Baghdad College of Medicine / 4
th
grade
Student’s Name :
Dr. Tariq Al-Obaidi
Lec. 3
DISEASES OF BREAST
Mon. 21 / 12 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016

Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
2
©Ali Kareem 2015-2016
Diseases of Breast
Carcinoma of the breast : is the most common cause of death in middle aged
women in western countries. In 2004 approximately one and half million new cases
were diagnosed worldwide. In England and Wales one in 12 women will develop
the disease during their life time.
Risks factors
1) Geographical: it occurs most commonly in western world, accounting 3-5%
of all death in women. In developing countries it accounts for 1-3% of death.
2) Age: it is extremely rare below the age of 20 years but thereafter the
incidence steadily rise that by the age of 90 years nearly 20% of women are
affected.
3) Gender: it is less than 0.5% of patients with breast cancer are male.
4) Genetics: it occurs more commonly in women with a family history of breast
cancer than in general population. Breast cancer related to specific
mutation account for about 5% of breast cancer.
5) Diet: there is some evidence that there is a link with diets low in
phytoestreogen, a high intake of alcohol is associated with increase risk.
Diets are recommended are walnut, broccoli, peach and curcuma.
6) Endocrine: it is more common in nulliparous women , breast feeding in
particular approved to be protective. Also protective in having a first child
Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
3
©Ali Kareem 2015-2016
at an early age, especially if associated with late menarche and early
menopause. It is known that in postmenopausal, breast cancer is more in
obese. This is thought to be because of increased conversion of steroid
hormone to oestrodiol in the body fat.
7) Previous radiation; this was considered to be historical interest, with the
majority of women exposed to the atomic bombs at Hiroshima and Nagasaki
having dead, again using of utilized uranium in Iraqi war play a role in this
disease. It is, however a real problem in women who have been treated with
mantle radiotherapy as a part of the management of Hodgkin lymphoma
disease, in which significant dose of radiation is received. The risk appears
about decade after treatment and is higher if radiotherapy occurred during
breast development.
Incidences in carcinoma breast
o 30% of all female cancers.
o 20% of cancer related deaths in females.
o 2-4% bilateral.
o 2-5% hereditary.
o Lump is most common Presentation.(75%)
o 10% present with pain.
o 35%-45% with mutation of BRCA1 gene
o 70% blood spread occurs to bones.

Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
4
©Ali Kareem 2015-2016
Risk Factors
o BC in 1
st
degree relatives.
o BC in contralateral breast.
o BRCA1/BRCA2 gene mutation.
o Obesity and alcohol intake.
o Gynaecomastia in male breast.
o Nulliparty.
o Early menarche and late menopause.
Pathology : breast cancer may arise
from the epithelium of the duct system
anywhere from the nipple end of major
lactiferous ducts to the terminal duct
unit, which is in breast lobule. The
disease may be entirely in situ, an
increasingly common finding with the
advent of breast cancer screening or
may be invasive cancer. The degree of differentiation of the tumor is
usually described using three grades as well differentiation, moderately
differentiation or poorly differentiation. Commonly numerical grading
system based on the scoring of the three individual factors (nuclear
pleomorphism, tubular formation, and mitotic rate) is used in grade 3
cancers roughly equating the poorly differentiated group.
Previously, descriptive terms were used to classify breast cancer scirrhous
meaning woody or medullary meaning brain like. More recently histological
descriptions have been used. however with the increasing application of
molecular markers (immunohistochemistry) there will be a change in the
way that the breast cancers are classified, and it is likely that much more
information about individual tumor will be routinely reported, such as its
likelihood of metastases, and to which therapeutic agents it will be susptible.
Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
5
©Ali Kareem 2015-2016
Gene array analysis of breast cancer has identified five subtypes. Some of
these correlate with known markers such as estrogen receptor status.
