
POLIOMYELITIS
Epidemiology, Prevention & Control
Introduction
A
viral
infection
most
often
recognized by acute onset of flaccid
paralysis.
Infection with poliovirus results in a
spectrum of clinical manifestations
from inapparent infection to non-
specific
febrile
illness,
aseptic
meningitis, paralytic disease, and
death.
Poliovirus
• Genus:
Enterovirus
•
3 serotypes type 1, 2 & 3
• All types can cause paralysis
• Type 1 most frequently causes
epidemics
• Most vaccine-associated cases
are due to type 2 or 3

Poliomyelitis Pathogenesis
• Entry into mouth
• Replication in pharynx, GI tract, local
lymphatics
• Hematologic spread to lymphatics and
central nervous system
• Viral spread along nerve fibers
• Destruction of motor neurons
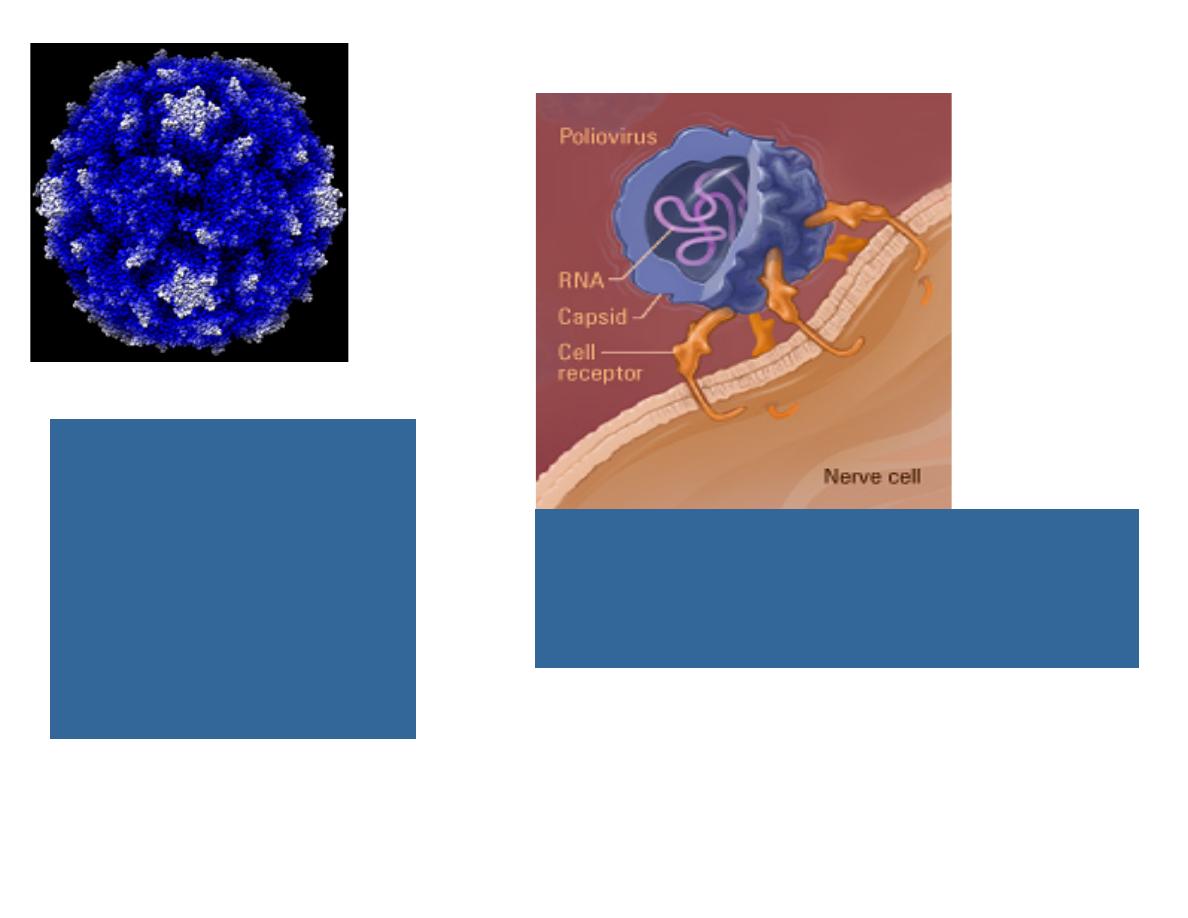
Left: Picture of
poliovirus. The poliovirus
is extremely small, about
50 nm (nanometer = one-
billionth of a meter)
Cour tesy of David Belnap
and J ames Hogle
Right: Cross-section of the poliovirus
showing the RNA, capsid, and nerve cell
receptors
Illustr ation cour tesy of Link
Studio

Case definition
The following case definition for paralytic
poliomyelitis has been approved by CDC
(1997)
Clinical case definition
Acute onset of a flaccid paralysis of one
or more limbs with decreased or absent
tendon reflexes in the affected limbs,
without other apparent cause, and
without sensory or cognitive loss.

