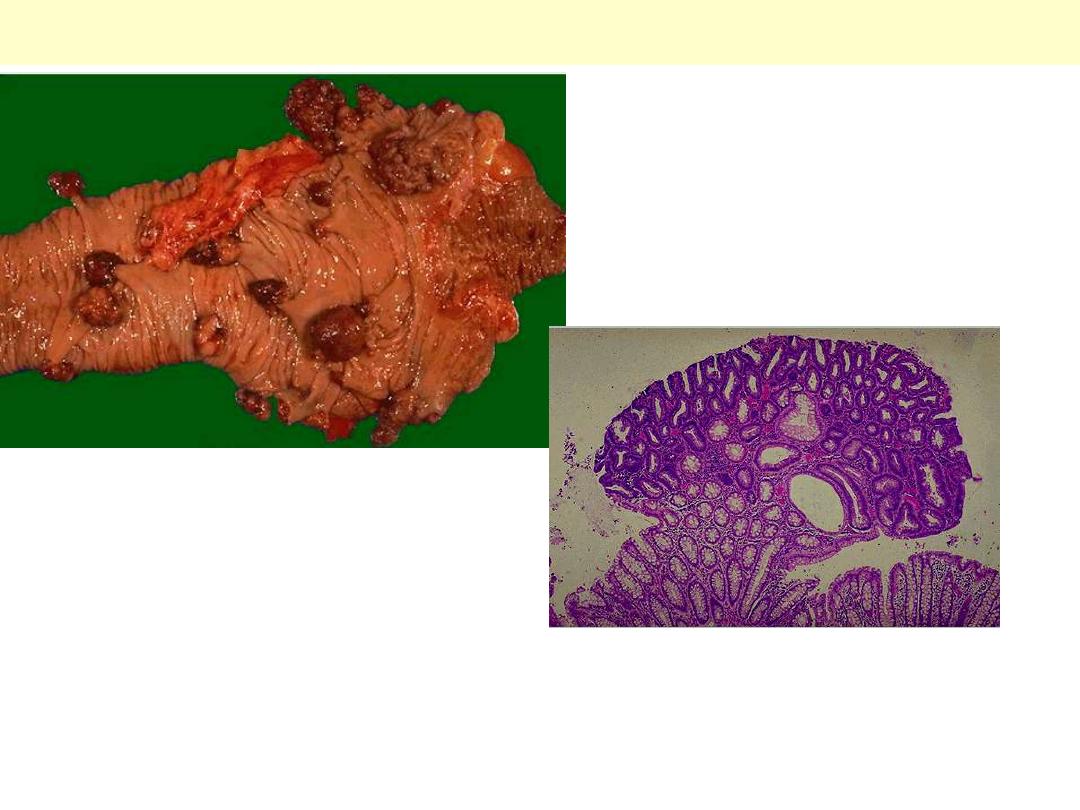
Adenomatous polyps large intestine
Lt. upper, a segment of large intestine opened
longitudinally to display multiple pale to
brownish, variably-sized polyps. These arise
from the mucosa.
Rt. Lower, a microscopic sections of one of the
polyps showing closely packed, glandular
structures that appear more densely staining
than the native crypts. This is by definition an
adenomatous polyp.

MIXED PAROTID TUMOR (Pleomorphic Adenoma)
Two clinical examples of parotid pleomorphic adenomas. These tumors classically present as
preauricular swelling. In the early stages the tumor is small but it may progressively increase in size if
left untreated. The Rt. Photo is an usually large pleomorphic adenoma. The only way of establishing
the diagnosis & excluding malignancy is through microscopic examination of sections from the excised
tumor. This has revealed features of pleomorphic adenoma in these two examples.

MIXED PAROTID TUMOR
(pleomorphic adenoma)
A well-defined pleomorphic
adenoma arsing from the
parotid. A residual native
salivary tissue is present to the
Rt. of the tumor. The tumor is
soild with predominantly
greyish-white color. The glisteing
nodules with bluish hue
represent foci of cartilage.
