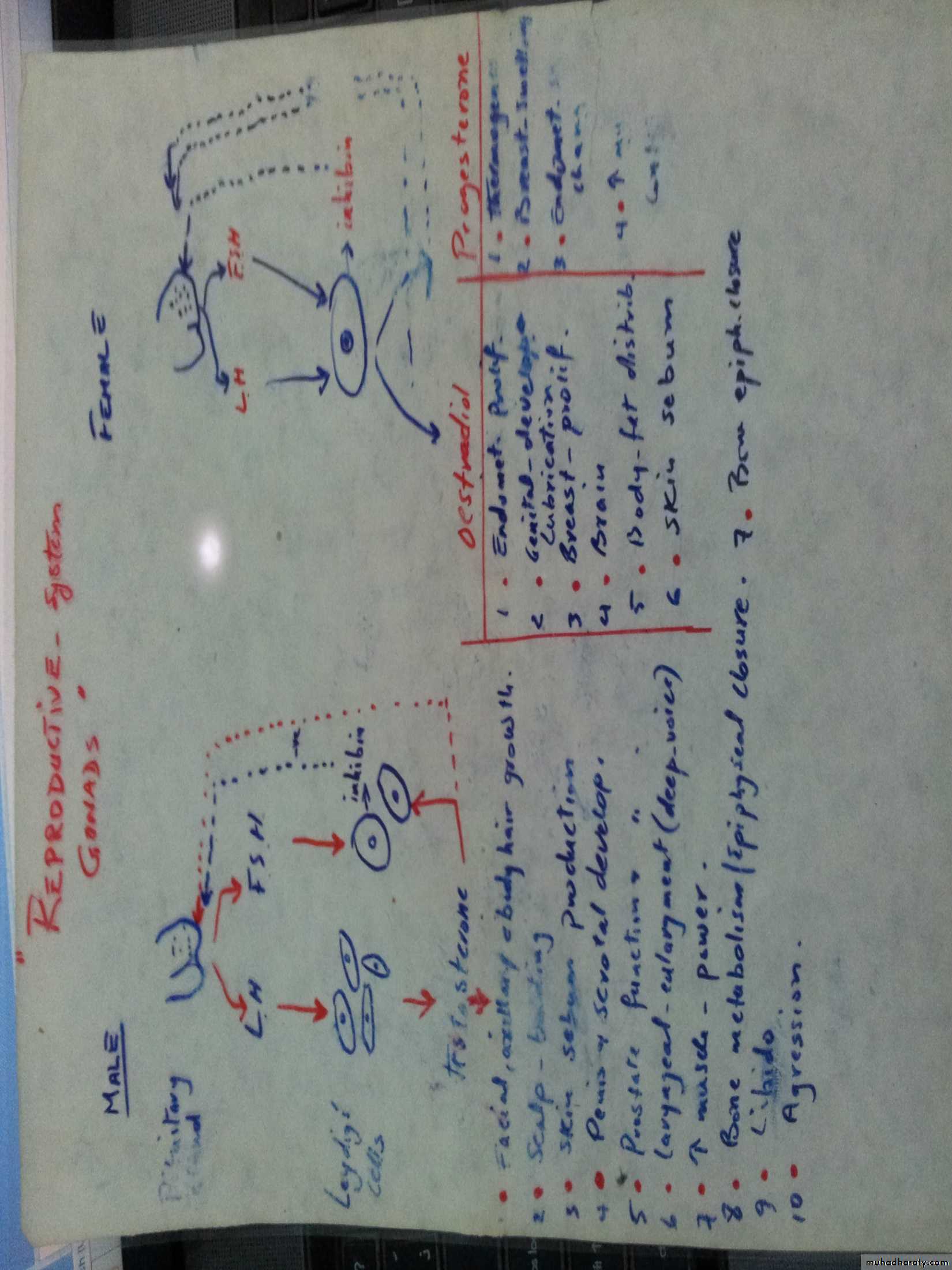
Gonads
Human life is an active male androgenic activity interacting with female estrogenic activity producing fertilized ovum leading to genotypic and phenotypic criteria in their off springsmale androgenic and female estrogenic act. Are at risk for variety of pathologic disorders .
