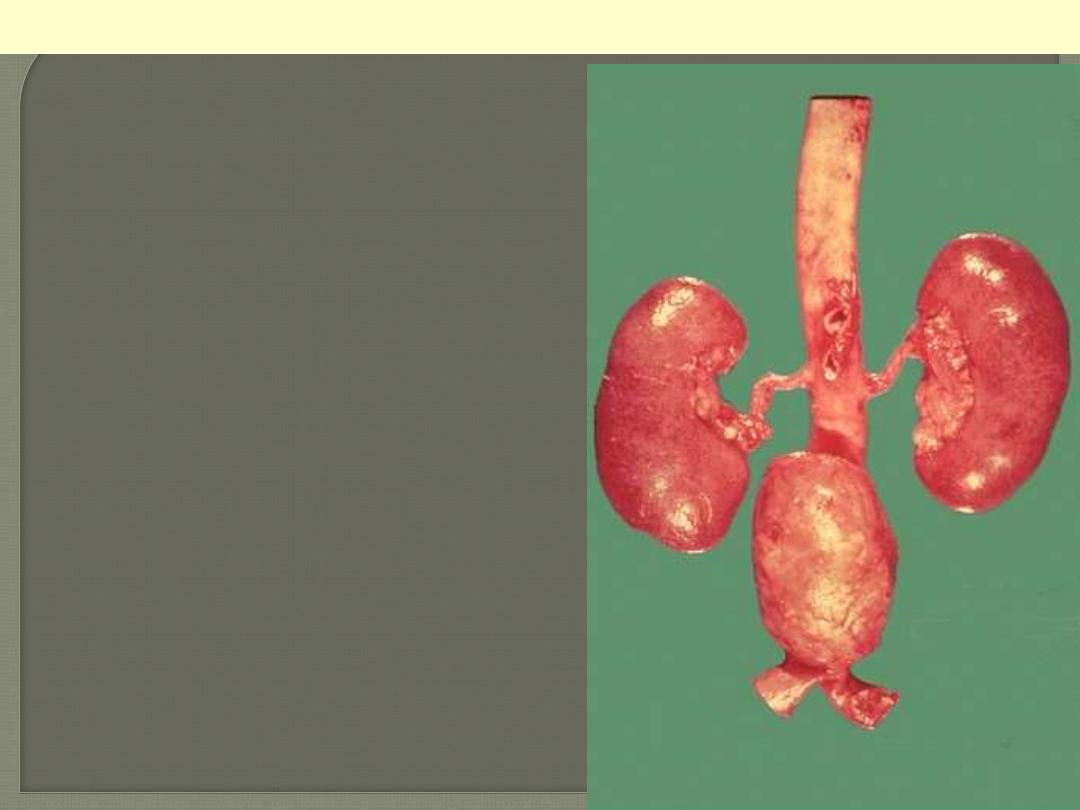
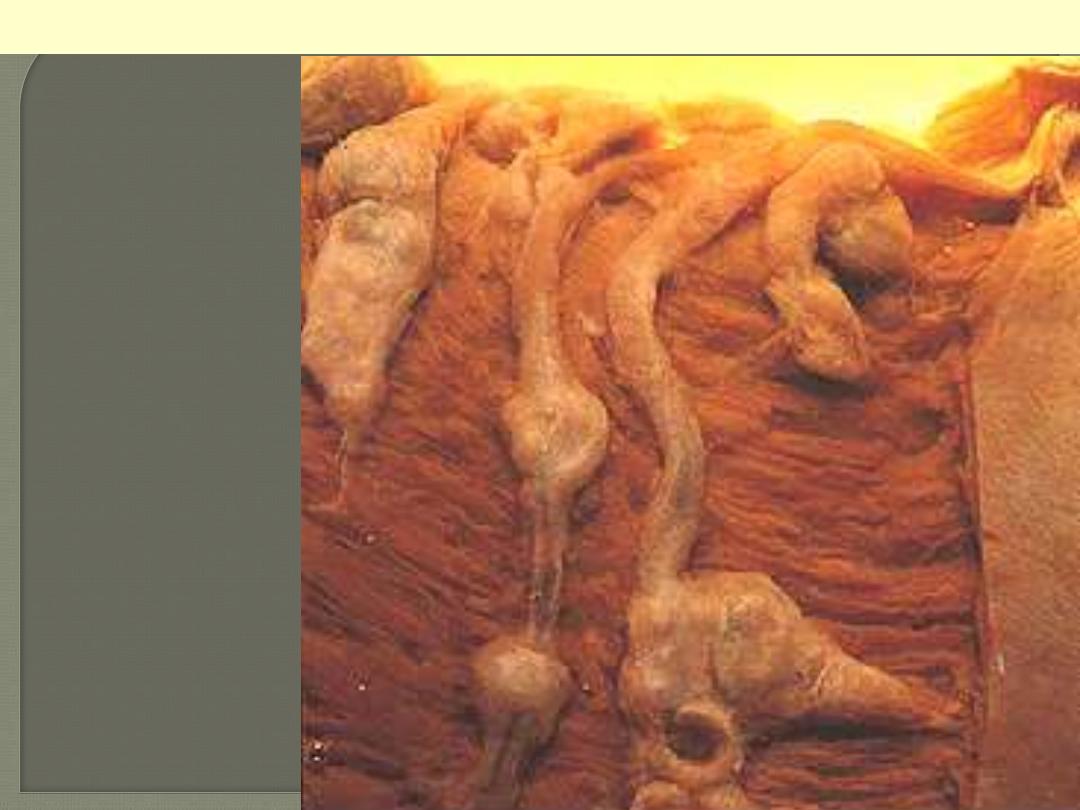
A large "bulge" appears just above the aortic
bifurcation. Such aneurysms are prone to rupture
when they reach about 6 to 7 cm in size. They may be
felt on physical examination as a pulsatile mass in the
abdomen. Most such aneurysms are located below the
renal arteries so that surgical resection can be
performed with placement of a dacron graft.
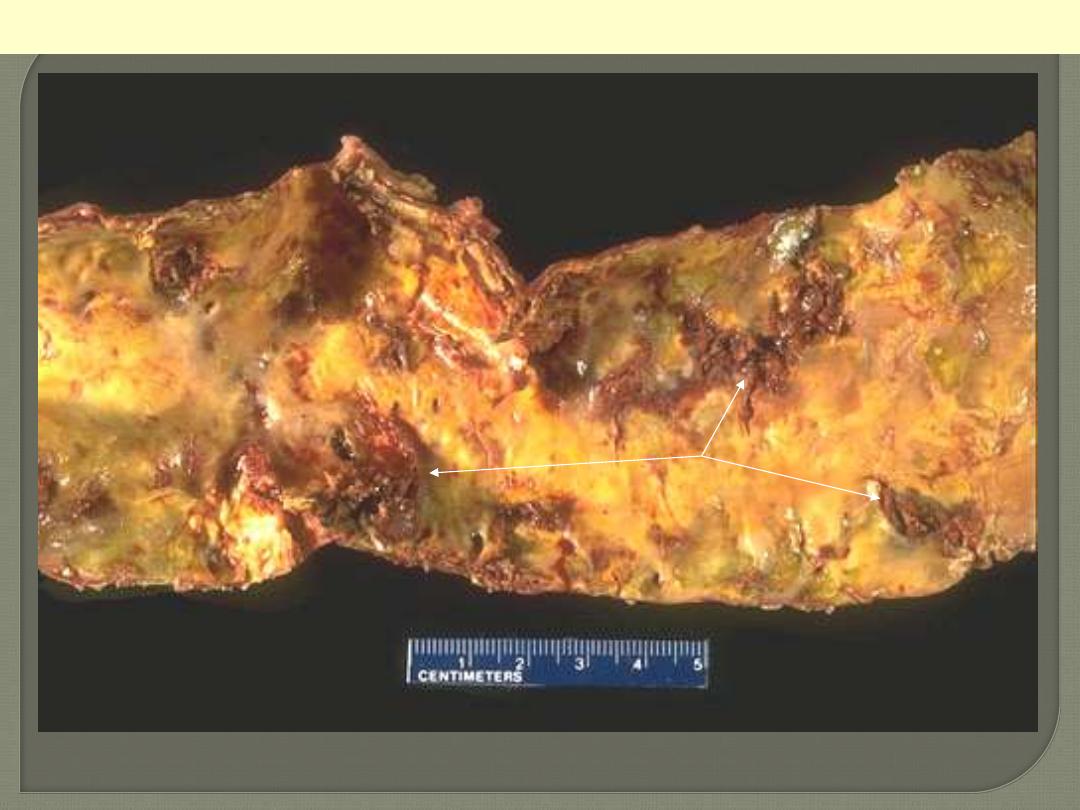
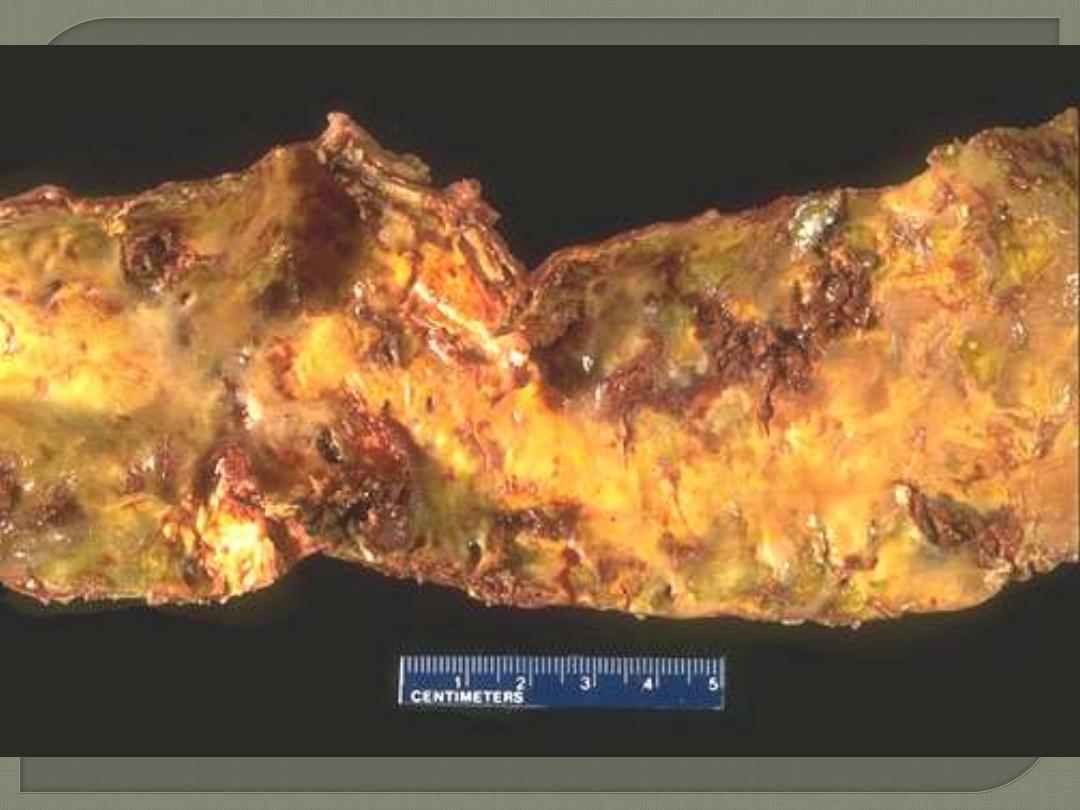
Atherosclerotic aneurysm of the abdominal aorta
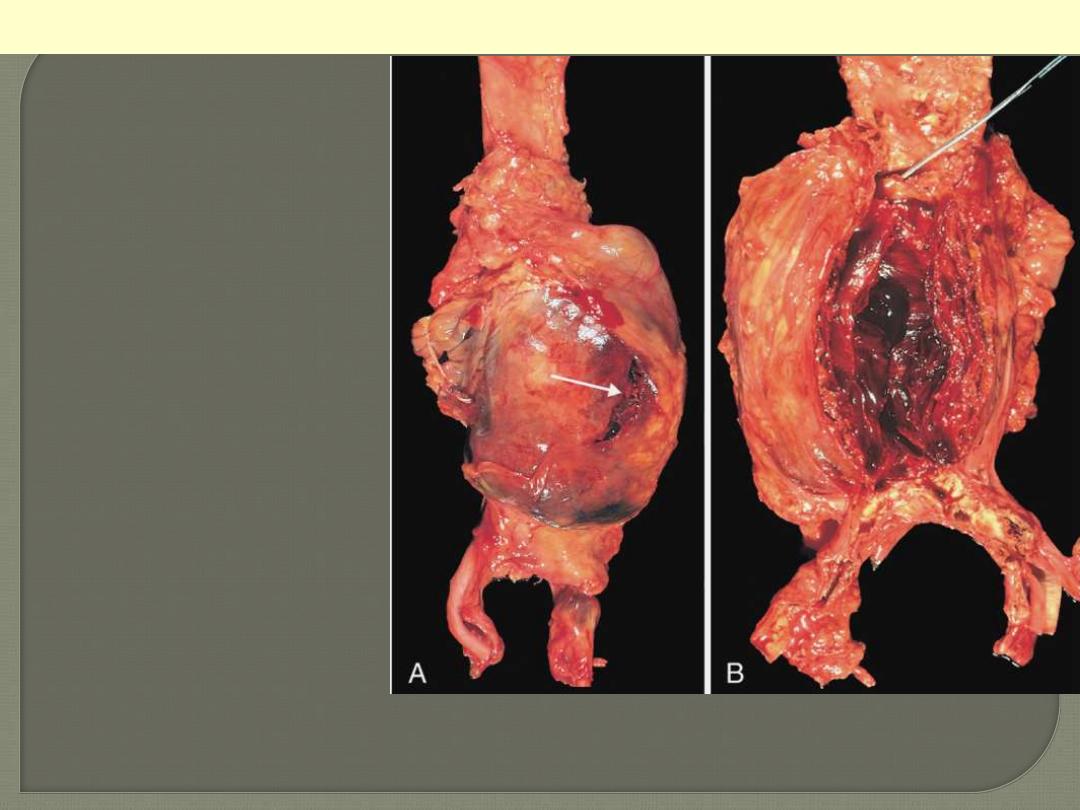
A, External view, gross
photograph of a large aortic
aneurysm that ruptured (arrow).
