Acute inflammatory
dermatoses
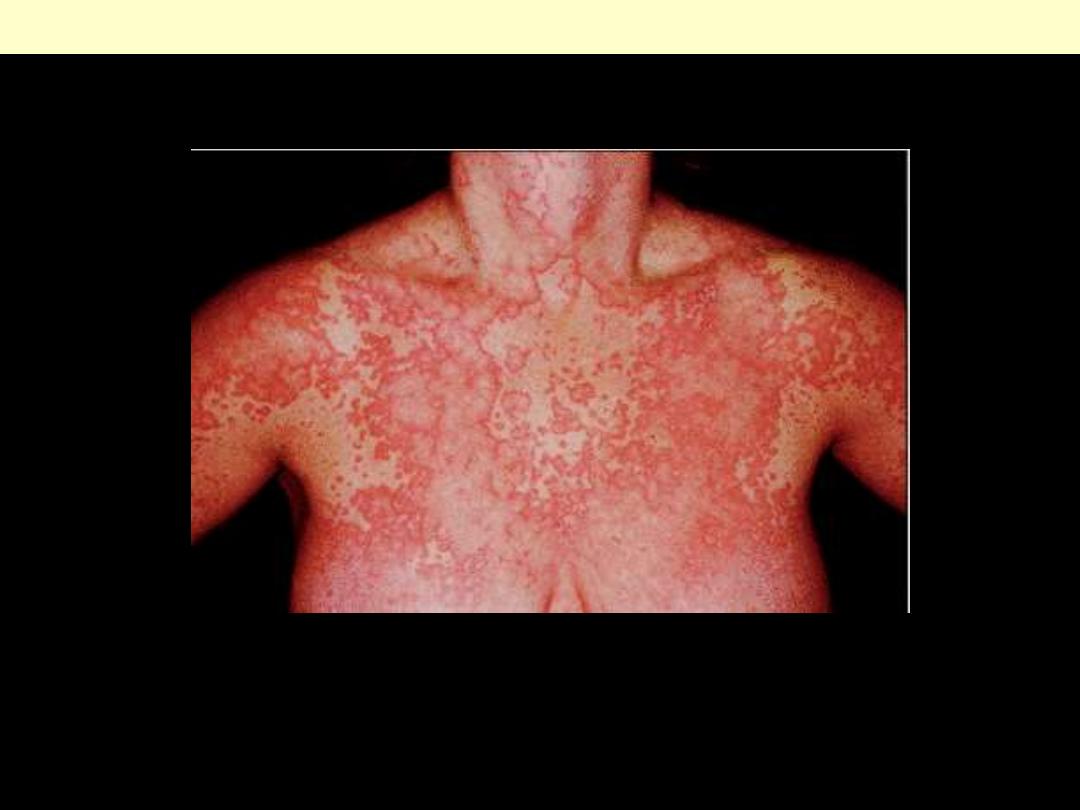
This extensive example of urticaria shows erythematous, edematous, and pruritic plaques termed
wheals
Urticaria

Hives (urticaria) is a common skin condition with an itchy rash of pink to red bumps that appear and
disappear anywhere on the body. An individual lesion typically lasts a few hours before fading away,
and new lesions can appear as older areas disappear.
Urticaria
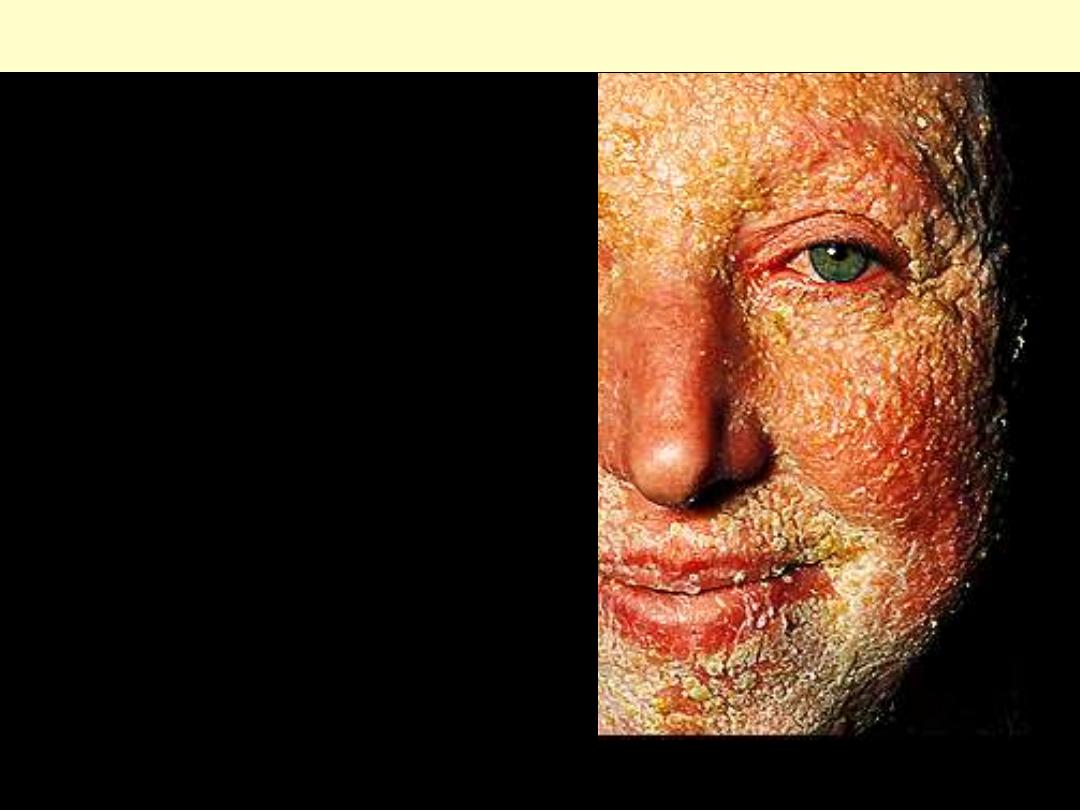
Contact dermatitis (eczema)
CD (eczema): acute vesicular, crusted lesions on the
face of a young girl. There is an intense conjunctival
injection and edema of the eyelids.
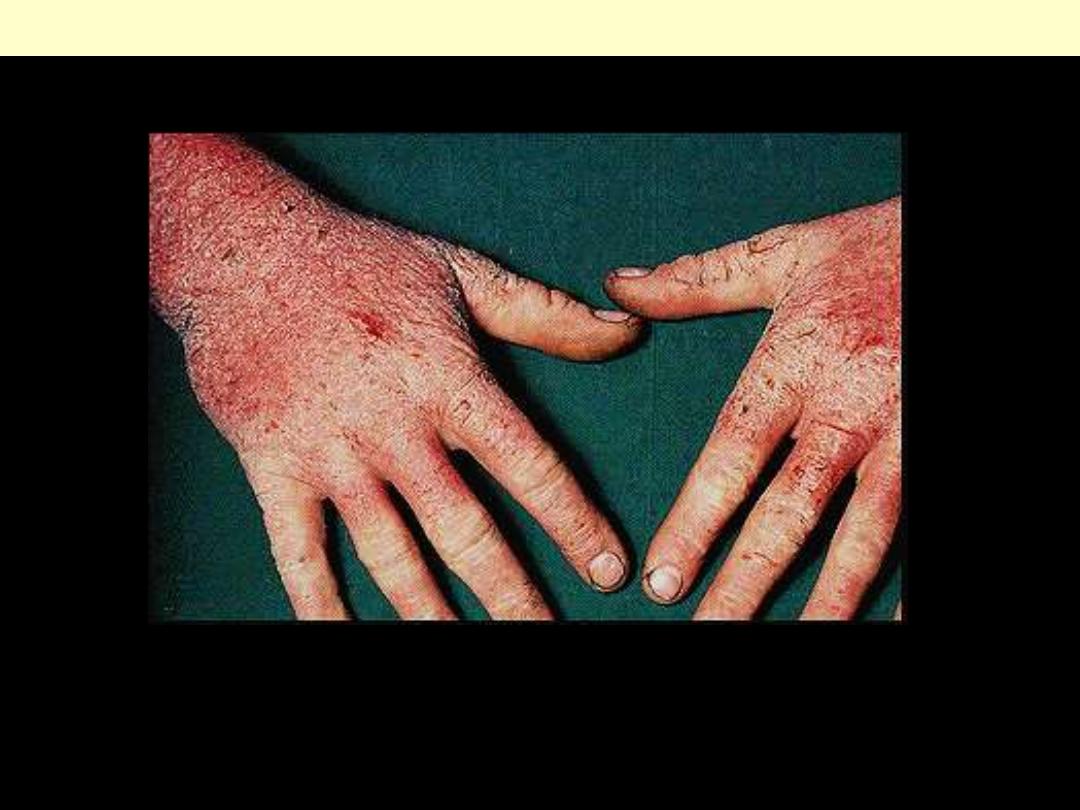
Contact dermatitis (eczema)
This was due to a reaction to rubber gloves.
