BY:DR.ISHRAQ MOHAMMED

1- post-partum hemorrhage
2- retained placenta
3- uterine inversion
4- ruptured uterus
5- obstetric shock (collapse)
Postpartum hemorrhage, defined as the loss of more
than 500 mL of blood from the genital tract following,
but within the first 24 hours of, the delivery of the
baby.
, occurs in up to 5 percent of all deliveries.
Blood loss
exceeding 1,000 mL is considered physiologically
significant and can result in hemodynamic
instability.
Even with appropriate management,
approximately 0,7percent of vaginal deliveries will
result in severe post-partum hemorrhage.
It is the
most common maternal morbidity in developed
countries and a major cause of death worldwide
Is more of a subjective diagnosis, as its
definition is blood loss from the genital tract
of a volume greater than expected after the
first 24 hours, but within the first 6 weeks of
delivery.
The major etiological factors associated with
secondary pph are retained placental
fragments & endometritis.
Complications from postpartum hemorrhage
include :
1- maternal death
2- acute renal failure
3- embolism
4- anemia
5- sheehan,s syndrome
6- sepsis
7- failure of lactation
Causes of postpartum hemorrhage are
,
, and
, commonly referred to as the
"four Ts":
is the inability of the uterus to contract and
may lead to continuous bleeding. Retained placental tissue and
infection may contribute to uterine atony.
: trauma from the delivery may tear tissue and vessels
leading to significant postpartum bleeding.
: retention of tissue from the
may lead to
bleeding.
: a
occurs when there is a failure
, such as with diseases known as
Causes of postpartum hemorrhage and their
incidence
CauseIncidenceUterine atony70%Trauma20%Retained
tissue10%Coagulopathy1%
Risk factors
Factors relating to the pregnancy:
(15 x risk)
(5 x risk)
x risk)
multiparity (3 x risk)
Previous PPH (3 x risk)
Asian ethnic origin (2 x risk)
Maternal obesity (2 x risk)

Factors relating to delivery:
[
]
Elective CS (4 x risk) - especially if >3 repeat procedures
Retained placenta (5 x risk)
Mediolateral episiotomy (5 x risk)
Operative vaginal delivery (2x risk)
Labour of >12 hours (2 x risk)
>4 kg baby (2 x risk)
Maternal pyrexia in labour (2 x risk)
Pre-existing maternal haemorrhagic conditions:
carrier
carrier
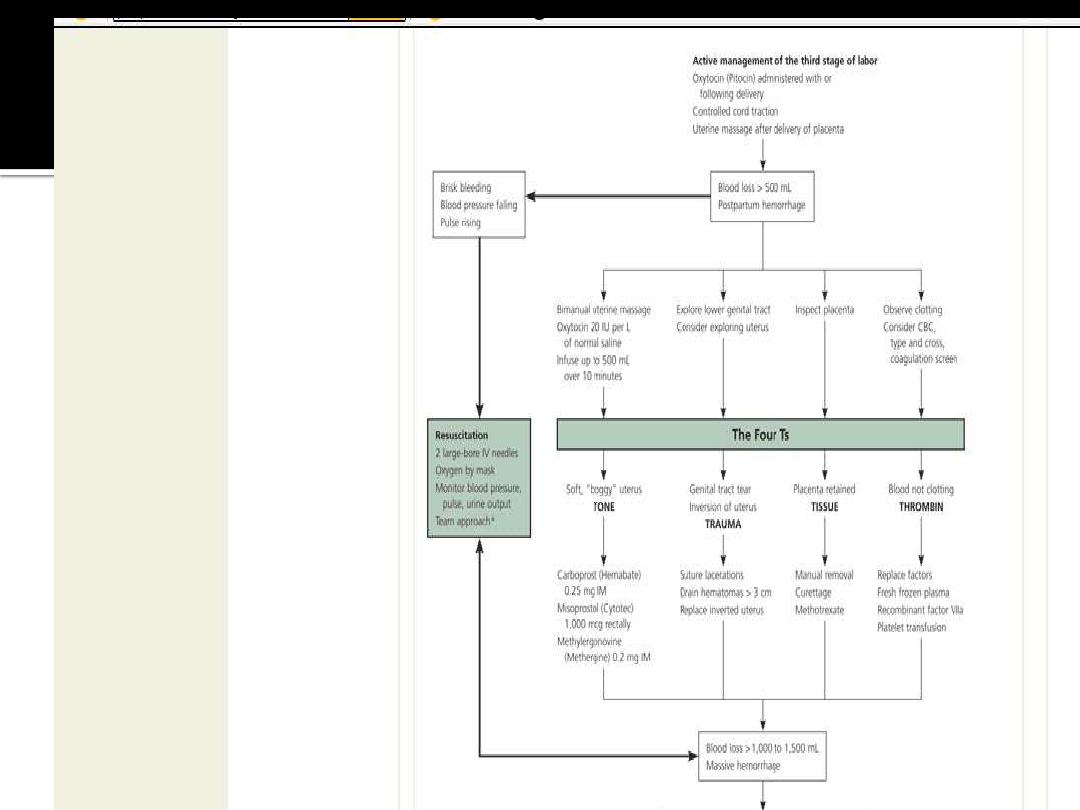
The best preventive strategy is active management of the
third stage of labor .
