Baghdad College of Medicine / 4
th
grade
Student’s Name :
Dr. Mohammed Basil
Lec. 2
Pediatric Urology
Thurs. 17 / 3 / 2016
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016
Pediatric Urology Dr. Mohammed Basil
17-3-2016
2
©Ali Kareem 2015-2016
Pediatric Urology
Undescended testes
o The testes descend into the scrotum in the third trimester (passing through
the inguinal canal at 24–28 weeks). Failure of testicular descent results in
cryptorchidism (or undescended testes).
o Incidence is 3% at birth (unilateral > bilateral). Approximately 80% will
spontaneously descend by 3 months. The incidence at 1 year is 1%.
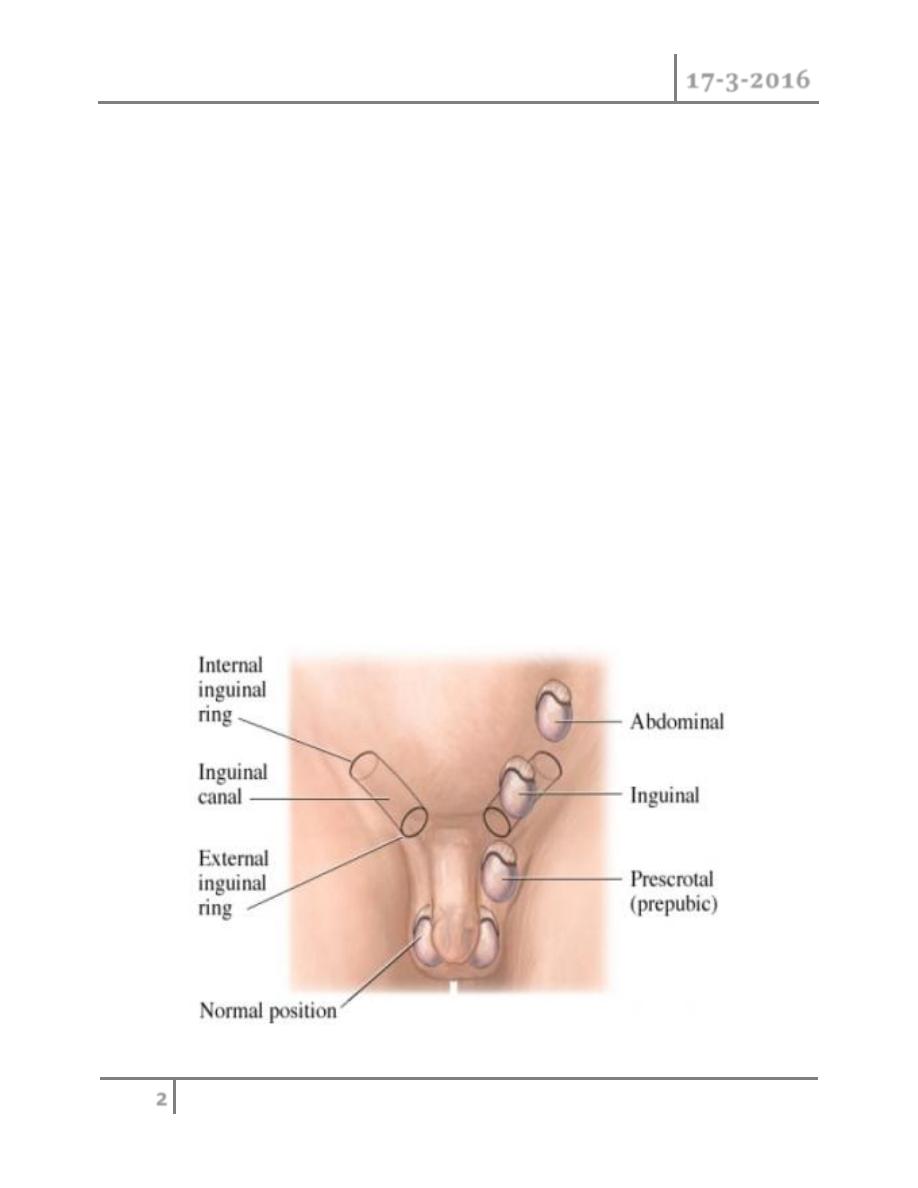
o Classification
Retractile: an intermittent active cremasteric reflex causes the testis
to retract up and out of the scrotum.
Ectopic (<5%): abnormal testis migration below the external ring of
the inguinal canal (to perineum, base of penis, or femoral areas)
Incomplete descent (~95%): testis may be intra-abdominal,
inguinal,or prescrotal
Atrophic/absent

Pediatric Urology Dr. Mohammed Basil
17-3-2016
3
©Ali Kareem 2015-2016
Risk factors
o These include preterm infants, low birth weight, small for gestational age,
and twins.
Etiology
o This includes abnormal testis or gubernaculum (tissue that guides the testis
into the scrotum during development); endocrine abnormalities (low level of
androgens, human chorionic gonadotrophin [hCG], luteinizing hormone
(LH), calcitonin gene–related peptide); and decreased intraabdominal
pressure (prune-belly syndrome, gastroschisis).
Pathology
o There is degeneration of Sertoli cells, loss of Leydig cells, and atrophy and
abnormal spermatogenesis.
Long-term complications
o Relative risk of cancer is 40-fold higher in the undescended testis. Most are
seminomas; carcinoma in situ represents a small percentage (~2%).There is
a slightly increased risk of cancer in the contralateral, normally descended
testis.
o Reduced fertility
o Increased risk of testicular torsion
o Increased risk of direct inguinal hernias (due to a patent processus
vaginalis)
Management
o Full examination is required to elucidate if the testis is palpable and to
identify location. Assess for associated congenital defects. If neither testis is
palpable, consider chromosome analysis (to exclude an androgenized
female) and hormone testing (high LH and FSH with a low testosterone
indicates anorchia).
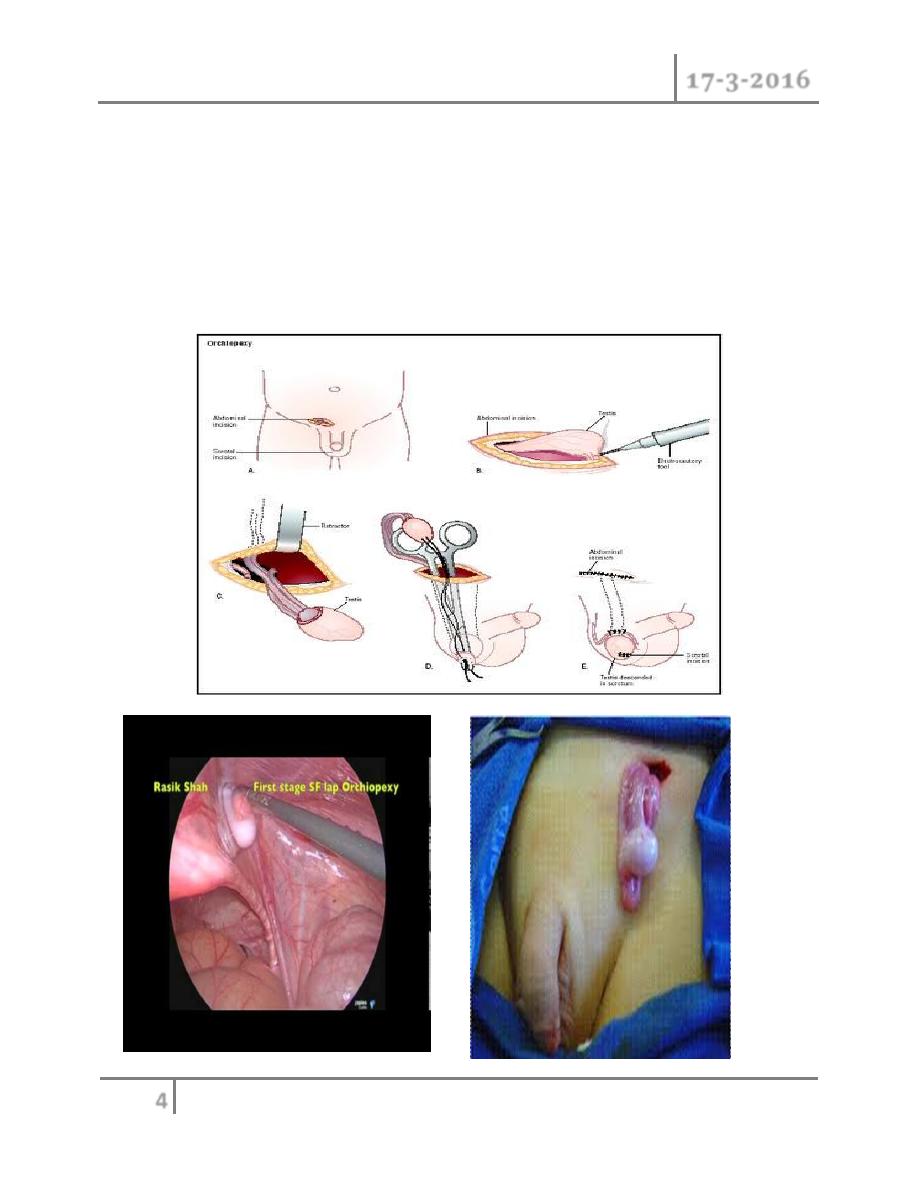
o Treatment should be performed within the first year. Hormone therapy
(hCG, LHRH) stimulates testosterone production. Surgery consists of
Pediatric Urology Dr. Mohammed Basil
17-3-2016
4
©Ali Kareem 2015-2016
inguinal exploration, mobilization of spermatic cord, ligation of processus
vaginalis, and securing the testis into a dartos pouch in the scrotal wall
(orchidopexy). Laparoscopy can be used in planning surgery and for
treatment. Intra-abdominal testes may require division of spermatic vessels
to provide extra length (Fowler-Stevens procedure, relying on collateral
blood flow from vas), two-stage procedures, or microvascular
autotransplantation.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
5
©Ali Kareem 2015-2016
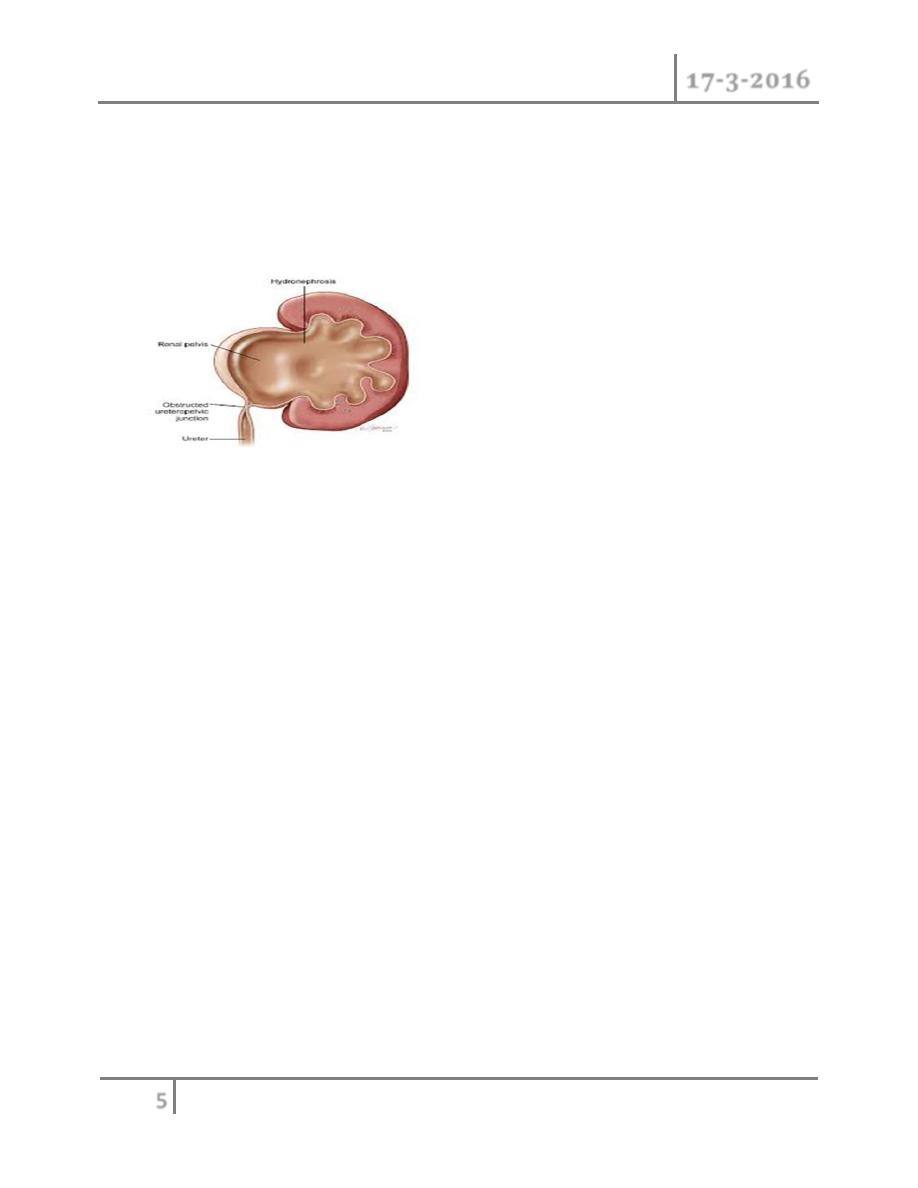
Pelviureteric junction (PUJ) obstruction
o A ureteropelvic junction (UPJ) obstruction can be thought of as a restriction
to flow of urine, from the renal pelvis to the ureter, which, if left
uncorrected, will lead to progressive renal deterioration
o UPJ obstruction occurs in all pediatric age groups, but there tends to be a
clustering in the neonatal period because of the detection of antenatal
