Dr.Najma Induction of labor 17/3/2016
:
1
BY: TAHER ALI TAHER
Induction of labour
Induction of labour ( IOL):- is a process of artificially initiating
uterine contraction to induce cx effacement & dialatation
aiming for delivery of fetus .
Incidence of IOL :- 15-25%
induced labor is an abnormal labor , any pt arranged for IOL
should have PV exam to determine Bishop score which
include
which include the following parameters:
1. Cervical dilatation.
2. Cervical effacement: shorting of the length of cervix at time
and during labour (normally the cervix is 3.5-4 cm, if during
labour its length is 2cm, therefore it is 50% effaced).
3. Consistency of the cervix: the cervix is firm but during labour
it becomes softer to ease the delivery.
4. Position of the cervix: the cervix normally posteriorly located,
at time of labour it becomes at the midline then anteriorly.
5. Station of the presenting part.
*the greater the score the easier it should be to initiate
labor
يعني كي باراميميي عنني سكايايمييامثيراري بايرالراميمييياب كي عنني صييراري بايي
ر كي ك سيي
1
-
2
ي سي عنموبي سكايي
1
ي يراريي
3
-
4
ي سي عنموبي سكايي
2
ي ير ميياييي
5
سي عنموبيي
سكايي
3
يوهسذر
.ي
راري بايرالسكاير ميياييي
7
ي ييميريي
favorable cervix
يورانيايي مييرالي جي عيونيي
ب
C\S
ي يرابيراري بايرالسكايراقكياييي
3
ي ليعبهبيي
unfavorable cervix
يورايلباي جمييي
عيونيبيي
C\S
.ي
Dr.Najma Induction of labor 17/3/2016
:
2
BY: TAHER ALI TAHER
At first we should take history we she is planned for IOL (is there
any indication?), then we do abdominal examination to decide
the size of the baby (in case of big baby, it may end with C\S), lie
of the baby, fetal heart normal (any sign of fetal distress like non
reacting ST, abnormal CTG, we can’t do IOL because it will put
burden on already distress baby; uterine contractions cause fetal
hypoxia).
Then we do PV to calculate Bishop Score.
Indication for induction of labour:
1. Post term pregnancy:IOL usually done if she pass the 41 week
+3 days (10 days after EDD) or she pass 42 weeks and the baby
must be normal (kick count normal, reactive ST), if
abnormality present IOL may be done earlier.
2. DM: IOL done at 39 week (to prevent sudden IUD).
3. PE, renal disease&SLE.
4. Rh isoimmunization (even in not sensitized mother we do IOL
to prevent sensitization at 39-40 week, if sensitized the
earlier).
5. Congenital abnormality of fetus: as in case of anencephaly we
must deliver the baby because this abnormality is incompatible
with life, and it is usually done after 24
th
week, if it is done
before 24
th
week it is called induction of abortion.
6. IUD.
7. IUGR.
8. PROM.
9. APH.
Dr.Najma Induction of labor 17/3/2016
:
3
BY: TAHER ALI TAHER
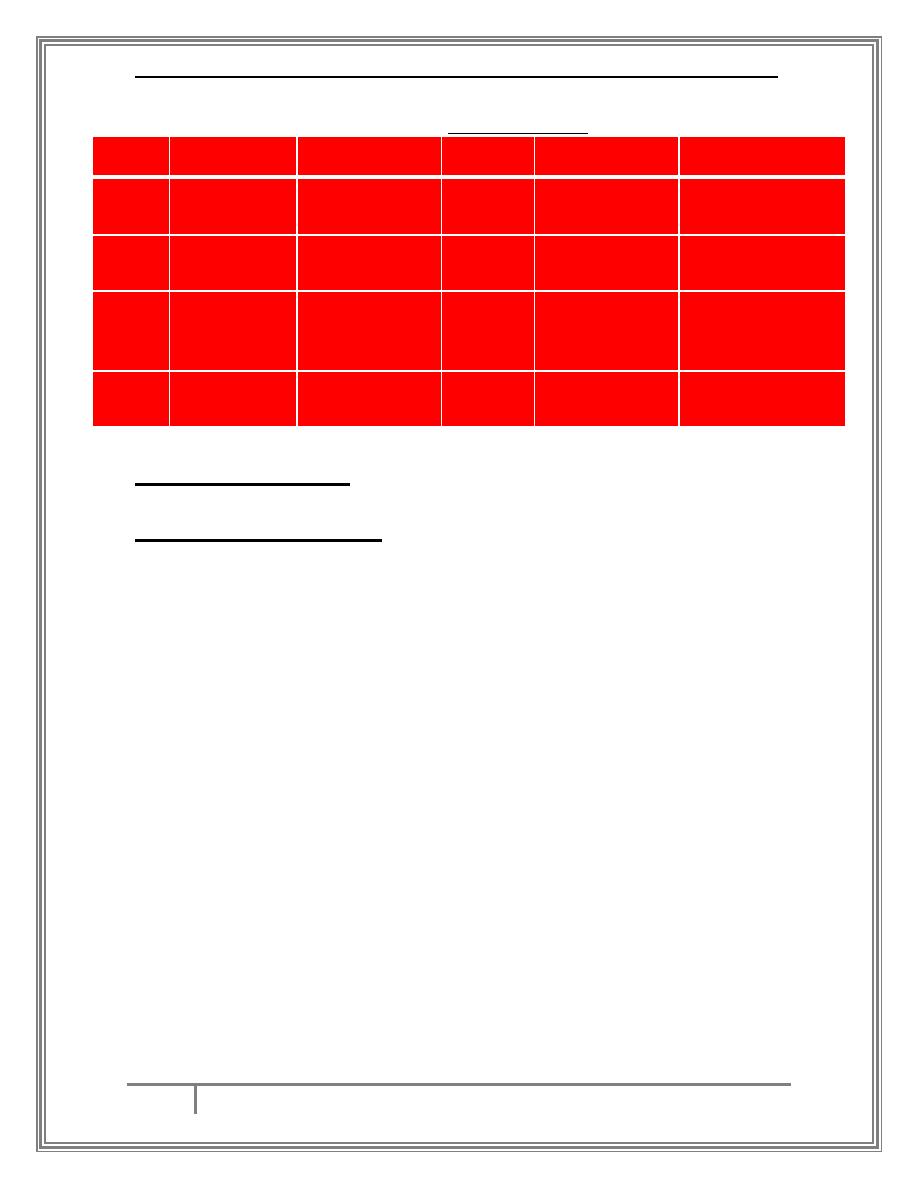
Bishope Score
Cx position
Cx consistency
Station
Effacement
CX dialatation
score
posterior
Firm
-3
0-30 %
closed
O
midposition
Medium
-2
40-50 %
1-2 cm
1
Anterior
Soft
-1
60-70 %
3-4 cm
2
-----------------
------------------
+1,+2
80 %
≤
5
≤
3
Methods of IOL:-
1 - Natural methods :-
a. Castor oil: used to induce smooth muscle contractions of the
bowel leading to diarrhea and in the same time it initiates
uterine contraction.