Current nomenclature: ductal carcinoma: is the most variant (85%),
lobular carcinoma occurring about 15% of cases, there are subtypes of
lobular carcinoma including the classical type which carries a better
prognosis than the pleomorphic type, occasionally pictures may be mixed
with both ductal and lobular features. There are different pattern of spread
depending on histological type.
If there is doubt whether as tumor is predominantly lobular in type,
immunohistochemical analysis using the e- cadherin antibody which reacts
positively in lobular carcinoma will help in diagnosis. Rare histological
variants, usually carrying a better prognosis, include colloid carcinoma
whose cells produce a abundant mucin.
Medullary carcinoma with solid sheets of large cells usually associated with
a marked lymphocytic reaction. Invasive lobular carcinoma is commonly
multifocal and or bilateral. Cases detected via screening program are often
smaller and better differentiation than those presenting to symptomatic and
are of a special type.

Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
6
©Ali Kareem 2015-2016
Cases detected via screening program are often smaller and better
differentiation than those presenting to symptomatic and are of a special
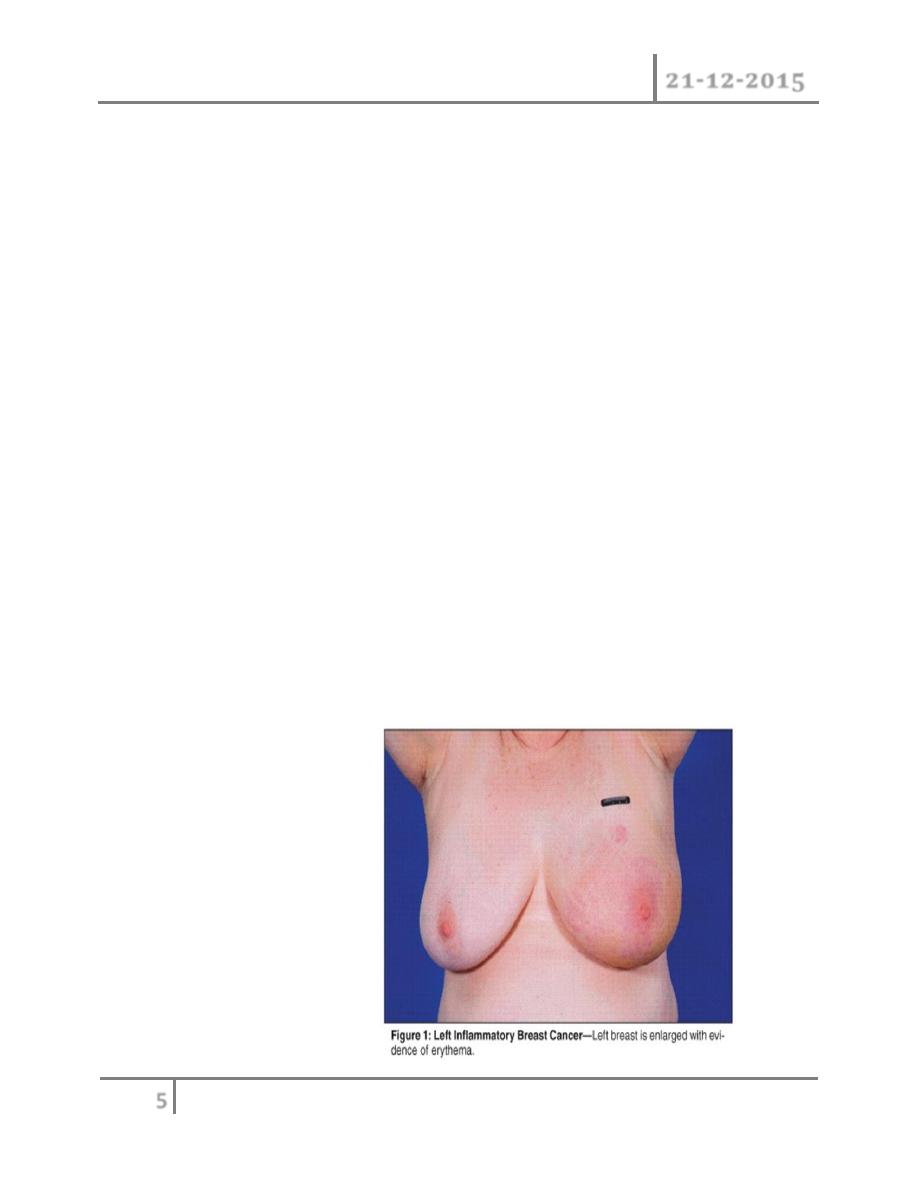
type. Inflammatory carcinoma is a fortunately rare, highly aggressive that
present as painful swollen breast which is warm with cutaneous edema; this
is result of blockage of the subdermal lymphatics with cancer cells.
