Screening
Basic Public Health Concepts

SCREENING: DEFINITION
“The PRESUMPTIVE identification of UNRECOGNIZED disease
or defect by the application of
tests, exams or other procedures
which can be applied RAPIDLY to sort out apparently well persons
who PROBABLY have a disease from those who PROBABLY do
not”*
Key Elements: disease/disorder/defect
screening test
population
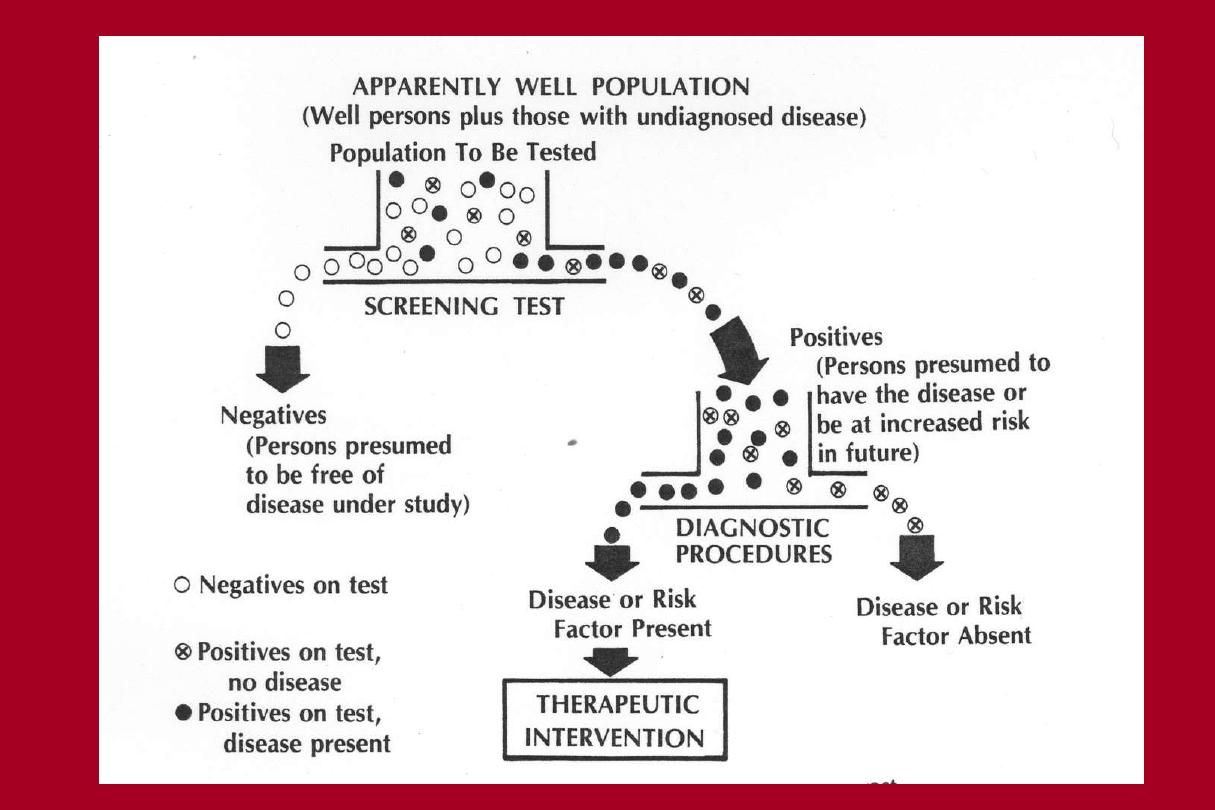

Issues in Screening
Disease
-Disease/disorder should be an important public health problem
High prevalence
Serious outcome
-Early Detection in asymptomatic (pre-clinical) individuals is
possible
-Early detection and treatment can affect the course of disease (or
affect the public health problem?)
Screening Test
Concerned with a Functional Definition of
Normality versus Abnormality
Screening Test
Normal
Abnormal

Test
(Screening test)
Disease
No disease
total
Positive
80
100
180
Negative
20
800
820
total
100
900
1000
Sensitivity = 80 /100 = 80%
Specificity = 800 / 900 = 89%
A population of 1000 people, of whom 100 have a disease and 900 do not
have the disease. A screening test is used to identify the 100 people with
disease.
Test result
With disease
Without disease
Positive
True positive (TP)
False positive (FP)
False negative (FN) True negative (TN)

Positive
predictive value
(+ PV)
The fraction of people
with positive tests
who actually have
the condition.
Negative
predictive value
(-PV)
The fraction of people
with negative tests
who actually don't have
the condition.