hydronephrosis and again later in life because of symptomatic occurrence.
At one point about 25% of cases were discovered within the first year of life.
o UPJ obstruction is the most common cause of significant dilation of the
collecting system in the fetal kidney.
o Obstruction occurs more commonly in boys than in girls.
o Left-sided lesions predominate, particularly in the neonate (approximately
67%).
o Bilateral UPJ obstruction is present in 10% to 40% of cases and it has been
known to affect members of more than one generation.
ETIOLOGY
Intrinsic :
o Interruption in the development of the circular musculature of the UPJ.
o Or an alteration of the collagen fibers and composition between and around
the muscle cells (The muscle fibers become widely separated and attenuated,
leading to a functional discontinuity of the muscular contractions and
ultimately to insufficient emptying) .
o A significant increase in the lamina muscularis and in the number of inner
longitudinal muscular bundles of the UPJ complex of obstructed kidneys in

Pediatric Urology Dr. Mohammed Basil
17-3-2016
6
©Ali Kareem 2015-2016
infants younger than 1 year of age, compared with age-matched normal
infants
o Valvular mucosal folds.
o Persistent fetal convolutions .
o Upper ureteral polyps.
o Such folds that does not flatten out when the ureter is distended or
stretched.
o "östling's folds" are now considered folds that are not obstructive and
disappear with a person's lineargrowth they are rarely seen in an older
child or adult.
Extrinsic :
o An aberrant, accessory, or early-branching lower-pole vessel is the most
common cause of extrinsic UPJ obstruction. These vessels pass anteriorly to
the UPJ or proximal ureter and contribute to mechanical obstruction.
o An aberrant or accessory renal artery to the lower pole of the kidney is
present and the ureter courses behind it, the ureter may angulate at both the
UPJ and the point at which it traverses over the vessel as the pelvis fills and
bulges anteriorly. Further angulation of the ureter occurs as it becomes
adherent to the UPJ secondary to an inflammatory process. A two-point
obstruction ensues, with kinking of the ureter at the UPJ and at the point
where the ureter drapes over the vessel.
Secondary Ureteral Pelvic Junction Obstruction
o UPJ obstruction may also be seen with severe vesicoureteral reflux (VUR);
these conditions coexist in 10% of cases. The ureter elongates and develops
a tortuous course in response to the obstructive element of reflux. A kink
may develop in the UPJ area, a point of relative fixation, and may cause
obstruction secondarily . In such a situation the obstructive lesion needs to
be corrected initially, even though the VUR contributed to the initial
problem.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
7
©Ali Kareem 2015-2016
Associated Anomalies
o UPJ obstruction is the most common anomaly encountered in the opposite
kidney; it occurs in 10% to 40% of cases.
o Renal dysplasia and multicystic dysplastic kidney are the next most
frequently observed contralateral lesions.
o In addition, unilateral renal agenesis has been noted in almost 5% of
children.
o UPJ obstruction may also occur in either the upper or the lower half
(usually the latter) of a duplicated collecting system,or of a horseshoe or
ectopic kidney.
o VUR has been found in as many as 40% of affected children.
o UPJ obstruction was noted in 21% of children with the VATER (vertebral
defects, imperforate anus, tracheoesophageal fistula, and radial and renal
dysplasia) association.