B, Opened view, with the location
of the rupture tract indicated by
a probe. The wall of the
aneurysm is exceedingly thin, and
the lumen is filled by a large
quantity of layered but largely
unorganized thrombus.
Abdominal aortic aneurysm
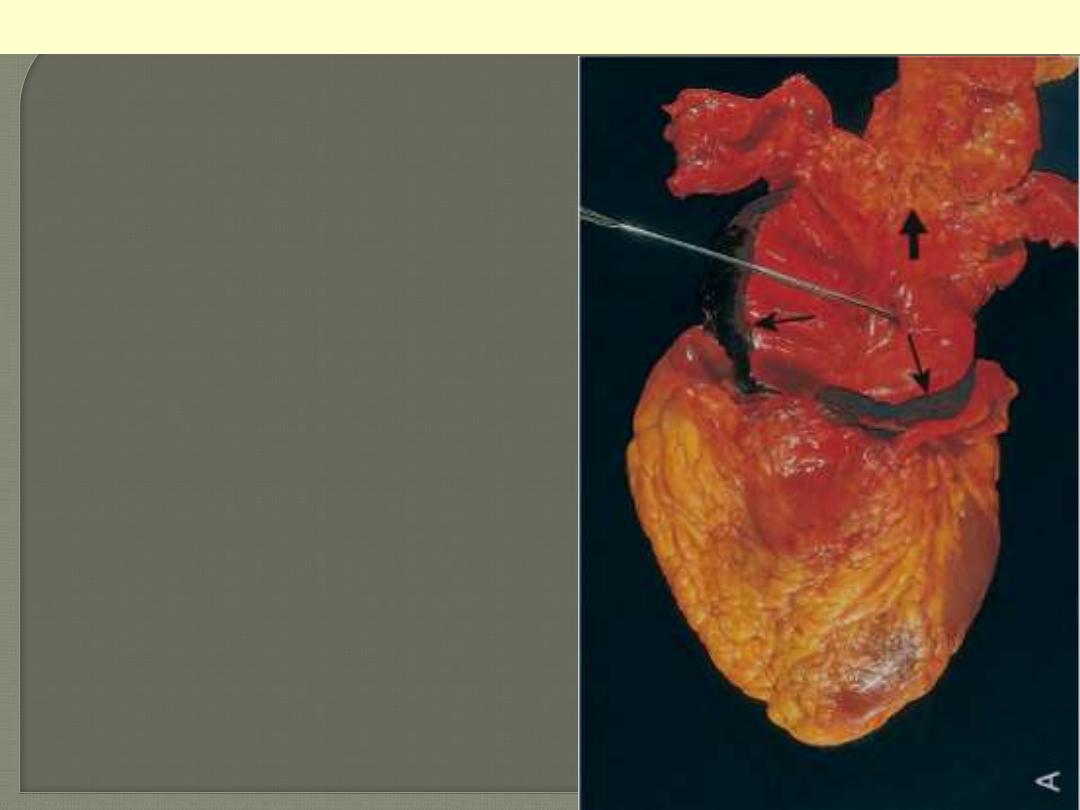
an opened aorta with proximal dissection originating
from a small, oblique intimal tear (identified by the
probe), allowing blood to enter the media and create
an intramural hematoma (narrow arrows). Note that
the intimal tear has occurred in a region largely free
of atherosclerotic plaque and that propagation of the
intramural hematoma is arrested at a site more
distally where atherosclerosis begins (broad arrow).