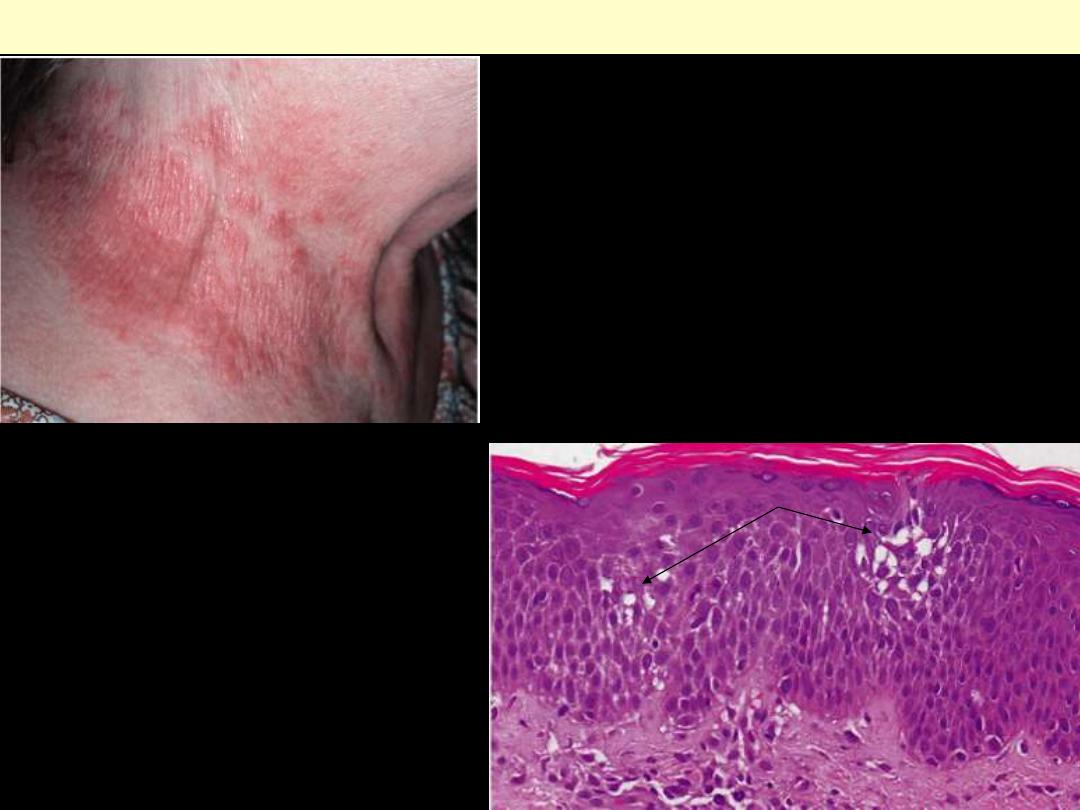
A. Note the patterned erythema and scale associated
with nickel contact dermatitis resulting from this
woman's necklace.
B. Fluid accumulation between epidermal cells results
in spongiosis that can proceed to small vesicles if
intercellular connections are stretched until broken-
thus the term spongiotic dermatitis.
Eczematous dermatitis
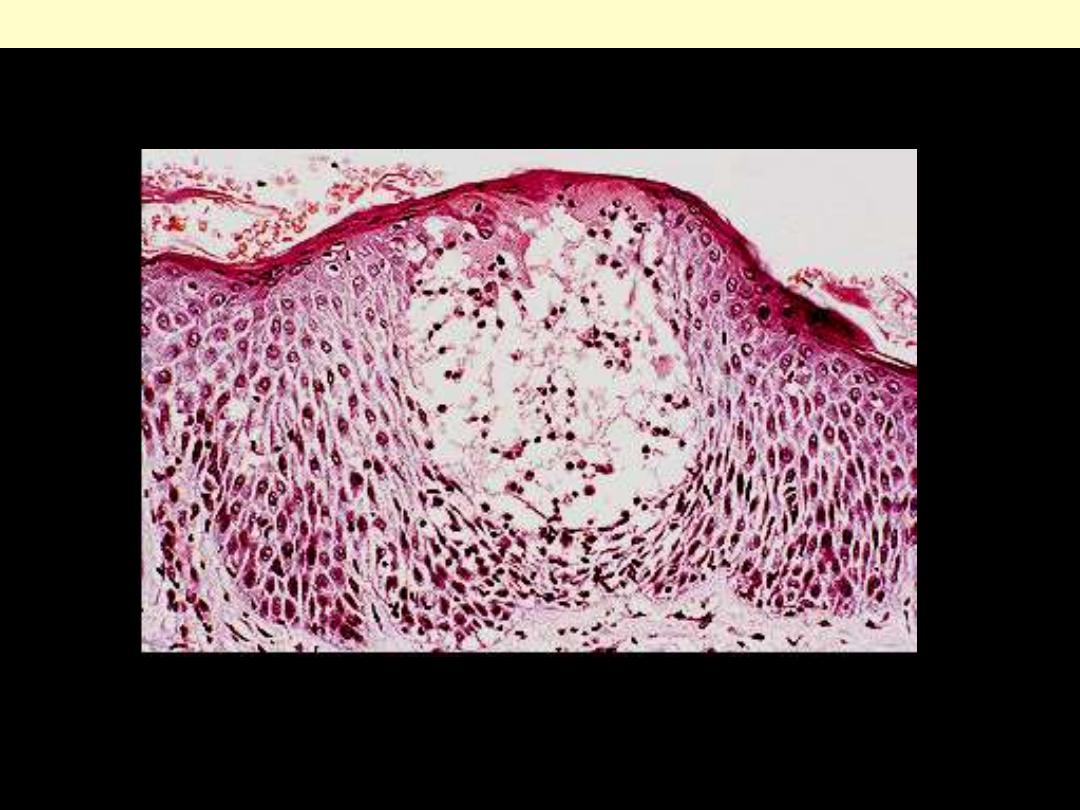
Acute eczematous dermatitis
Fluid-filled vesicle due to intense spongiosis. Note the separation of the epidermal cells adjacent vesicle.
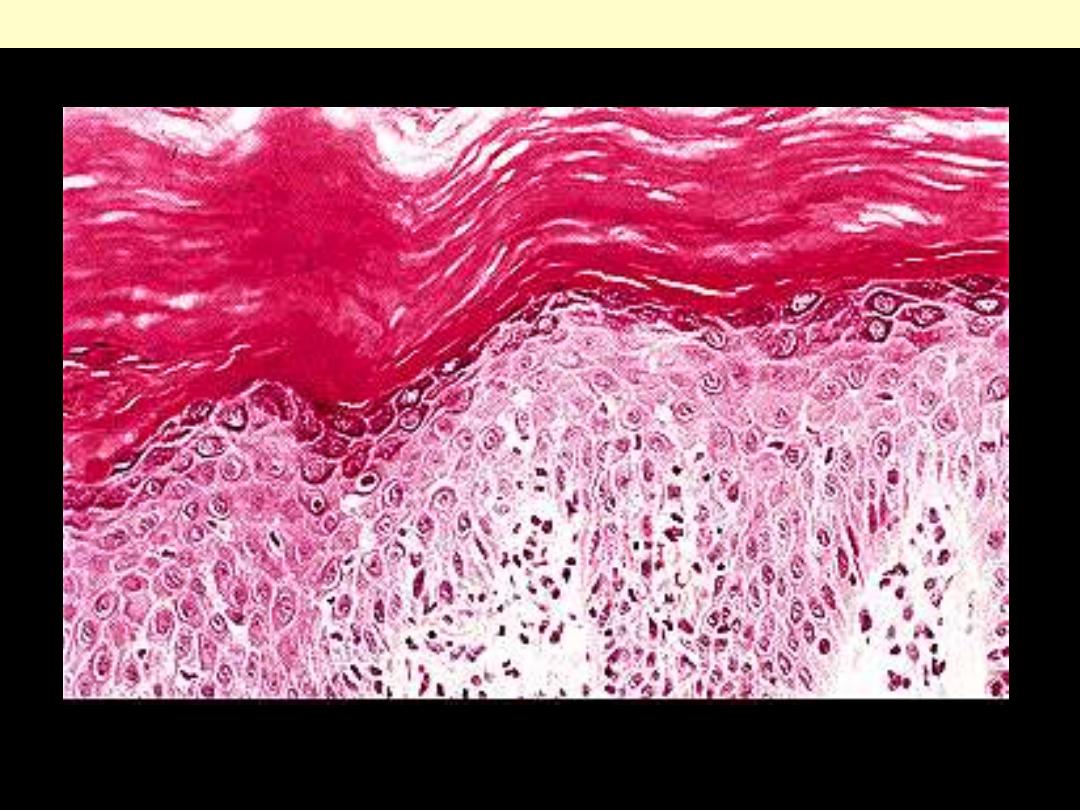
Chronic dermatitis (eczema)
Hyperkeratosis, acanthosis and only slight spongiosis.
