Baghdad College of Medicine / 4
th
grade
Student’s Name :
Dr. Saad Dakhil
Lec. 1
Benign Prostatic
Hyperplasia (BPH)
Tues. 22 / 3 / 2016
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
2
©Ali Kareem 2015-2016
M
ODULE
3: B
ENIGN
P
ROSTATIC
H
YPERTROPHY
K
EYWORDS
: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction,
lower urinary tract symptoms (LUTS)
At the end of this clerkship, the medical student will be able to:
1. Identify and name the major anatomic and histologic features of the prostate
gland
2. Identify the predominant location in the prostate where BPH develops and
describe how this fact relates to the symptoms and signs of BPH
3. Define BPH
4. Describe the distinctive epidemiological features and natural history of BPH
5. List the symptoms and signs of BPH
6. List the important components of the history when interviewing a patient with
BPH
7. List the important components of the physical exam of a patient with BPH
8. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should
be ordered in a patient with BPH
9. List the indications for treatment of BPH
10. List the medical and surgical treatment options for BPH.
11. Describe when a patient with BPH should be referred to a urologist
P
ROSTATE
A
NATOMY
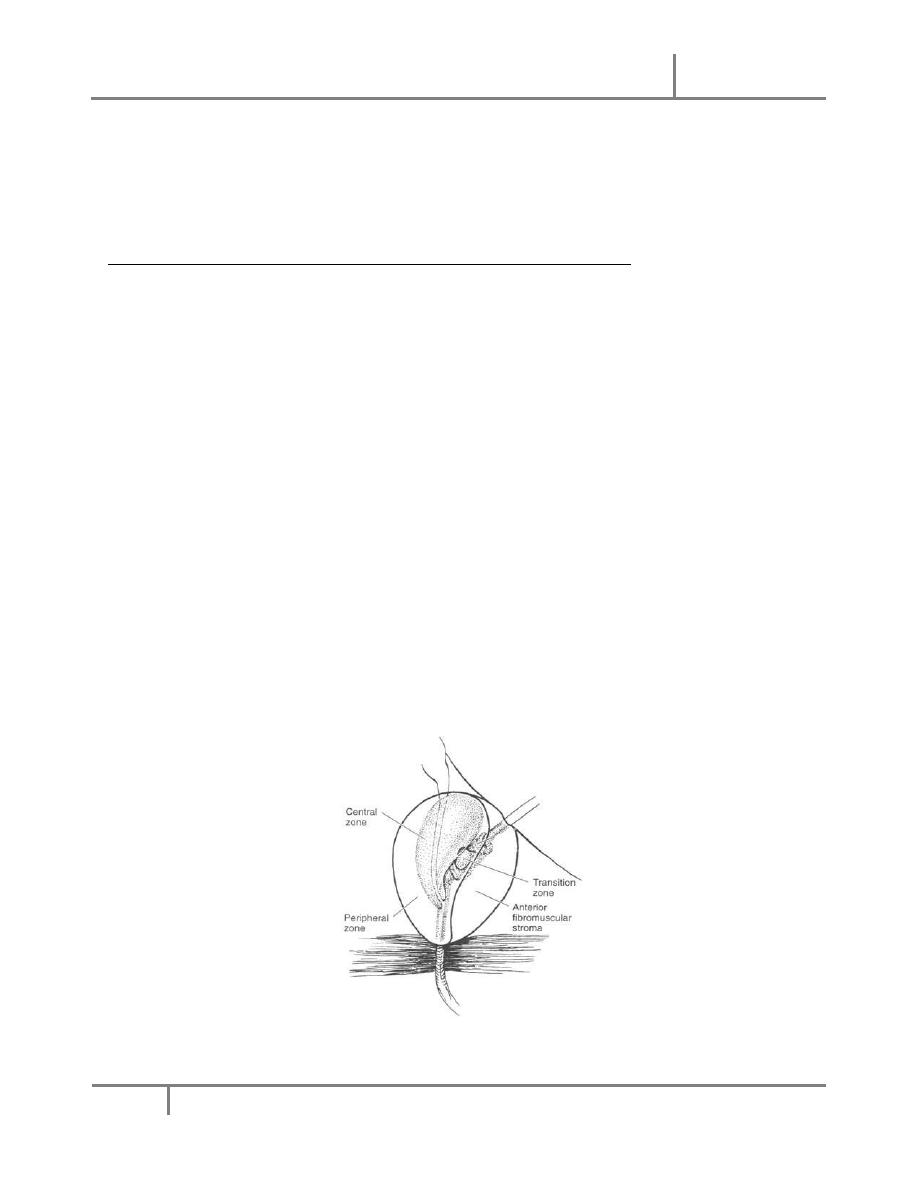
There are three basic anatomic regions of the prostate: the anterior prostate, central
gland and peripheral gland, as illustrated in Figure 1.
