Dr. Muayad Abbas
Lec. 5
Congenital Abnormalities
of the Gall bladder &
Bile Ducts
Thurs. 12 / 11 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016

Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
2
Congenital Abnormalities of the Gall bladder & Bile Ducts
o Absence of the gall bladder
o The Phrygian cap
o Floating gall bladder
o Double gall bladder
o Absence of the cystic duct
o usually a pathological, mirizzi syndrom, anomaly and indicates the recent
passage of a stone or the presence of a stone at the lower end of the cystic
duct, which is ulcerating into the common bile duct.
o The main danger at surgery is damage to the bile duct, and particular care
to identify the correct anatomy is essential before division of any duct.
o Low insertion of the cystic duct
o An accessory cholecystohepatic duct
o Ducts passing directly into the gall bladder from the liver(duct of Luschka)
Choledochal cyst
o congenital dilatations of the intra- and/or extrahepatic biliary system.
o Patients may present at any age with jaundice, fever, abdominal pain and a
right upper quadrant mass on examination.
o increased risk of developing cholangiocarcinoma with the risk varying
directly with the age at diagnosis
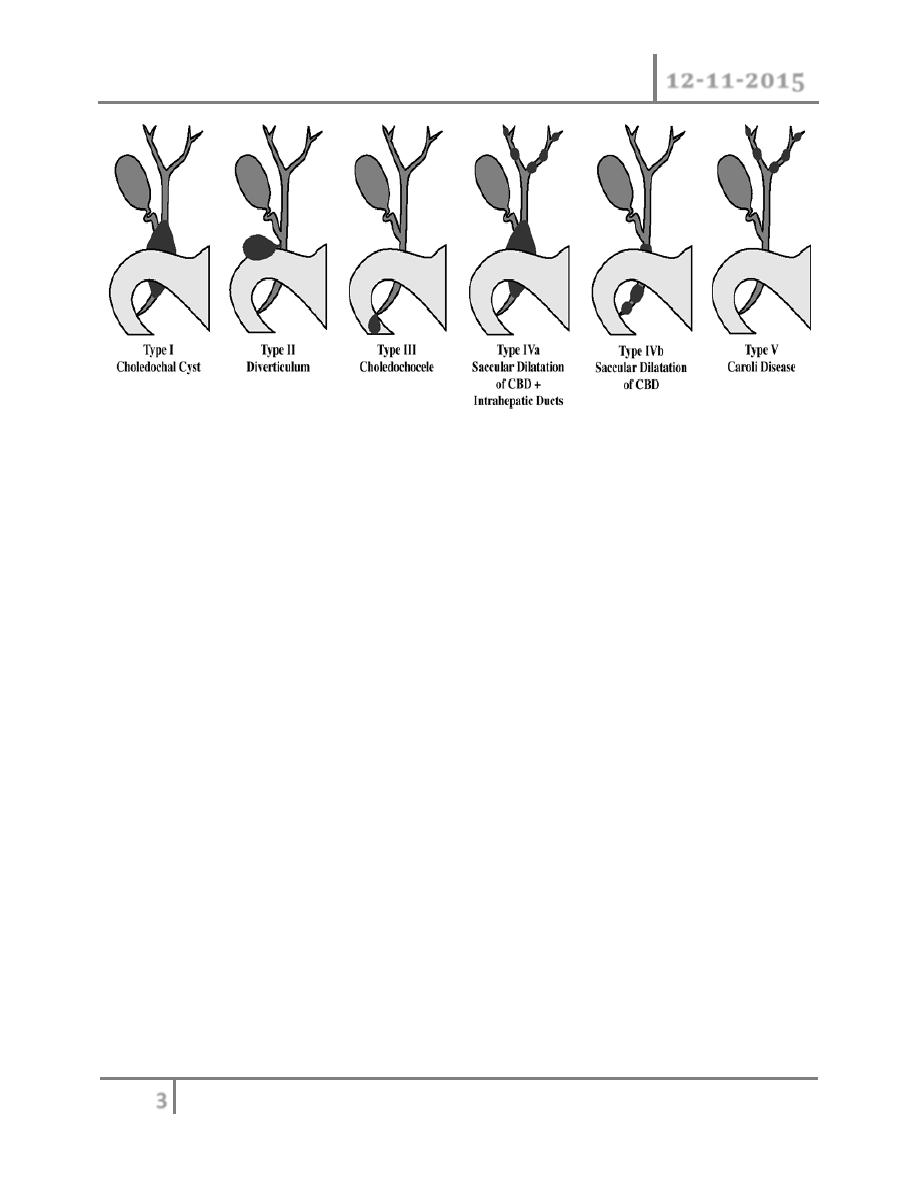
Classification
Type I cysts are the most
common and account for approximately 75% of patients
Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
3
o Ultrasonography will confirm the presence of an abnormal cyst
o magnetic resonance imaging (MRI/MRCP) will reveal the anatomy, in
particular the relationship between the lower end of the bile duct and the
pancreatic duct.