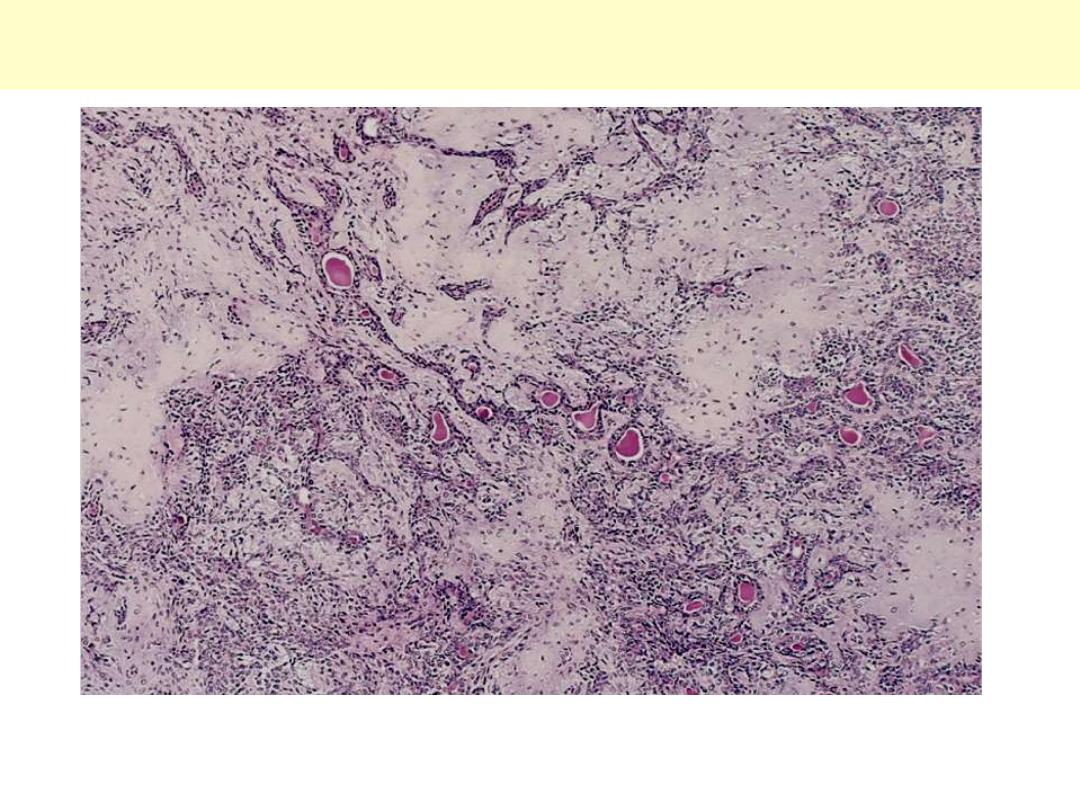
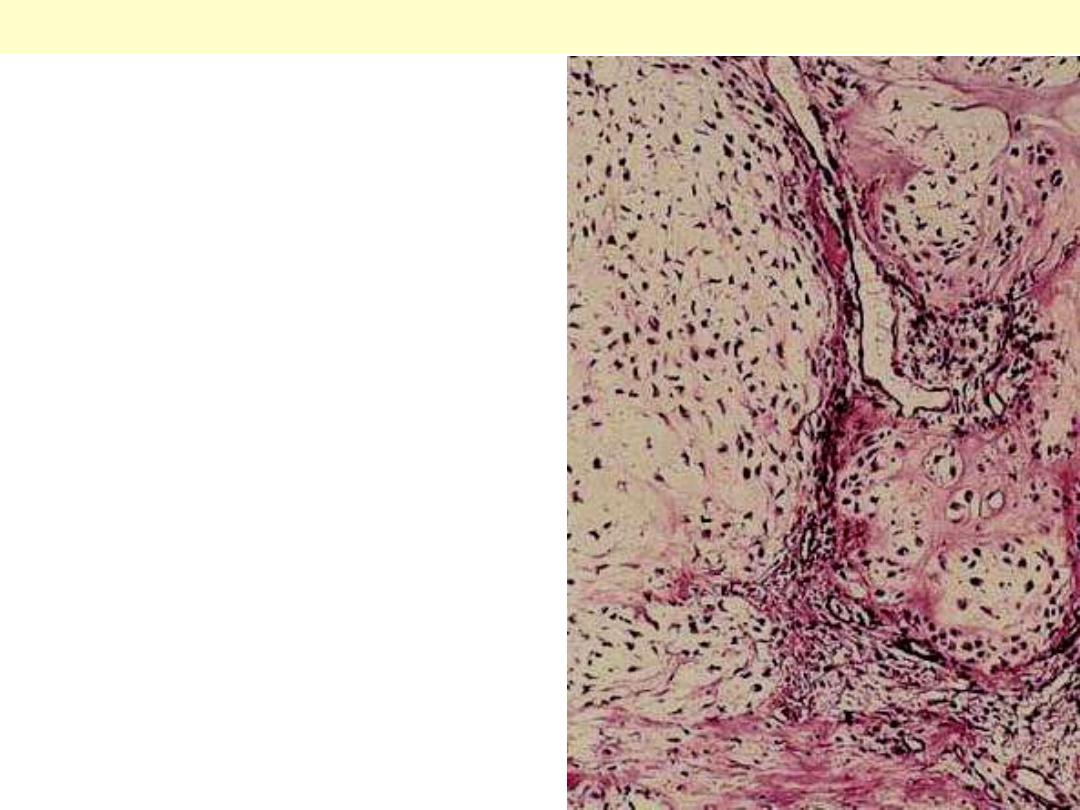
Mixed salivary gland tumor (Pleomorphic adenoma)
Sheets of epithelial/myoepithelial cells with glandular arrangement. There are several nodules of
cartilaginous tissue composed of chrondrocytes within a bluish background. The capsule of the tumor
is to the Lt.
