Mohannad Al-Fallouji, PhD (London), FRCS, FRCSIUniversity Staff and Consultant SurgeonBaghdad’s Medical City Teaching HospitalsDirector: www.ihams.org
The Spleen


1992
19861998
Speaker’s Background
خلفية المحاضر
• I Love You (in Hebrew)

2012 - 2013
Magnum Opus1. To reveal the surgical anatomy and the applied physiology of the Spleen.
2. To know clinical differences between the Splenomegalyand tumour of the left kidney.
3. To be acquainted with indications for splenectomy.
4. To be acquainted with post-splenectomy complications.5. To sum it up in a clinical scenario of (splenic injury).
Objectives of SpleenSurgical Anatomy:
Location• It lies under the diaphragm in the left hypochondrium.
• It is summarised by (1, 3, 5, 7, 9, 11):
- it measures 1 X 3 X 5 inches (2.5 X 7.5 X 12.5 cm).
- it weighs 7 ounces (200 gm).
- it lies beneath the 9th - 11th ribs.
Surgical Anatomy:
RelationSpleen lies at the far left extremity of lesser sac under diaphragm.
It is related:- to pancreatic tail,
- splenic flexure of the colon,
- left kidney.
- diaphragm.
- 6 short gastric arteries (from splenic artery) supply
the fundus of the stomach.
Surgical Physiology: FISH(H)
Spleen is the largest lymphoid organ in the body.F: Filtration and removal of old, abnormal, and senescent RBCs and recycling iron as well as removal of encapsulated microorganisms مقبرة الخلايا.
I: Immunological functions (production of IgM and Opsonins)
S: Storage Pool functions (30% of total Platelets are located within spleen: it also receives 5% of total cardiac output approximately 150-300 ml/min so that each RBC averages 1000 passes through spleen each day).H: Haematopoiesis (usually in the developing foetus, but in adults only reactivated in myeloproliferative disorders that impair bone marrow to produce sufficient RBCs).
H: hormonally active? It has recently been evoked that the spleen has an endocrine function through the production of an immuno-potentiating peptide called (tuftsin).
Palpate from right iliac fossa upwards towards left hypochondrium.
Splenomegaly may be mistaken for left renal tumour.The following points will help in differentiation:
1. A renal tumour is bimanually palpable moving backwards and forwards between one hand on the loin behind, and the other on the anterior abdominal wall. Splenomegaly is not palpable bimanually.
2. Fingers can usually be passed between the kidney and the ribs but not between the ribs and splenomegaly.
3. The spleen has a sharp edge with a notch. The kidney edge always rounded and has no notch.
4. An enlarged kidney tends to bulge forwards. Peri-nephric abscesses bulge backwards. Splenomegaly bulges towards RIF.
5. Because of overlying colonic splenic flexure percussion on splenomegaly may be resonant.
DD of Splenomegaly from Renal tumour
Causes of Spenomegaly
Massive SplenomegalySpleen MUST be enlarged to 3 times its normal size before it becomes clinically palpable.
Massive splenomegaly is likely due to malignant disease:- Chronic myeloid leukemia,
- Myelofibrosis,
- Lymphoma (Hodgkin’s and Non-Hodgkin’s).
Hypersplenism (see next slide)
Causes of Splenomegaly:Tropical splenomegaly:
- Malaria- Kala-azar
- Shistosomiasis
Infective Splenomegaly:
• Bacterial: Typhoid, Paratyphoid, Tuberculosis,
Splenic Abscess, Septicaemia.
2. Viral: infectious mononucleosis, HIV, psittacosis.
3. Parasitic: Hydatid cyst, Trypanosomiasis, Syphilis,Weil’s disease.
Hypersplenism: Possible indications for Splenectomy
• Inherited haemolytic anaemia (Congenital Spherocytosis & Elliptocytosis). Mechanism: ↑ RBCs fragility (Anaemia).
• Autoimmune haemolytic anaemias.
Mechanism: Antibodies to RBCs (Anaemia).• Thalassaemia and Sickle cell disease.
Mechanism: Abnormal haemoglobins (Anaemia).• Immune thrombocytopenic purpura (primary & secondary)
Mechanism: Antibodies to platelets (Thrombocytopenia).• Portal Hypertension. Mechanism: ↑splenic venous
pressure with delayed transit of blood (Pancytopenia).• Rheumatoid arthritis (Felty’s syndrome)
Mechanism: Uncertain (Leucopenia or pancytopenia).Splenectomy: other indications
• Traumatic rupture of spleen
• Iatrogenic splenectomy
• Part of other surgical procedures, e.g. total gastrectomy,
distal pancreatectomy, lower oesophagectomy, left sided renal cell carcinomas and adrenal cancer, and retroperitoneal sarcoidosis in left upper quadrant.
• Vascular diseases:
splenic vein thrombosis, splenic artery aneurysm.
• Storage disease:
Gaucher disease, Letterer-Siwe disease, amyloidosis.
• Collagen disease: Felty’s syndrome, Still’s disease.
• Cysts, abscesses, primary splenic tumours.
• Diagnostic staging laparotomy with splenectomy is now replaced by CT abdomen.
• Rare: wandering spleen, splenic ectopic pregnancy (!).
Post-Splenectomy Complications
1. Overwheming post-splenectomy infection (OPSI)Serious late complicationdue to pneumococci, meningococci and Haemophilus influenzae. Sepsis into fulminant infection with fever, vomiting, dehydration and collapse. Prophylactic immunization (pneumovac) 2 week prior to surgery, antibiotics after emmergency surgery continued for life (Penicillin V 250 mg b.d.).
