Evaluation of renal masses
Dr Montadhar AlmadaniCauses
Benign causes :• Ureteropelvic junction obstruction ( most common cause ).
• Obstructed mega ureter.
• Sever grade of reflux.
• Polycystic kidney disease ( adult ,infantile )
• Simple renal cyst.
• calyseal diverticulum.
• Abscess
• Angiomyolipoma.
• Oncocytoma.
• Others .
Malignant causes
• Renal cell carcinoma .adult• Wilm's tumor. children
• Liposarcoma.
• Sarcoma.
• Lymphoma.
• Transitional cell carcinoma .
• Metastatic tumors .
Presentation
During antenatal ultrasound .
Accidental finding during imaging study doing for an other cause.
Abdominal mass.
Hematuria ( macroscopic or microscopic ).
Flank pain, bone pain
Anemia, cough.
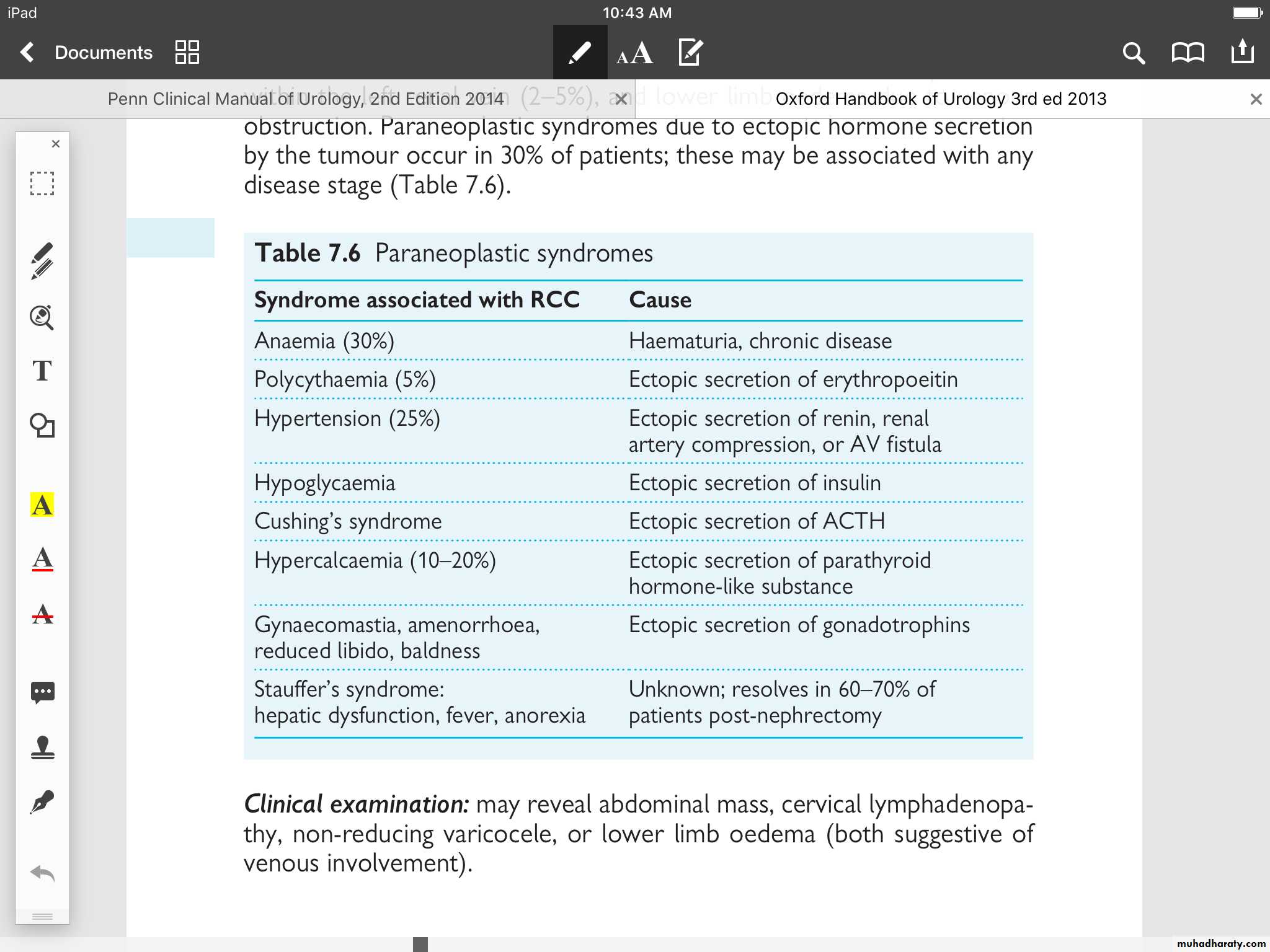
Paraneoplastic syndrome .