o CT is also useful for delineating the extent of the intra- or extrahepatic
dilatation.
o Radical excision of the cyst is the treatment of choice with reconstruction of
the biliary tract using a Roux-en-Y loop of jejunum.
o Complete resection of the cyst is important because of the association with
the development of cholangiocarcinoma.
TRAUMA of biliary tree
o blunt or penetrating abdominal trauma.
o Operative trauma is perhaps more frequent than external trauma.
o physical signs are those of an acute abdomen.
o Management depends on the location and extent of the biliary and
associated injury.
o In the stable patient, a transected bile duct is best repaired by a Roux-en-Y
choledochojejunostomy.
o Injuries to the gall bladder can be dealt with by cholecystectomy.
Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
4
THE CHOLECYSTOSES (CHOLESTEROSIS, POLYPOSIS,
ADENOMYOMATOSIS AND CHOLECYSTITIS GLANDULARIS
PROLIFERANS)
o This is a not uncommon group of conditions affecting the gall bladder, in
which there are chronic inflammatory changes with hyperplasia of all tissue
elements.
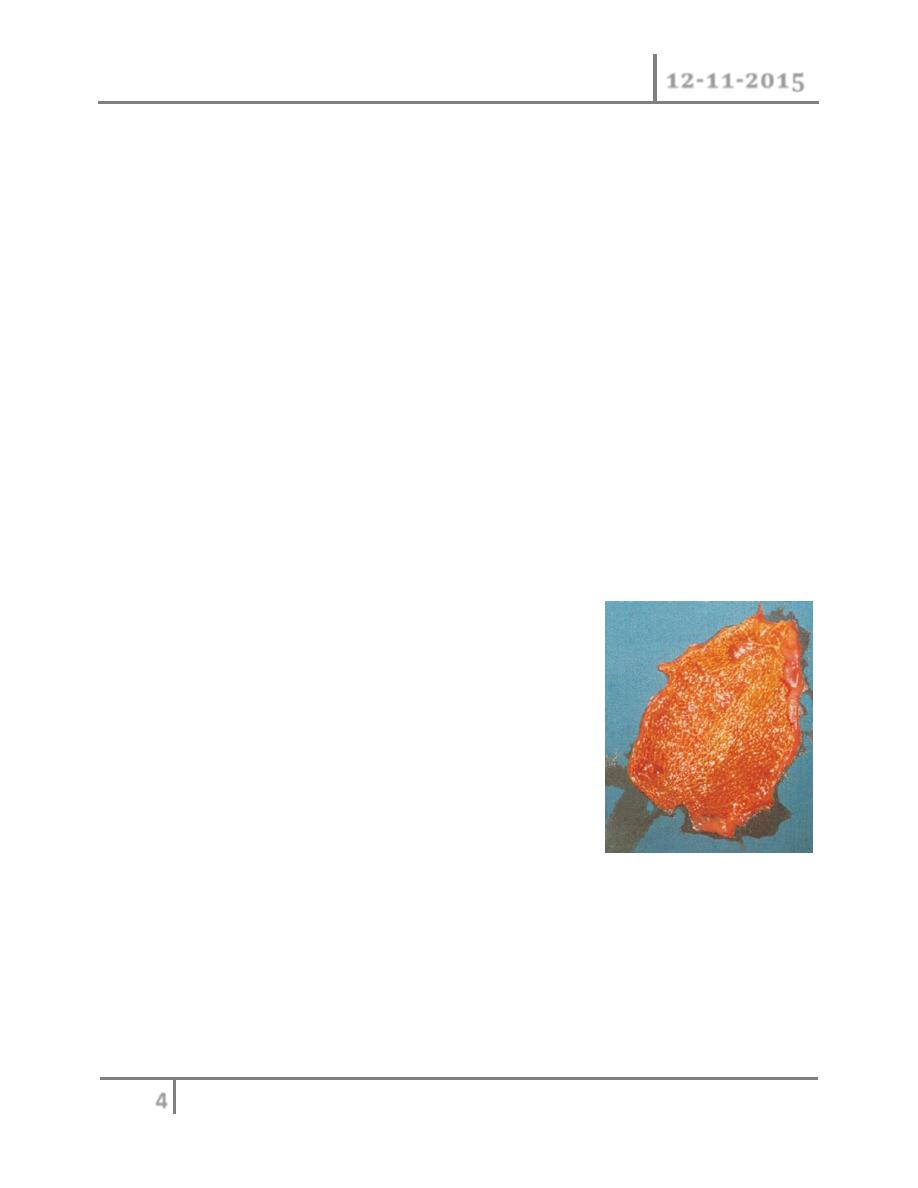
o Cholesterosis (‘strawberry gall bladder’)
o In the fresh state, the interior of the gall bladder looks something like a
strawberry;
o the yellow specks (submucous aggregations of
o cholesterol crystals and cholesterol esters) correspond to the Seeds .