Criteria for Evaluating a Screening Test
•Validity
:
provide a good indication of who does and does not have
disease
-Sensitivity of the test
-Specificity of the test
•Reliability
:
(precision): gives consistent results when given to
same person under the same conditions
•Yield
:
Amount of disease detected in the population, relative to the
effort
-Prevalence of disease/predictive value

Validity of Screening Test
(Accuracy)
-
Sensitivity:
Is the test detecting true cases of disease?
(Ideal is 100%: 100% of cases are detected)
-
Specificity:
Is the test excluding those without disease?
(Ideal is 100%: 100% of non-cases are negative)

True Cases of Glaucoma
Yes
No
IOP > 22:
Yes
50
100
No
50
1900
(total)
100
2000
Sensitivity =
50%
(50/100) False Negative=
50%
Specificity =
95%
(1900/2000) False Positive=
5%
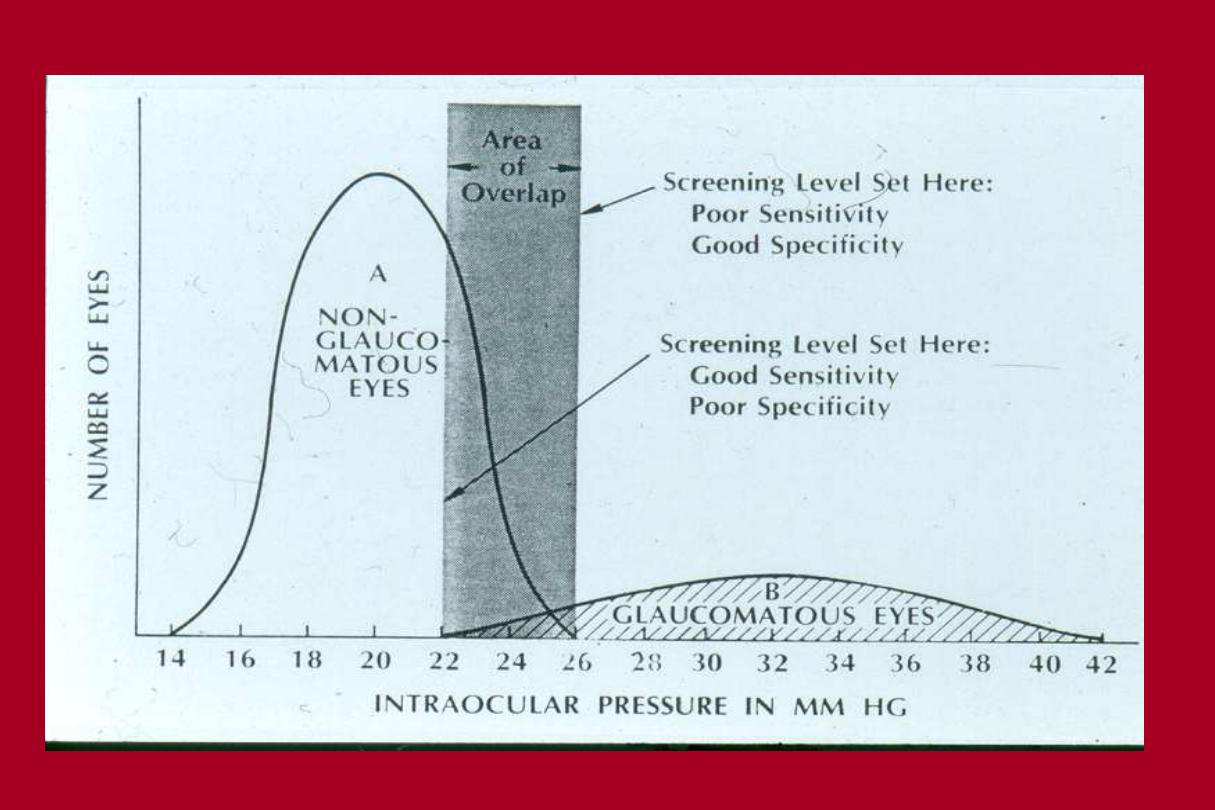
Screening for Glaucoma using IOP
Consider:
-The impact of high number of
false positives:
anxiety, cost of further testing
-Importance of not missing a
case:
seriousness of disease,
likelihood of re-screening
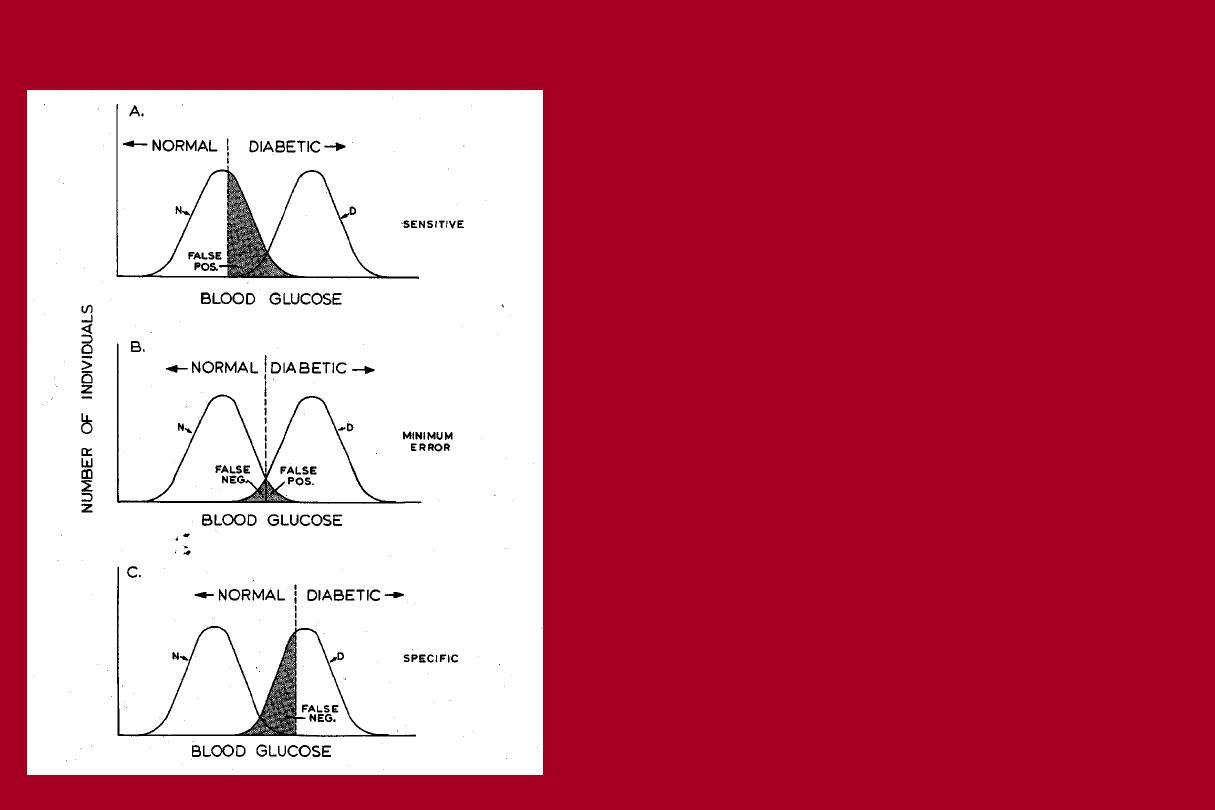
Where do we set the cut-off for a screening test?
Yield from a Screening Test
for Disease X
Predictive Value
X
X
Screening Test
Negatives
Positives
X
X
X
X