PRESENTATION
o most infants are asymptomatic and most children are discovered because of
their symptoms. infants were discovered to have UPJ obstruction because of
a palpable mass.
o infants who present with failure to thrive, feeding difficulties, sepsis
secondary to urinary tract infection, or pain or hematuria related to
nephrolithiasis. Urinary tract infection is the presenting sign in 30% of
affected children beyond the neonatal period.
o In the older child, episodic flank or upper abdominal pain, sometimes
associated with nausea and vomiting due to intermittent UPJ obstruction, is
a prominent symptom.
o cyclic vomiting alone is caused by intermittent UPJ obstruction.
o Hematuria, which is seen in 25% of children, may occur after minor
abdominal trauma.
o This hematuria is believed to be caused by disruption and rupture of
mucosal vessels in the dilated collecting system.

Pediatric Urology Dr. Mohammed Basil
17-3-2016
8
©Ali Kareem 2015-2016
o In the young adult, episodic flank or abdominal pain, particularly during
diuresis, is a common manifestation. Occasionally, a patient with the UPJ
obstruction presents with hypertension. The pathophysiology is thought to be
a functional ischemia with reduced blood flow caused by the enlarged
collecting system that produces a renin-mediated hypertension .
DIAGNOSIS
o Ultrasonography; is the standard method for identifying hydronephrosis in
infancy. Postnatal ultrasound imaging is usually deferred until day 3 of life,
to allow for improvement in the relative oliguria, which could lead to
underestimation of the degree of hydronephrosis.
o If prenatal US has shown a large or bilateral hydronephrosis, a follow-up
renal tract ultrasound scan should be performed soon after birth. If there is
a prenatal unilateral hydronephrosis (and the bladder is normal), the scan is
deferred until days 3–7 (to allow normal physiological diuresis to occur,
which may spontaneously improve or resolve hydronephrosis).
o If upper tract obstruction persists, a voiding cystourethrogram (VCUG) is
indicated (to rule out VUR and examine for posterior urethral valves), and a
renogram can assess individual renal function and drainage (DTPA,
MAG-3).
IVU
Pediatric Urology Dr. Mohammed Basil
17-3-2016
9
©Ali Kareem 2015-2016
o CT
Treatment
o Children may be observed with US and renogram if they remain stable and
have good renal function and no other complications (such as persistent
infection or stones).
o If children are symptomatic or have a signifi cant hydronephrosis with
impaired renal function (<40%), pyeloplasty is recommended
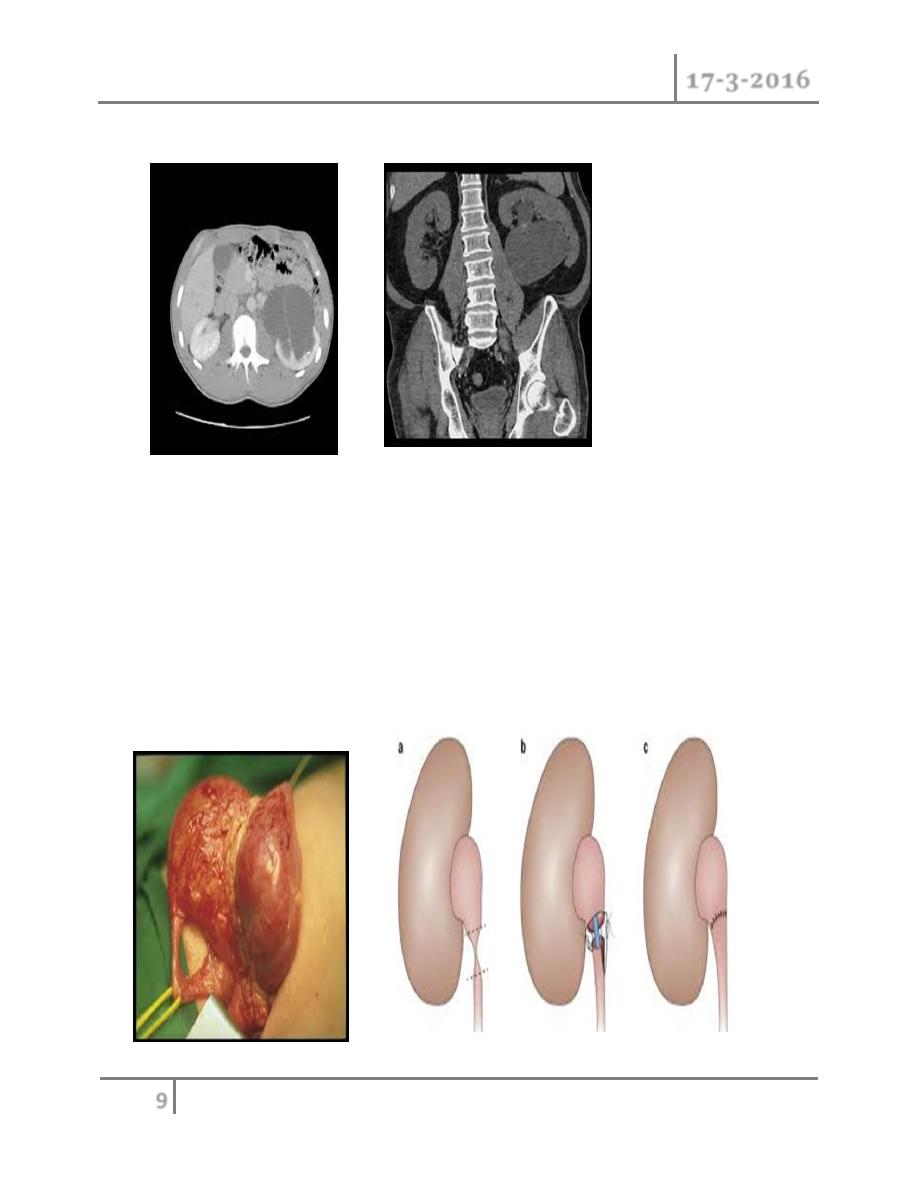
PYELOPLASTY
Pediatric Urology Dr. Mohammed Basil
17-3-2016
10
©Ali Kareem 2015-2016
Vesicoureteric reflux (VUR)
o VUR results from abnormal retrograde flow of urine from the bladder into
the upper urinary tract.
Epidemiology
o Overall incidence in children is >10%, with younger children affected more
than older children, girls more than boys (female–male ratio 5:1). VUR
occurs more often in Caucasian than in Afro-Caribbean children.
o Siblings of an affected child have a 40% risk of reflux, and routine screening
of siblings is recommended.
Pathogenesis
o The ureter passes obliquely through the bladder wall (1–2 cm), where it is
supported by muscular attachments that prevent urine reflux during bladder
filling and voiding. The normal ratio of intramural ureteric length to
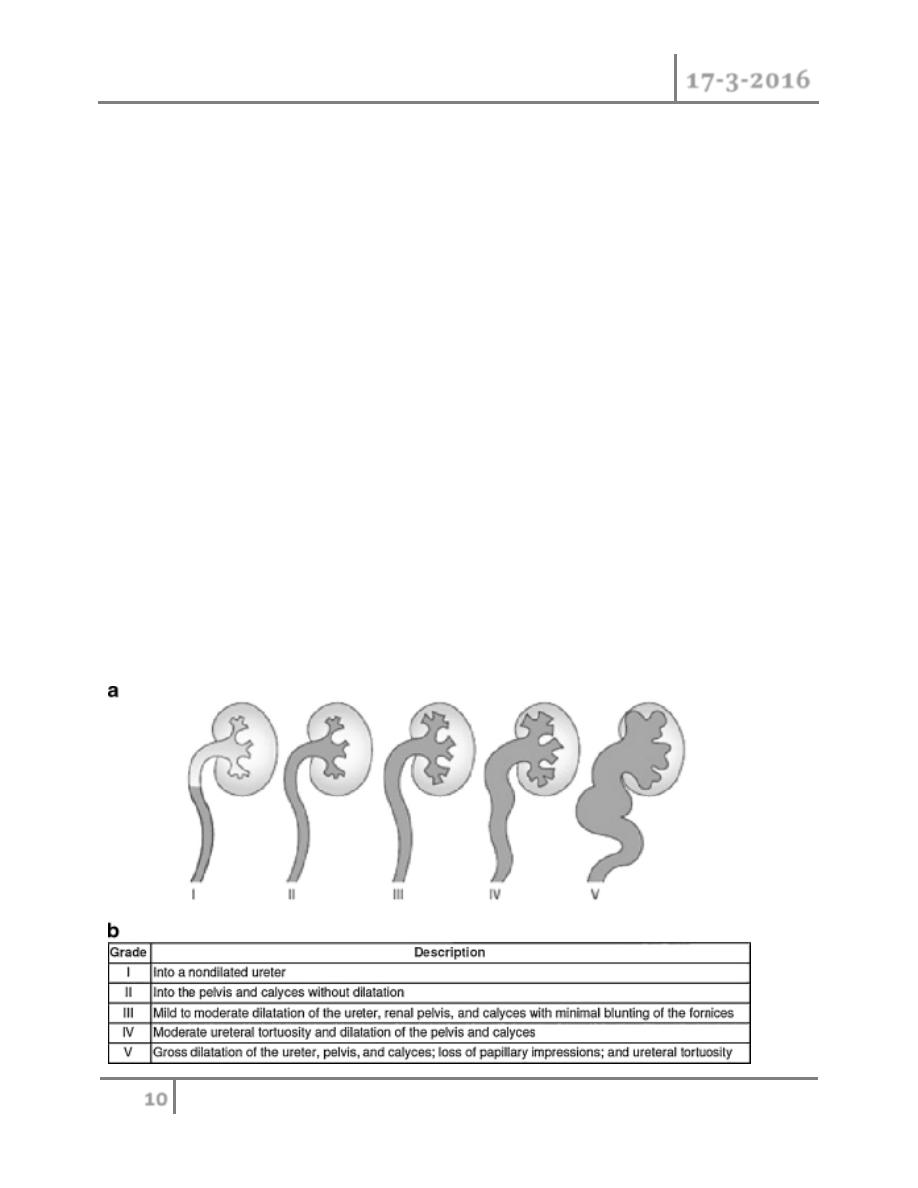
ureteric diameter is 5:1. Reflux occurs when the intramural length of ureter
is too short (ratio<5:1). The degree of reflux is graded I–V . The
appearance of the ureteric orifice changes with increasing severity of reflux,
classically described as stadium, horseshoe, golf-hole, or patulous.