Assessments of testicular functions :
Hx & C/F then investigations :
1. hormonal essay : testesterone, prolactin, LH/FSH
and gonadotrophic hormone
2. urine 17-ketosteroids
3. seminal fluid analysis : volume, sperm count,
liquefaction, morphology,
activity, any pus cells or RBC
4. gonadotropin stimulation test and response ( HCG
injection 2000 iu IM per 4 days then chek
testosterone level one day before the inaitial
dose and after the 4th dose )
5. testicular biopsy ( rarely indicated )
Hypogonadism
b. secondarySheehans syndrome
kalmanns syndrome
Impotence
A. With decrease lipido: hypogonadismdepression
B. With normal lipido : psychological (anxiety)
ischemic ( atheroma )
neuropathic (DM, alcohol, D.S)
drugs (β blockers, thiazides)
Workup of such cases includes :
Hx C/E ( local and systemic )
investigation ; 1. FBS
2. HbA1C
3. hormone ( testosterone, LH-FSH &
prolactin )
4. in Cushings syndrome : Dex. Supp. test .
5. further rare investigations :
a. nocturnal tumescence- monitoring
b. intracavernosal inj. of papaverine
/PGE1 to test the adequacy of blood supply
c. int. pudendal art. angiography .
d. tests for autonomic N.S functions
e. = = P.N conduction
Treatment :
1. treat the cause when possible
2. supportive
a. sildenafil ( viagra 50,100 mg ) it is
phosphodiesterase inhibitor
cardiac, IHD & arrhythmias
b. self administered intracavernosal or
urethral of PGE1
c. prosthetic-implants (fixed-rod,
inflatable-reservoir availability ???
Cost ???
Hirsutism
A. Without virilization : 1. idiopathic (familial)2. PCOS ( hypertension & obesity
primary amenorrhea,
cyst by ultrasound &
infertility )
LH , FSH ,
LH/FSH = 2.5 : 1
20% testosterone & prolactin
B. With virilization : 1. exogenous androgen abuse
2. adrenal tumor, C.A.H
3. overian tumors ( arrhenoplastomas,
ovarian rest tumor)
rapid onst
investigated by : 1. abdominal CT scan
2. hormonal study ( high androgens but not
supp. by dex. or estrogen)
Rx of the cause and low LH-FSH
What is gynecomastia?
Gynecomastia is enlargement of the gland tissue of the male breast. During infancy, puberty, and in middle-aged to older men, gynecomastia can be common. Gynecomastia must be distinguished from pseudogynecomastia, which refers to the presence of fat deposits in the breast area of obese men. True gynecomastia results from growth of the glandular, or breast tissue, which is present in very small amounts in men.
What causes gynecomastia?
Gynecomastia results from an imbalance in hormone levels in which levels of estrogen (female hormones) are increased relative to levels of androgens (male hormones). Gynecomastia that occurs in normally-growing infant and pubertal boys that resolves on its own with time is known as physiologic gynecomastia.All individuals, whether male or female, possess both female hormones (estrogens) and male hormones (androgens). During puberty, levels of these hormones may fluctuate and rise at different levels, resulting in a temporary state in which estrogen concentration is relatively high. Studies regarding the prevalence of gynecomastia in normal adolescents have yielded widely varying results, with prevalence estimates as low as 4% and as high as 69% of adolescent boys. These differences probably result from variations in what is perceived to be normal and the different ages of boys examined in the studies.
Gynecomastia caused by transient changes in hormone levels with growth usually disappears on its own within six months to two years. Occasionally, gynecomastia that develops in puberty persists beyond two years and is referred to as persistent pubertal gynecomastia.
Anumber of condtions that cause gynecomastia includes :
Malnutrition and re-feeding (recovery from malnutrition) have both been shown to create a hormonal environment that may lead to gynecomastia. Similarly, cirrhosis of the liver alters normal hormone metabolism and may lead to gynecomastia.Disorders of the male sex organs (testes) can result in decreased testosterone production and relatively high estrogen levels, leading to gynecomastia. These disorders may be genetic, such as Klinefelter's syndrome, or acquired due to trauma, infection, reduced blood flow, or aging. Testicular cancers may also secrete hormones that cause gynecomastia.
Other conditions that are associated with an altered hormonal environment in the body and may be associated with gynecomastia are chronic renal failure and hyperthyroidism. Rarely, cancers other than testicular tumors may produce hormones that can cause gynecomastia.
Anumber of drugs that cause gynecomastia includes :
Spironolactone a diuretic that has anti-androgenic activity;Calcium channel blockers used to treat hypertension [such as nifedipine];
ACE inhibitor drugs for hypertension captopril, enalapril
some antibiotics {for example, isoniazid, ketoconazole , and metronidazole }
anti-ulcer drugs [such as ranitidine, cimetidine and omeprazole ]
anti-androgen or estrogen therapies for prostate cancer
methyldopa
highly active anti-retroviral therapy (HAART) for HIV disease, which may cause fat redistribution leading to pseudogynecomastia or, in some cases, true gynecomastia
digitoxin
Diazepam
drugs of abuse (for example, alcohol, marijuana, heroin) and
lavender oil and tea tree oil, when used in skin-care products, have been associated with gynecomastia.