Inflammatory carcinoma usually involves at least 1/3 of the breast and may
mimic breast abscess.
A biopsy will confirm the diagnosis and show undifferentiated cells, it used
to be rapidly fatal but with aggressive chemotherapy and radiotherapy and
with salvage surgery the prognosis has improved considerably. In situ
carcinoma is a preinvasive cancer that has not breached the epithelium
basement membrane.
This was previously a rare usually asymptomatic, finding in breast biopsy
specimens but is becoming increasingly common because of the advent of
mammographic screening. In situ carcinoma may be ductal (DCIS) or
lobular (LCIS). The latter is often being multifocal and bilateral. Both are
markers for later development of invasive cancers which will develop in at
least 20% of patients. Although mastectomy is curative, this constitutes
overtreatment in many cases. The best treatment for carcinoma in situ is
depend if it is a high grade tumor treated by excision and radiotherapy,
whereas those of low grade whose tumor completely excised need no further
treatment.
Staining for estrogen and progesterone receptors is now considered routine,
as their presence will indicate the use of adjuvant hormone therapy with
tamoxifin or the newer aromatase inhibitors as anastrazole. Tumors also
stained for c- erb2( a growth factor receptor)as patients who are positive
can be treated with monoclonal antibody as trastuzumab (herciptin) either
in the adjuvant or relapse sitting. The pathologist is an important member of
breast cancer team (MDT) and will increasingly help decide which adjuvant
therapies will be appropriate.
Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
7
©Ali Kareem 2015-2016
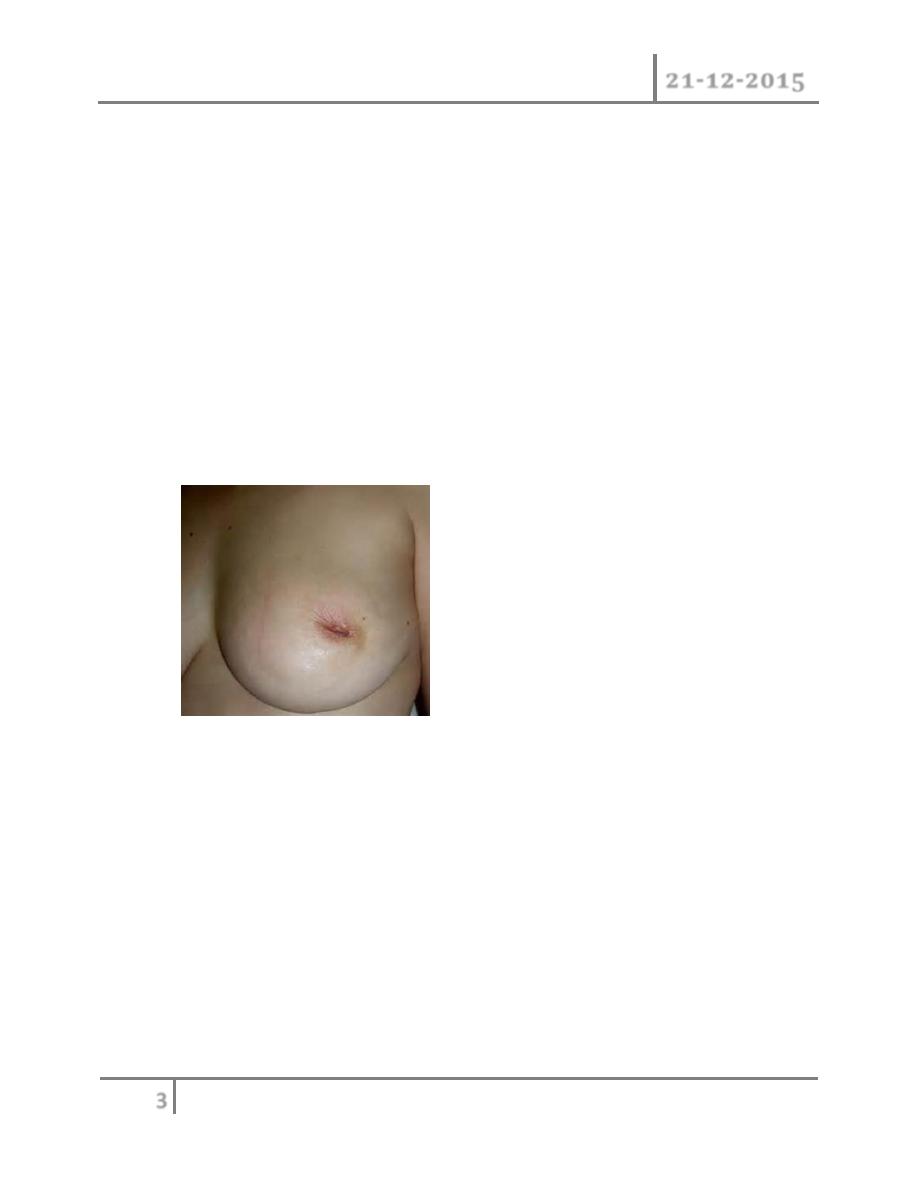
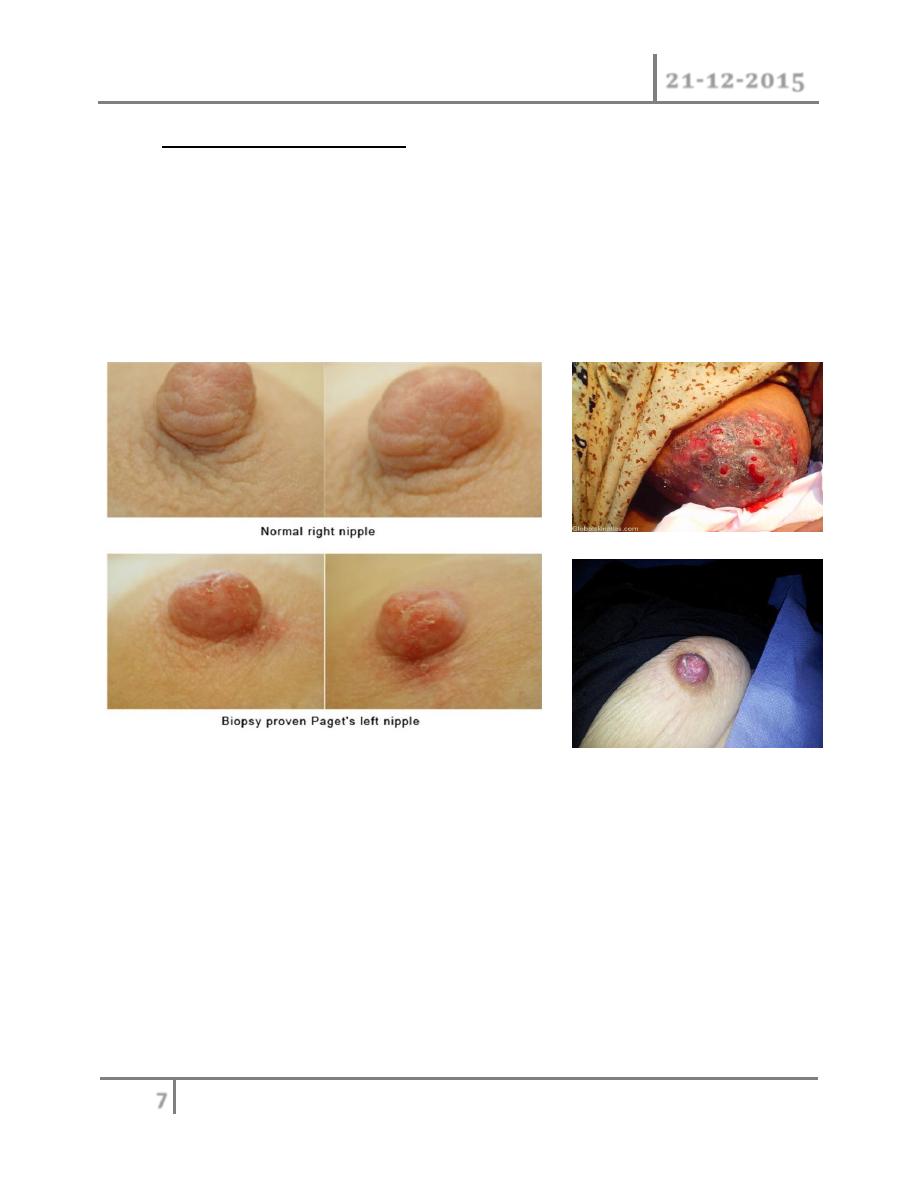
Paget's disease of the nipple: is a superficial manifestation of underlying
disease of the breast carcinoma. It presents as eczema- like condition of the
nipple and areola which persists despite local treatment. The nipple is
eroded slowly and eventually disappears. If it left the underlying carcinoma
will sooner or later become clinically evident. Nipple eczema should