Aortic dissection
The dissection goes into the muscular wall creating an aorta with double lumina.
Aortic dissection
Original lumen
Dissection
Circle of Willis with anterior, middle and posterior
cerebral arteries linked by communicating vessels.
Berry aneurysms are seen arising where the internal
carotid bifurcates into middle and anterior cerebral
arteries (arrow).
Berry aneurysms
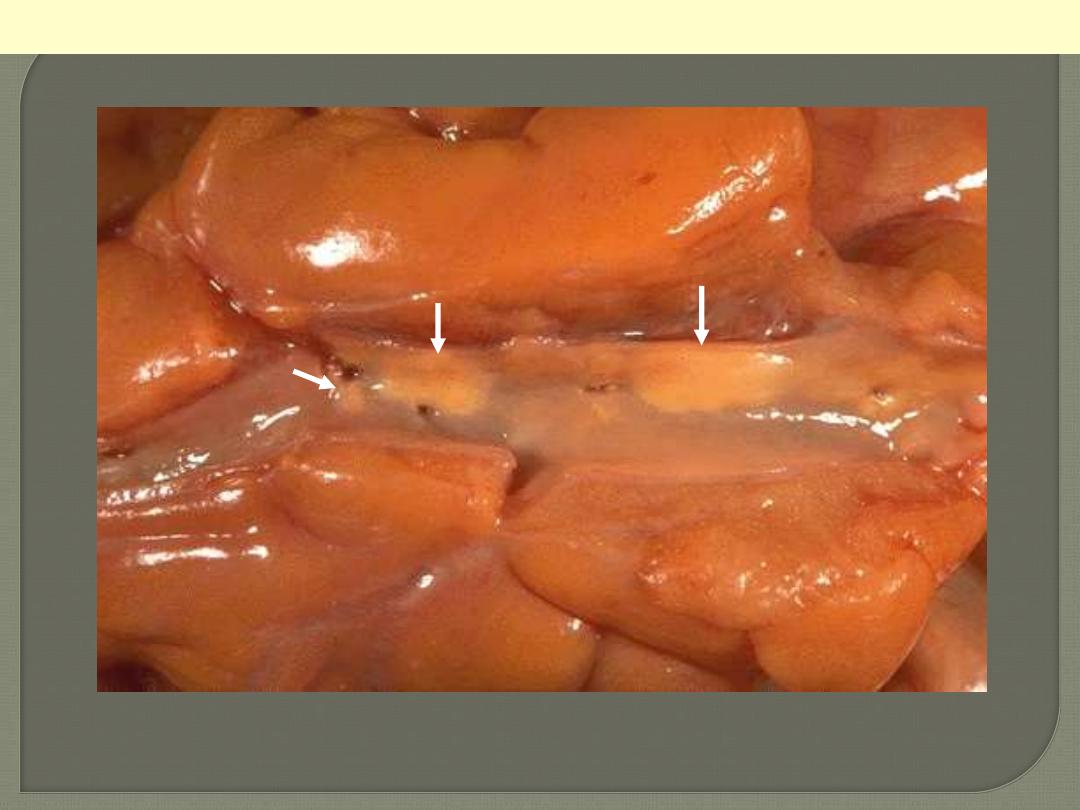
A coronary artery has been opened longitudinally. The coronary extends from left to right across the
middle of the picture and is surrounded by epicardial fat. This coronary shows only mild
atherosclerosis, with only an occasional yellow-tan lipid plaques (arrows) and no narrowing.
Mild degree of coronary athersclerosis
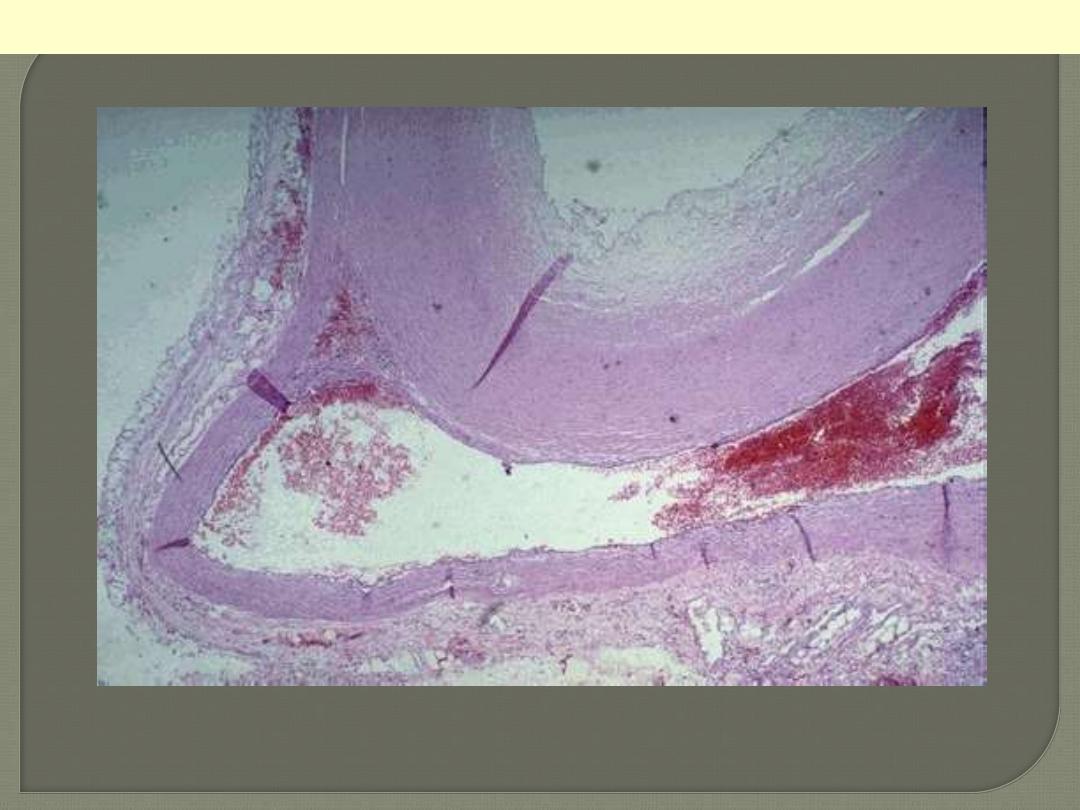
The lumen of the artery is at the top right corner, and the band of smooth muscle at the bottom is the
atrophic media. The intima is enormously thickened, by the presence deep in it (centre and left) of
amorphous material containing large numbers of cholesterol crystals (the unstained clefts). There are
many foamy (lipid-filled) macrophages and chronic inflammatory cells in this zone and also in the
thick layer of dense fibrous tissue layer (arrow) which separates it from the lumen.