2. Unexplained postoperative abdominal pain with fever may herald portal vein thrombosis (anticoagulant and antibiotic must be given).
3. Others: Acute gastric distension, paralytic ileus, left basal atelectasis, haematemesis (due to gastric mucosal congestion after vasa brevia ligation), pancreatic leak, possible abdominal wound dehiscence or persistent hiccup due to left subphrenic irritation by blood collection or an abscess.
Blunt trauma (slipped and fell on edge of bath-tub) 6 hr ago.
Severe upper abdominal pain
Pain in left shoulder (Kehr sign)
BP 100/60 PR: 100 Temp: 37.3 Resp Rate 18
Not in shock now - (barely haemodynamically stable)Ecchymosis left lower chest wall
Upper abdominal tenderness
Otherwise soft abdomen What to do next?
Chest x-ray (trachea central, chest clear but fractured rib 10)
FAST (fluid collection peri-splenic area).What to do next?
A Clinical Scenarioof ‘Splenic Injury’ (to sum it up)
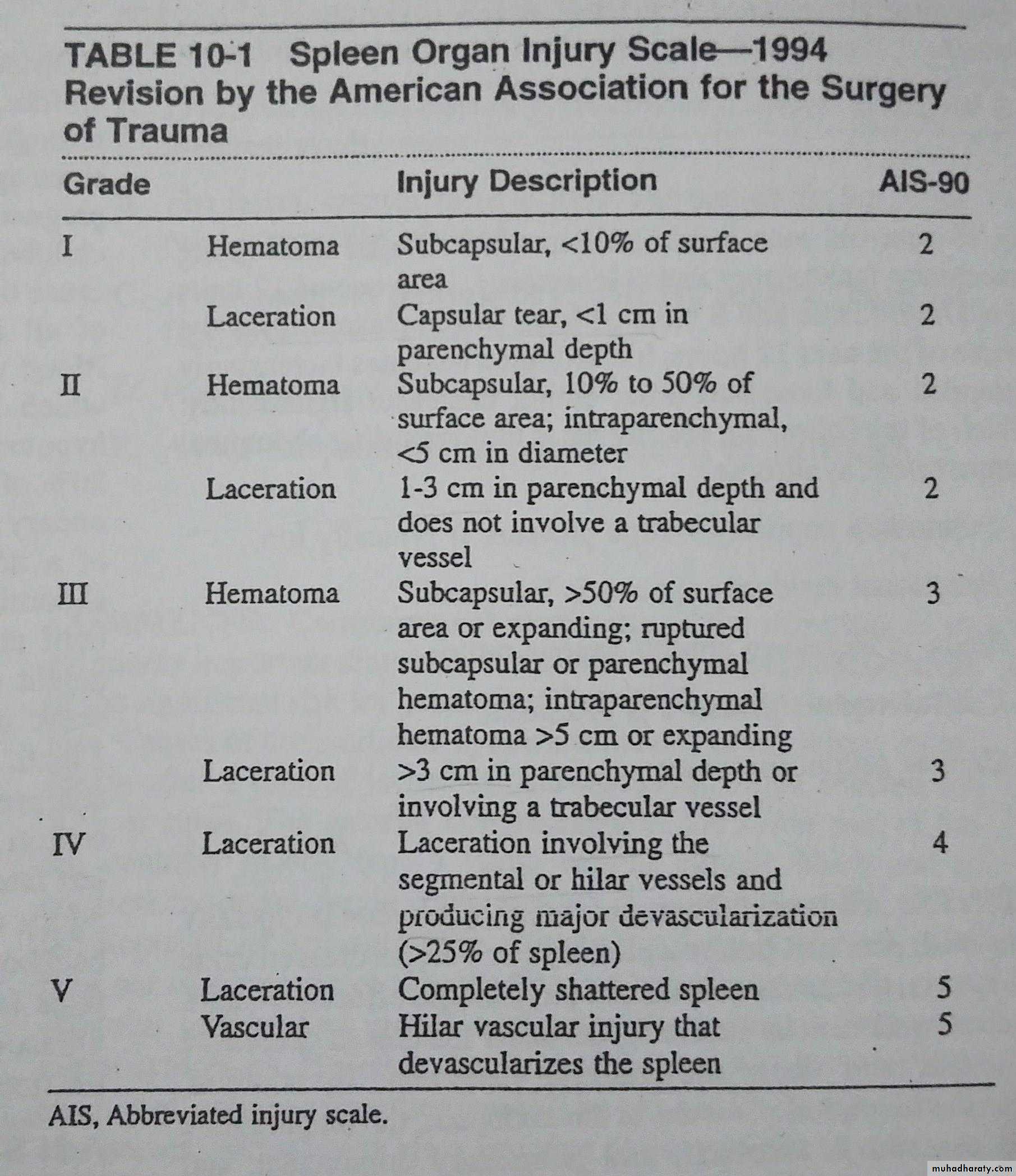
CT abdomen:
Stable patients >55y with isolated Grade 1 or 11 injury can be managed conservativelyHaemodynamically this patient became unstable.
How to treat?
Laparotomy and SplenectomyA Clinical Scenario
of ‘Splenic Injury’ (to sum it up)What is conservative Splenectomy ?
Look for spleniculus or spleniculi.• Partial splenectomy. or
• Splenic repair (as in liver).
• Splenic Auto-transplantation (splenosis).
A Clinical Scenario
of ‘Splenic Injury’ (to sum it up)
Thanks for Participation