What are the risk factors for gynecomastia?
Normally-developing pubertal males may be at risk for gynecomastia that is part of the normal developmental process. Other risk factors include aging, since aging may promote decreases in testosterone production that can cause gynecomastia. The risk factors for developing gynecomastia related to specific diseases and conditions (such as cirrhosis of the liver) are the same risk factors that predispose to those conditions. Taking certain medications (see above) may increase the risk of developing gynecomastia.
What are the symptoms of gynecomastia?
The primary symptom of gynecomastia is enlargement of the male breasts. As mentioned before, gynecomastia is the enlargement of glandular tissue rather than fatty tissue. It is typically symmetrical in location with regard to the nipple and may have a rubbery or firm feel. Gynecomastia usually occurs on both sides but can be unilateral in some cases. The enlargement may be greater on one side even if both sides are involved. Tenderness and sensitivity may be present, although there is typically no severe pain.The most important distinction with gynecomastia is differentiation from male breast cancer, which accounts for about 1% of overall cases of breast cancer. Cancer is usually confined to one side, is not necessarily centered around the nipple, feels hard or firm, and can be associated with dimpling of the skin, retraction of the nipple, nipple discharge, and enlargement of the underarm (axillary) lymph nodes.
How is gynecomastia diagnosed?
The definition of gynecomastia is the presence of breast tissue greater than 0.5 cm in diameter in a male. As previously discussed, gynecomastia is the presence of true breast (glandular) tissue, generally located around the nipple. Fat deposition is not considered to be true gynecomastia.In most cases, gynecomastia can be diagnosed by a physical examination. A careful medical history is also important, including medication and drug use. If there is a suspicion of cancer, a mammogram may be ordered by a health care practitioner. Further tests may be recommended to help establish the cause of gynecomastia in certain cases. These can include blood tests to examine liver, kidney, and thyroid function. Measurement of hormone levels in the bloodstream may also be recommended in some cases.
What is the treatment for gynecomastia?
Gynecomastia, especially in pubertal males, often goes away on its own within about six months, so observation is preferred over specific treatment in many cases. Stopping any offending medications and treatment of underlying medical conditions that cause gynecomastia are also mainstays of treatment.Treatments are also available to specifically address the problem of gynecomastia, but data on their effectiveness are limited, and no drugs have yet been approved by the U.S. Food and Drug Administration (FDA) for treatment of gynecomastia. Medications are more effective in reducing gynecomastia in the early stages, since scarring often occurs after about 12 months. After the tissue has become scarred, medications are not likely to be effective, and surgical removal is the only possible treatment.
Medications that have been used to treat gynecomastia include:
Testosterone replacement has been effective in older men with low levels of testosterone, but it is not effective for me who have normal levels of the male hormone.
The selective estrogen receptor modulators (SERMs) tamoxifen and raloxifene have been shown to reduce breast volume in gynecomastia, although they are not able to entirely eliminate all the breast tissue. This type of therapy is most often used for severe or painful gynecomastia.
Aromatase inhibitors [such as anastrozole ] are a class of medication that interferes with the synthesis of estrogen. While these drugs theoretically should be able to reduce breast mass in gynecomastia, studies have failed to show a significant benefit in treating gynecomastia.
What are the complications of gynecomastia?
Although pubertal gynecomastia typically regresses on its own, in rare cases it may persist, requiring treatment. Gynecomastia that is present over the long term (12 months or more) may undergo scarring (medically termed fibrosis), making treatment with medications much more difficult if not impossible to achieve a response.Psychological consequences can occur if the breast enlargement is pronounced or is a source of embarrassment.
Can gynecomastia be prevented?
Gynecomastia that occurs because of hormonal fluctuations with growth or aging cannot be prevented. Gynecomastia related to medical conditions can only be prevented to the extent that the underlying or responsible condition can be prevented.
What is the outlook for gynecomastia?
Many cases of gynecomastia resolve without treatment, and medical treatment is effective in reducing gynecomastia in many cases. For severe cases or cases in which the breast tissue has become scarred, surgical techniques can help restore normal appearance. Typically, gynecomastia is not associated with long-term problems.
Men with gynecomastia have about a five-fold greater risk for developing male breast cancer when compared with the general population. It is believed that the gynecomastia itself is not a precancerous condition, but rather that the hormonal changes (relative increase in estrogens, lower levels of androgens) that produce gynecomastia in adult men also increase their risk of developing breast cancer.