biopsied if there any doubt of its cause. Microscopically Paget's disease
characterized by the presence of a large ovoid cells with abundant, clear,
pale staining cytoplasm in malpighian layer of the epithelium.
CLASSIFICATIONS
1- DUCTAL CARCINOMA
LOBULAR CARCINOMA
2-
(a) In Situ Carcinoma
o DUCTAL CARCINOMA IN-SITU (DCIS)
o LOBULAR CARCINOMA IN-SITU (LCIS)
(b)Invasive carcinoma.
o Invasive ductal carcinoma.
o Invasive lobular carcinoma.
Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
8
©Ali Kareem 2015-2016
TYPES
1) Scirrhous carcinoma:60% common
2) Medullary carcinoma:also called “encephaloid type”
3) Inflammatory carcinoma/lacatating carcinoma/mastitis carcinoma:most
malignant type
4) Colloid carcinoma:produces abundant mucin
5) Paget’s disease of nipples
6) Tubular, Papillary, Cribriform of ductal carcinoma.
7) Atypical Scirrhous carcinoma
8) Lobular insitu carcinoma
Spread of the breast cancer :
1) Local spread : the tumor increases in size and invade other portion of the
breast. It tends to involve the skin and to penetrate the pectorals muscles
and even the chest wall if diagnosed later.