Hospital guidelines encouraging this
practice have resulted in significant reductions in the
incidence of massive hemorrhage.
which involves administering a uterotonic drug with or
soon after the delivery of the anterior shoulder, controlled
cord traction, and, usually, early cord clamping and
cutting, decreases the risk of postpartum hemorrhage and
shortens the third stage of labor with no significant
increase in the risk of retained placenta.
,
Compared
with expectant management, in which the placenta is
allowed to separate spontaneously aided only by gravity
or nipple stimulation, active management decreases the
incidence of postpartum hemorrhage by 68 percent.
Prophylactic administration of oxytocin (Pitocin)
reduces rates of postpartum hemorrhage by 40
; this reduction also occurs if oxytocin is
given after placental delivery.
Oxytocin is the
drug of choice for preventing postpartum
hemorrhage because it is at least as effective as
ergot alkaloids or prostaglandins and has fewer
side effects.
Misoprostol (Cytotec) has a
role in the prevention of postpartum
hemorrhage (NNT = 18)
; this agent has more
side effects but is inexpensive, heat- and light-
stable, and requires no syringes.
The diagnosis of postpartum hemorrhage
begins with recognition of excessive bleeding
and methodic examination to determine its
cause (
). The “Four Ts” mnemonic
(Tone, Trauma, Tissue, and Thrombin) can be
used to detect specific causes (
).
Two large-bore intravenous cannulae(16G).
Fluid administration(studies failed to show
any benefit of colloids over crystalloids).
Application of facial oxygen.
Examination to determine the etiology of the
hemorrhage, often performing uterine
massage.
Obtain blood for a full blood count, clotting
studies&group&cross-matching.
Is a life threatening complication of massive
PPH.
Regardless the etiology, the management
should aim to follow four basic principles:
1-to maintain the intravascular volume.
2-to administer fresh frozen plasma at a rate to
keep the APTT:control ratio less than 1,5.
3-to administer platelets to maintain their count
more than 75000.
4-to administer cryoprecipitate to keep
fibrinogen level more than 1 gm/dl.
TONE
Uterine atony is the most common cause of postpartum
hemorrhage.
Because hemostasis associated with placental
separation depends on myometrial contraction, atony is treated
initially by pharmcological or a combination of pharmacological &
surgical intervention( ergometrine administeration followed by a
syntocinon infustion).
Should these efforts fail to control bleeding, examination of the
genital tract need to be performed in an operating theatre . This
include examination of vagina, cervix &, in case of continued
bleeding, exploration of the uterine cavity digitally to identify &
removed any retained fragments of placenta.

At this time, if no other cause for the hemorrhage ,
administration of prostaglandin analogues .
Syntocinone i.v bolus dose of 5 i.u followed if
necessary by an infusion of 40 i.u .
Ergometrine i.v/i.m 250-500 ug
Misoprostol p.r 800-1000 ug
Bimanual compression of the uterus , put the
uterine arteries under tension .
In addition to uterotonics, drugs that promote
coagulation can be administered, such as
tranexamic acid & recombinant active factor 7.