o It may be associated with cholesterol stones.
The interior of a strawberry gall bladder (cholesterosis)
o Cholesterol polyposis of the gall bladder
o These are either cholesterol polyposis or adenomatous change.
o With improving ultrasonography, they are seen more frequently,
o surgery is advised only if they change in size or are longer than 1 cm.
Cholecystitis glandularis proliferans (polyp, adenomyomatosis and intramural
diverticulosis)
Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
5
o A polyp of the mucous membrane is fleshy and granulomatous.
o All layers of the gall bladder wall may be thickened, but sometimes an
incomplete septum forms that separates the hyperplastic from the normal.
o
Intraparietal ‘mixed’ calculi may be present.
o These can be complicated by an intramural, and later extramural, abscess.
o If symptomatic, the patient is treated by cholecystectomy
o Diverticulosis of the gall bladder is usually manifest as black pigment stones
impacted in the outpouchings of the lacunae of Luschka.
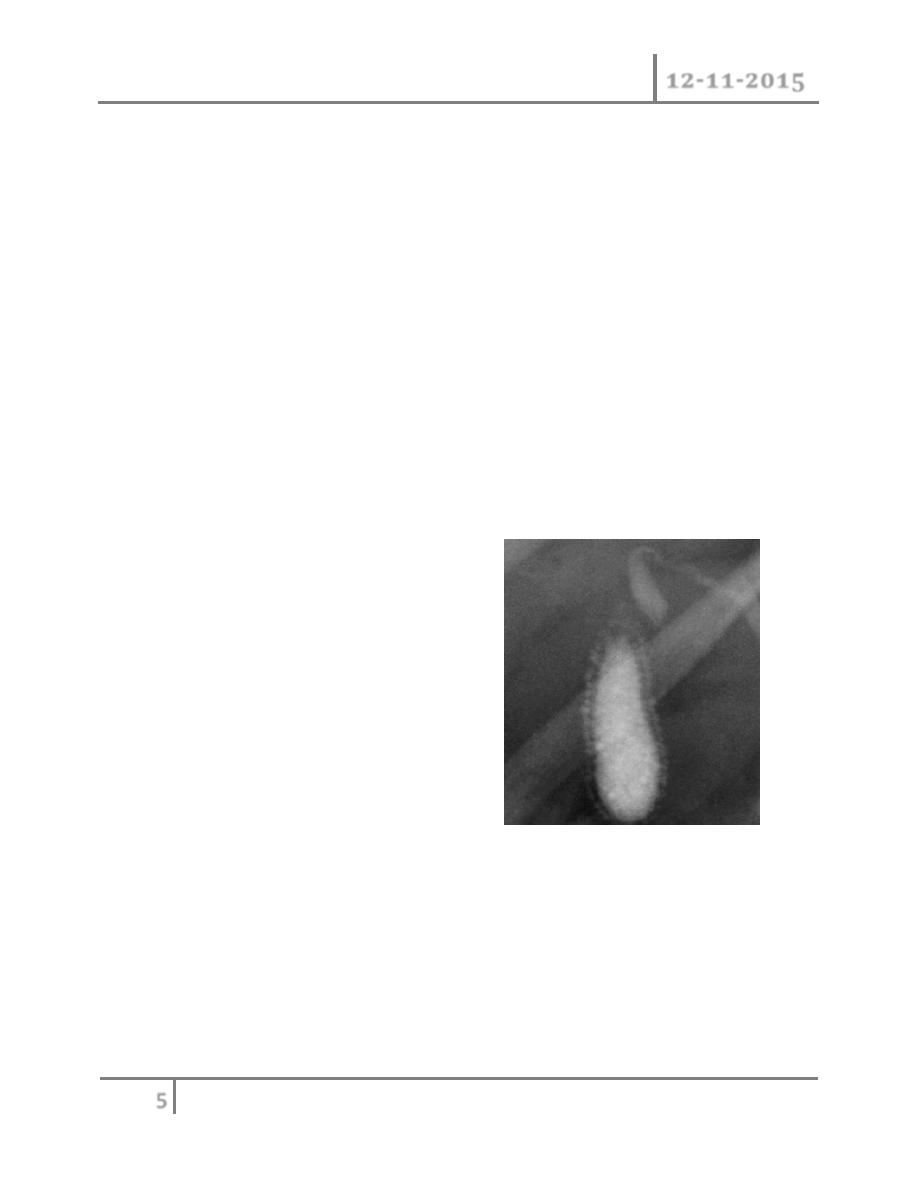
o Diverticulosis of the gall bladder may be demonstrated by cholecystography,
especially when the gall bladder contracts after a fatty meal.