Clinical case definition of WHO
•Any child under 15 years of age
with acute flaccid paralysis
(AFP)* or any person of any age
with paralytic illness if polio is
suspected
...
Two phases of acute poliomyelitis
can be distinguished: a non-specific
febrile
illness
including:
fever,
malaise,
headache,
nausea
&
vomiting
(minor illness)
followed, in
a small proportion of patients, by
aseptic meningitis and/or paralytic
disease
(major illness)
.

•
Flaccid paralysis occurs in less than
1% of poliovirus infection
; over 90%
of infections are either inapparent or
result of nonspecific infection.
•
The paralysis of polio is usually
asymmetric
& the maximum extent is
reached in a short period (3-4 days).
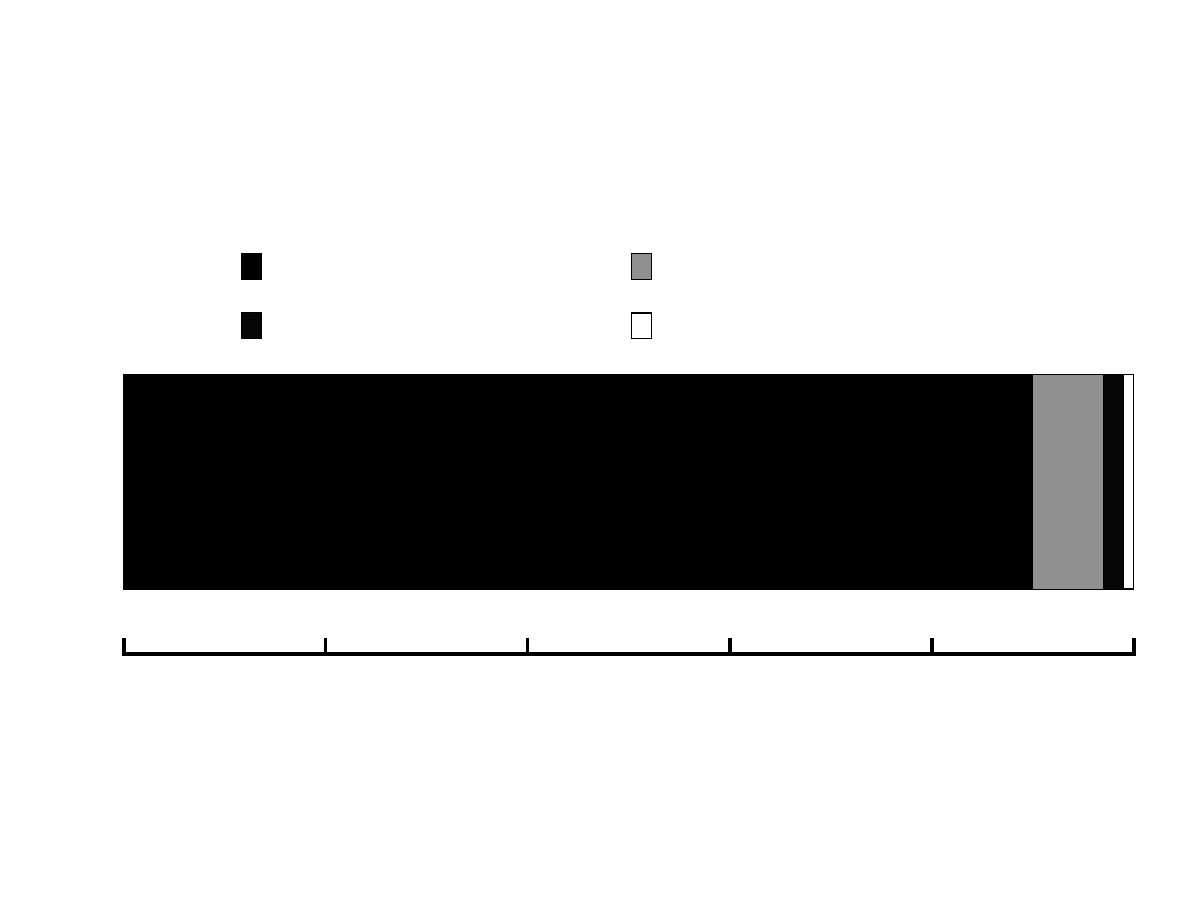
0
20
40
60
80
100
Percent
Asymptomatic
Minor non-CNS illness
Aseptic menigitis
Paralytic
Outcomes of poliovirus infection