Figure 1: The zones and glandular regions of the normal prostate.
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
3
©Ali Kareem 2015-2016
The arterial blood supply to the prostate is from the inferior vesical artery. The
anterior prostate is entirely fibromuscular and non-glandular, and it appears to have
little significance in prostatic function or pathology. This area comprises
approximately 20% of the bulk of prostatic tissue. The central gland is composed of
the proximal urethra, the prostate tissue around the posterior urethra and the smooth
muscle of the internal sphincter, which is mediated by
1
A receptors. It forms the
central portion of the prostate and extends from the base of the prostate to the
verumontanum. The transition zone surrounds the urethra, and although this region
accounts for only 10% of prostate glandular tissue in young men, it exhibits significant
growth with age. Indeed, it is in the transition zone is where benign prostatic
hypertrophy (BPH) develops. The peripheral gland or zone is composed entirely of
acinar tissue. It comprises the posterior surface of the prostate, including the apical,
lateral, posterolateral and anterolateral portions of the prostate. The peripheral zone
represents approximately 70% of glandular volume in the normal adult prostate. The
vast majority of prostatic carcinomas arise in this region of the prostate.
B
ENIGN
P
ROSTATIC
H
YPERPLASIA
D
EFINITION
The term “benign prostatic hyperplasia (BPH)” has been used to describe a
constellation of voiding symptoms that occurs in men with aging. These symptoms
include decreased force of stream, hesitancy, straining, incomplete bladder
emptying, and nocturia; dysuria is usually not a symptom of BPH. Such symptoms are
generally referred to as obstructive in nature. Irritative symptoms are also associated
with BPH and include urinary frequency, urgency, and occasionally dysuria. BPH has
been used synonymously with “prostatism” and “bladder outlet obstruction”, implying
that obstruction to urinary outflow, secondary to prostatic enlargement, is the cause
of such symptoms. More recently, it has been recognized that prostatic enlargement
is not necessary for such symptoms. Furthermore, women may experience similar
symptoms with age. Thus, “lower urinary tract symptoms” (LUTS) is currently the
preferred term to describe this complex of obstructive and irritative urinary
symptoms that occur in both sexes with age.
Voiding dysfunction in the aging male may be due to a variety of factors including
changes in the bladder, prostate and/or urethra. Intrinsic changes in the bladder,
such as bladder instability, decreased bladder compliance and decreased bladder
capacity may all lead to LUTS. However, in many men these symptoms are due to
BPH, mediated via
1
A receptors. With age, the prostate exhibits glandular
enlargement, increased smooth muscle tone and decreased compliance secondary to
altered collagen deposition; these changes can lead to altered urinary symptoms.
Urethral stricture and bladder neck contracture are other forms of obstruction or
blockage that can present with similar symptoms.
BPH is one of the most frequent diagnoses leading to urology referral. It is commonly
found in men of all ages. It begins to develop before age 30 with almost 10% of men
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
4
©Ali Kareem 2015-2016
having histologic evidence of BPH by 40 years of age, and 50% of men showing

Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
5
©Ali Kareem 2015-2016
evidence by age 60. Overall, nearly 80% of men will develop BPH, and as many as 30%
will receive treatment for it. In studies that examine the natural history of BPH, the
incidence of acute urinary retention or the development of a significant post-void
residual urinary volume is 2% per year. Thus, the burden of BPH on the healthcare
system is substantial.