Bullous diseases
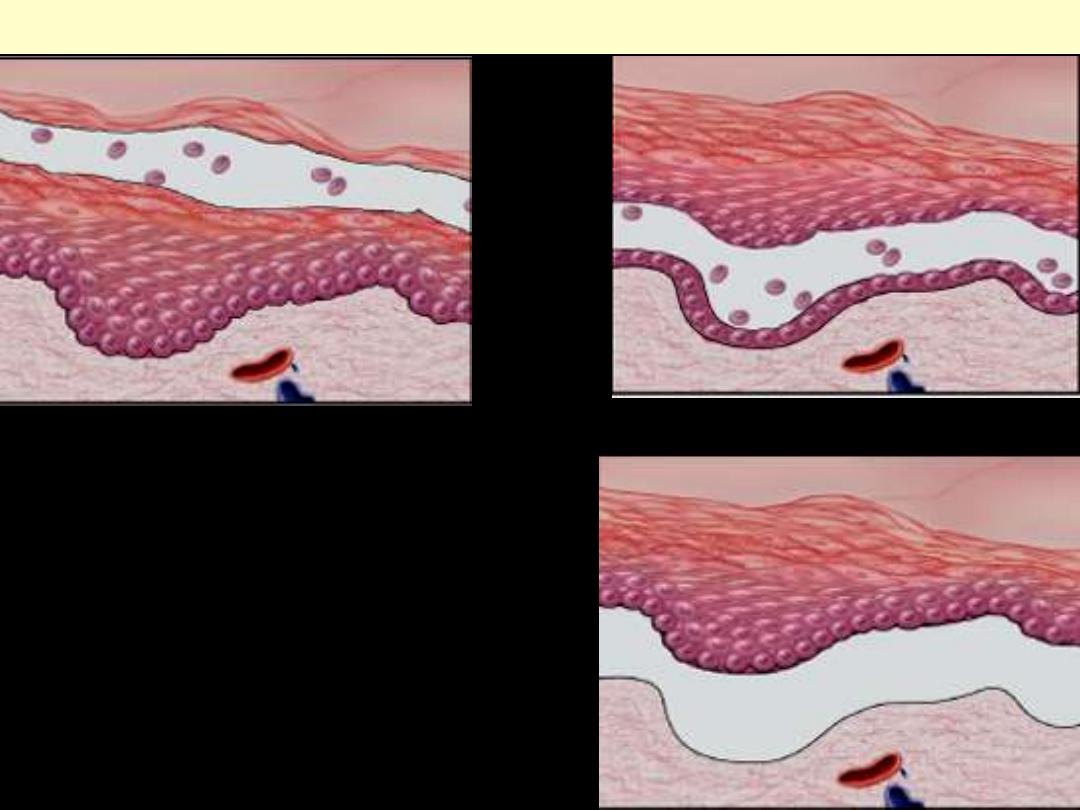
A, Subcorneal (as in pemphigus foliaceus).
B, Suprabasal (as in pemphigus vulgaris).
C, Subepidermal (as in bullous pemphigoid &
dermatitis herpetiformis).
Assessment of the levels of epidermal separation
forms the basis of the initial differential diagnosis of
these lesions.
Levels of blister formation
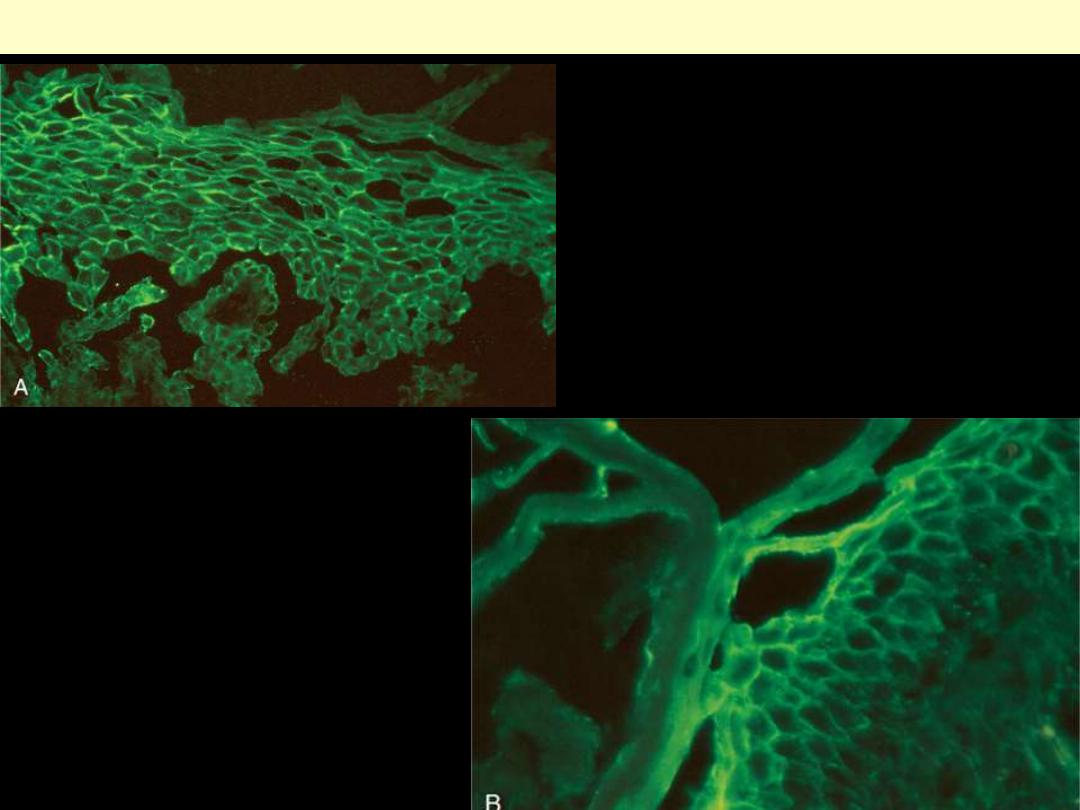
A, Pemphigus vulgaris. There is
uniform deposition of immunoglobulin
and complement (green) along the cell
membranes of keratinocytes, producing
a characteristic "fishnet" appearance.
B, The immunoglobulin deposits are
more superficial in pemphigus foliaceus.
Pemphigus direct IF microscopy

Pemphigus vulgaris
Suprabasal acantholysis results in an intraepidermal blister containing rounded keratinocytes that are
separating from their neighbors. Initially, a single row of basal cells is present on the floor of the blister
with dermal papillomatosis (tombstone effect). Follicular involvement by acantholysis is also common.

There is subcorneal acantholysis leading to suncorneal blister.
Pemphigus foliaceus
P. Vulgaris
Extensive erosions and blistering on the front of the knee.

P. Vulgaris intact and ruptured blisters
Umblical lesions showing intact blisters as well as raw erosions

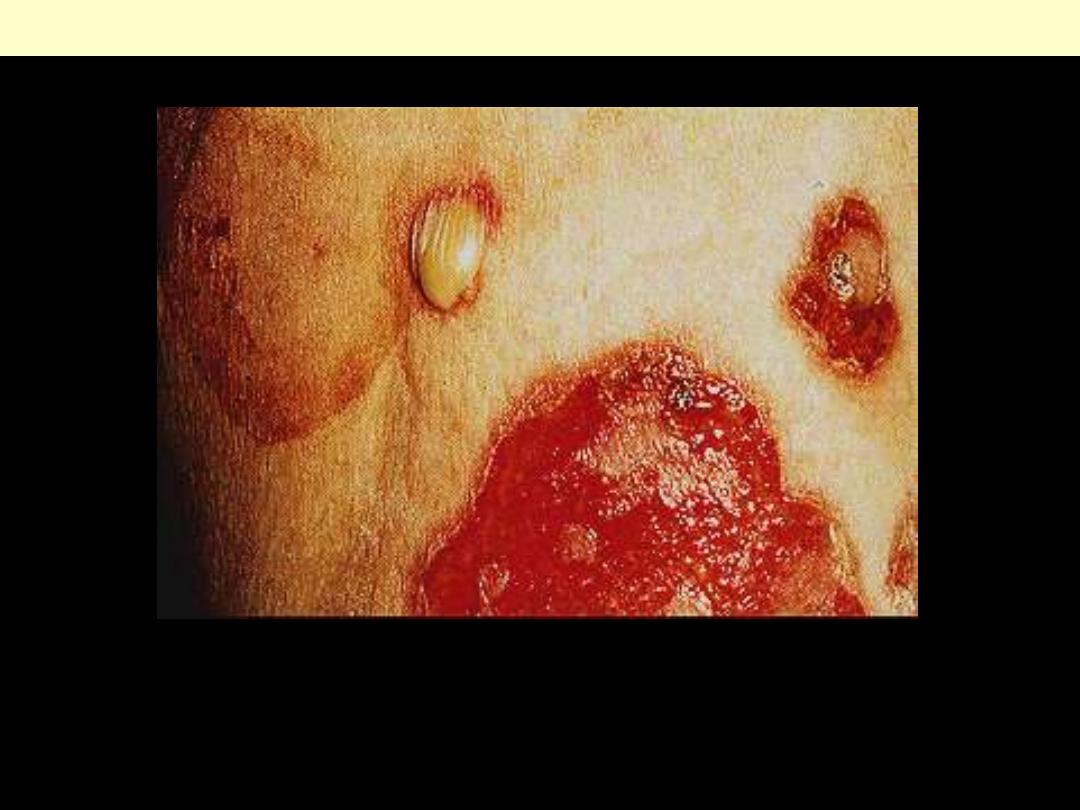
P. Foliaceus
Blisters are much less erosive than those seen in
pemphigus vulgaris, since the level of the blisters
is more superficial (subcorneal). In this patient,
the disease was induced by penicillamine therapy,
and there are intact blisters, erosions, and
crusting. Picture on Rt. & below are close-up
views.