Epidemiology of polio
• Reservoir: Human…
• Incubation period: 7-14 days for
paralytic cases…
• Period of communicability:
not
precisely
defined
,,
in
throat
secretion 36 hours & in feces 72
hours
after
exposure
to
infection.

Epidemiological pattern
The epidemiological pattern of polio
depends upon the degree of the
socioeconomic development and
health care services of a country.
The pattern of the disease has been
considerably
modified
by
widespread immunization.

Mode of transmission
Since foci of infection are the throat and small
intestines, poliomyelitis spreads by two
routes:
•
Fecal-oral infection
…
•
Oral-oral infection
: direct droplet infection ..
Where sanitation are high… pharyngeal
spread may be more important !!
In rare cases,
Food-borne
(ingestion) infection
through the ingestion of contaminated foods.
Vehicles include milk, water, or any others that
may be contaminated by handling, flies, dust….

Diagnosis
• Definitive
laboratory
diagnosis
required
isolation
of
the
wild
poliovirus from stool samples, CSF
or oropharyngeal secretions in cell
culture system of human or monkey
origin (primate cells).
Prevention
General prevention:
Health promotion through
environmental sanitation.
Health education (modes of
spread, protective value of
vaccination).

Prevention …
• Active immunization:
–
Salk vaccine
(intramuscular
polio trivalent killed vaccine).
–
Sabin
vaccine
(oral
polio
trivalent
live
attenuated
vaccine).

Inactivated Polio Vaccine
• Contains 3 serotypes of vaccine virus
• Grown on monkey kidney (Vero) cells
• Inactivated with formaldehyde

Oral Polio Vaccine
• Contains 3 serotypes of vaccine virus
• Grown on monkey kidney (Vero) cells
• Contains neomycin and streptomycin
• Shed in stool for up to 6 weeks
following vaccination
Inactivated Polio Vaccine
• Highly effective in producing
immunity to poliovirus
• >90% immune after 2 doses
• >99% immune after 3 doses
• Duration of immunity not
known with certainty

Oral Polio Vaccine
• Highly effective in producing
immunity to poliovirus
• 50% immune after 1 dose
• >95% immune after 3 doses
• Immunity probably life-long