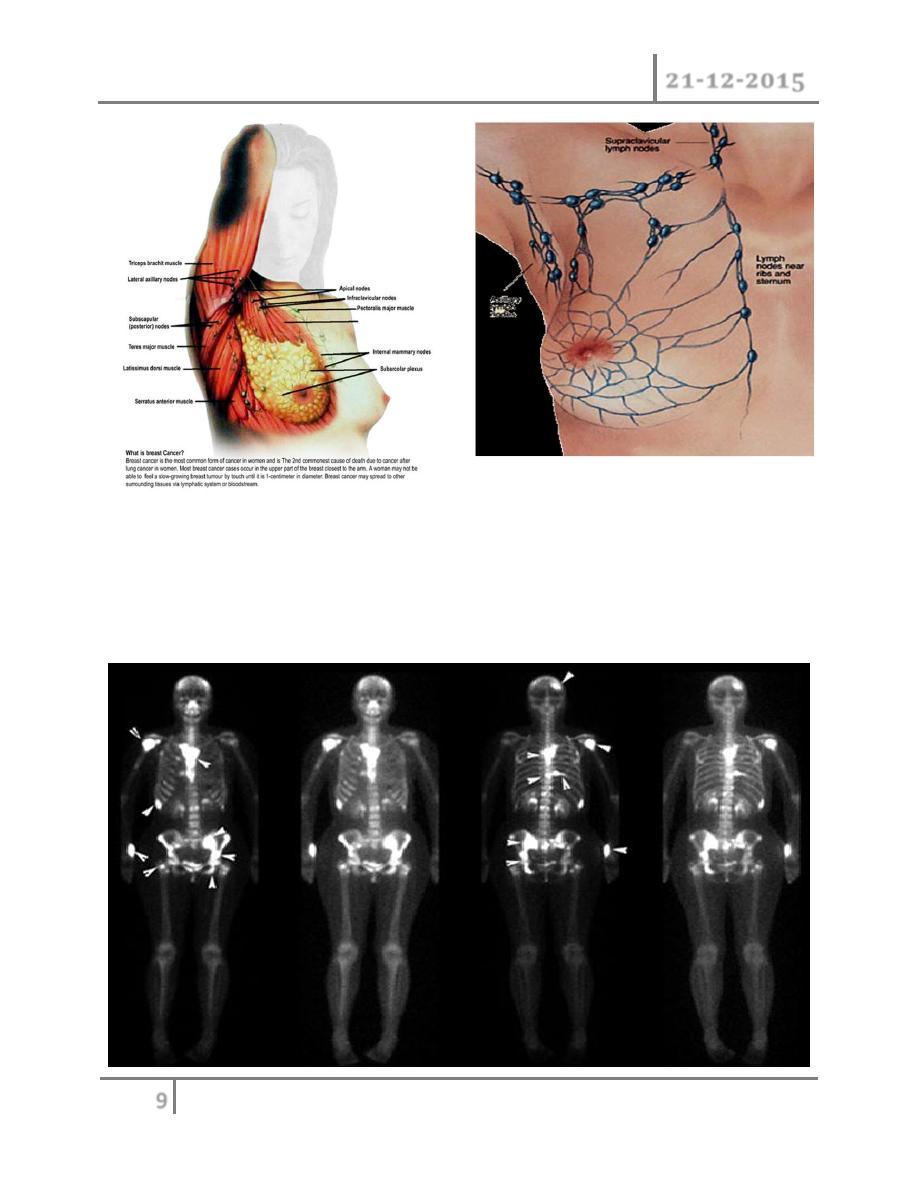
2) Lymphatic metastasis : it occurs primarily to axillary and internal
mammary lymph nodes. A tumor in the posterior one third tends to spread to
internal mammary lymph nodes. The involvements of lymph nodes have both
biological and chronological event in the spread of carcinoma and it also a
marker of metastases potential of that tumor. Involvement of the
supraclavicular lymph nodes and of any of the contra lateral breast
represents advanced disease.
Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
9
©Ali Kareem 2015-2016
3) Blood streams : it is by this route skeletal metastases occur. In order of the
frequency the lumbar vertebrae, femur, thoracic vertebrae, rib and skull are
affected and these deposits are generally osteolytic. Metastases may also
commonly occur in the liver, lung, brain, and occasionally adrenal glands
and ovaries.

Diseases of Breast Dr. Tariq Al-Obaidi
21-12-2015
10
©Ali Kareem 2015-2016
END …