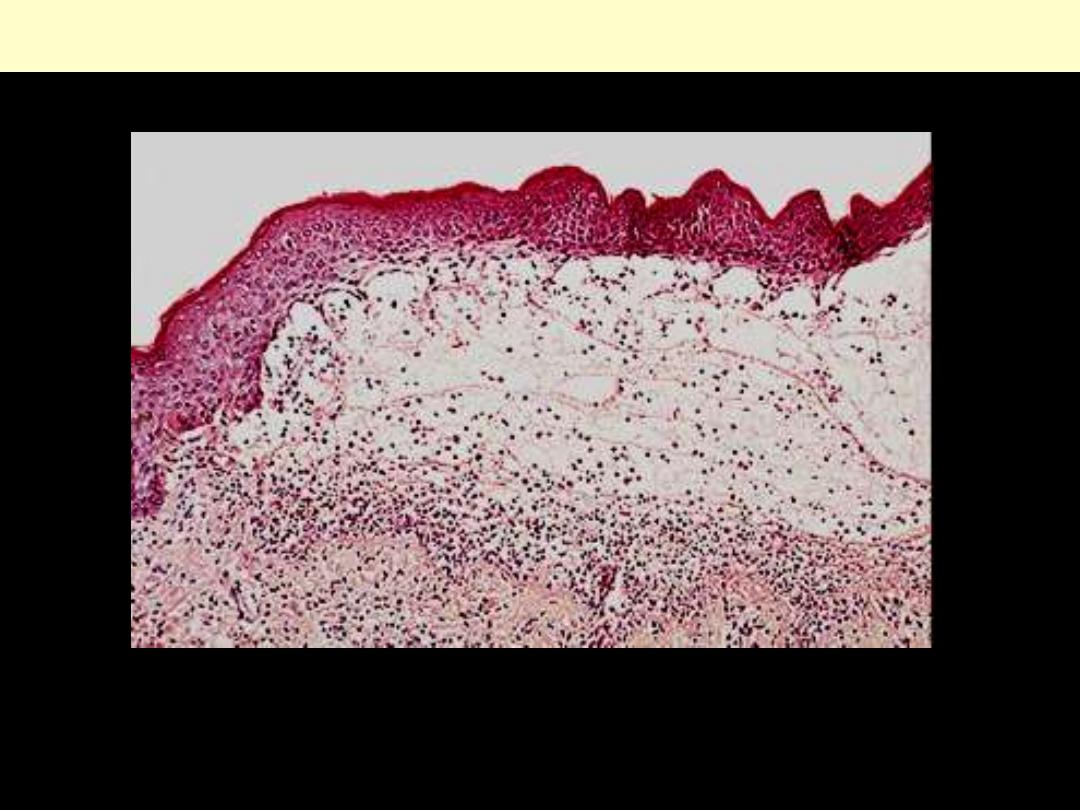
Bullous pemphigoid

Tense, fluid-filled blisters result from vacuolization of the basal layer, producing subepidermal blisters
Bullous pemphigoid
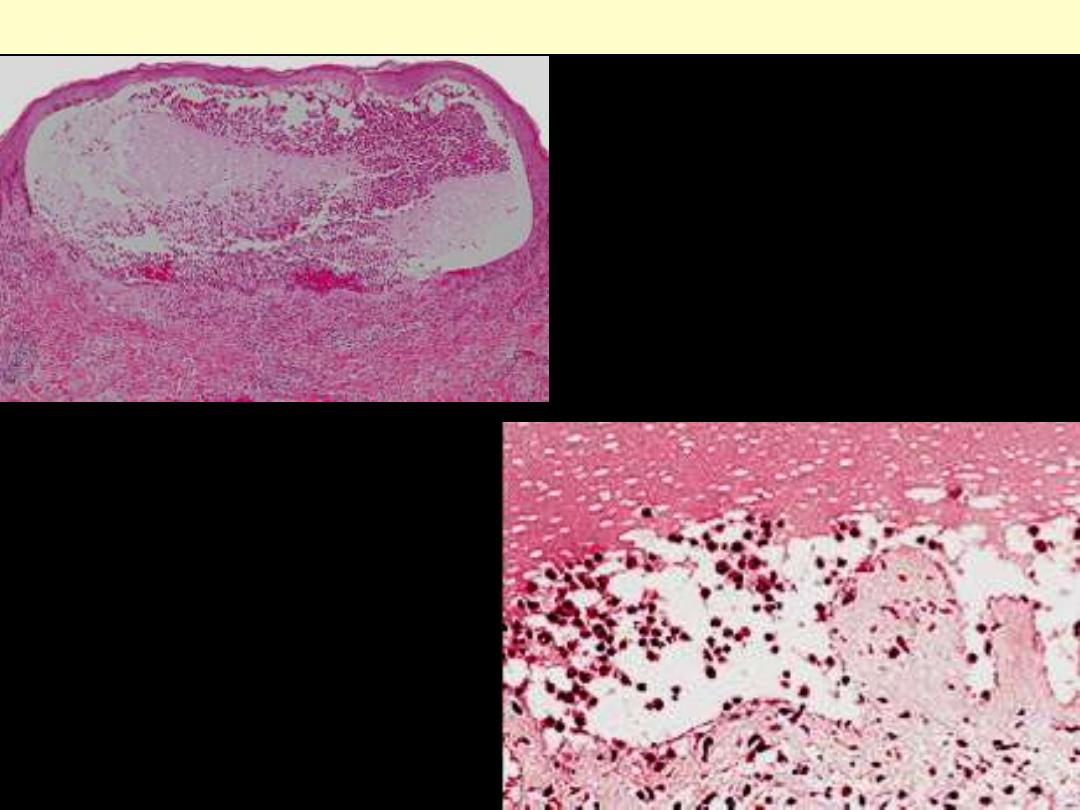
The subepidermal vesicle has an inflammatory
infiltrate rich in eosinophils
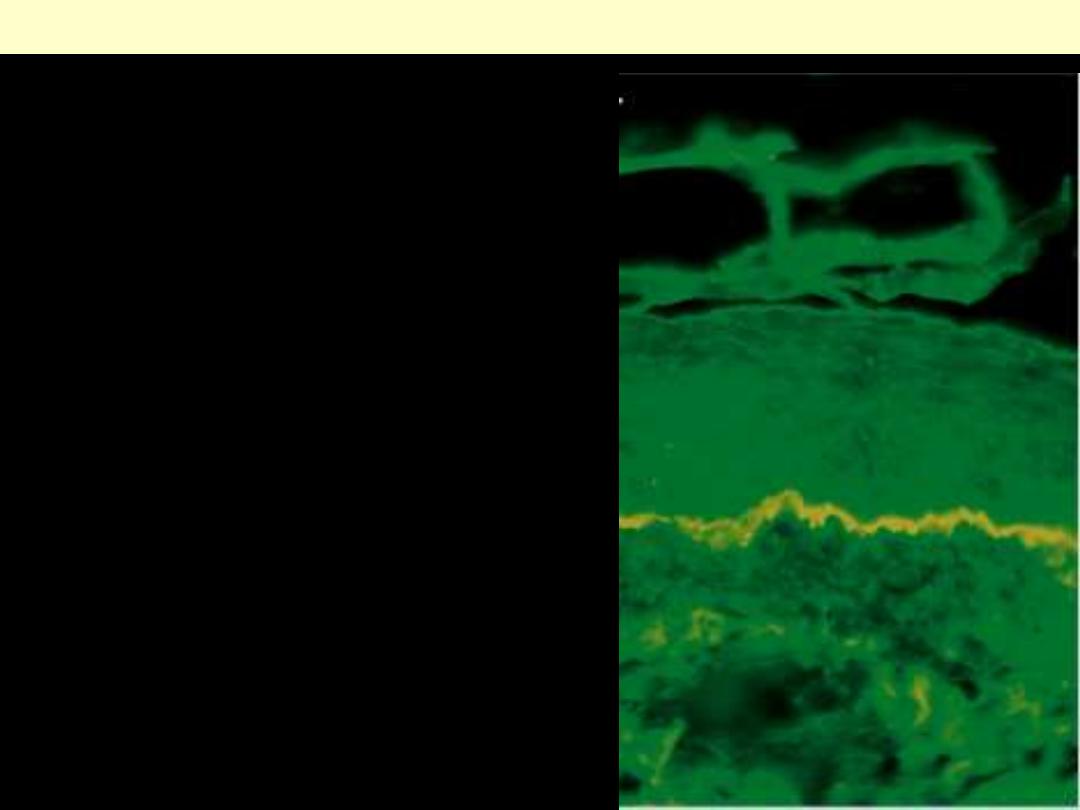
In bullous pemphigoid, both IgG antibody and
complement can be detected by direct
immunofluorescence as a linear band outlining the
subepidermal basement membrane zone
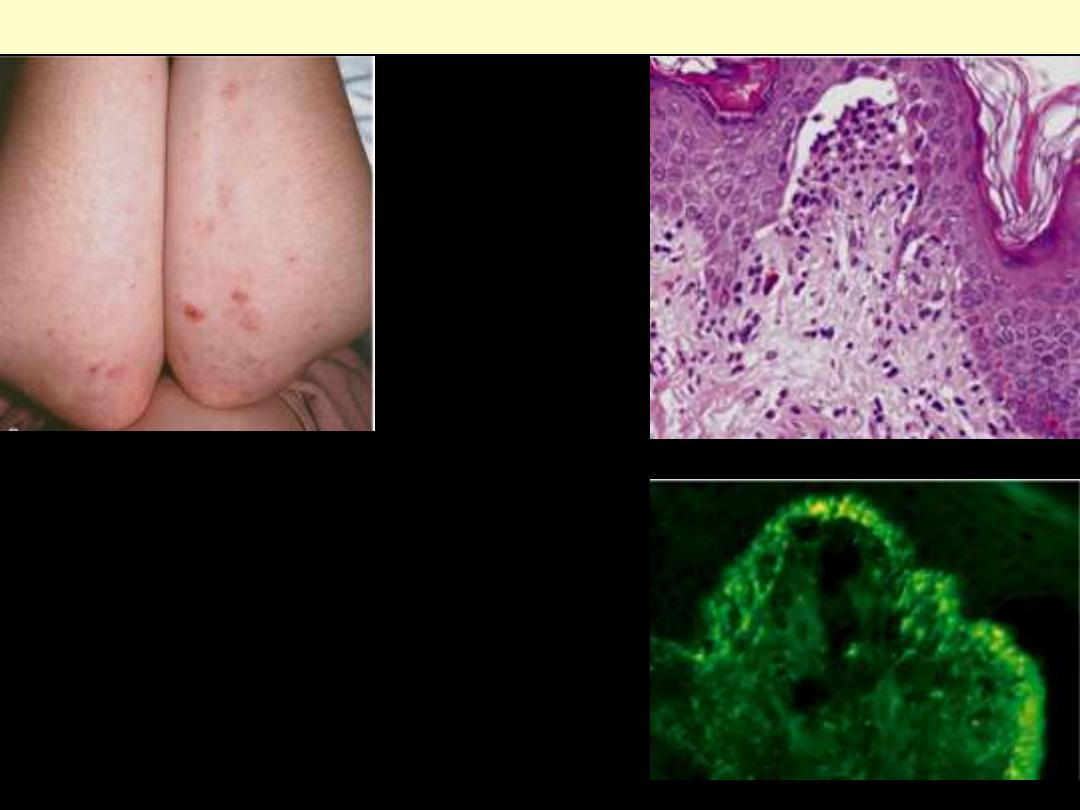
Upper Lt. Lesions consist of intact and eroded
(usually scratched) erythematous blisters, often
grouped (seen here on elbows and arms).