B
ENIGN
P
ROSTATIC
H
YPERTROPHY
-D
IAGNOSIS
After excluding other causes of LUTS, both objective and subjective parameters are
used to decide whether or not treatment is indicated. Objective parameters include
determination of prostate size, measurement of urinary flow rate and determination
of the post-void residual urine volume. While it is useful in assessing the size of the
prostate gland, the main objective of the digital rectal exam in evaluation of men
with LUTS is to identify prostatic nodules. Although several subjective instruments are
available to quantify the severity of LUTS, the American Urological Association
Symptom Score Index (AUASI) also known as the International Prostatic Symptom
Score (IPSS) is used by most clinicians (Figure 2). This questionnaire consists of seven
items that determines the severity of irritative and obstructive voiding symptoms.
Figure 2: The validated AUA Symptom Score tool for voiding symptoms.
Symptom severity related to urinary frequency, nocturia, weak urinary stream,
hesitancy, intermittency, incomplete bladder emptying and urinary urgency are
assessed. On a scale of 0-35, mild symptoms exist with scores of 0-7, moderate
symptoms with scores of 7-15 and severe symptoms with a score of >15. This index
demonstrates predictive validity, reliability and internal consistency. There is some

Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
6
©Ali Kareem 2015-2016
correlation between the objective and subjective measures in that the lower the peak
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
7
©Ali Kareem 2015-2016
History
PE & DRE
UA, Creatinine
PSA (optional)
Symptom Assessment
IF:
Urinary retention
Recurrent urinary tract infection
Recurrent or persistent gross hematuria
Bladder stones
Renal Insufficiency
Mild
Mod/ Severe
Surgery
urinary flow rate, the more severe the urinary symptoms and the larger the prostate.
Using the AUA Symptom score and the information from the clinical evaluation,
treatment options can be reviewed, as outlined in Figure 3.
Importantly, there are several signs or symptoms that may coexist with voiding
symptoms that can alter the treatment algorithm. If the patient has urinary retention,
an acute condition in which urine is unable to be voluntarily voided, then immediate
treatment with surgery may be indicated. A trial of Foley catheter or clean
intermittent catheterization and alpha-blocker medication may avoid surgical
treatment in the future in about 80% of cases in which retention coexists with LUTS.
The likelihood of going into retention is related to prostate size, patient age, and the
severity of the symptoms. Recurrent urinary tract infections, persistent or recurrent
gross hematuria, and bladder stones are also coexisting conditions that may
necessitate surgical instead of medical treatment.
Figure 3.
Diagnostic and treatment
algorithm for BPH.
Watchful Waiting
Non surgical
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
8
©Ali Kareem 2015-2016
B
ENIGN
P
ROSTATIC
H
YPERTROPHY
-T
REATMENT
Drug Therapy
Medical therapy for BPH attempts to shrink or stop the growth of the prostate or open
the urethral channel within the prostate, without using surgery. The FDA has currently
approved six drugs to relieve the symptoms associated with an enlarged prostate.
Finasteride, FDA-approved in 1992, and Dutasteride, FDA-approved in 2001, inhibit
production of the hormone dihydrotestosterone (DHT), which is responsible for growth
of the acinar glands of the prostate. These drugs can either prevent progression of
growth of the prostate or actually shrink the prostate in some men.
The drugs terazosin, doxazosin, tamsulosin, and alfuzosin are also used to treat BPH.
These drugs belong to the class known as alpha-blockers, and all act by relaxing the
smooth muscle of the prostate and bladder neck to improve urine flow and to reduce
bladder outlet obstruction. Terazosin and doxazosin were developed as blood pressure
pills, but tamsulosin and alfuzosin were developed specifically to treat BPH. There is
excellent clinical trial data that shows that finasteride and doxazosin together is more
effective than using either drug alone to relieve symptoms and prevent BPH
progression. The dual-drug regimen reduced the risk of BPH progression by 67
percent, compared with 39 percent for doxazosin alone and 34 percent for finasteride
alone.
Because drug treatment is not effective in all cases, a number of minimally invasive
procedures have been developed to relieve BPH symptoms. In general, these
procedures are less invasive than conventional surgery for BPH, which is the
transurethral resection of the prostate (TURP).