Mixed salivary gland tumor (Pleomorphic adenoma)
Within a sheet of myoepithelial cells there are nests of squamous differentiation having central
laminated keratin.

Ovarian Cystic Teratoma (Dermoid cyst)
These cysts are typically filled with sebum (secretion of sebaceous glands) & hair.

Ovarian Cystic Teratoma (Dermoid cyst)
Well-developed teeth in ovarian mature cystic teratoma.
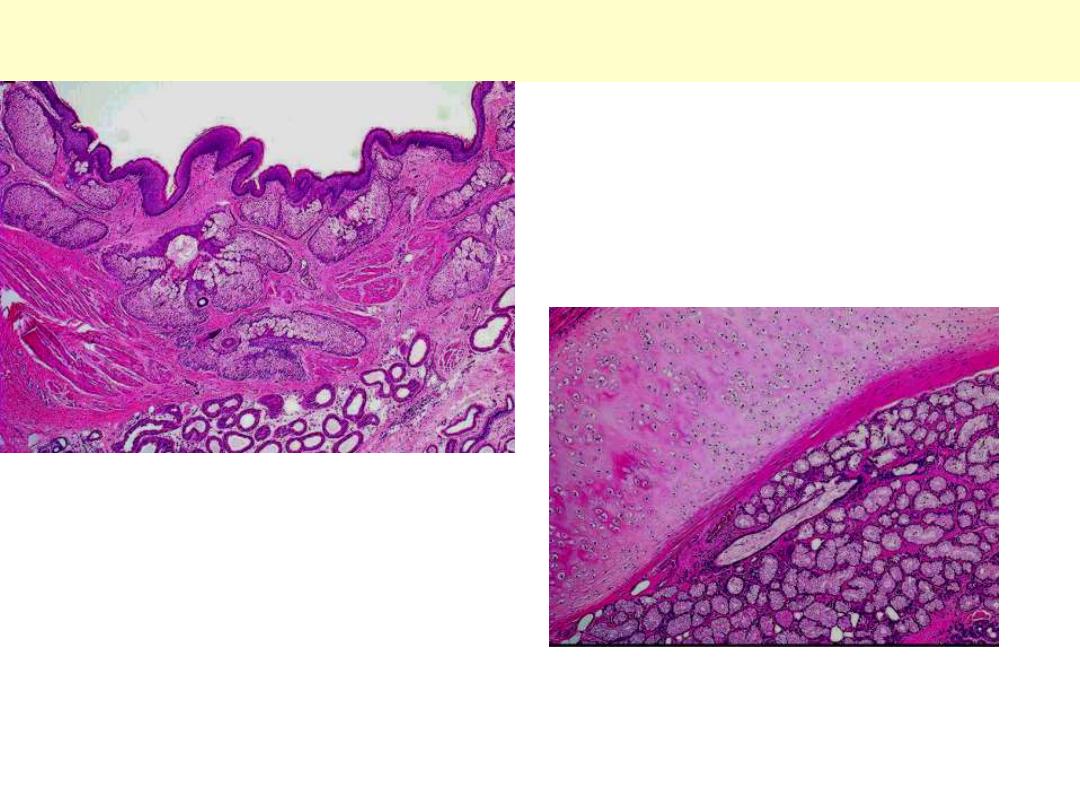
Cystic teratoma ovary
Upper, skin & its adnexae (hair follicles with
related sebaceous glands & sweat glands)
Lower, part of a bronchial wall showing a plate of
cartilage & mucus secreting glands.

Staging – TNM
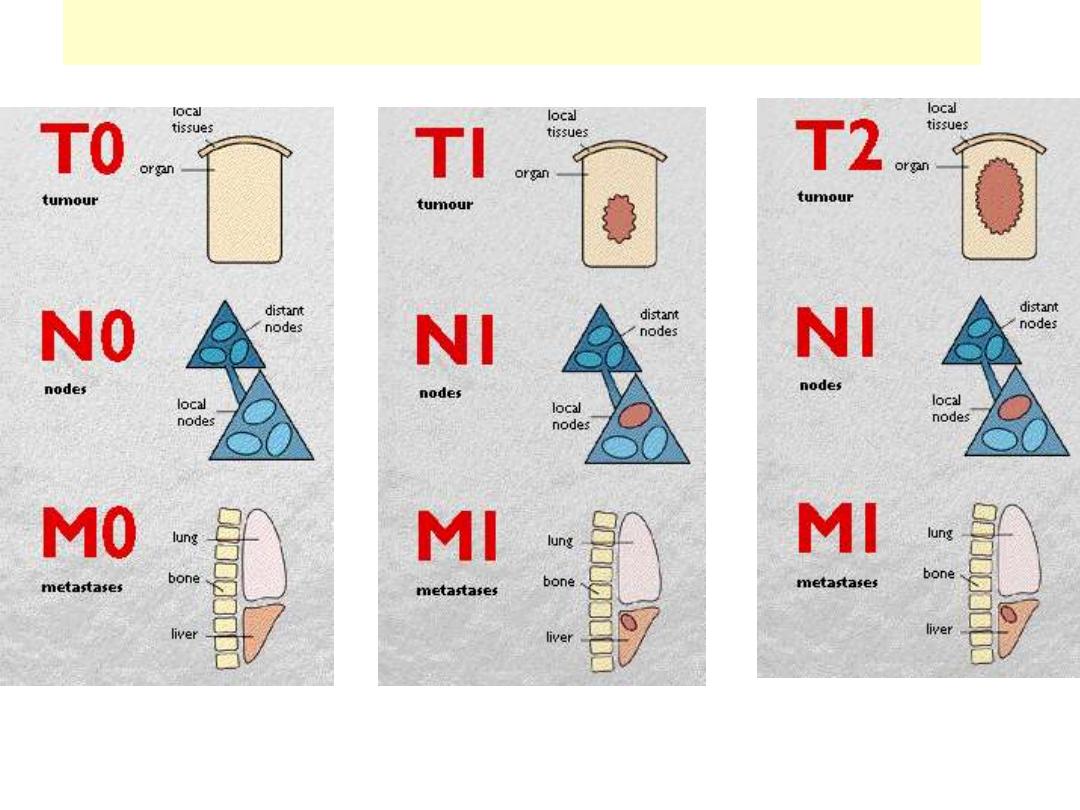