Yield from the Screening Test: Predictive Value
•
Relationship between Sensitivity, Specificity, and Prevalence
of Disease
Prevalence is low, even a highly specific test will give
large numbers of False Positives
•Predictive Value of a Positive Test (PPV): Likelihood that a
person with a positive test has the disease
•Predictive Value of a Negative Test (NPV): Likelihood that a
person with a negative test does not have the disease

True Cases of Glaucoma
Yes
No
IOP > 22:
Yes
50
100
No
50
1900
(total)
100
2000
Specificity =
95%
(1900/2000) False Positive=
5%
Positive Predictive Value =33%
Screening for Glaucoma using IOP

How Good does a Screening Test have to be?
IT DEPENDS
-
Seriousness of disease, consequences of high false positivity rate:
-
Rapid HIV test should have >90% sensitivity, 99.9%
specificity
-Screen for nearsighted children proposes 80% sensitivity,
>95% specificity
-Pre-natal genetic questionnaire could be 99% sensitive, 80%
specific

Screening tests
• A test for a particular disease given to patients who have
no symptoms
– Should be an important, morbid health condition
– Generally cheap
– Highly sensitive
– Not too demanding or risky
– There should be a treatment

Screening tests
• Universal screening
– Screening all individuals of a certain category (e.g. PKU
screening in kids)
• Case finding
– Screening a small group of individuals based on the presence of
risk factors (e.g cancer clusters, family members diagnosed
with hereditary disease)

Screening tests
• Adverse effects
– Stress and anxiety caused by false positive results
– Unnecessary radiation/chemical exposure and test discomfort
– Prolonged knowledge of a disease with no treatment
– False sense of security over false negative results
– Overuse of medical resources

Principles for Screening Programs
1. Condition should be an important health problem
2. There should be a recognizable early or latent stage
3. There should be an accepted treatment for persons with
condition
4. The screening test is valid, reliable, with acceptable yield
5. The test should be acceptable to the population to be
screened
6. The cost of screening and case finding should be
economically balanced in relation to medical care as a whole