Pediatric Urology Dr. Mohammed Basil
17-3-2016
11
©Ali Kareem 2015-2016
Classification
o Primary reflux (1%) results from a congenital abnormality of the
ureterovesical junction.
o Secondary refl ux results from urinary tract dysfunction associated with
elevated intravesical pressures. Causes include posterior urethral valves
(reflux seen in 50%), urethral stenosis, neuropathic bladder, and detrusor
sphincter dyssynergia (DSD).
o VUR is also seen with duplex ureters. The Weigert–Meyer rule states that
the lower-pole ureter enters the bladder proximally and laterally, resulting
in a shorter intramural tunnel, which predisposes to reflux.
Complications
o VUR associated with UTI can result in refl ux nephropathy with
hypertension and progressive renal failure.
Presentation
o Patients have symptoms of UTI, fever, dysuria, suprapubic or abdominal
pain, failure to thrive, vomiting, and diarrhea.
Investigation
o Urinalysis and culture to diagnose UTI
o Urinary tract ultrasound scan and VCUG to diagnose and grade reflux and
establish reversible causes .
o Urodynamic assessment if suspicious of voiding dysfunction
o DMSA scan to detect and monitor associated renal cortical scarring.
Management
o Correct problems contributing to secondary reflux. Most primary VUR
grade I–II cases will resolve spontaneously (~85%), with 50% resolution in
grade III. Observation and medical treatment are initially recommended.
Medical treatment
Pediatric Urology Dr. Mohammed Basil
17-3-2016
12
©Ali Kareem 2015-2016
o Low-dose antibiotic prophylaxis should be given to keep the urine sterile
and lower the risk of renal damage until refl ux resolves. Anticholinergic
drugs are given to treat bladder overactivity.
Typical indications for antireflux surgery include
1. Breakthrough UTIs despite prophylactic antibiotics
2. Noncompliance with medical management
3. Severe grades of reflux (grade IV or V), especially with pyelonephritic
changes
4. Failure of renal growth, new renal scars, or deterioration of renal function
on serial ultrasounds or scans
5. Reflux that persists in girls as full linear growth is approached at puberty
6. Reflux associated with congenital abnormalities at the UVJ (e.g., bladder
diverticula)
o Surgery is indicated for severe refl ux, breakthrough UTIs, evidence of
o progressive renal scarring, and VUR that persists after puberty.
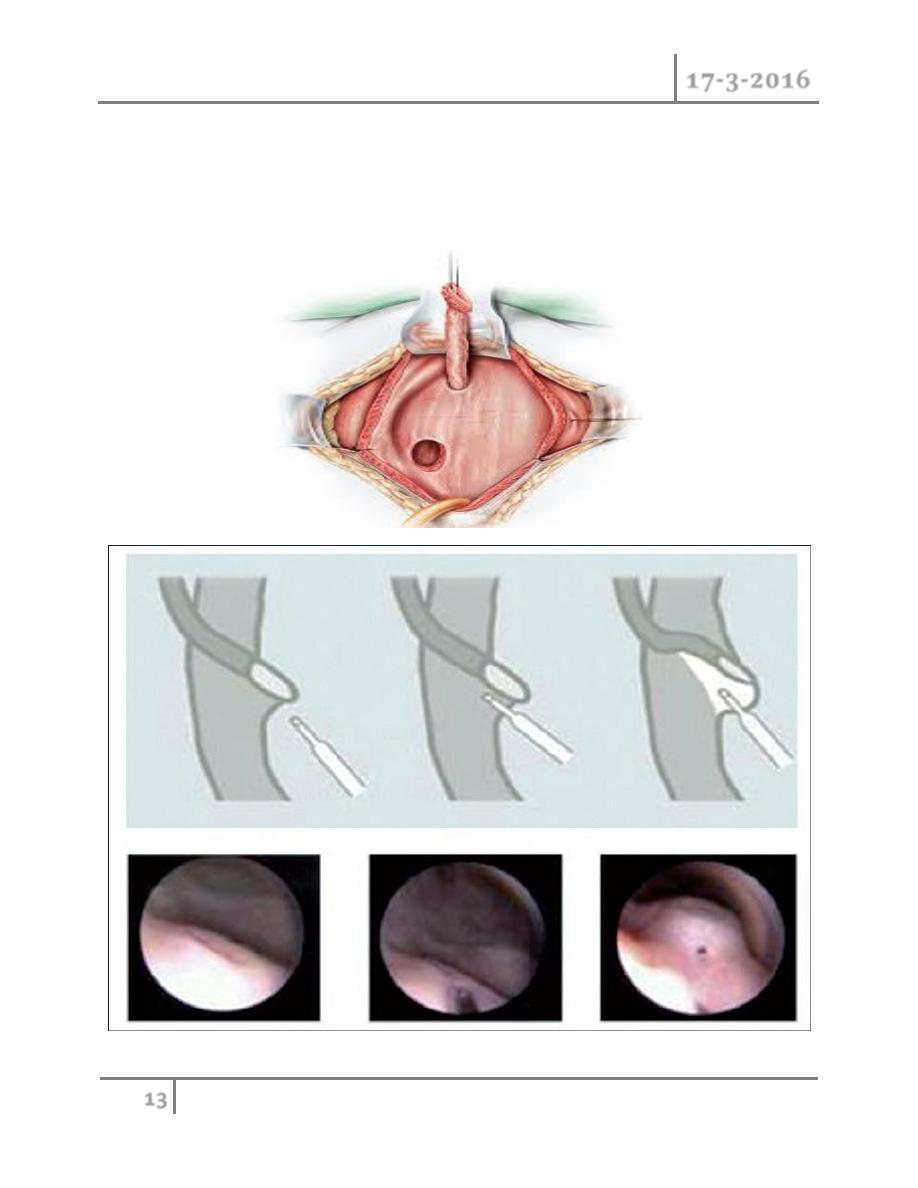
Techniques of ureteral re-implantation include the following:
o Intravesical methods involve mobilizing the ureter and advancing it across
the trigone (Cohen repair) or reinsertion into a higher, medial position in
the bladder (Politano–Leadbetter repair).