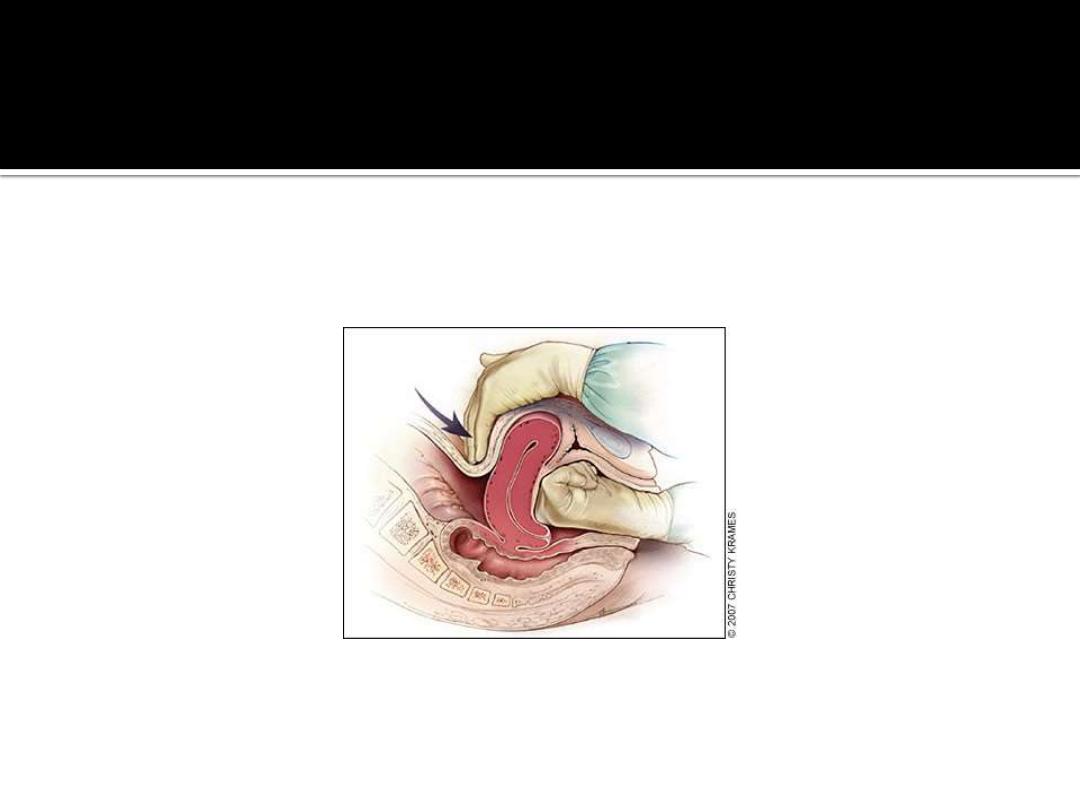

Figure 2.
Technique of bimanual massage for uterine atony.
Bimanual uterine compression massage is performed by
placing one hand in the vagina and pushing against the
body of the uterus while the other hand compresses the
fundus from above through the abdominal wall. The
posterior aspect of the uterus is massaged with the
abdominal hand and the anterior aspect with the vaginal
hand.
Redrawn with permission from Anderson J, Etches D, Smith
D. Postpartum hemorrhage. In: Baxley E. Advanced Life
Support in Obstetrics course syllabus. 4th ed. Leawood,
Kan.: American Academy of Family Physicians, 2001.

If these measures failed, the uterus can be packed
(gauze, balloon insufflation).
Laparotomy: unilateral or bilateral uterine artery
ligation with success rate of more than 90 percent.
Five steps: unilateral ligation of the uterine artery at
the level of the lower uterine segment .
Bilateral ligation.
Low ligation of the uterine artery after mobilization of
the bladder.
Unilateral ovarian vessel ligation.
Bilateral ovarian vessel ligation.
Internal iliac arteries ligation.

Compression sutures: B-lynch sutures.
Arterial embolization.
Hysterectomy with ovarian conservation may
be required as a life saving procedure.
Post operative management:
ICU, CVP, professional counseling.
Prostaglandins enhance uterine contractility and cause
vasoconstriction.
The prostaglandin most commonly used is 15-
methyl prostaglandin F
2a
, or carboprost (Hemabate). Carboprost
can be administered intramyometrially or intramuscularly in a
dose of 0.25 mg; this dose can be repeated every 15 minutes for a
total dose of 2 mg. Carboprost has been proven to control
hemorrhage in up to 87 percent of patients.