Upper Rt. The blisters are associated with basal
cell layer injury initially caused by
accumulation of neutrophils (microabscesses) at
the tips of dermal papillae.
Lower Rt. Selective deposition of IgA
autoantibody at the tips of dermal papillae is
characteristic.
Dermatitis herpetiformis
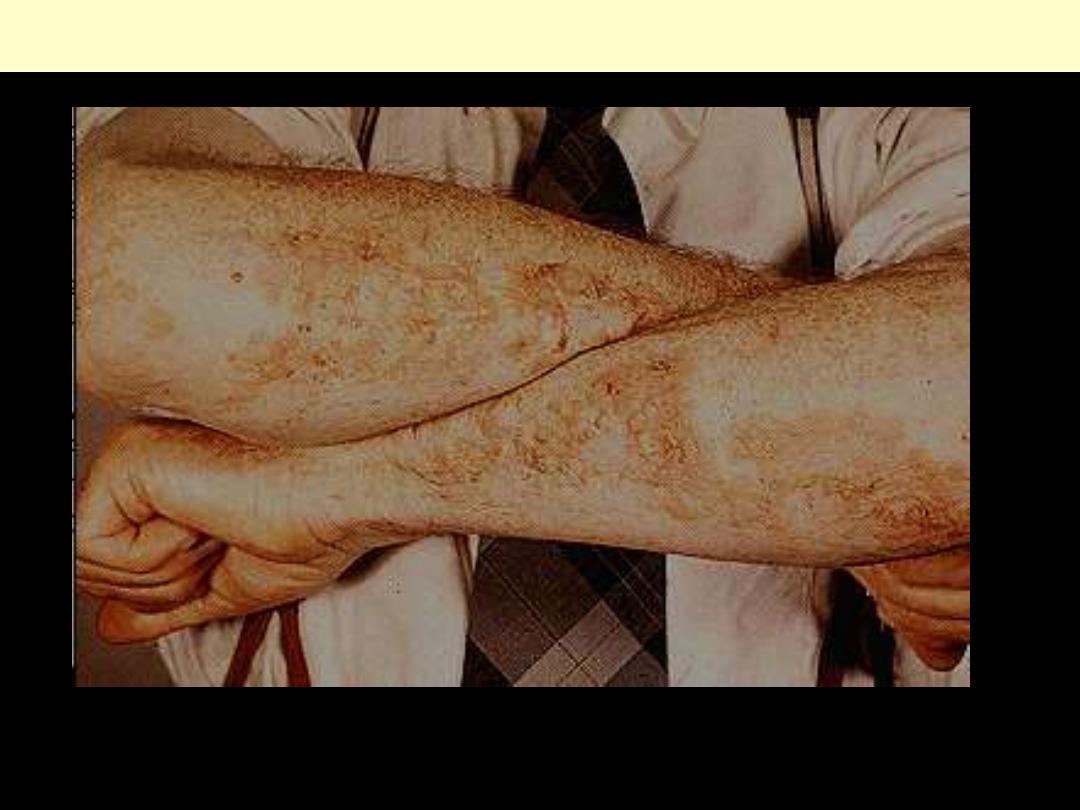
Dermatitis herptiformis
Extensive lesions on the extensor aspects of the forearms

Dermatitis herpetiformis
Dermatitis herptiformis
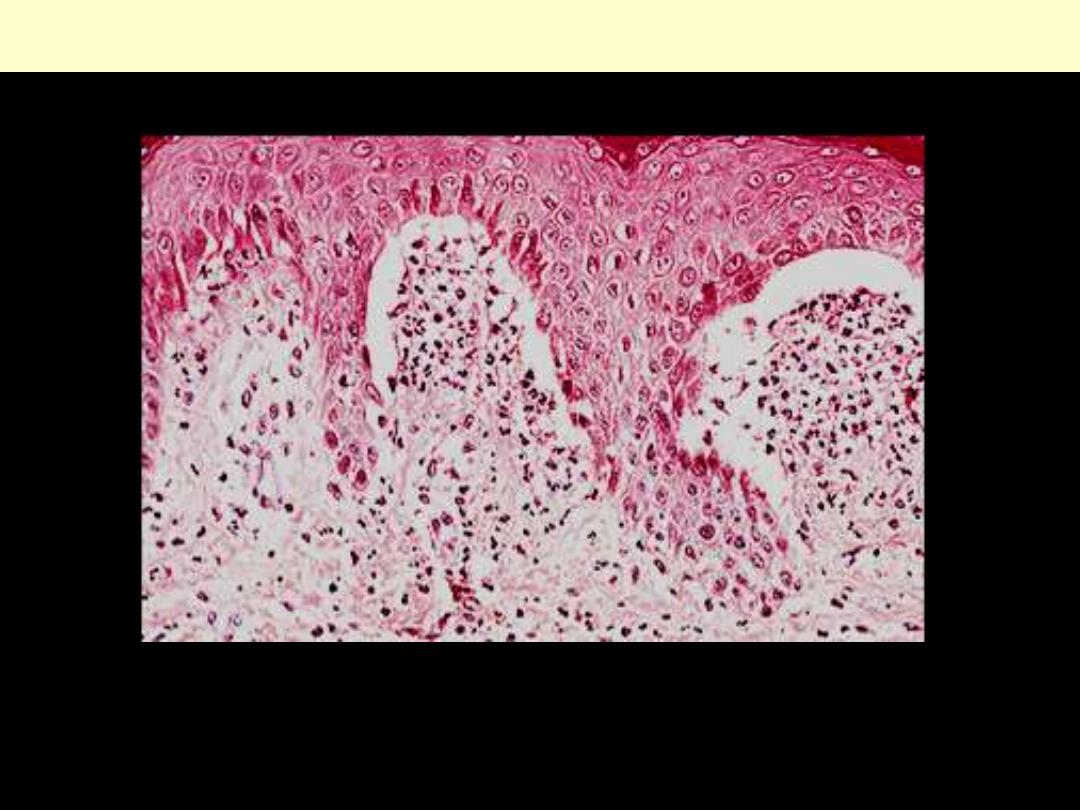
The dermal papillae are distended by microabscesses of neutrophils and fibrin. there is evidence of
early vesiculation.
Dermatitis herptiformis
Part of an established subepidermal blister containing edema fluid, fibrin and neutrophils.
Dermatitis herptiformis
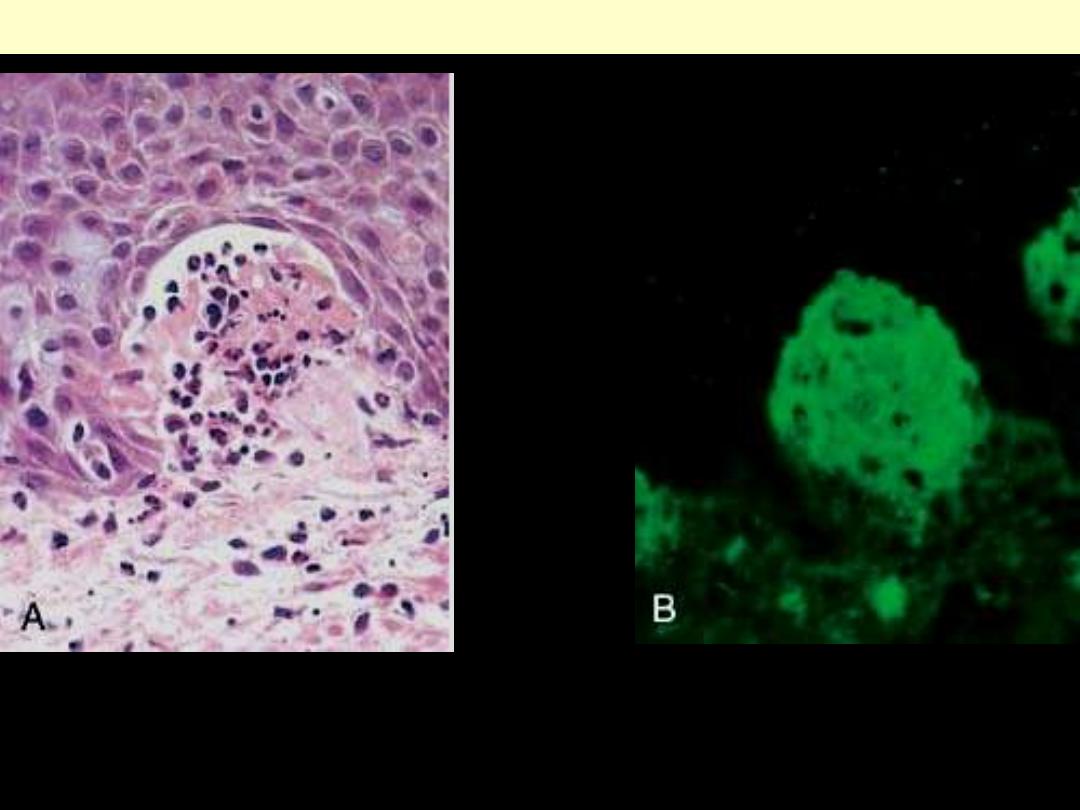
Dermatitis herpetiformis. A, Papillary dermal microabscesses are associated with zones of
dermoepidermal cleavage that eventually coalesce to form a clinical blister. B, By direct
immunofluorescence, these abscesses are rich in IgA and fibrin deposits.