b. Nipple stimulation: this will release oxytocin from posterior
pituitary gland.
c. Sexual intercourse: because the seminal fluid contains
prostaglandins that will induce uterine contractions.
d. Herbal remedies: some herbals contain ergot derivatives that
cause uterine contractions.
e. Acupuncture( ) را ييرالمعمييي
Dr.Najma Induction of labor 17/3/2016
:
4
BY: TAHER ALI TAHER
2- Medical method :-
a . PG :-
there are many routes for administration, local (vaginally, gel) or
systematically (oral, IV, IM, rectally), the local route is more
preferable because it less associated with side effects
(hypotension, diarrhea, GIT upset), in small dose the PG induces
ripping the cervix and cause favorable cervix (increase the rate of
vaginal delivery and decrease the rate of C\S).
b . misoprostol :-
is cheaper than PG, and the tablet contains 200µg, we divide into
several doses, 25µg used for ripping, up to 50µg for IOL every 4
hours vaginally for 5 doses.
c . oxytocin :-
put into oxytocin pump (not given as direct injection) but given
as units with normal saline drops,
first we start by 15 drops per minute of saline with two unites of
oxytoccin then 30, 45, 60 drops per minute and gradually
increase the units, first we start by 2 units then 4,6 up to 32 units
according to the efficient state of uterine contraction achieved.
يعنيراعني جلديو بهبيي
2
ي ك نيبيي
15
يانيريوارهبي ن ليي
4
يبيي
30
ي ي
4
يبيي
45
ي ي
6
يبيي
60
يهمينيي
شنياحلياعك كياك
efficient uterine contractions
يورانيهكيي
(3 contractions)
per 10 minutes each contraction lasts 30-60 seconds
ي
يوارهبي ليلييرا صمكشيي عصسيرالوزيراني كراعنيرا
efficient contractions
يورهسيشنيي
اعن ليرالوزياايرايلباي لمييي
tetanic uterine contractions
يورانيرايلباي لك يعنيي
rupture uterus
.ي
Dr.Najma Induction of labor 17/3/2016
:
5
BY: TAHER ALI TAHER
Oxytocin infusion should be monitored regularly especially if
there is risk of rupture uterus.
d . mifeprostone
e . castor oil.
3- surgical method :-
Amniotomy: there are 2 type,
Forewater amniotomy :- a sterile plastic hook is inserted into the
vagina and used to puncture the membranes containing the
amniotic fluid. With the membranes punctured, amniotic fluid is
able to escape from the uterus and exit the vagina. The absence
of a fluid buffer between the fetus and uterus stimulates uterine
contractions.
hindwater amniotomy :- a special catheter is used for rupture of
the membrane .
notes : forewater is safer than hind water
both types carry risk of :-
Infection.
Placental separation (abruptio placentae).
If the head is high, there is a risk of cord prolapse.(more in
hindwater type)
4- Sometimes we used combination of methods like:
Start cervical ripping by PG, then ARM, then oxytocin infusion
but oxytocin must be used after 6 hours after the use of PG.
ميياك ميي عننيايباياك
PG
ي لكديار جعكيايلمي سسيورا
ARM
ي ن ليراسك يير يييوراريي
اصقباي حنيوبيي
oxytocin
سيواريي
6
ي بعبت
.ي
Dr.Najma Induction of labor 17/3/2016
:
6
BY: TAHER ALI TAHER
complications of IOL :-
failure of induction
-
increase incidence of cs
-
Fetal distress due to hypertonic uterus
-
uterine rupture
-
-Uterine atony & PPH
-Chorioamnionitis
Management of tetanic uterine contractions :(هبدياحيميوبيرال يكاري سيي
اك كاري لحبايرتي عييرايراني فصيوبيي
)
1. Stop oxytocin infusion.
2. Give normal saline not glucose water (because oxytocin has
antidiuretic effect).
3. Facial O
2
.
4. Tocolytic administration.
…THE END…