In cases where it is
not effective, chorioamnionitis or other risk factors for
hemorrhage often are present.
absolute contraindication, but carboprost should be used with
caution in patients with asthma or hypertension. Side effects
include nausea, vomiting, diarrhea, hypertension, headache,
flushing, and pyrexia.
Misoprostol is another prostaglandin that increases
uterine tone and decreases postpartum
bleeding.
Misoprostol is effective in the treatment of
postpartum hemorrhage, but side effects may limit its
use.
,
It can be administered sublingually, orally,
vaginally, and rectally. Doses range from 200 to 1,000
mcg; the dose recommended by FIGO is 1,000 mcg
administered rectally.
,
Higher peak levels and larger
doses are associated with more side effects, including
shivering, pyrexia, and diarrhea.
is widely used in the treatment of postpartum
hemorrhage, it is not approved by the U.S. Food and Drug
Administration for this indication.
TRAUMA
Lacerations and hematomas resulting from birth trauma can cause
significant blood loss that can be lessened by hemostasis and timely
repair. Sutures should be placed if direct pressure does not stop the
bleeding. Episiotomy increases blood loss and the risk of anal sphincter
tears,
and this procedure should be avoided unless urgent delivery
is necessary and the perineum is thought to be a limiting factor.
Hematomas can present as pain or as a change in vital signs
disproportionate to the amount of blood loss. Small hematomas can be
managed with close observation.
Patients with persistent signs of
volume loss despite fluid replacement, as well as those with large or
enlarging hematomas, require incision and evacuation of the clot.
The
involved area should be irrigated and the bleeding vessels ligated. In
patients with diffuse oozing, a layered closure will help to secure
hemostasis and eliminate dead space.

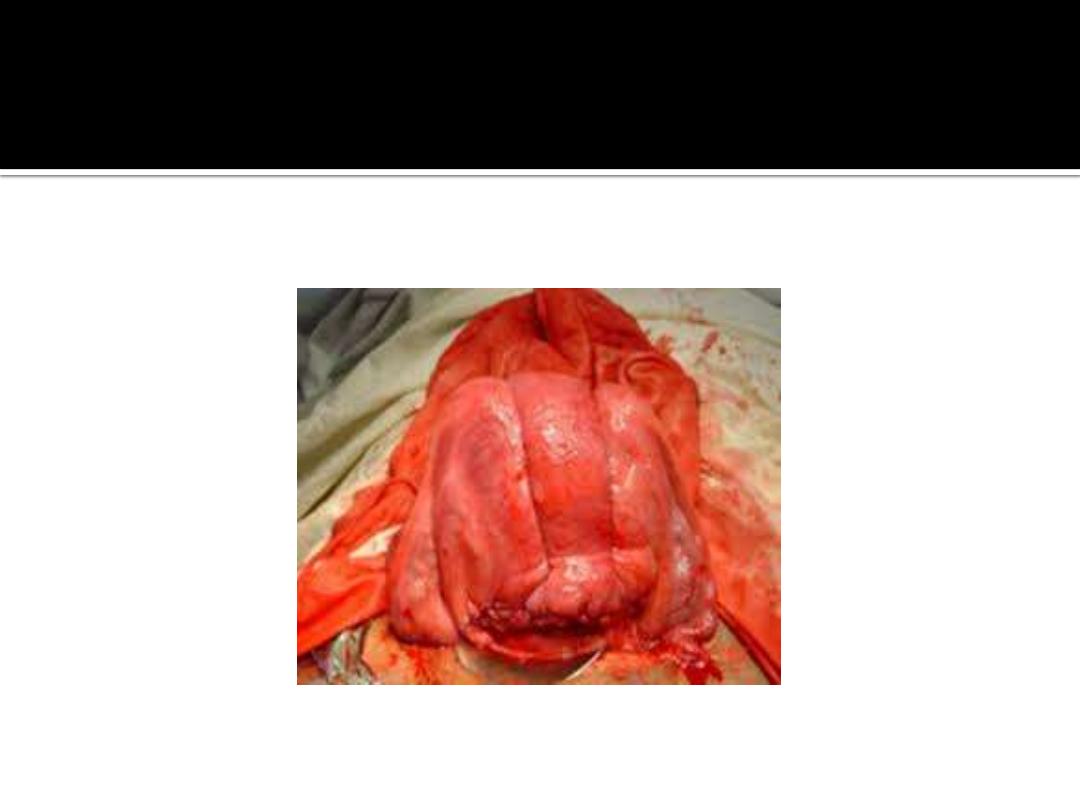
Uterine Inversion
Uterine inversion is rare, occurring in 0.05 percent of deliveries.
management of the third stage of labor may reduce the incidence of uterine
inversion.