Coronary artery atheromatous plaque: (HE) medium power
Media
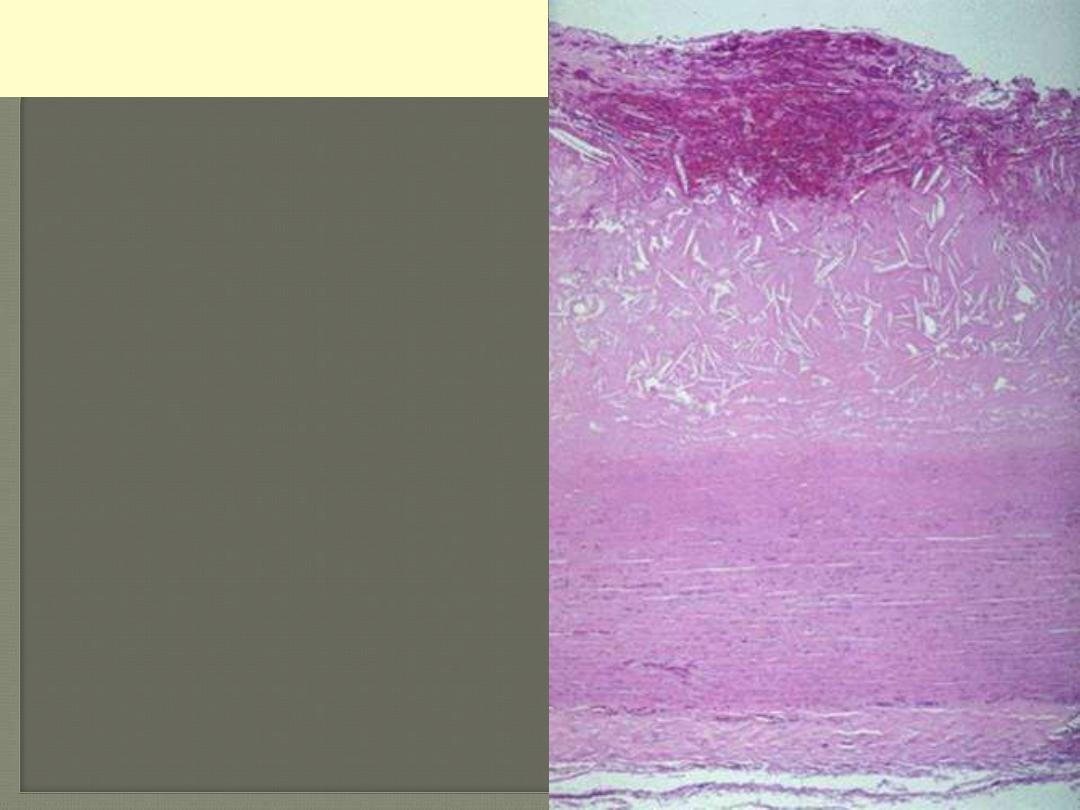
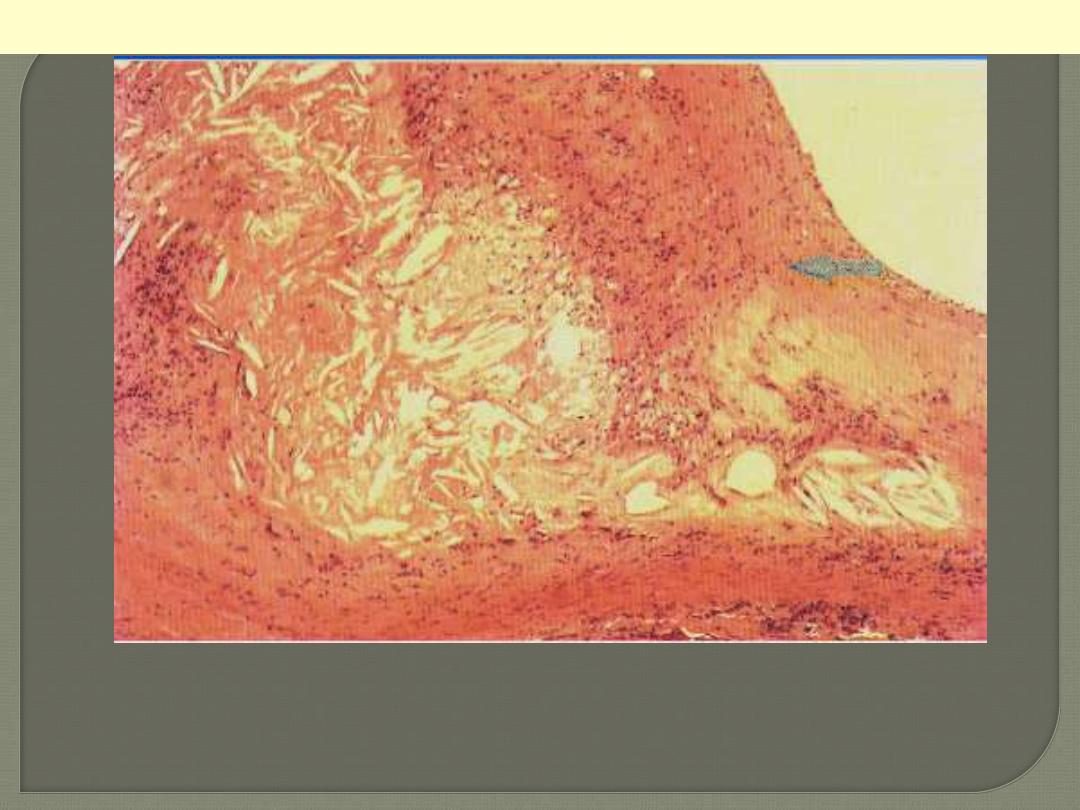
This microscopic cross section of the aorta shows
a large luminal atheroma. Cholesterol clefts are
numerous in this atheroma. The surface shows
intraplaque hemorrhage.
Aorta: atheromatous plaque with
hemorrhage. (HE) low power
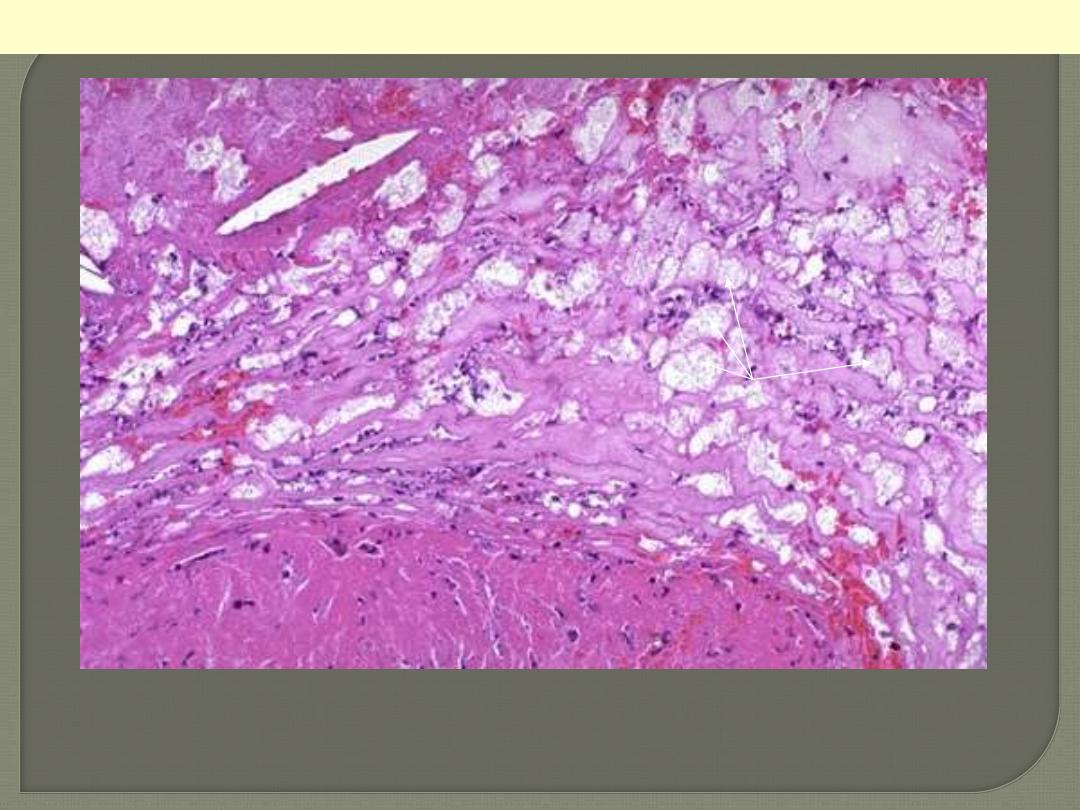
This high magnification of an atheroma shows numerous foam cells (arrows) and an occasional
cholesterol cleft. A few dark blue inflammatory cells are scattered within the atheroma.