TNM staging for ca breast

Tumor growth - Biology
Biology of tumor growth and evolution
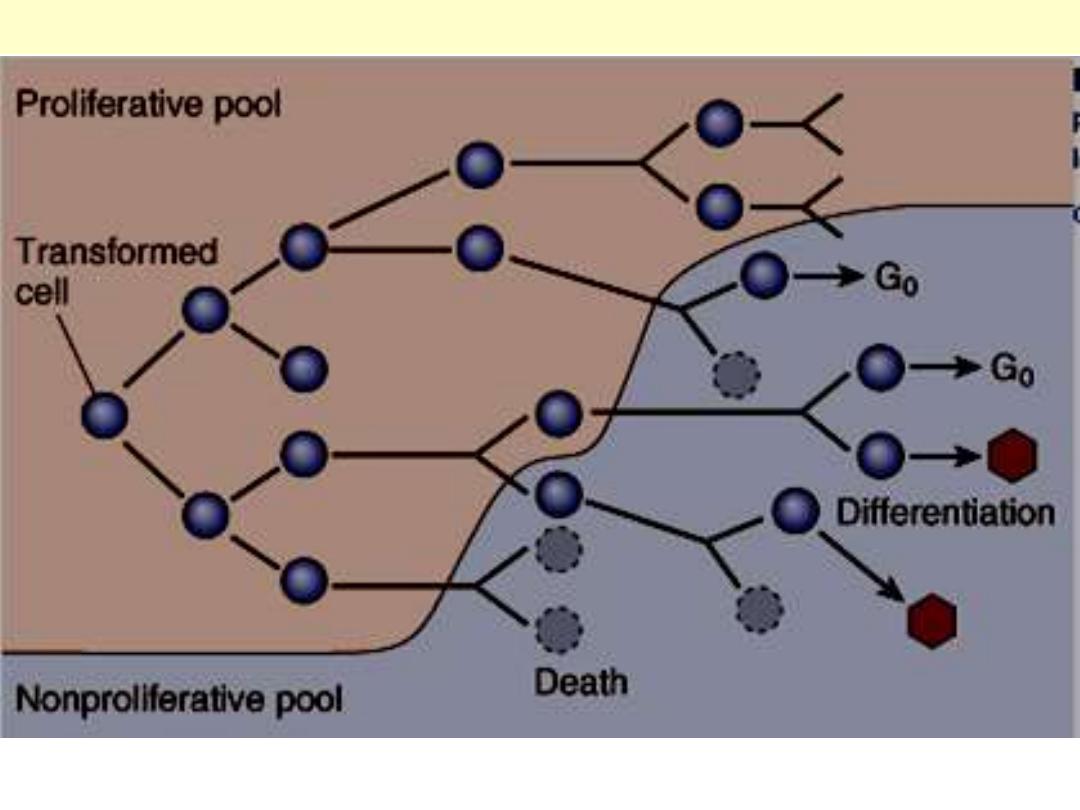
As the cell population expands, a progressive higher percentage of tumor cells leaves the replicative
pool by reversion to G
0
, differentiation and death.
Schematic representation of tumor growth