Dermatitis herptiformis
Chronic inflammatory
dermatoses

Typical plaque with an irregular, but
sharply demarcated border showing
the characteristic erythema and silvery
white scaling
Note the symmetrical distribution
Psoriasis
Psoriasis
Typical appearance of psoriasis. Note the
engorgement of papillae and Munro
microabscesses.
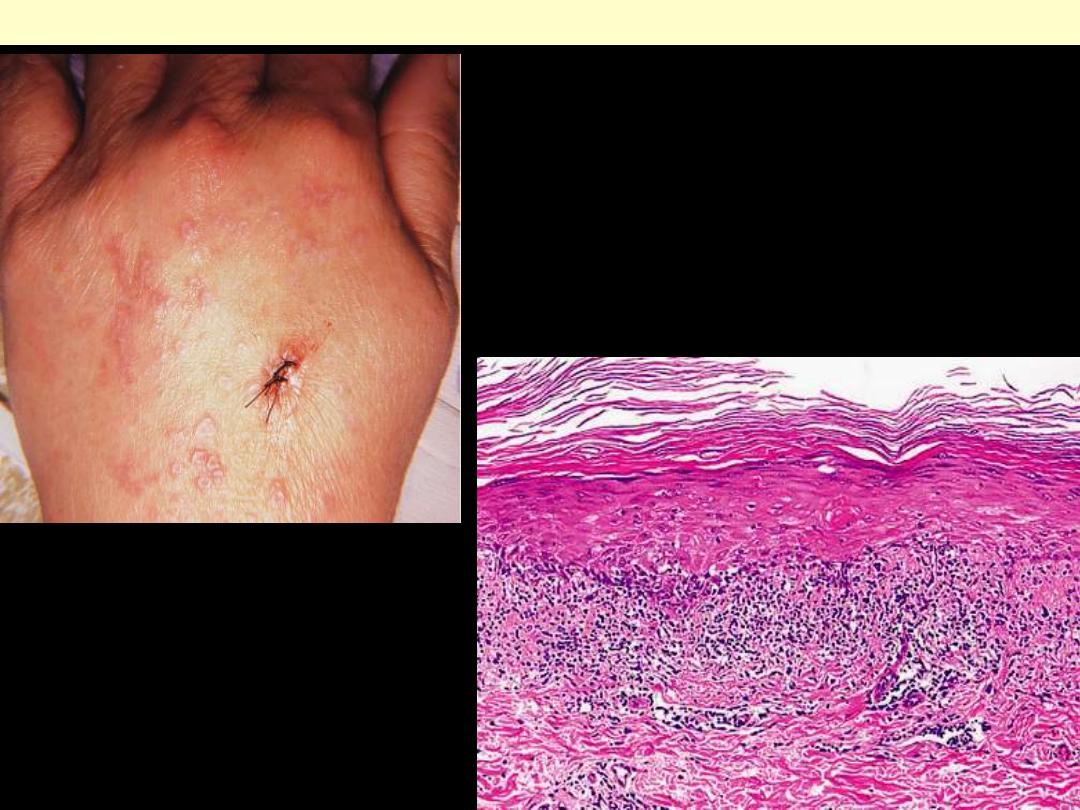
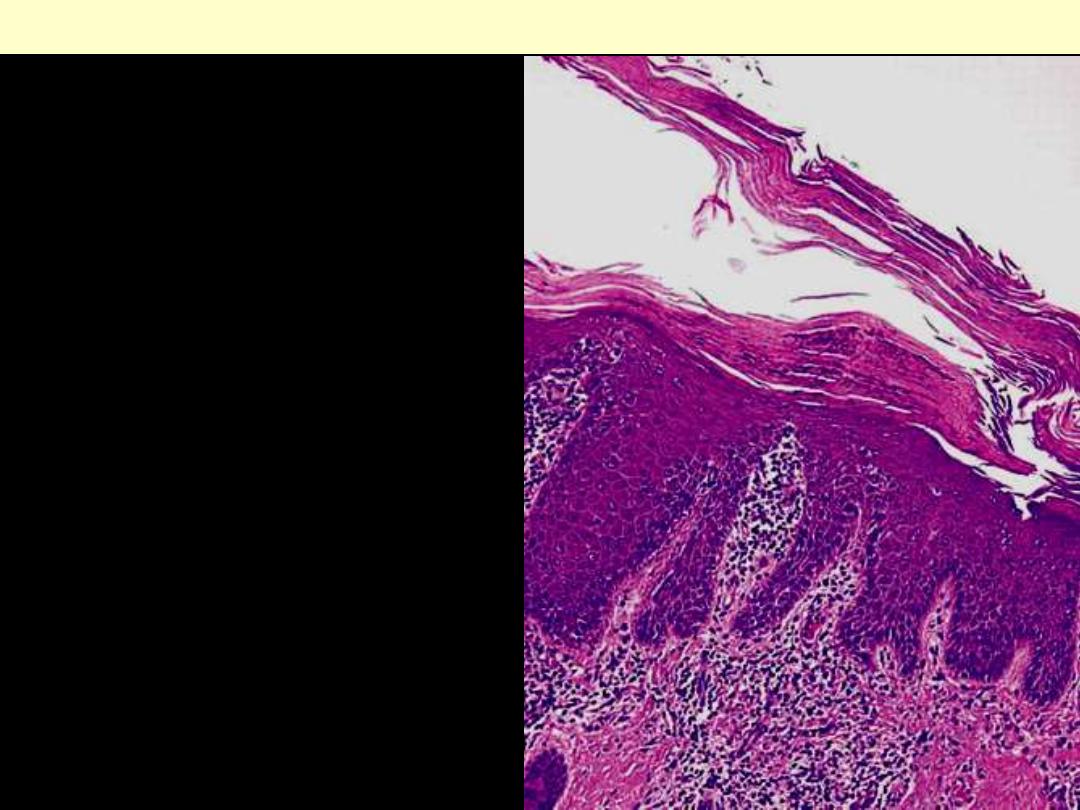
Lichen planus
Clinical appearance of lichen planus affecting the dorsum
of the hand. One of the lesions has been biopsied.
There is hyperkeratosis, hypergranulosis,
hydropic degeneration of the basal layer,
and a band-like inflammatory infiltrate.
Multiple flat-topped papules with white, lacey
or netlike markings (Wickham striae) are
characteristic.
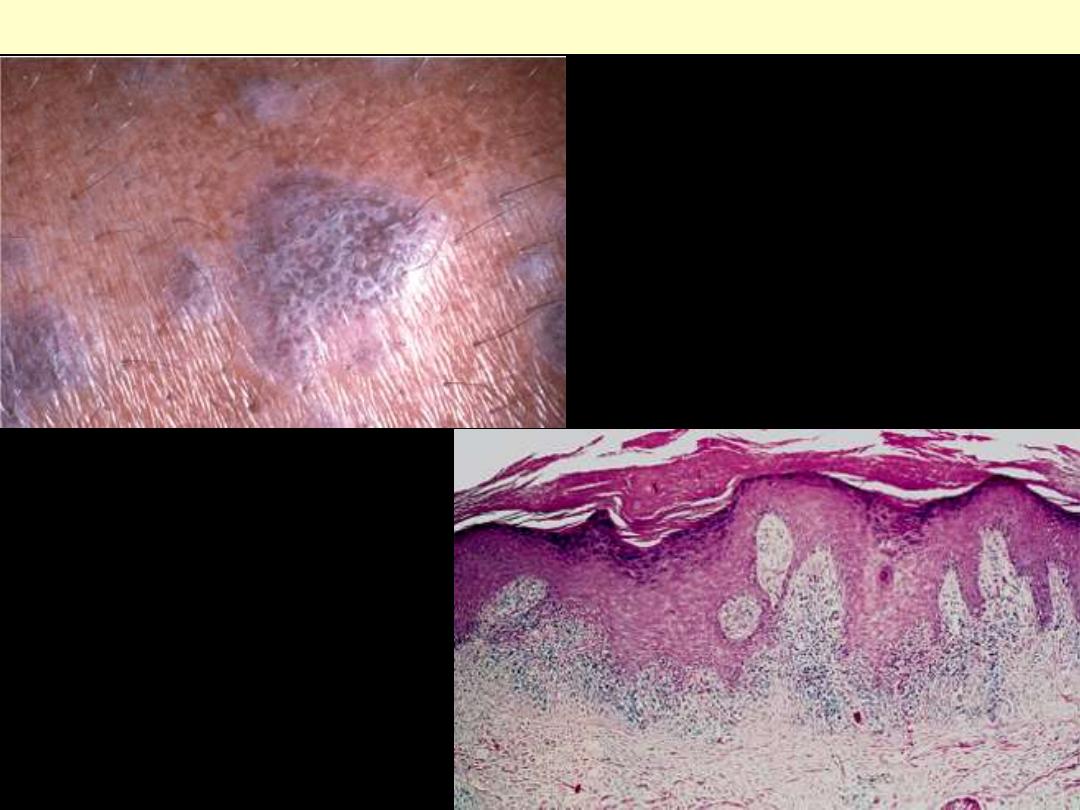
Lichen planus
There is a band of lymphocytes along the
dermoepidermal junction (interface
dermatitis). The rete ridges have acquired
a pointed, or "sawtooth," architecture.
The hyperkeratosis and hypergranulosis
are definite signs of chronicity.