Atheromatous plaque. (HE) High power
Media
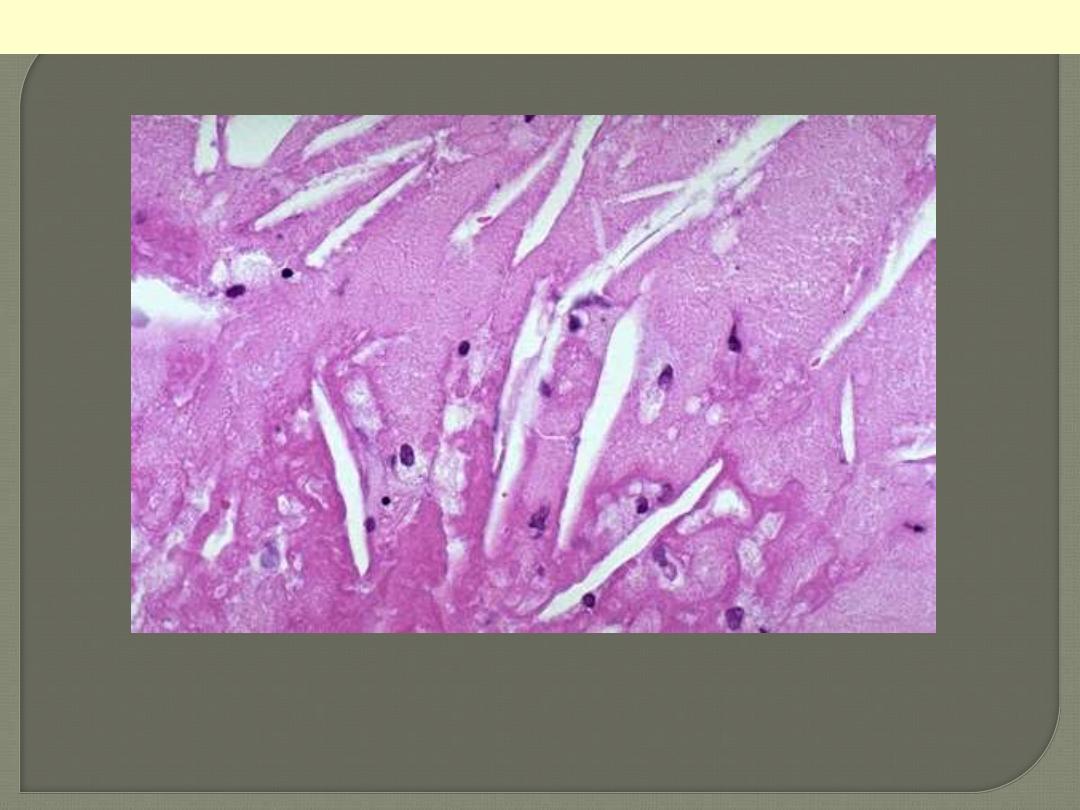
Atheromatous plaque. (HE) High power
This is a high magnification of an atheroma with foam cells and cholesterol clefts.

These three aortas demonstrate mild, moderate, and severe atherosclerosis from bottom to top. At the
bottom, the mild atherosclerosis shows only scattered lipid plaques (arrows). The aorta in the middle
shows many more larger whitish plaques. The severe atherosclerosis in the aorta at the top shows
extensive ulceration in the plaques (arrows).
Atherosclerosis aorta
This is severe atherosclerosis of the aorta in which the atheromatous plaques have undergone
ulceration along with formation of overlying mural thrombus (arrows).
Atherosclerosis aorta: ulcerations with superadded thrombosis

This is coronary atherosclerosis with the complication of hemorrhage into atheromatous plaque
(arrow). Such hemorrhage acutely may narrow the arterial lumen.
Coronary atherosclerosis: plaque hemorrhage

There is a severe degree of narrowing in this coronary artery. It is "complex" in that there is a large
area of calcification on the lower right, which appears bluish on this H&E stain. Complex atheroma
have calcification, thrombosis, or hemorrhage. Such calcification would make coronary angioplasty
difficult.
Stenosing coronary atheroma with calcification

Lt. the anterior descending coronary (opened longitudinally) to show severe stenosing atherosclerosis
with superimposed reddish thrombosis with its propagating portion filling the minimally narrowed
proximal portion. Lt. A closer view showing the artery cross section, which totally occluded by the
reddish thrombus. the dark red thrombus is apparent in the lumen of the coronary.
Coronary atherosclerosis with superimposed thrombosis

There is a pink to red recent thrombosis in this narrowed coronary artery. The open, needle-like spaces
in the atheromatous plaque are cholesterol clefts.
Coronary atherosclerosis with superimposed occlusive thrombosis
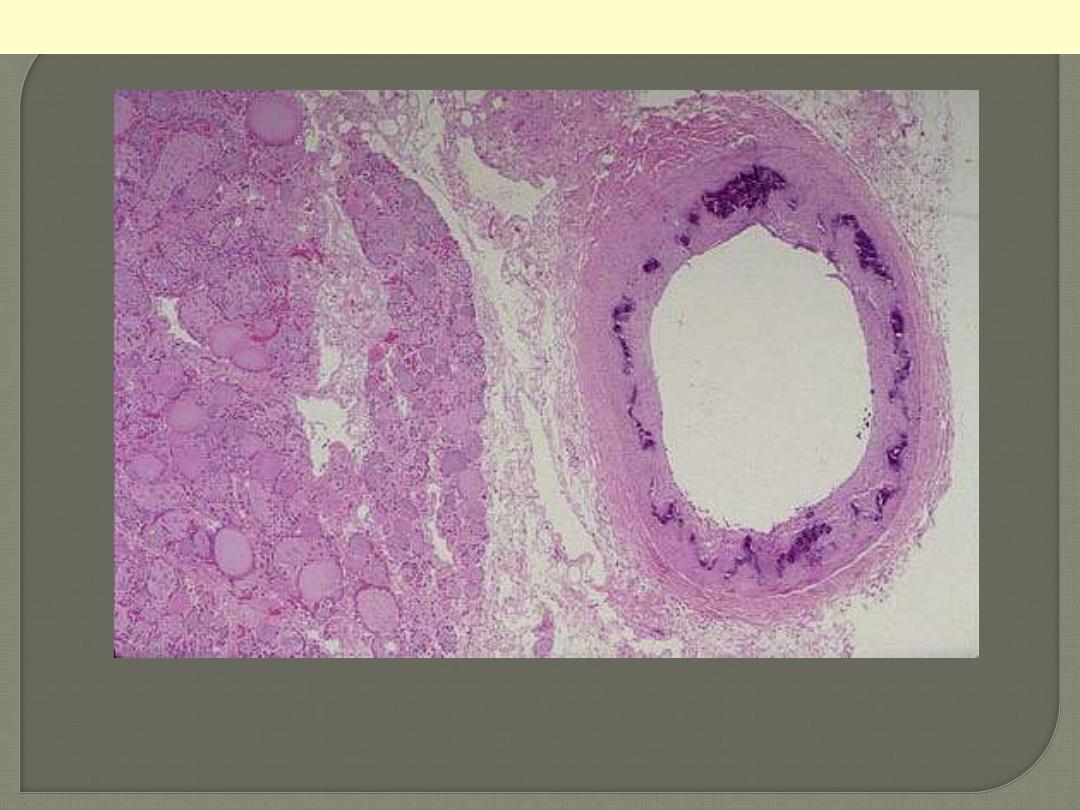
Ring-like calcification (blue color) seen affecting the media of this artery to the right of thyroid tissue
at the left; there is no luminal narrowing. This finding occurs most often in the elderly and is of no
clinical significance, other than that the calcified arteries may be visualized on radiographs, and you
need to know what is represented.
Monckeberg's medial calcific sclerosis thyroid

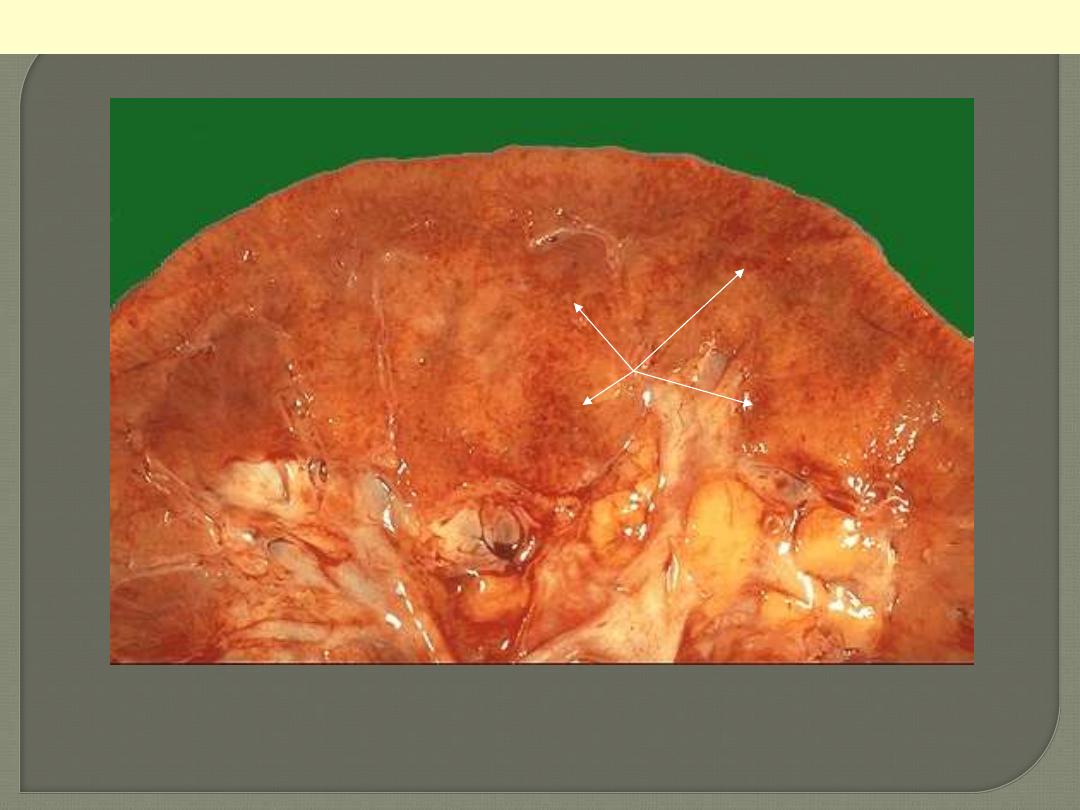
The smaller arterioles in the kidney have become
thickened and narrowed. This leads to patchy
ischemic atrophy with focal loss of parenchyma that
gives the surface of the kidney the characteristic
granular appearance as seen here.