Pediatric Urology Dr. Mohammed Basil
17-3-2016
13
©Ali Kareem 2015-2016
o Extravesical techniques involve attaching the ureter into the bladder base
and suturing muscle around it (Lich–Gregoir procedure).
o Alternatively, endoscopic subtrigonal injection of Defl ux into the ureteral
orifi ce has 70% success, and 95% with repeated treatments.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
14
©Ali Kareem 2015-2016
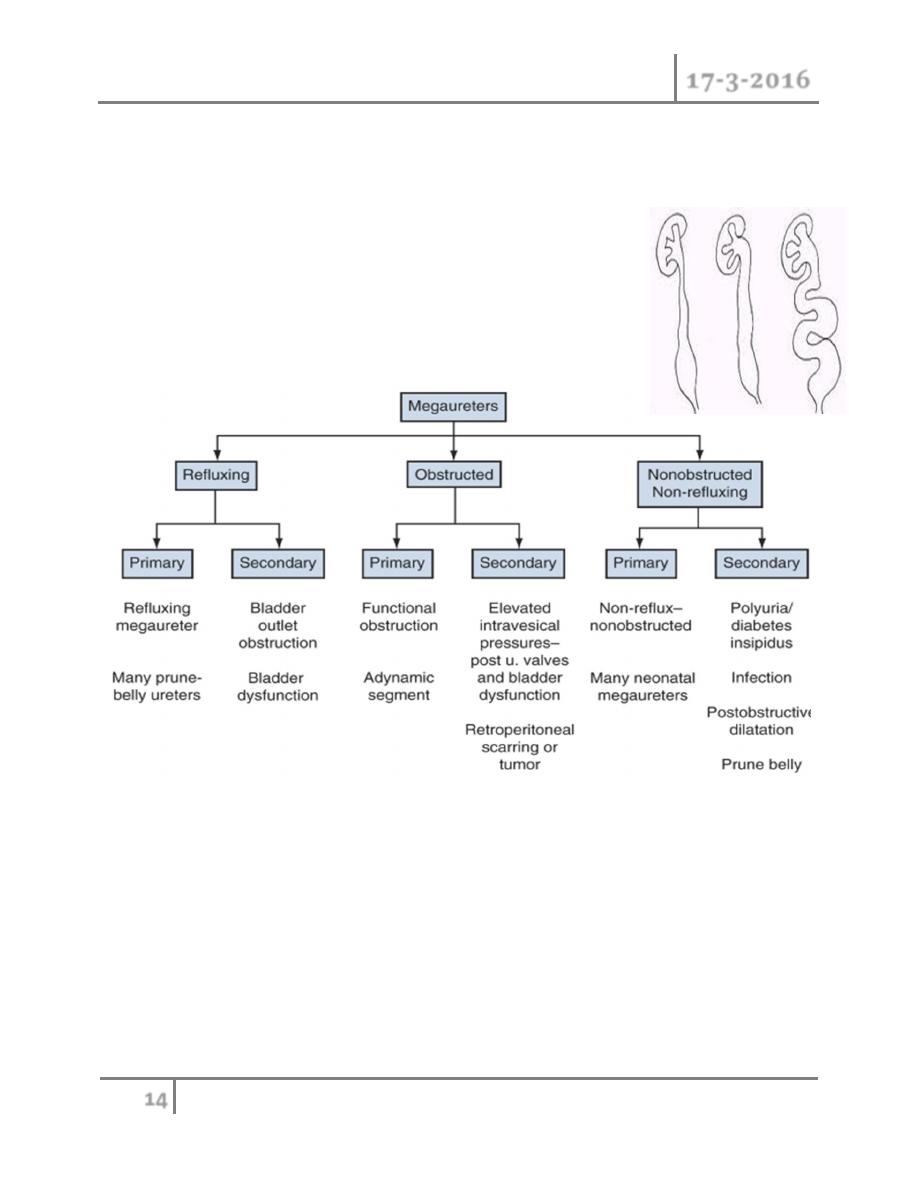
MEGAURETER
o MGU is a nonspecific term implying a spectrum of anomalies associated
with pathologically excessive ureteral diameter
o Children up to 12 year-ureteral width>7mm
o Older children ureteral width>10mm
Classification
Presentation
o Bilateral in approximately 25% of patients .
o In up to 10% to 15% of children the contralateral kidney may be absent or
dysplastic .
o UTIs, abdominal pain, or hematuria.
o The diagnosis may be made later in life in some asymptomatic patients.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
15
©Ali Kareem 2015-2016
Pathophysiology
o The distal end of the ureter, as it becomes intramural and subsequently
submucosal, rearranges the muscular layers in its wall. All layers become
longitudinally oriented, and the ureteral adventitia fuses to the bladder
trigone .
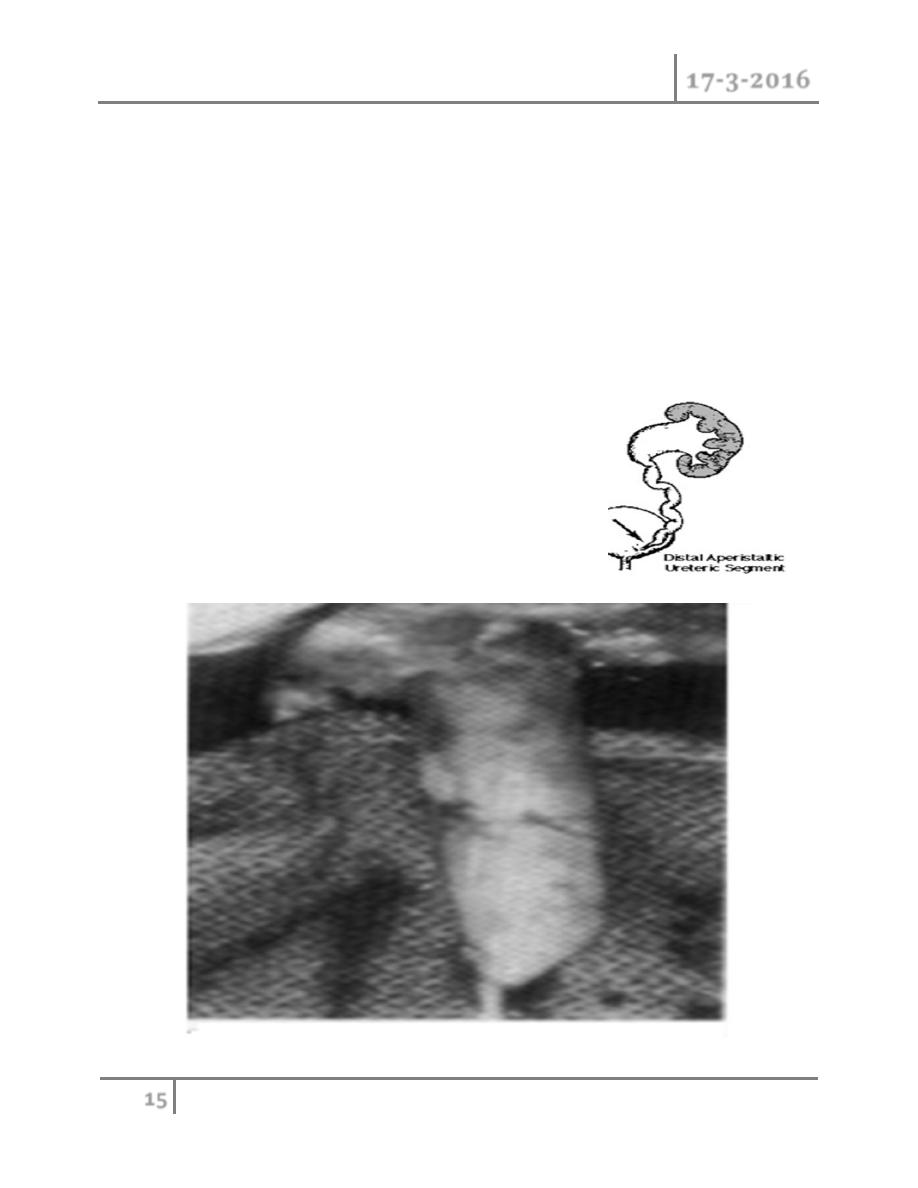
Primary Obstructive Megaureter
o The precise etiology of primary obstructive MGU remains unclear, it is
generally agreed that the most common finding is an
aperistaltic juxtavesical (adynamic) ureteral
segment that prevents urine from flowing
at an acceptable rate ,and functional
obstruction results