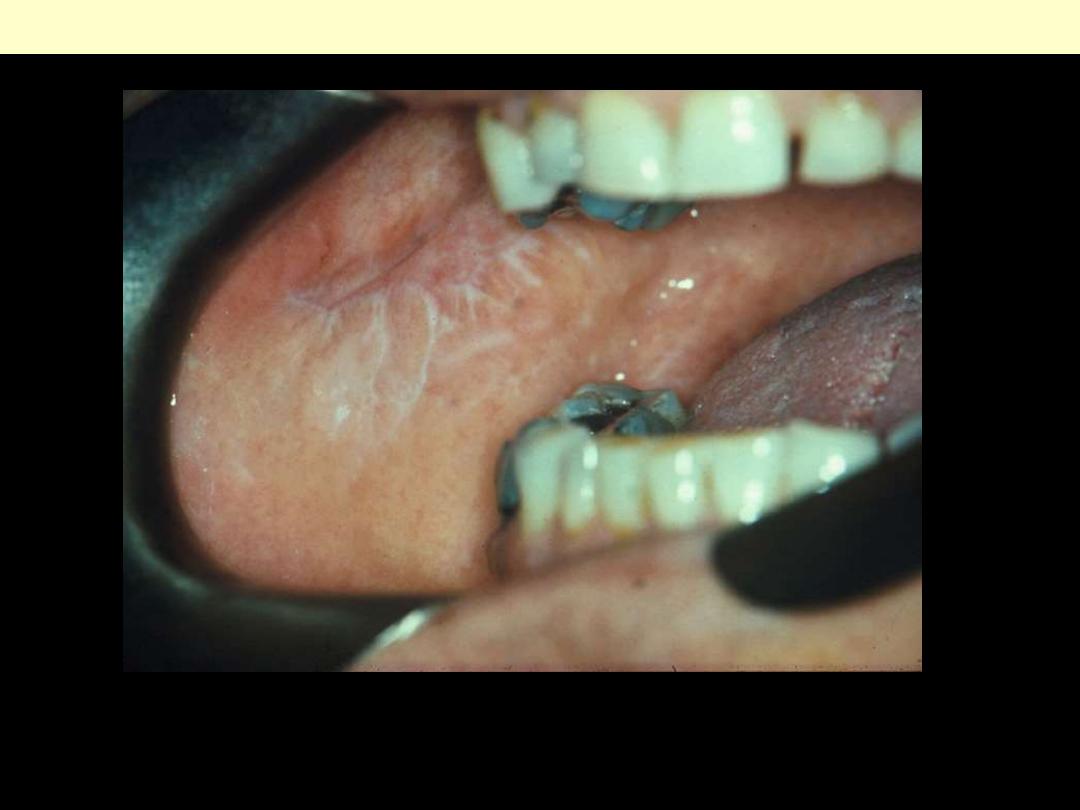
Interlacing white lines (Wickham's striae) of buccal mucosa.
Lichen planus

Acanthosis with hyperkeratosis and hypergranulosis are distinctive. Superficial dermal fibrosis with
vascular ectasia is also common.
Lichen simplex chronicus
Infectious dermatoses

Closer up view
Note that the vesicles are covered by a golden crust.
These perioral lesions are at a characteristic site.
Impetigo

Multiple papules with rough, pebble-like surfaces at infection sites
Verruca vulgaris
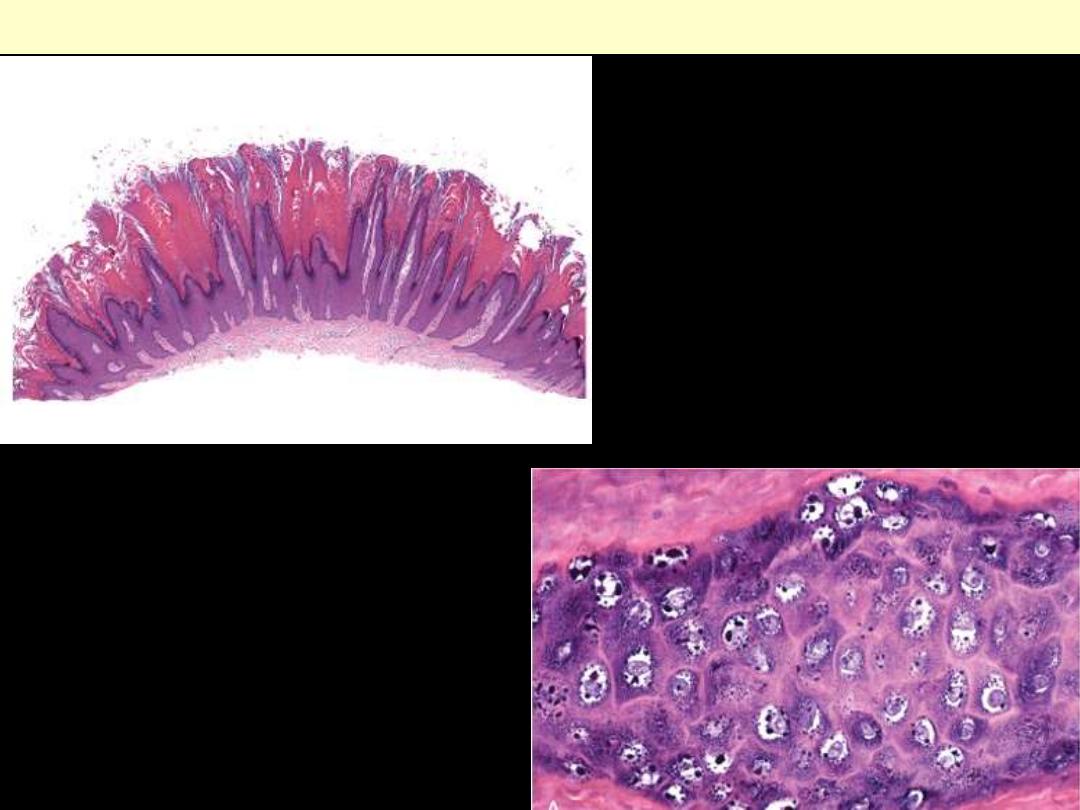
A.
Lesions are formed by symmetric
zones of papillary epidermal
proliferation that often radiate
symmetrically like the points of a
crown (top).
B.
Nuclear pallor, prominent keratohyalin
granules, and related cytopathic
changes of human papillomavirus are
confirmed at higher magnification
(bottom).
Verruca vulgaris
Melanocytes - abnormalities
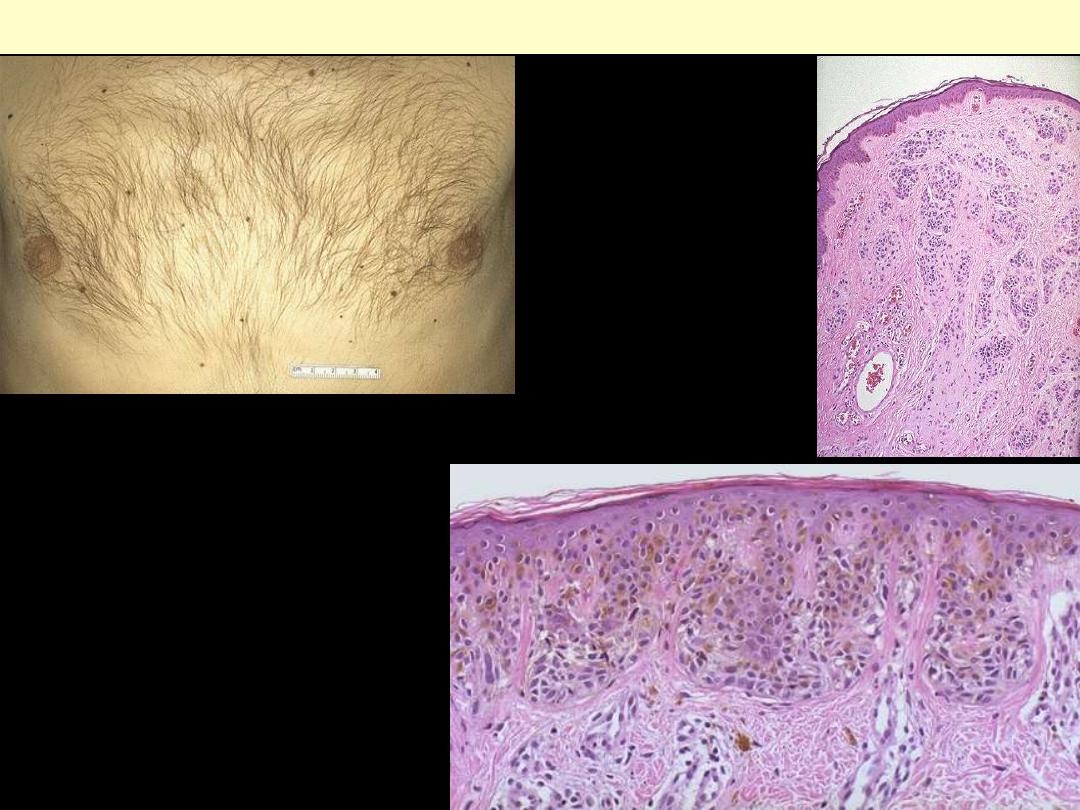
A. These are benign nevi. Small brown flat to
slightly raised nevi. They are usually less
than a centimeter in diameter.
B. LP micro appearance of a benign
pigmented nevus. Small amounts of dark
pigment are seen near the skin surface. The
small blue nevus cells can extend into the
dermis and around adnexal structures, but
this is not invasion.
C. In this junctional nevus, there are nevus
cells in nests in the lower epidermis as well
as nests appearing to "drop off" into the
upper dermis. Unlike a melanoma, there is
no significant atypia and no inflammation.