Fever, wt loss and sweating, symptoms of metastasis
Polycythemia .
Shock
Lower limb odema, varicose veins.
Others
Work up
Biochemical :• Urine analysis to evaluate infections and hematuria.
• Renal function tests to evaluate renal impairment .
• Complete blood picture and ESR .
• Electrolyte assessment .
• AFB and PCR .
• Urine cytology.
Imaging study:
• CXR.
• Abdominal ultrasound .
• Abdominal CT scan and MRI.
• Chest CT scan and MRI.
• Isotope study.
• Brain CT scan and MRI.
• Doppler ultrasound .
• IVP
Other tests:
FNA, biopsy.Radiological classification of renal cysts
Uncomplicated simple (smooth-walled, round or oval, without internal echoes, and complete transmission with a strong acoustic shadow poste- riorly.), benign; no follow-up if asymptomaticMinimally complicated; septa, calcification, hyperdense (contain blood); benign, but require radiological follow-up
Complicated; irregular margin, thickened septa, thick irregular calcification; indeterminate, surgical exploration indicated unless there is history of trauma or infection
Large, irregular cyst margins with solid components internally; cystic renal carcinoma until proven otherwise; surgery required
Staging of wilm's tumor
Stage I Wilms’ tumour (43% of patients)—at least one of the following criteria must be met.• - Tumour is limited to the kidney and is completely excised.
• - The surface of the renal capsule is intact.
• - The tumour is not ruptured or biopsied (open or needle) prior to removal.
• - No involvement of extrarenal or renal sinus lymph–vascular spaces.
• - No residual tumour apparent beyond the margins of excision.
• - Metastasis of tumour to lymph nodes not identified.
Stage II Wilms’ tumour (23% of patients)—at least one of the following criteria must be met.
• - Tumour extends beyond the kidney, but is completely excised.
• No residual tumour apparent at or beyond the margins of excision.
• Any of the following conditions may also exist.
• Tumour involvement of the blood vessels of the renal sinus and/or outside the renal parenchyma.
• The tumour has been biopsied prior to removal or there is local spillage of tumor during surgery, confined to the flank.
• Extensive tumour involvement of renal sinus soft tissue.
Stage III Wilms’ tumour (23% of patients) at least one of the following criteria must be met.
• - Unresectable primary tumour. –
• Lymph node metastasis. –
• Tumour is present at surgical margins.
• - Tumour spillage involving peritoneal surfaces, either before or during surgery, or transected tumour thrombus.
Stage IV Wilms’ tumour (10% of patients) is defined as the presence of haematogenous metastases (lung, liver, bone, or brain) or lymph node metastases outside the abdominopelvic region.
Stage V Wilms’ tumour (5% of patients) is defined as bilateral renal involvement at the time of initial diagnosis.