Minimally Invasive Therapy
Transurethral microwave procedures: This device uses microwaves to heat and
destroy excess prostate tissue. In the procedure called transurethral microwave
thermotherapy (TUMT), the device sends microwaves through a catheter to heat
selected portions of the prostate to at least 111 degrees Fahrenheit. A cooling system
protects the urinary tract during the procedure. The procedure is performed on an
outpatient basis in an hour without general anesthesia. TUMT has not been reported
to lead to erectile dysfunction or incontinence. Although microwave therapy does not
cure BPH, it reduces urinary frequency, urgency, straining, and intermittent flow. It
does not correct the problem of incomplete emptying of the bladder. The long-term
effects of microwave therapy are still not clear however.
Transurethral needle ablation (TUNA): The TUNA system delivers low-level
radiofrequency energy through twin needles to burn away selected regions of the
enlarged prostate. Shields protect the urethra from heat damage. The TUNA system

Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
9
©Ali Kareem 2015-2016
improves urine flow and relieves symptoms with fewer side effects when compared
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
10
©Ali Kareem 2015-2016
with conventional surgery, transurethral resection of the prostate (TURP). No
incontinence or impotence has been observed with this procedure.
Water-induced thermotherapy: This therapy uses heated water to destroy excess
tissue in the prostate. A catheter containing multiple shafts is positioned in the
urethra so that a treatment balloon rests in the middle of the prostate. A computer
controls the temperature of the water, which flows into the balloon and heats the
surrounding prostate tissue. The system focuses the heat in precise regions of the
prostate, while surrounding tissues in the urethra and bladder are protected.
Destroyed tissue either escapes with urine through the urethra or is reabsorbed by the
body.
High-intensity focused ultrasound (HIFU): The use of low frequency ultrasound waves
to destroy prostate tissue is the youngest of the minimally invasive therapies
developed for BPH. It appears as safe as other minimally invasive methods but long-
term outcome data is not available as of yet.
Transurethral laser surgery: Surgical procedures that employ side-firing laser fibers
and Nd: YAG lasers to vaporize obstructing prostate tissue are also used to treat BPH.
A laser fiber is passed into the urethra near the prostate using a cystoscope and then
several bursts of energy lasting 30 to 60 seconds are delivered through the laser fiber.
The laser energy destroys prostate tissue and causes shrinkage. As with TURP, laser
surgery requires anesthesia and a hospital stay. One advantage of laser surgery over
TURP is that laser surgery causes less blood loss and allows for a quicker recovery.
However, laser surgery may not be effective on larger prostates and the long-term
effectiveness of laser surgery is unclear. There are two variations of laser surgery for
BPH: Photoselective Vaporization of the Prostate (PVP) uses a high-energy laser to
destroy prostate tissue and seal the treated area, and Interstitial Laser Coagulation
involves placing the tip of the fiberoptic probe directly into the prostate tissue to
destroy it.
Conventional Surgical Therapy
Transurethral resection of the prostate (TURP): Surgical therapy with transurethral
resection of the prostate (TURP) has traditionally been the “gold standard” treatment
for men with BPH. In 1986, it was estimated that TURP accounted for 24% of the
professional workload for practicing urologists in the U.S. In this type of surgery, no
external incision is needed. After giving anesthesia, the surgeon reaches the prostate
by inserting an instrument called a resectoscope through the urethra. The
resectoscope is about 12 inches long and 1/2 inch in diameter, contains a light, valves
for controlling irrigating fluid, and an electrical loop that cuts tissue and seals blood
vessels. During the 60-90-minute operation, the surgeon uses the scope's wire loop to
remove the obstructing tissue one piece at a time. The pieces of tissue are carried by
the fluid into the bladder and then flushed out at the end of the operation. A TURP is
used for approximately 90% of all prostate surgeries for BPH. In most patients, before
TURP is performed, consideration has already been given to medical therapy. In
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
11
©Ali Kareem 2015-2016
general, TURP is reserved for very symptomatic men or those who develop
complications including urinary tract infection, urinary retention, bladder stones, or
gross hematuria.
A variation of the TURP procedure is called transurethral incision of the prostate
(TUIP). Instead of removing tissue, as with TURP, this procedure widens the urethra
by making a few small cuts in the bladder neck, where the urethra joins the bladder,
and in the prostate gland itself. Although some people believe that TUIP gives the
same relief as TURP with less risk of side effects such as retrograde ejaculation, its
advantages and long-term side effects have not been clearly established.