o There are small dots of contrast medium just
o within and outside the gall bladder . A septum mayalso be present [to be
distinguished from the Phrygian cap
o The treatment is cholecystectomy.
Cholecystogram showing diverticulosis with
dots of contrast medium in the gall bladder
wall.
Typhoid gall bladder
o Salmonella typhi and occasionally, Salmonella typhimurium can infect the
gall bladder.
o Acute cholecystitis can occur.
o More frequently, chronic cholecystitis occurs, and the patient, being a
typhoid carrier, excretes the bacteria in the bile.
o Gallstones may be present (surgeons

Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
6
o should not give patients their stones after their operation if there is any
suspicion of typhoid!).
o It is debatable whether the stones are secondary to the Salmonella
cholecystitis or whether pre-existing stones predispose the gall bladder to
chronic infection.
o Salmonellae can, however, frequently be cultured from these stones.
o Ampicillin and cholecystectomy are indicated.
PARASITIC INFESTATION OF THE BILIARY TRACT
o Biliary ascariasis
o The round worm, Ascaris lumbricoides, commonly infests the intestine of
inhabitants of Asia, Africa and Central America.
o It may enter the biliary tree through the ampulla of Vater and cause biliary
pain.
o Complications include strictures, suppurative cholangitis, liver abscesses
and empyema of the gall bladder.
o In the uncomplicated case, anti-spasmodics can be given to relax the
sphincter of Oddi, and the worm will return to the small intestine to be dealt
with by antihelminthic drugs.
o Operation may be necessary to remove the worm or deal with complications.
Worms can be extracted via the ampulla of Vater by ERCP.
Clonorchiasis (Asiatic cholangiohepatis)
o The disease is endemic in the Far East. The fluke, up to 25 mm long and 5
mm wide, inhabits the bile ducts, including the intrahepatic ducts.
o Fibrous thickening of the duct walls occurs
o Complications include biliary pain, stones, cholangitis, cirrhosis and bile
duct carcinoma.
o Choledochotomy and T-tube drainage and, in some cases,
choledochoduodenostomy are required.

Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
7
o Because a process of recurrent stone formation is set up, a
choledochojejunostomy with Roux
o loop affixed to the abdominal parietes is performed in some centres to allow
easy subsequent access to the duct system.
o Hydatid disease
o A large hydatid cyst may obstruct the hepatic ducts.
o Sometimes,a cyst will rupture into the biliary tree and its contents cause
obstructive jaundice or cholangitis, requiring appropriate surgery
Primary sclerosing cholangitis
o Primary sclerosing cholangitis is an idiopathic fibrosing inflammatory
condition of the biliary tree that affects both intrahepatic and extrahepatic
ducts.
o It is of unknown origin, but association with hypergammaglobulinaemia and
elevated markers such as smooth muscle antibodies and anti-nuclear factor
suggests an immunological basis.
o The majority of patients are between 30 and 60 years of age.
o There appears to be a male predominance and a strong association with
inflammatory bowel disease, especially ulcerative colitis.
Common symptoms
o right upper quadrant discomfort,
o jaundice,
o pruritus,
o fever,
o fatigue and weight loss.
Investigation
Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
8
o cholestatic pattern in liver function tests
o elevation of serum alkaline phosphatase and gamma-glutamyl transferase
o and smaller rises in the aminotransferases.
o Bilirubin values can be variable and may fluctuate.