Polio Vaccination Schedule
Age
2 months
4 months
6-18 months
4-6 years
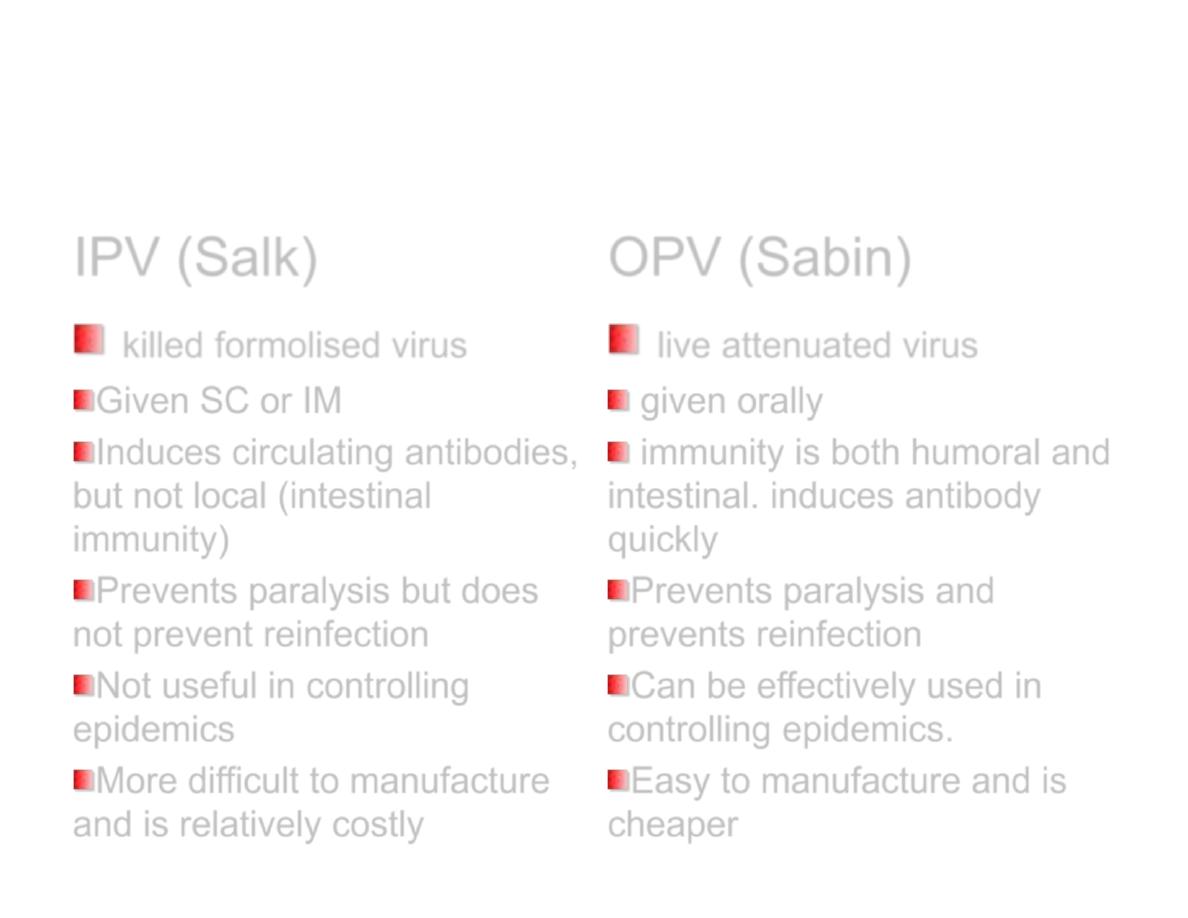
Salk versus Sabin vaccine
IPV (Salk)
OPV (Sabin)
killed formolised virus
Given SC or IM
Induces circulating antibodies,
but not local (intestinal
immunity)
Prevents paralysis but does
not prevent reinfection
Not useful in controlling
epidemics
More difficult to manufacture
and is relatively costly
live attenuated virus
given orally
immunity is both humoral and
intestinal. induces antibody
quickly
Prevents paralysis and
prevents reinfection
Can be effectively used in
controlling epidemics.
Easy to manufacture and is
cheaper

Polio Vaccine Adverse Reactions
• Rare local reactions (IPV)
• No serious reactions to IPV have
been documented
• Paralytic poliomyelitis (OPV)

Polio Vaccine
Contraindications and Precautions
• Serious allergic reaction to
component or following prior dose
• Moderate or severe acute illness

Polio Eradication
• Last case in United States in 1979
• Western Hemisphere certified polio
free in 1994
• Last isolate of type 2 poliovirus in
India in October 1999
• Global eradication goal by 2005

In Iraq…
•
The
last
laboratory-confirmed
indigenous polio case was reported on 28
January, 2000.
•
In 2014 two wild polio cases were
reported from Baghdad – Resafa
province. Dates of onset of the cases were
February and April 2014. Both cases
were linked to Syria outbreak of 2013.