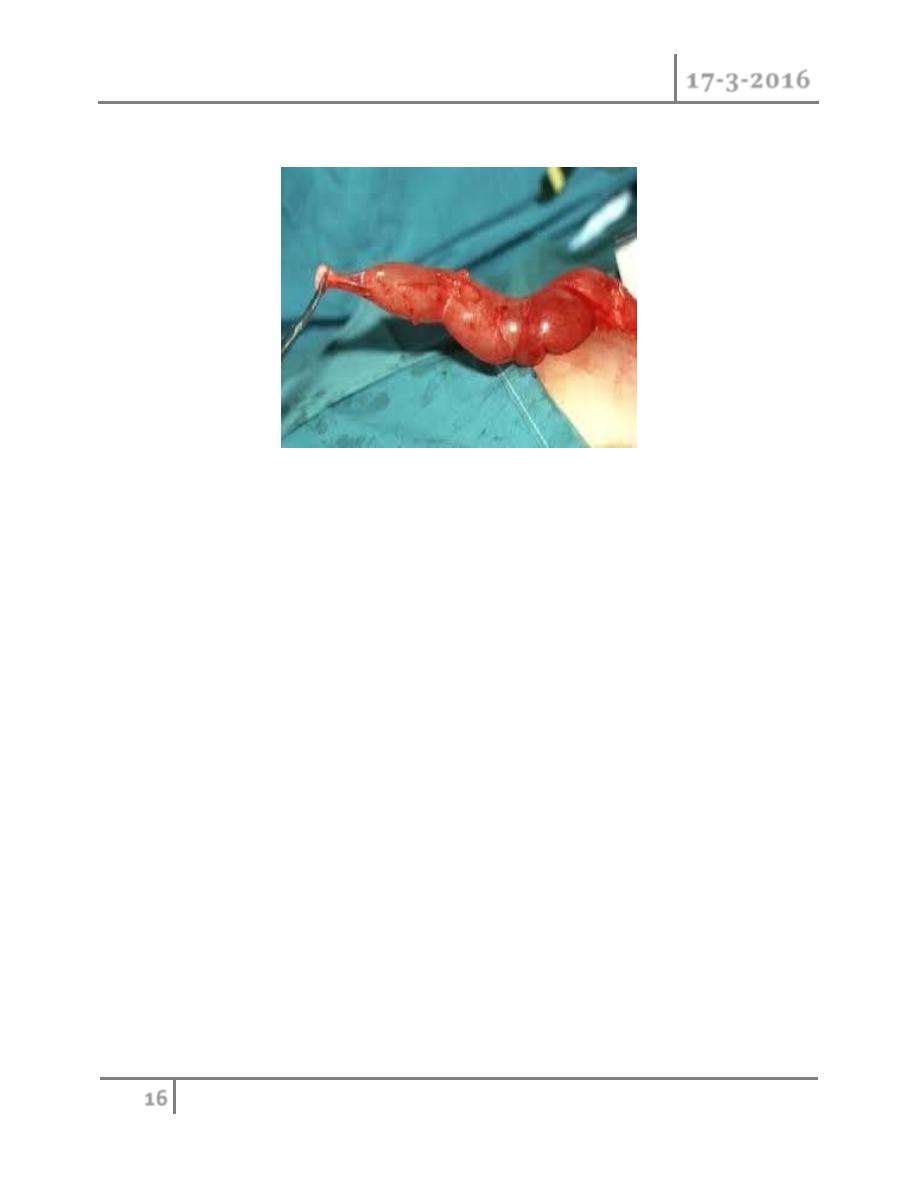
Operative exposure a dynamic segment
Pediatric Urology Dr. Mohammed Basil
17-3-2016
16
©Ali Kareem 2015-2016
TREATMENT
Penile and Urethral disorders
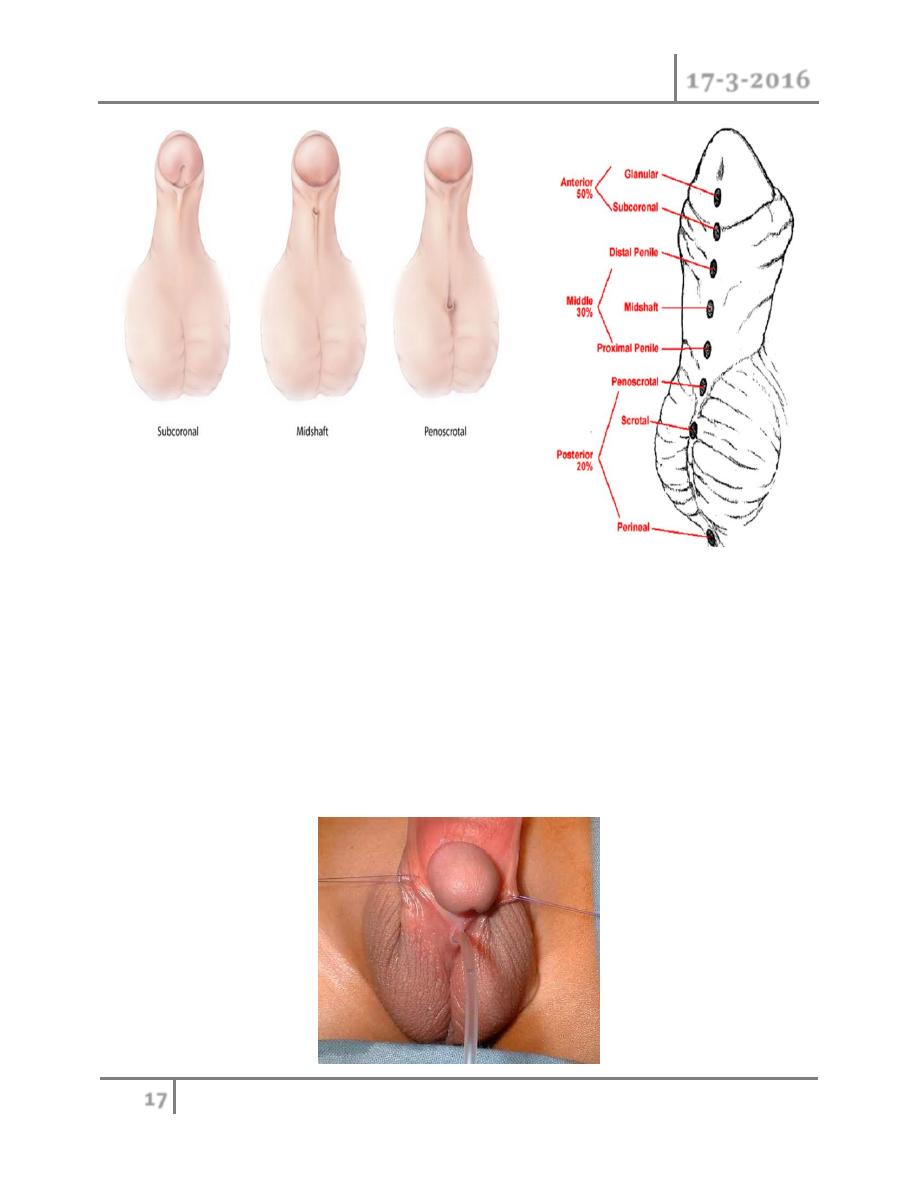
Hypospadias
Classification
Hypospadias can be classified according to the anatomical location of the urethral
meatus .
o Anterior (or distal)—glandular, coronal, and subcoronal (~50%)
o Middle—distal penile, midshaft, and proximal penile (~30%)
o Posterior (or proximal)—penoscrotal, scrotal, and perineal (~20%)
Pediatric Urology Dr. Mohammed Basil
17-3-2016
17
©Ali Kareem 2015-2016
Etiology
o Hypospadias results from incomplete closure of urethral folds on the
underside of the penis .
o Chordee is caused by abnormal urethral plate development.
o and the hooded foreskin is due to failed formation of the glandular urethra
and fusion of the preputial folds.
o A full clinical examination will make the diagnosis. However, it is also
important to seek out associated abnormalities that will need treatment.
o Patients with absent testes and severe hypospadias should undergo
chromosomal and endocrine investigation to exclude intersex conditions.

Pediatric Urology Dr. Mohammed Basil
17-3-2016
18
©Ali Kareem 2015-2016
Treatment
o Surgery is indicated where deformity is severe, interferes with voiding, OR is
predicted to interfere with sexual function. Surgery is now performed
between 6 and 12 months of age. The aim of surgery is to correct penile
curvature (orthoplasty), reconstruct a new urethra, and bring the new
meatus to the tip of the glans.Severe cases may require staged procedures.