Benign nephrosclerosis
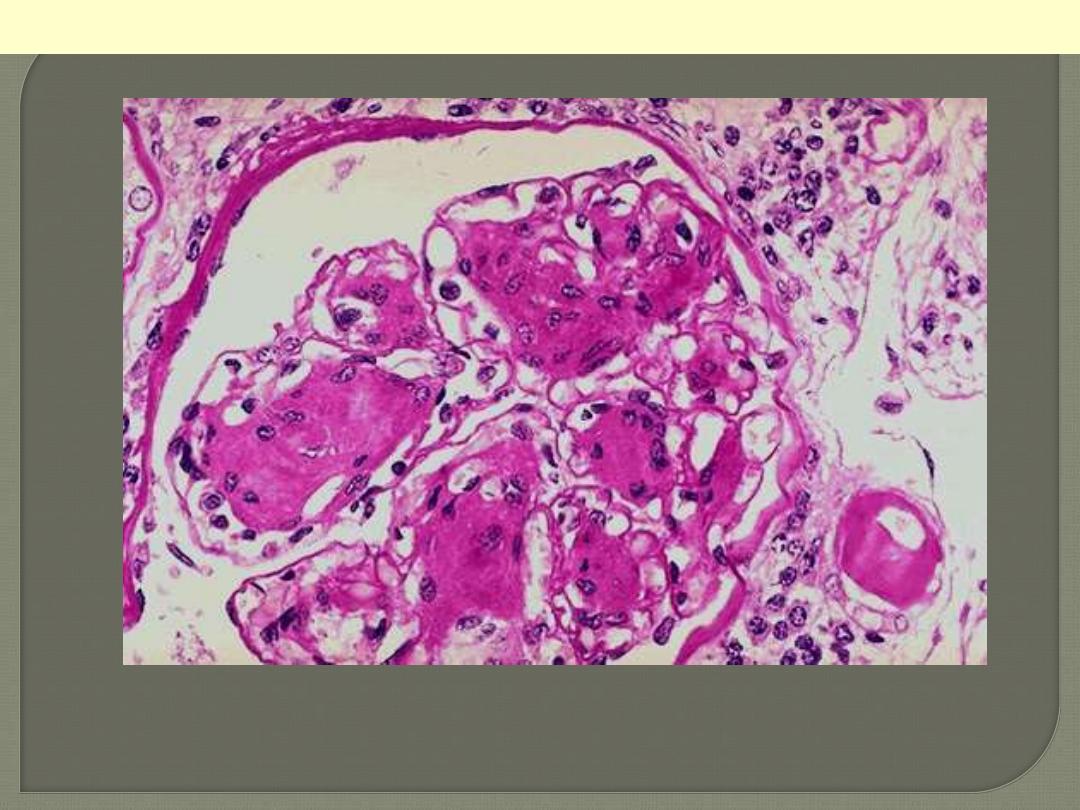
Arteriolosclerosis is typically seen in the kidneys. One form, called hyaline arteriolosclerosis, is
demonstrated by the markedly thickened arteriole to the lower right of this glomerulus with PAS stain.
Hyaline arteriolosclerosis is seen in the elderly, but more advanced lesions are seen in persons with
diabetes mellitus and/or with hypertension.
Hyaline arterioloscelrosis Kidney
In malignant nephrosclerosis, the kidney demonstrates focal small hemorrhages. This is due to an
accelerated phase of hypertension in which blood pressures are very high (such as 300/150 mm Hg).
Malignant neophrosclerosis
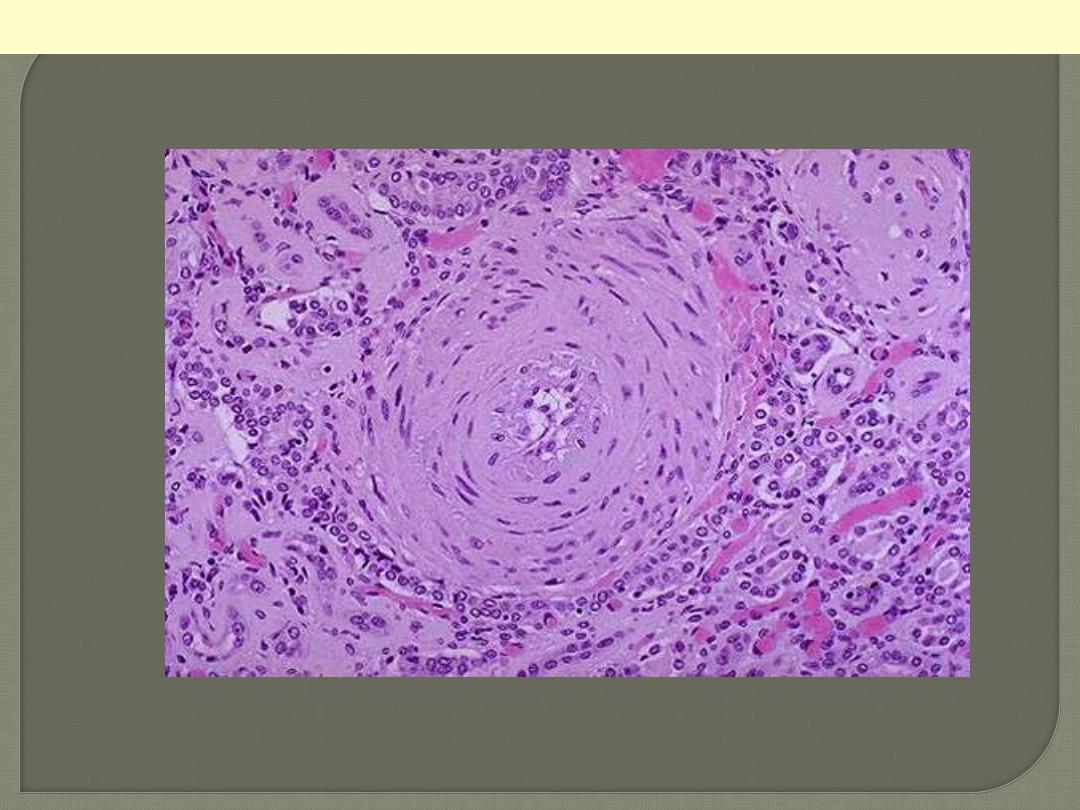
Onion-skin concentric, laminated thickening of the arteriolar wall with progressive narrowing of the
lumen.