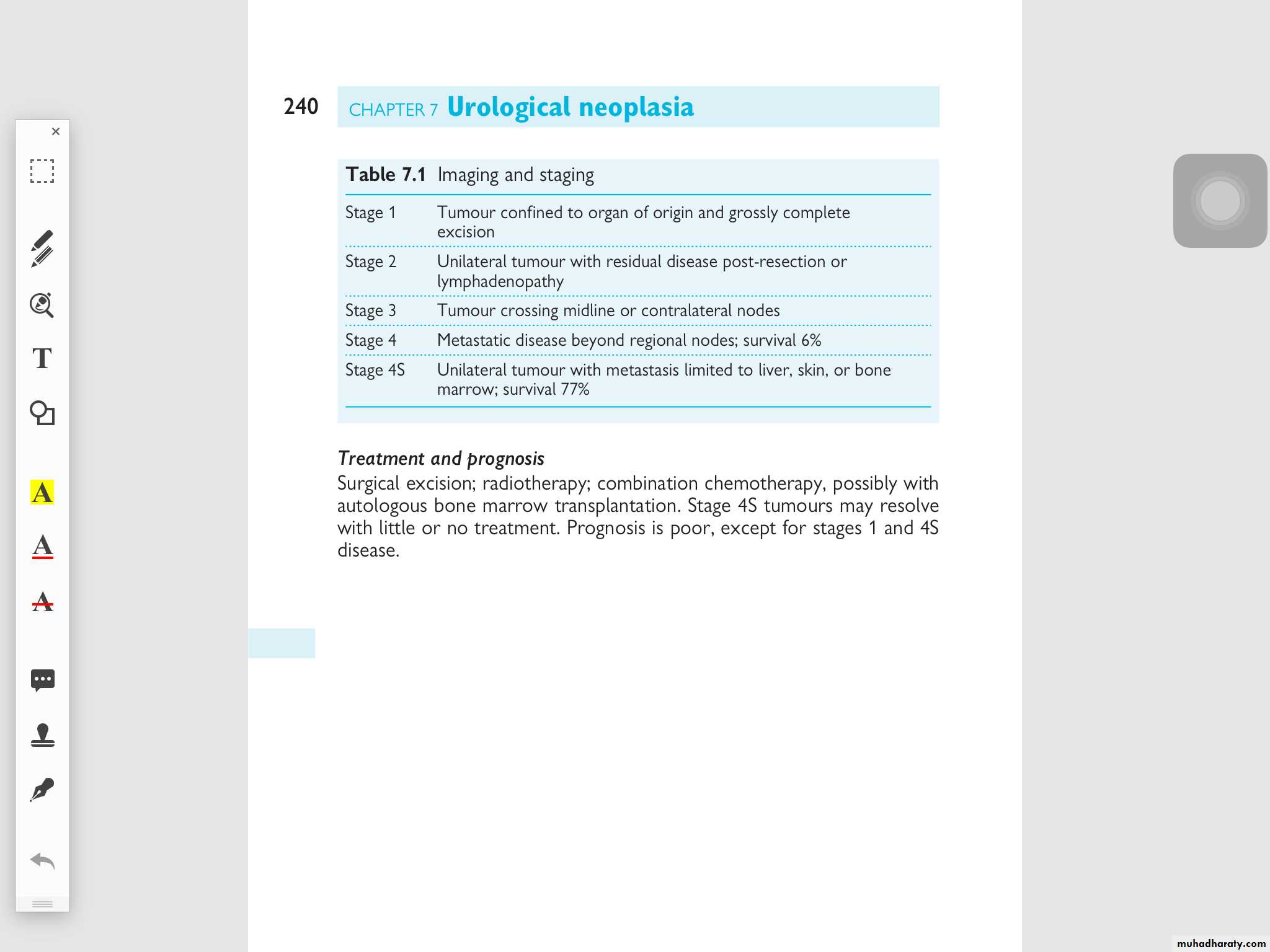
Neuroblastoma staging:
Management
The management depends on the following factors:• Behavior of mass ( benign or malignant )
• Unilateral or bilateral
• Total renal function
• Size of mass ( e.g. Angiomyolipoma)
• Age of patient
• Localize or metastatic ( if malignant)
• Mass effect like obstruction of renal pelvis
Options of treatment
In simple word the treatment range from no treatment to radical nephroctomy with chemoradiotherapy
• No treatment ( e.g simple cyst)
• Cyst aspiration with sclerotic agents in side the cyst
• Cystic removal ( open ,laparoscopic)
• Partial nephrectomy (open or laparo.. )
• Radical nephrectomy ( open ,laparo..)
• Simple nephrectomy .
• Chemoradiotherapyn.