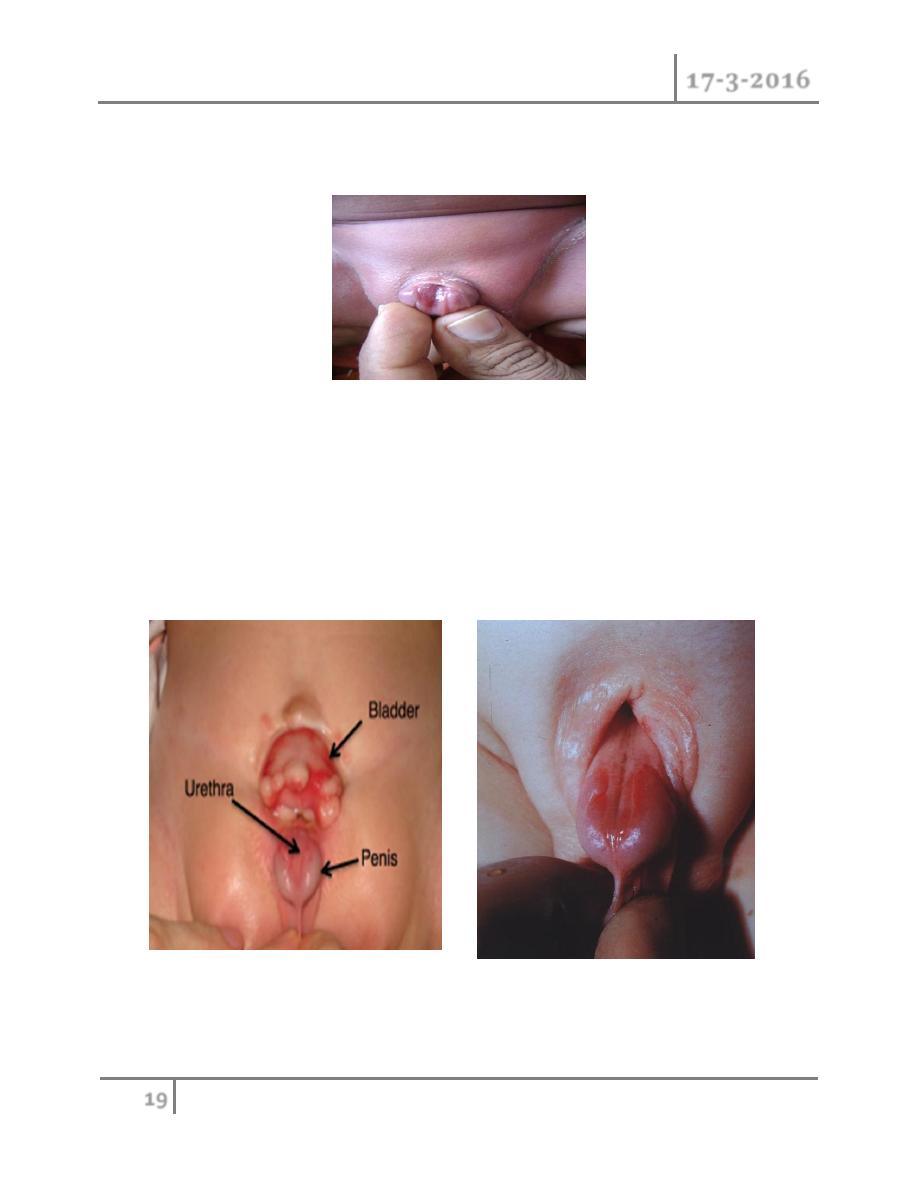
Epispadias
o In epispadias, the urethra opens onto the dorsal surface of the penis,
anywhere from the glans, penile shaft, or, most commonly, the penopubic
region. An incomplete urethral sphincter mechanism results in a high risk of
incontinence.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
19
©Ali Kareem 2015-2016
o Epispadias is also associated with dorsal chordee , with incomplete foreskin
dorsally. Epispadias is part of the exstrophy–epispadias complex
Associated anomalies
o Diastasis of the symphysis pubis results in splaying of the corpora
cavernosa and shortening of the penile shaft. Females have a bifid clitoris
and poorly developed labia and demonstrate a spectrum of urethral
deformities ranging from a patulous urethral orifice to a urethral cleft
affecting the entire length of the urethra and sphincter.
o There is a 40% risk of vesicoureteric reflux (VUR).

Pediatric Urology Dr. Mohammed Basil
17-3-2016
20
©Ali Kareem 2015-2016
Incidence
o Epispadias affects 1 in 117,000 males. It is rarely seen in females (male–
female ratio is 5:1).
Treatment
o This involves urethroplasty with functional and cosmetic reconstruction of
the external genitalia (penile lengthening and correction of chordee)at 6–12
months.
o From age 4–5 years, when children can be toilet trained, bladder neck
reconstruction can be performed . This achieves continence, and any
bladder residuals may then be emptied by urethral catheterization. If this
surgery fails, insertion of artifi cial urinary sphincters .
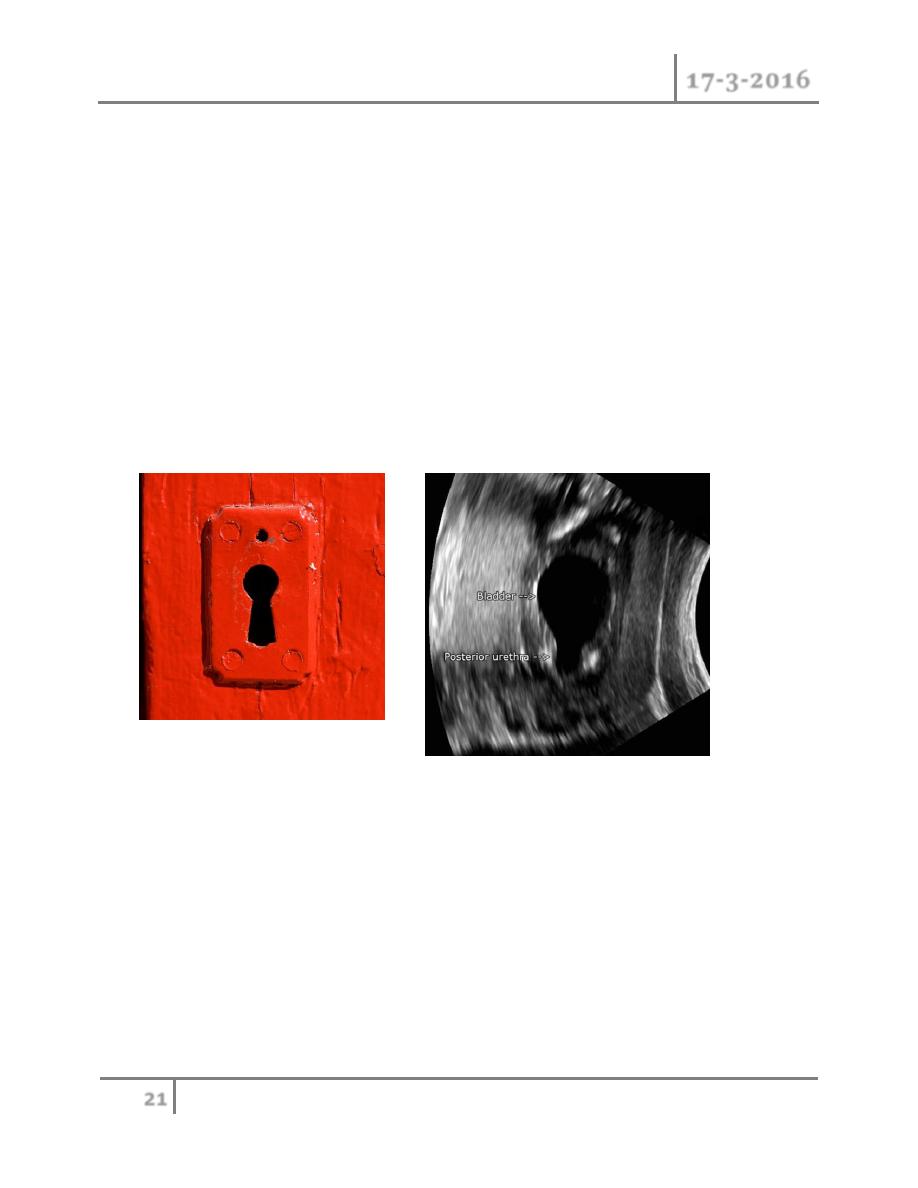
Posterior urethral valves
o Posterior urethral valves (PUV) are abnormal congenital mucosal folds in
the prostatic (posterior) urethra causing lower urinary tract obstruction.
Classification
o Type I (90–95%): Membranes arise from the distal lateral aspect of the
verumontanum,1 which extend distally and anteriorly to fuse in the midline.
o Type II: Longitudinal folds extending from the verumontanum to bladder
neck .
o Type III (5%): A ring-like membrane found distal to the verumontanum
Incidence is 1 in >5000 males.
Etiology
o Normal male urethra has small, paired lateral folds
found between the lateral, distal edge of verumontanum
and lateral urethral wall.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
21
©Ali Kareem 2015-2016
o PUVs probably represent a congenital overgrowth of these folds from
abnormal insertion of Wolffi an ducts into the posterior urethra during fetal
development.
Presentation
o Prenatal US features These include bilateral hydroureteronephrosis, dilated
bladder with elongated ectatic posterior urethra, thick-walled bladder,
oligohydramnios, and renal dysplasia.
o Newborn and infants
o These children have respiratory distress,palpable abdominal mass
(hydronephrotic kidney or distended bladder), ascites, UTI, electrolyte
abnormalities, and failure to thrive.
Older children
o Milder cases may present later with recurrent UTI, poor urinary
stream,incomplete bladder emptying, poor growth, and incontinence. There
is arisk of renal failure, vesicoureteric reflux, and voiding dysfunction
(overactive or underactive bladder), also described as valve bladder
syndrome.