Hyperplastic arterilosclerosis
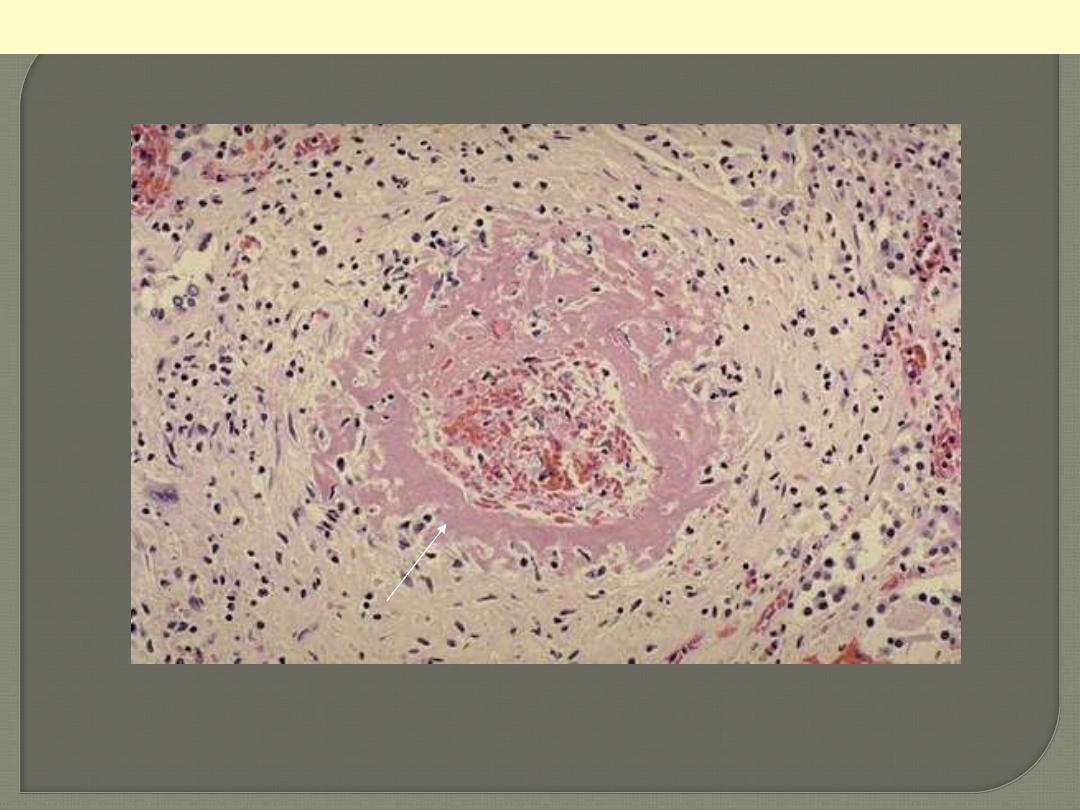
One complication of hyperplastic arteriolosclerosis with malignant hypertension is fibrinoid necrosis,
as seen here in a renal arteriole. Rupture of the affected arterioles lead to grossly visible minute
hemorrhages.
Hyperplastic arterilosclerosis with fibrinoid necrosis
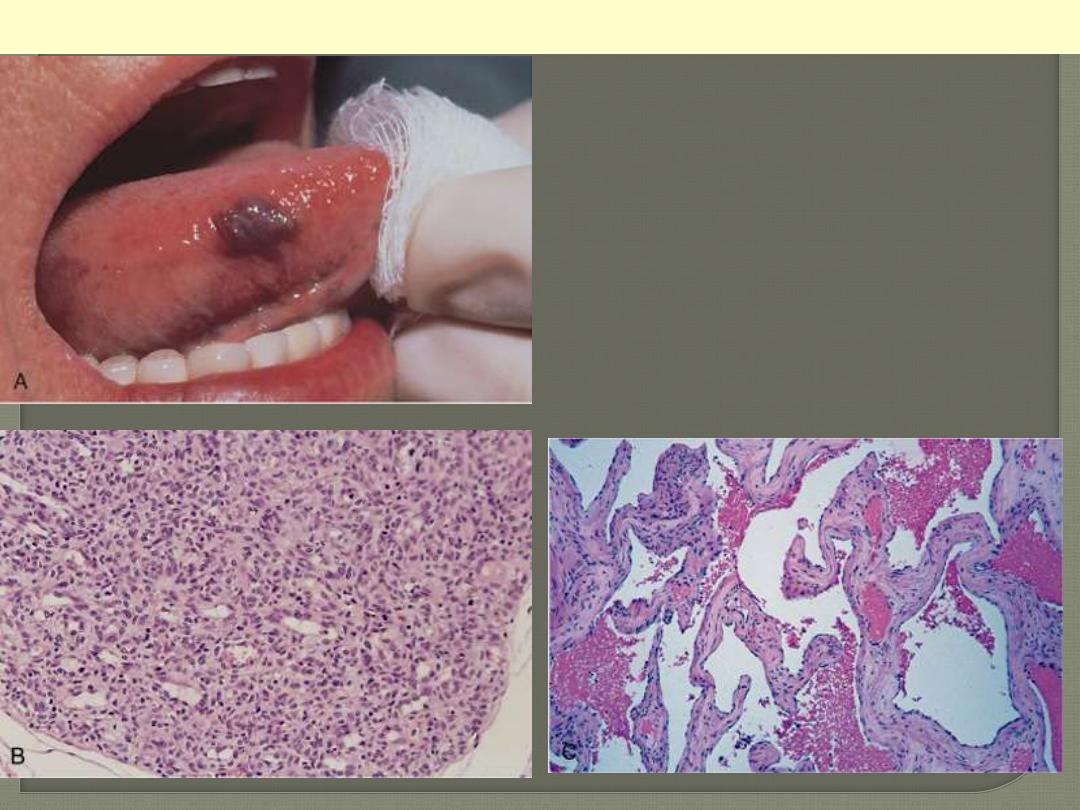
A, Hemangioma of the tongue. B, Histology of
juvenile capillary hemangioma. C, Histology of
cavernous hemangioma
Hemangioma
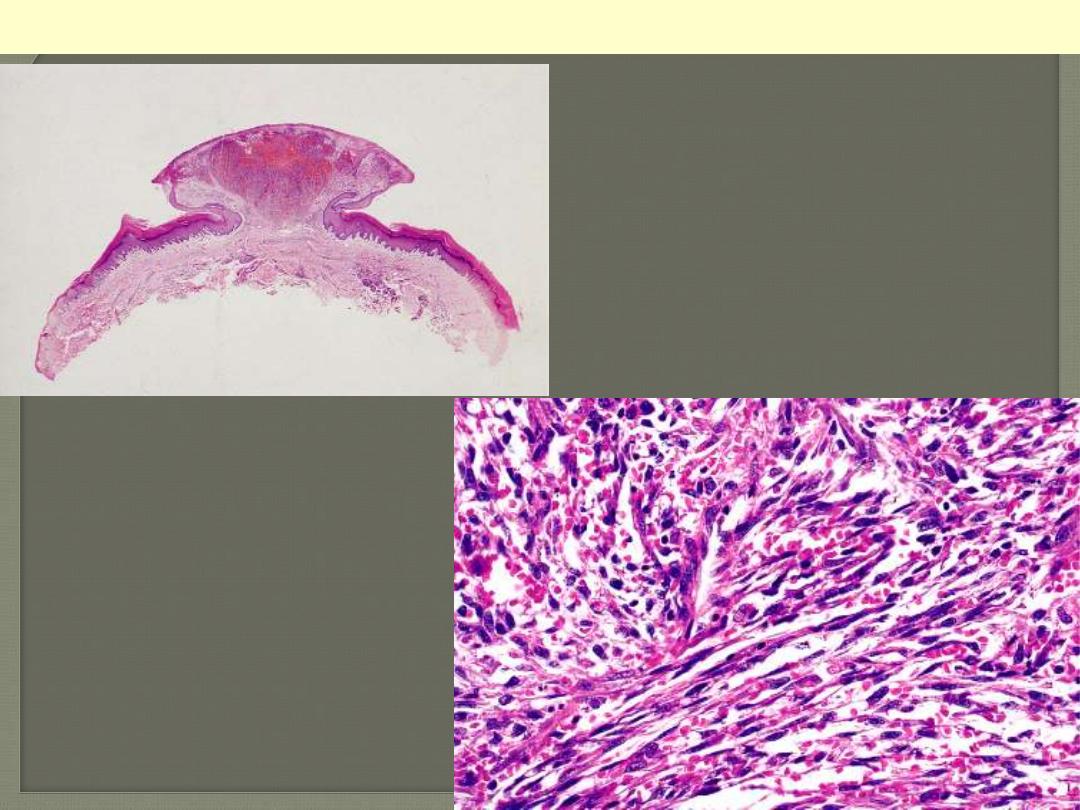
Low-power view of a lesion of Kaposi's sarcoma
having a prominent nodular shape.
Microscopic appearance of Kaposi’s
sarcoma. Elongated spindle cells
showing minimal atypia are separated
by slits containing red blood cells.