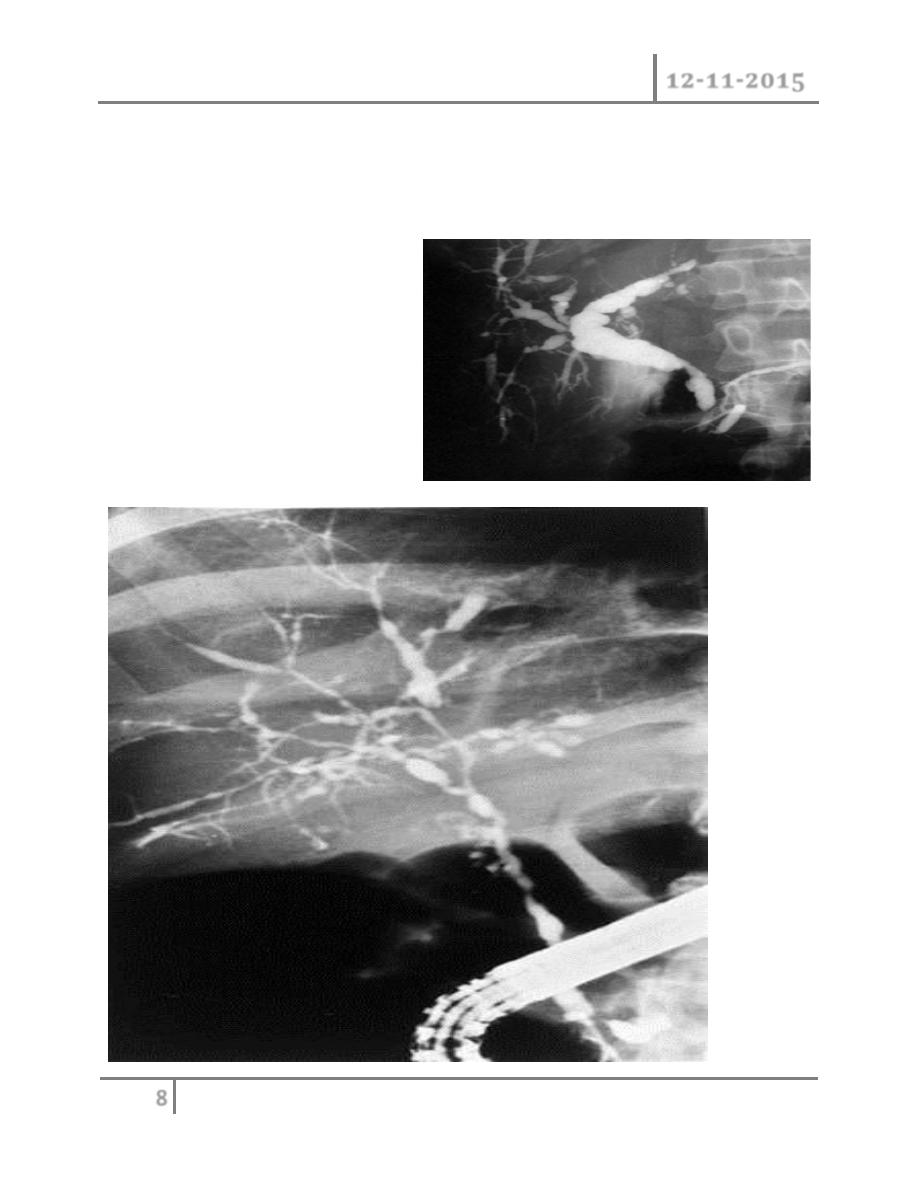
Imaging studies such as MRCP or
ERCP may demonstrate
stricturing and beading of the bile
ducts

Congenital Abnormalities of GB Dr. Muayad Abbas
12-11-2015
9
o A liver biopsy is helpful in confirming the diagnosis and may help to guide
therapy by excluding cirrhosis.
o The important differential diagnoses are secondary sclerosing cholangitis
and cholangiocarcinoma.
o Medical management with antibiotics,
o vitamin K,
o cholestyramine,
o steroids
o and immunosuppressants such as azathioprine is generally unsuccessful.
o Endoscopic stenting of dominant strictures and, in selected patients with
predominantly extrahepatic disease, operative resection may be worthwhile.
o For patients with cirrhosis, liver transplantation is the best option.
o Five-year survival following transplantation is in excess of 80%.
END …
Done by
Ali Kareem