Fundal implantation of the placenta may lead to inversion; the roles
of fundal pressure and undue cord traction are uncertain.
usually appears as a bluish-gray mass protruding from the vagina. Vasovagal
effects producing vital sign changes disproportionate to the amount of bleeding
may be an additional clue. The placenta often is still attached, and it should be
left in place until after reduction.
Every attempt should be made to replace the
uterus quickly. The Johnson method of reduction begins with grasping the
protruding fundus
) with the palm of the hand and fingers directed
toward the posterior fornix (
). The uterus is returned to position by
lifting it up through the pelvis and into the abdomen (
).
uterus is reverted, uterotonic agents should be given to promote uterine tone
and to prevent recurrence. If initial attempts to replace the uterus fail or a
cervical contraction ring develops, administration of magnesium sulfate,
terbutaline (Brethine), nitroglycerin, or general anesthesia may allow sufficient
uterine relaxation for manipulation. If these methods fail, the uterus will need to
be replaced surgically.

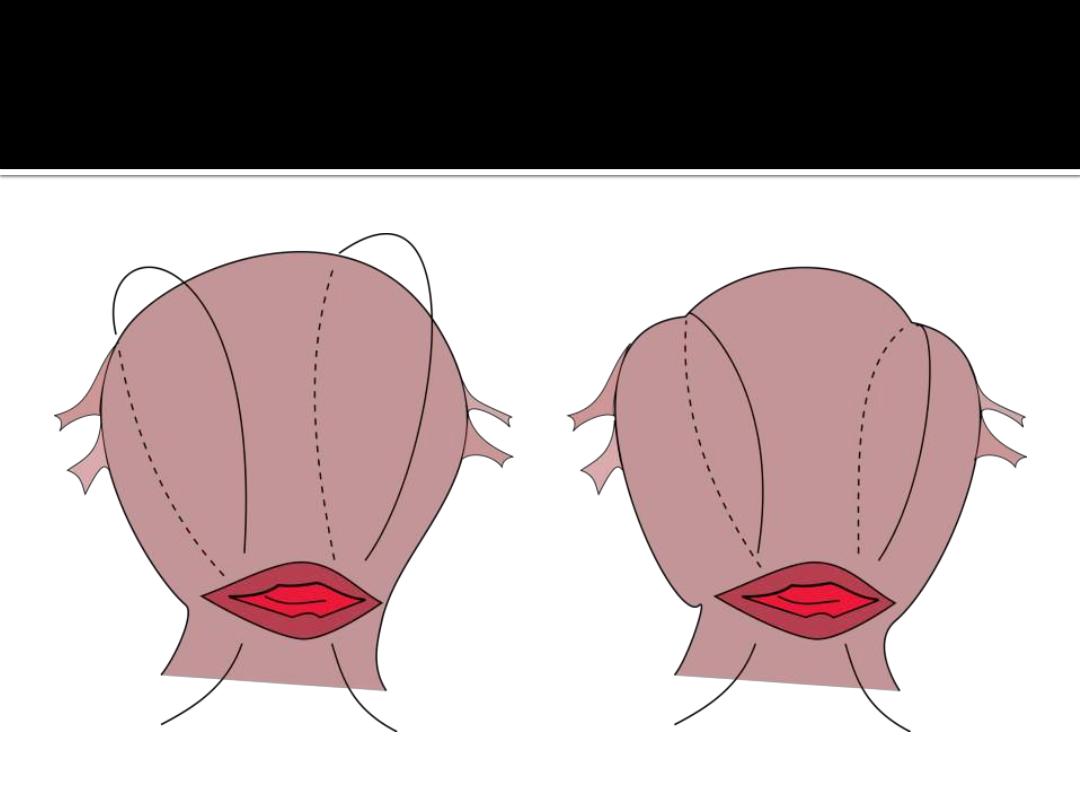
Figure 3.
Reduction of uterine inversion (Johnson
method). (A) The protruding fundus is grasped with
fingers directed toward the posterior fornix. (B, C) The
uterus is returned to position by pushing it through
the pelvis and into the abdomen with steady pressure
towards the umbilicus.