Surgical “open” prostatectomy: In the few cases when a transurethral procedure
cannot be done, because the prostate is too large, the bladder has been damaged or
contains bladder stones or important identifying landmarks not visible for TURP, open
prostatic surgery is indicated. With all open surgical procedures, anesthesia is given
and an incision is made. Once the surgeon reaches the prostate capsule, he or she
scoops out the enlarged tissue from inside the gland. Importantly, as with other types
of surgery and procedures for BPH, the part of the prostate at risk for prostate cancer
development is not removed and therefore men who have procedures for BPH are still
at risk for developing prostate cancer.
B
ENIGN
P
ROSTATIC
H
YPERPLASIA AND
PSA
Prostate Specific Antigen (PSA) is a serine protease produced by benign and malignant
prostate tissue. Functionally, PSA is the enzyme responsible for liquefaction of the
seminal fluid after ejaculation. Although produced in small amounts in other tissues,
it should be considered to be prostate specific. A strong correlation exists between
serum PSA level and prostate volume. PSA circulates in the serum in both free
(unbound) and complexed (bound) forms. In addition to being elevated by BPH and
prostate cancer, PSA may also be transiently elevated in cases of prostatic
inflammation (prostatitis) or infarction, and after prostatic manipulation by biopsy.
However, routine digital rectal examination (DRE) usually has little effect on serum
PSA levels. The half-life of serum PSA is 2.2 to 3.2 days. Therefore, one should wait 4
to 8 weeks after prostate manipulation and inflammation (cystoscopy, prostate
biopsy, and prostatitis) before obtaining a PSA.
The screening recommendations from the AUA advise that PSA screening be offered to
men 50 years or older, and who have a life expectancy of at least 10 years. Men with
a first-degree relative known to have prostate cancer or of African American ethnicity
should consider PSA screening at 45 years of age. Men with one first-degree relative
who has prostate cancer have a twofold increased risk of also developing the disease.
Potential screening should be preceded by an informed discussion of the risks and
benefits of screening, early diagnosis and treatment. Given the added cost and
anxiety associated with PSA screening, in combination with a lack of randomized trials

Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
12
©Ali Kareem 2015-2016
showing that screening decreases morbidity and mortality, such screening is not
Benign Prostatic Hyperplasia Dr. Saad Dakhil
22-3-2016
13
©Ali Kareem 2015-2016
recommended for everyone. With such information, the patient can make an
individual decision regarding PSA screening.
S
UMMARY
The prostate is composed of several regions and zones: two zones of interest
are the peripheral zone, where most cancers arise, and the transition zone,
where BPH arises.
The diagnosis of voiding dysfunction due to BPH is made based on both
subjective and objective findings on clinical evaluation.
Medical treatment of BPH involves treatment that relaxes the muscular
stromal tissue of the bladder neck and prostatic urethra (alpha-blockers) and
reduction in the acinar-glandular volume of the prostate through reduced DHT
production (5-alpha-reductase inhibitors).
Indications for surgical intervention with BPH include urinary retention, gross
hematuria, bladder stones, and urinary tract infection.
Serum PSA, a serine protease that liquefies the ejaculate, increases over time
with both BPH and prostate cancer, which makes it a difficult diagnostic
marker for cancer alone.
I
NTERACTIVE
C
ASES IN
U
ROLOGY
Benign Prostatic Hyperplasia 1 - The Case of Mr. Jones and the Urinal of Doom
http://www.auanet.org/eforms/casestudies/index.cfm?slnm=Urinal%20of%20Doom
Benign Prostatic Hyperplasia 2 - The Case of Mr. Presley's Urinary Retention
http://www.auanet.org/eforms/casestudies/index.cfm?slnm=Urinary%20Retention
R
EFERENCES
AUA Guideline on the Management of Benign Prostatic Hyperplasia: Diagnosis and
Treatment Recommendations.
http://www.auanet.org/content/guidelines-and-quality-care/clinical-guidelines.cfm?sub=bph
Harkaway RC, Issa MM. Medical and minimally invasive therapies for the treatment of
benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2006;9(3):204-14. Epub
2006 Jun 6