Kaposi sarcoma
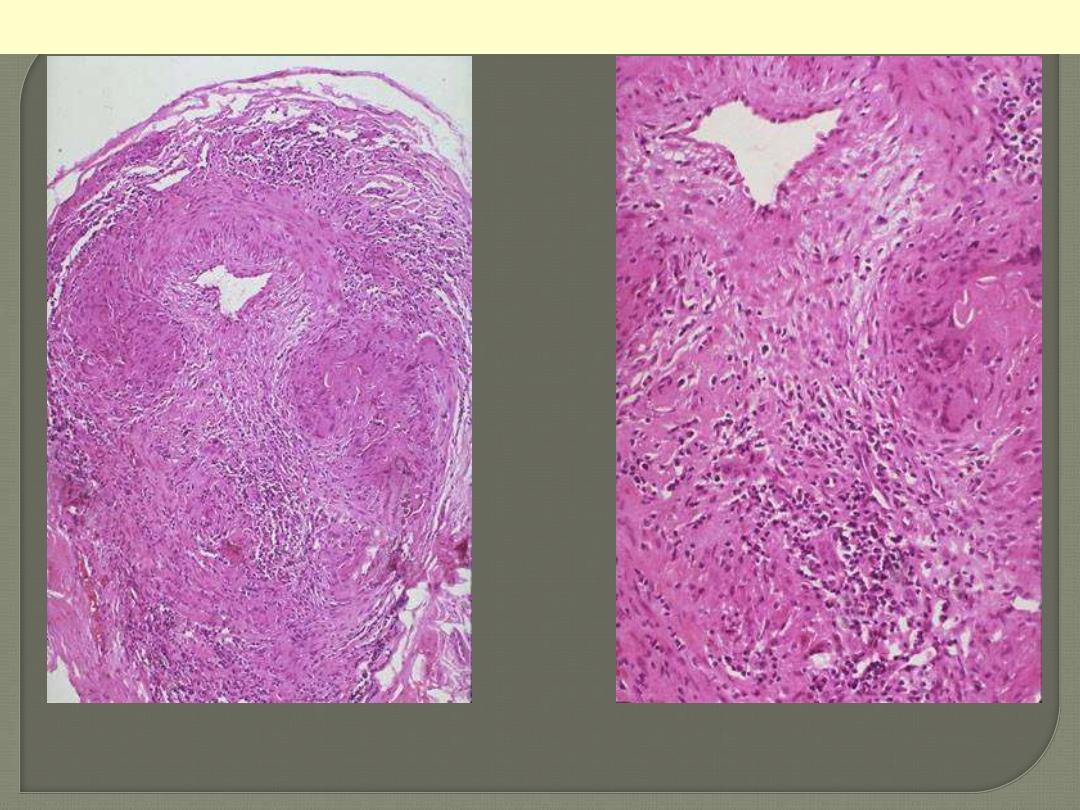
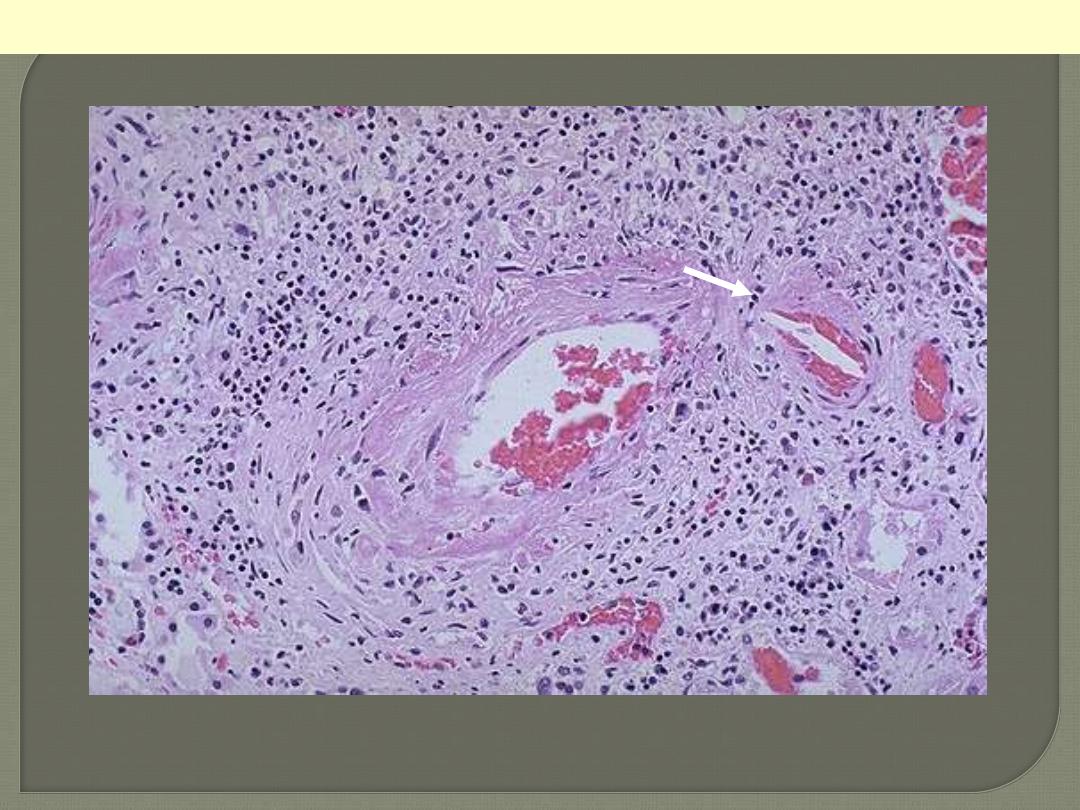
Giant cell (temporal) arteritis
Temporal arteritis is one manifestation of giant cell arteritis, which can affect mainly branches of
external carotid artery. There is thickening of the wall by granulomatous inflammation (with several
multinucleated giant cells) of the media. The lumen is markedly narrowed.
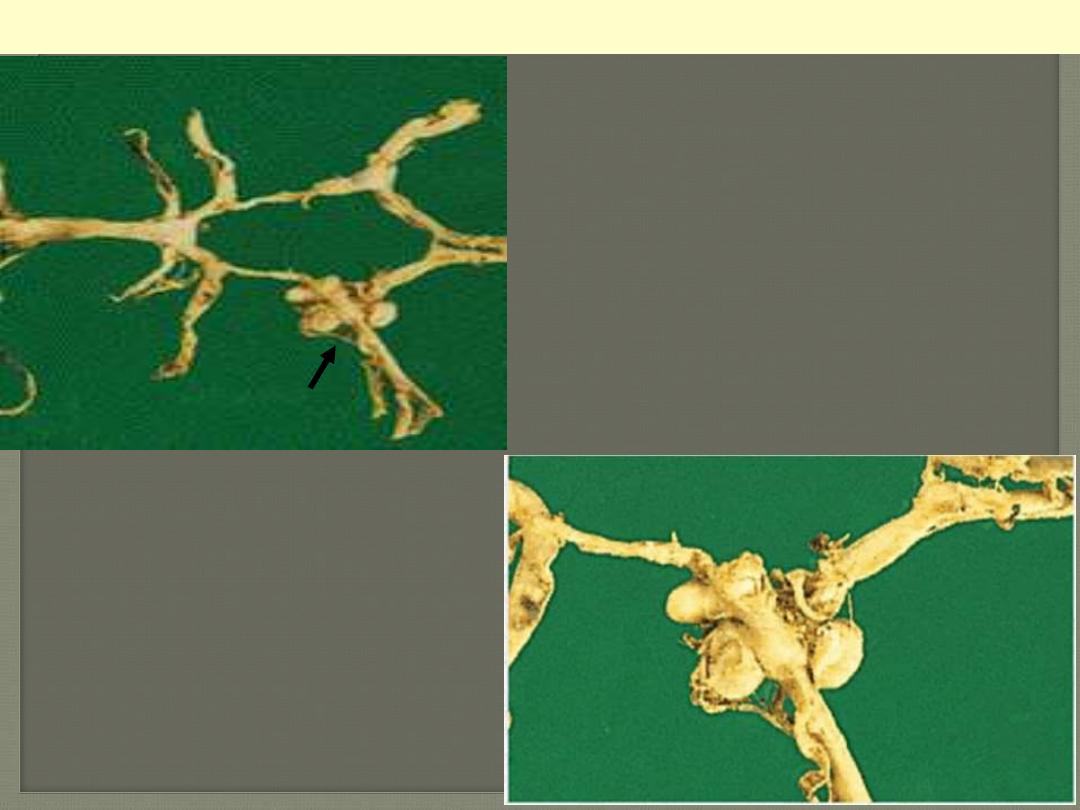
PAN coronaries prominent
aneurysmal dilatations
PAN of the coronary artery branches
PAN of the a renal arterial branch
There are inflammatory cell infiltration scattered in and around the vessel. The wall shows fibrinoid
necrosis with aneurysmal dilatation (arrow). The ANCA serology is usually positive.