Wild Poliovirus 1988
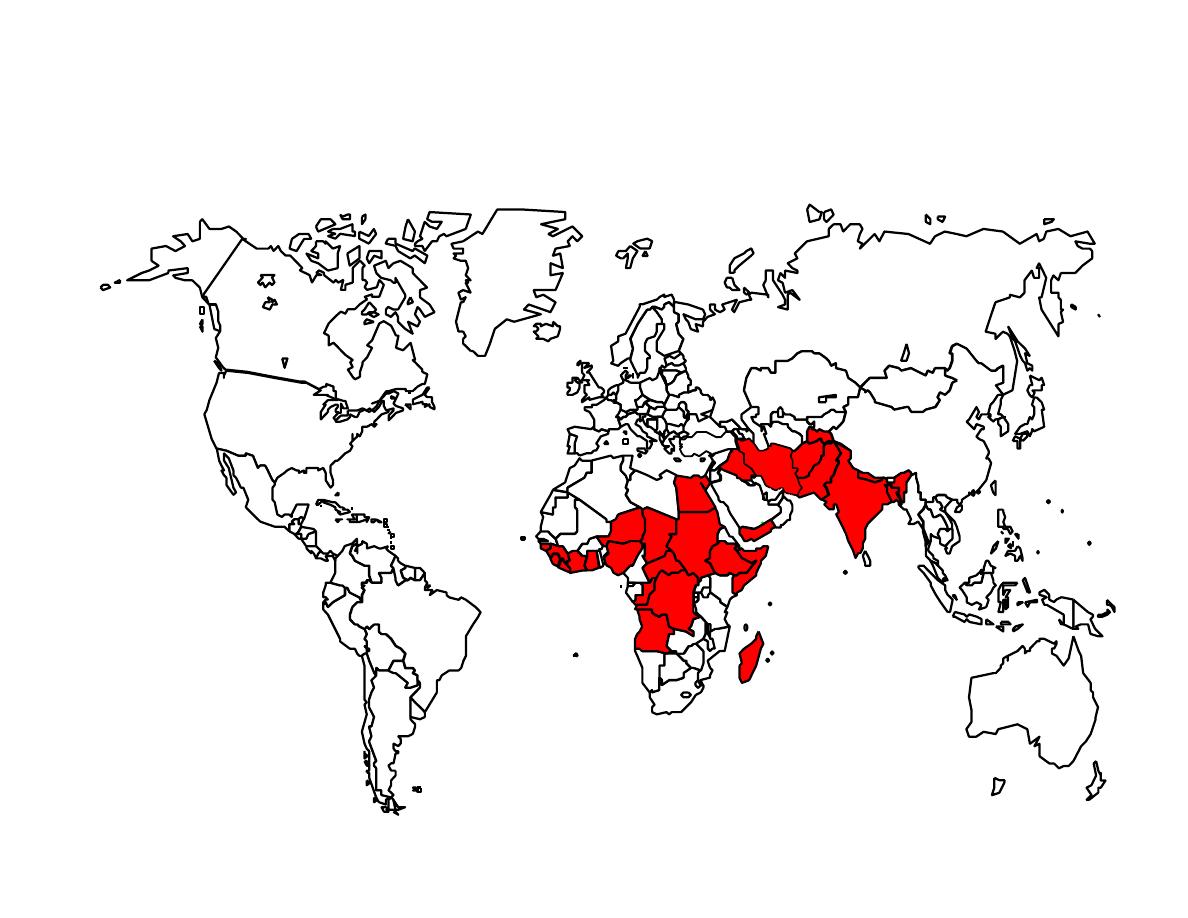
Wild Poliovirus 2000

Control of patients and contacts
- Report to local health authority..
- Isolation: Enteric precautions in
the hospital for wild virus
disease.
- Concurrent disinfection: throat
discharges, feces and articles…

• Protection of contacts: Immunization
of familial and other close contacts is
recommended.
• Investigation of contacts and source
of infection:
Occurrence of a single
case of poliomyelitis due to wild
infection must be recognized as a
public health emergency promoting
immediate investigation.

Epidemic measures:
• In any country,
a single case of
poliomyelitis
must
now
be
considered
a
public
health
emergency
,
requiring
an
extensive
supplementary
immunization response over a
large geographic area.
Disaster implications:
Overcrowding of non-immune
groups and collapse of the
sanitary infrastructure pose an
epidemic threat.
Pigmentation

E. International measures:
• Poliomyelitis is a Disease under surveillance by
WHO and is targeted for eradication by 2005.
• National health administrations are expected to
inform WHO immediately of individual cases and
to supplement these reports as soon as possible
with details of the nature and extent of virus
transmission.
• Planning a large-scale immunization response
must begin immediately and, if epidemiologically
appropriate,
in
coordination with
bordering
countries.

E. International measures (cont.):
Once
a
wild
poliovirus
is
isolated,
molecular epidemiology can often help
trace the source.
Countries should submit monthly reports
on
acute flaccid paralysis (
AFP) cases and
AFP surveillance performance to their
respective WHO offices.
International travelers visiting areas of high
prevalence must be adequately immunized.
THANK YOU