Redrawn with permission from Anderson J, Etches D,
Smith D. Postpartum hemorrhage. In: Baxley E.
Advanced Life Support in Obstetrics course syllabus. 4th
ed. Leawood, Kan.: American Academy of Family
Physicians, 2001.
Uterine Rupture
Although rare in an unscarred uterus, clinically significant uterine
rupture occurs in 0.6 to 0.7 percent of vaginal births after cesarean
delivery in women with a low transverse or unknown uterine
scar.
The risk increases significantly with previous classical
incisions or uterine surgeries, and to a lesser extent with shorter
intervals between pregnancies or a history of multiple cesarean
deliveries, particularly in women with no previous vaginal
deliveries.
Compared with spontaneous labor, induction or
augmentation increases the rate of uterine rupture, more so if
prostaglandins and oxytocin are used sequentially. However, the
incidence of rupture is still low (i.e., 1 to 2.4
percent).
Misoprostol should not be used for cervical ripening
or induction when attempting vaginal birth after previous
cesarean delivery.
Before delivery, the primary sign of uterine
rupture is fetal bradycardia.
Tachycardia or late
decelerations can also herald a uterine rupture,
as can vaginal bleeding, abdominal tenderness,
maternal tachycardia, circulatory collapse, or
increasing abdominal girth.
Symptomatic
uterine rupture requires surgical repair of the
defect or hysterectomy. When detected in the
postpartum period, a small asymptomatic lower
uterine segment defect or bloodless dehiscence
can be followed expectantly.
TISSUE
Classic signs of placental separation include a small gush of blood with
lengthening of the umbilical cord and a slight rise of the uterus in the pelvis.
Placental delivery can be achieved by use of the Brandt-Andrews maneuver,
which involves applying firm traction on the umbilical cord with one hand while
the other applies suprapubic counterpressure (
).
delivery until placental expulsion is eight to nine minutes.
associated with an increased risk of postpartum hemorrhage, with rates doubling
after 10 minutes.
Retained placenta (i.e., failure of the placenta to deliver within
30 minutes after birth) occurs in less than 3 percent of vaginal deliveries.
management option is to inject the umbilical vein with 20 mL of a solution of 0.9
percent saline and 20 units of oxytocin. This significantly reduces the need for
manual removal of the placenta compared with injecting saline
alone.
Alternatively, physicians may proceed directly to manual removal of the
placenta, using appropriate analgesia. If the tissue plane between the uterine
wall and placenta cannot be developed through blunt dissection with the edge of
the gloved hand, invasive placenta should be considered.
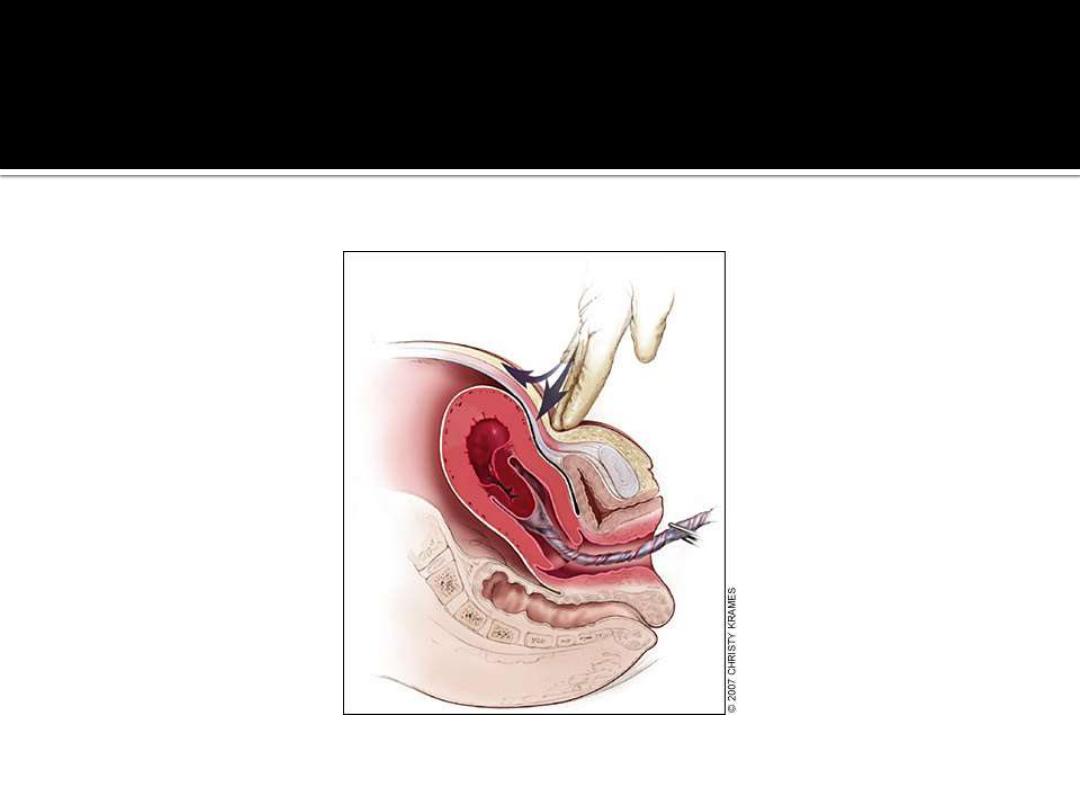

Figure 4.