Associated features
o POP-off valve syndrome is seen in 20%. It describes mechanisms by which
high urinary tract pressure is dissipated to allow normal renal development.
Pediatric Urology Dr. Mohammed Basil
17-3-2016
22
©Ali Kareem 2015-2016
It includes leaking of urine from small bladder or renal pelvis ruptures
(urinary ascites), reflux into a nonfunctioning kidney (vesicoureteral reflux
with renal dysplasia [VURD]), and formation of bladder diverticuli.
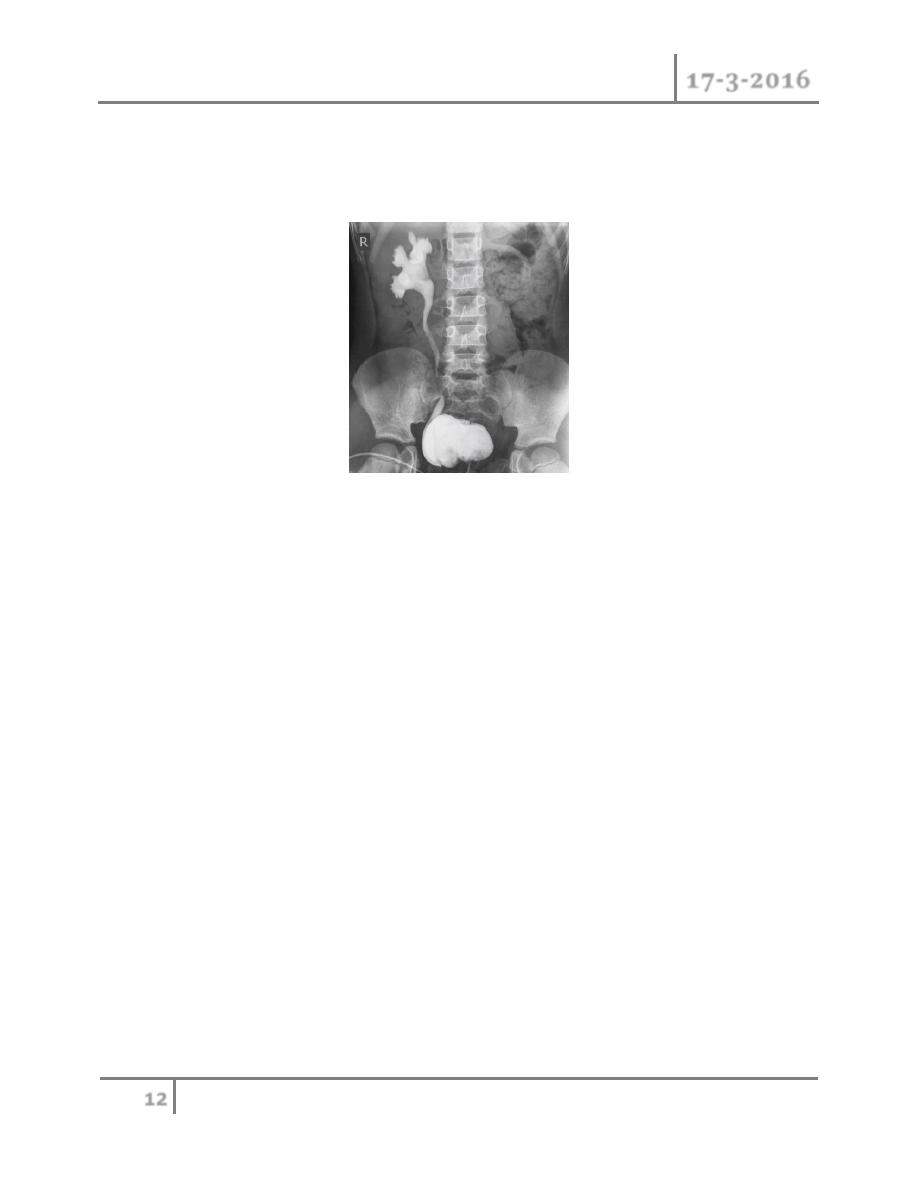
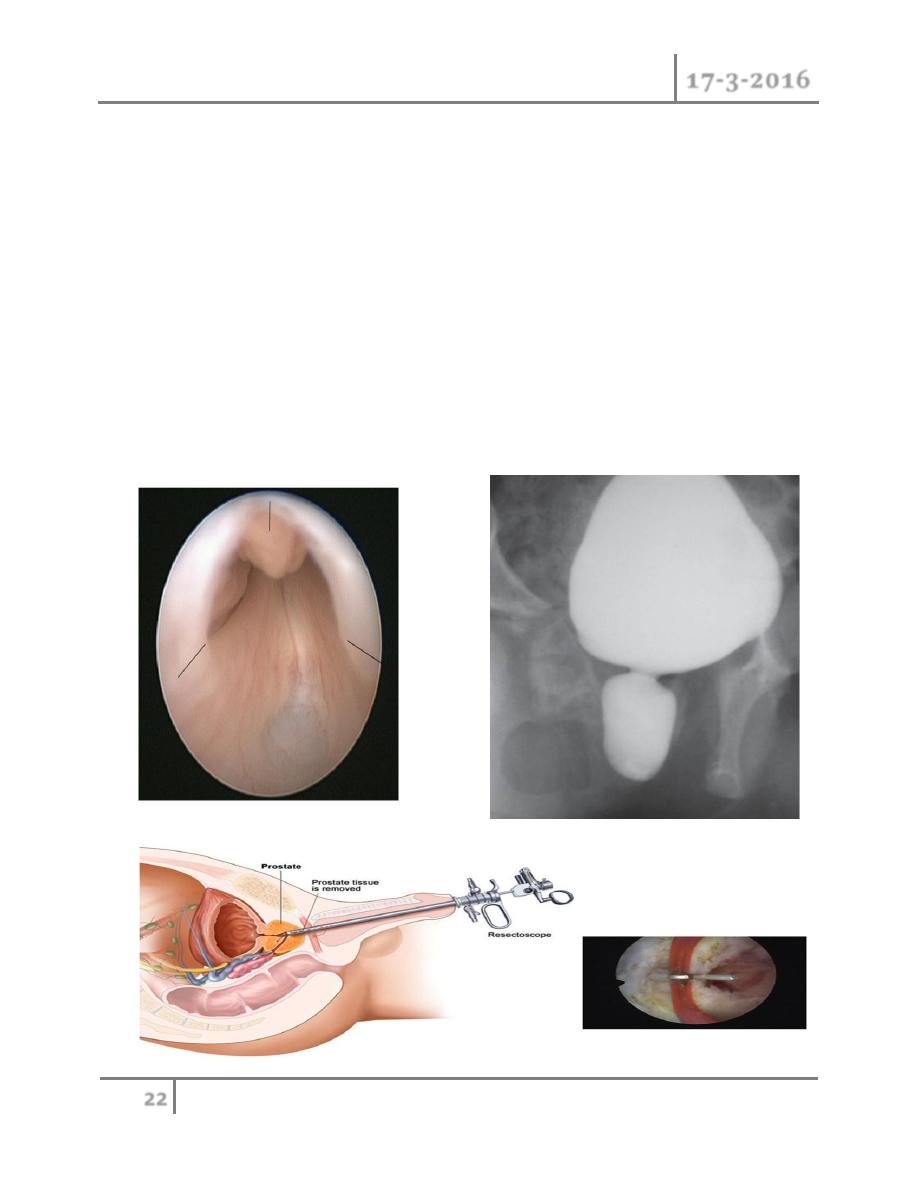
Investigation
o Ultrasound scan of kidneys and bladder.
o VCUG shows distended and elongated posterior urethra; partially filled
anterior urethra; bladder neck hypertrophy; lucencies representing valve
leaflets; thick-walled bladder (±diverticuli); incomplete bladder emptying;
reflux (50%).
o Isotope renal scan (MAG-3, DMSA) assesses renal function.
o Videourodynamics allows diagnosis of associated voiding dysfunction.

Pediatric Urology Dr. Mohammed Basil
17-3-2016
23
©Ali Kareem 2015-2016
Management
o Commence prophylactic antibiotics immediately, check serum electrolytes,
and drain the bladder with a pediatric feeding tube. If there is improvement,
cystoscopy and transurethral ablation of valve If upper tracts remain
dilated with raised creatinine after bladder drainage, a temporary
cutaneous vesicostomy is indicated.An alternative is ureterostomy drainage.
Valve ablation is performed at a later stage.
Prognosis
o Prognosis is 35% of patients will have poor renal function; 20% develop
end-stage renal failure.
Too much .. Too much !!
END OF THIS LECTURE …