Brandt-Andrews maneuver for cord traction.
Firm traction is applied to the umbilical cord
with one hand while the other applies
suprapubic counterpressure.
Redrawn with permission from Anderson J, Etches
D, Smith D. Postpartum hemorrhage. In: Baxley E.
Advanced Life Support in Obstetrics course
syllabus. 4th ed. Leawood, Kan.: American
Academy of Family Physicians, 200
Invasive placenta can be life threatening.
The incidence has increased
from 0.003 percent to 0.04 percent of deliveries since 1950s; this increase
is likely a result of the increase in cesarean section rates.
Classification
is based on the depth of invasion and can be easily remembered through
alliteration: placenta accreta adheres to the myometrium,
placenta increta invades the myometrium, and
placentapercreta penetrates the myometrium to or beyond the
serosa.
Risk factors include advanced maternal age, high parity,
previous invasive placenta or cesarean delivery, and placenta previa
(especially in combination with previous cesarean delivery, increasing to
67 percent with four or more).
The most common treatment for
invasive placenta is hysterectomy.
However, conservative management
(i.e., leaving the placenta in place or giving weekly oral
methotrexate
until ⊠ human chorionic gonadotropin levels are 0) is
sometimes successful.
Women treated for a retained placenta must be
observed for late sequelae, including infection and late postpartum
bleeding.
THROMBIN
Coagulation disorders, a rare cause of post-partum hemorrhage, are
unlikely to respond to the measures described above.
coagulopathies are identified before delivery, allowing for advance
planning to prevent postpartum hemorrhage. These disorders include
idiopathic thrombocytopenic purpura, thrombotic thrombocytopenic
purpura, von Willebrand's disease, and hemophilia. Patients also can
develop HELLP (hemolysis, elevated liver enzyme levels, and low platelet
levels) syndrome or disseminated intravascular coagulation. Risk factors
for disseminated intravascular coagulation include severe pre-eclampsia,
amniotic fluid embolism, sepsis, placental abruption, and prolonged
retention of fetal demise.
Abruption is associated with cocaine use
and hypertensive disorders.
Excessive bleeding can deplete coagulation
factors and lead to consumptive coagulation, which promotes further
bleeding. Coagulation defects should be suspected in patients who have
not responded to the usual measures to treat post-partum hemorrhage,
and in those who are not forming blood clots or are oozing from puncture
sites
Evaluation should include a platelet count and
measurement of prothrombin time, partial
thromboplastin time, fibrinogen level, and fibrin
split products (i.e.,
D
-dimer). Management
consists of treating the underlying disease
process, supporting intravascular volume,
serially evaluating coagulation status, and
replacing appropriate blood components.
Administration of recombinant factor VIIa or
clot-promoting medications (e.g., tranexamic
acid [Cyklokapron]) may be considered.
Significant blood loss from any cause requires
standard maternal resuscitation
measures (
). Blood loss of more than
1,000 mL requires quick action and an
interdisciplinary team approach.
is the definitive treatment in women with
severe, intractable hemorrhage. In patients who
desire future fertility, uterus-conserving
treatments include uterine packing or
tamponade procedures, B-lynch uterine
compression sutures, artery ligation, and uterine
artery embolization.
,