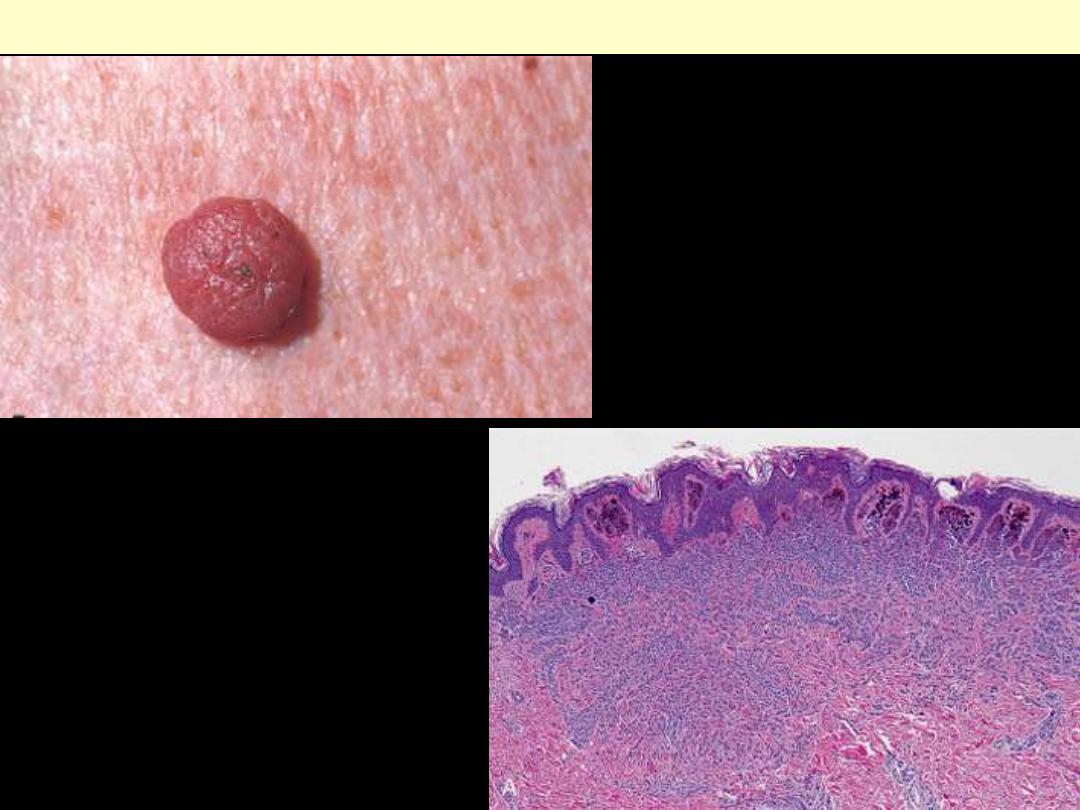
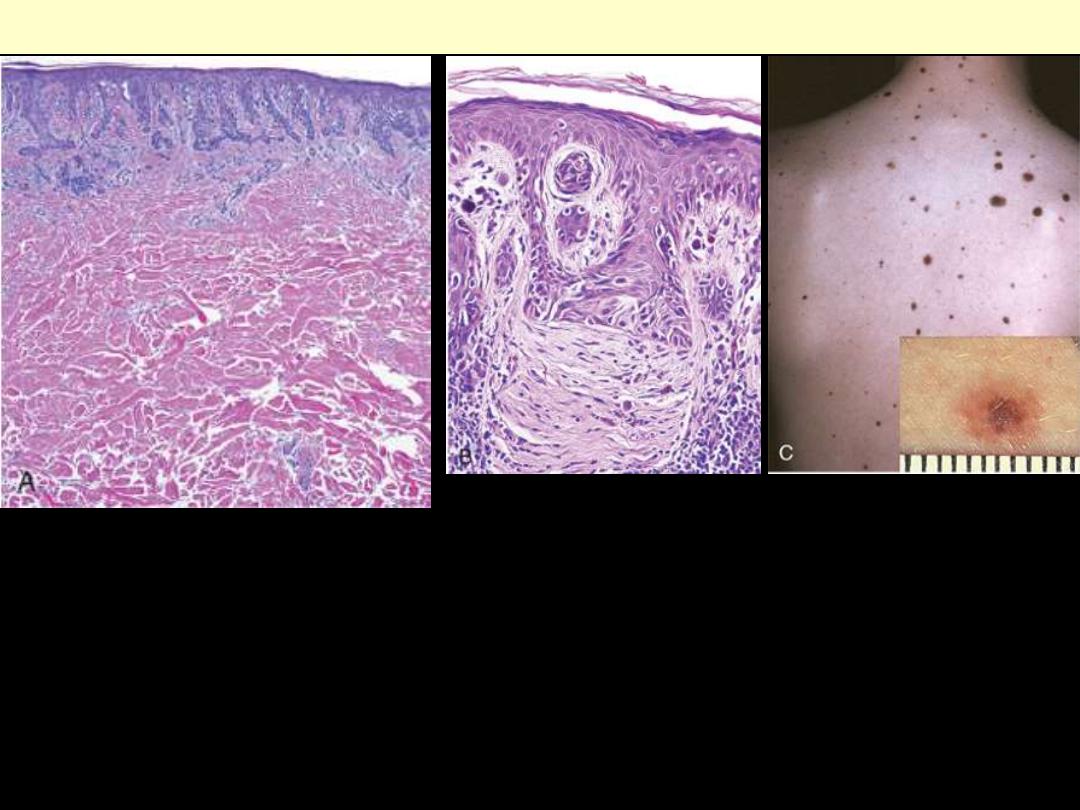
A, Melanocytic nevi are relatively small,
symmetric, and uniformly pigmented.
B. This dermal nevus shows rounded
melanocytes extending into the dermis with
loss of pigmentation and cells becoming
smaller and more separated with depth-all
reassuring signs of appropriate maturation.
Melanocytic nevus
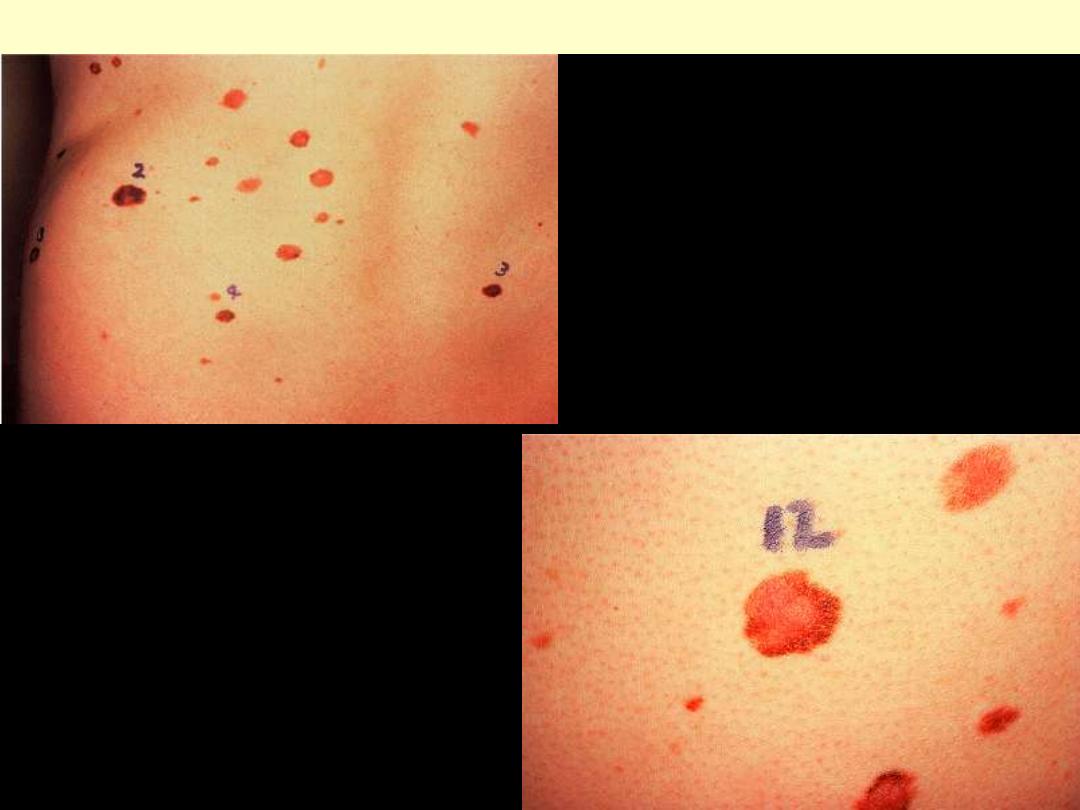
Dysplastic nevus syndrome
Clinical appearance of dysplastic nevi in
patient with the dysplastic nevus syndrome.
These nevi are large, have an irregular outline,
and feature a variegated appearance.
A, Compound dysplastic nevi feature a central dermal component with an asymmetric "shoulder" of
exclusively junctional melanocytes (left). The former correlates with the more pigmented and raised
central zone (see C, inset), and the latter with the less pigmented flat peripheral rim. B, An important
feature is the presence of cytologic atypia (irregular, dark-staining nuclei) at high magnification. The
dermis shows peculiar but characteristic parallel bands of fibrosis often encountered in dysplastic nevi-
part of the host response to these lesions. C, Numerous irregular nevi on the back of this individual
suggest the dysplastic nevus syndrome; the clinical features are intermediate to those of benign nevi
and melanoma. The lesions are usually greater than 5mm in diameter with irregular borders and
variable pigmentation (inset).
Dysplastic nevus
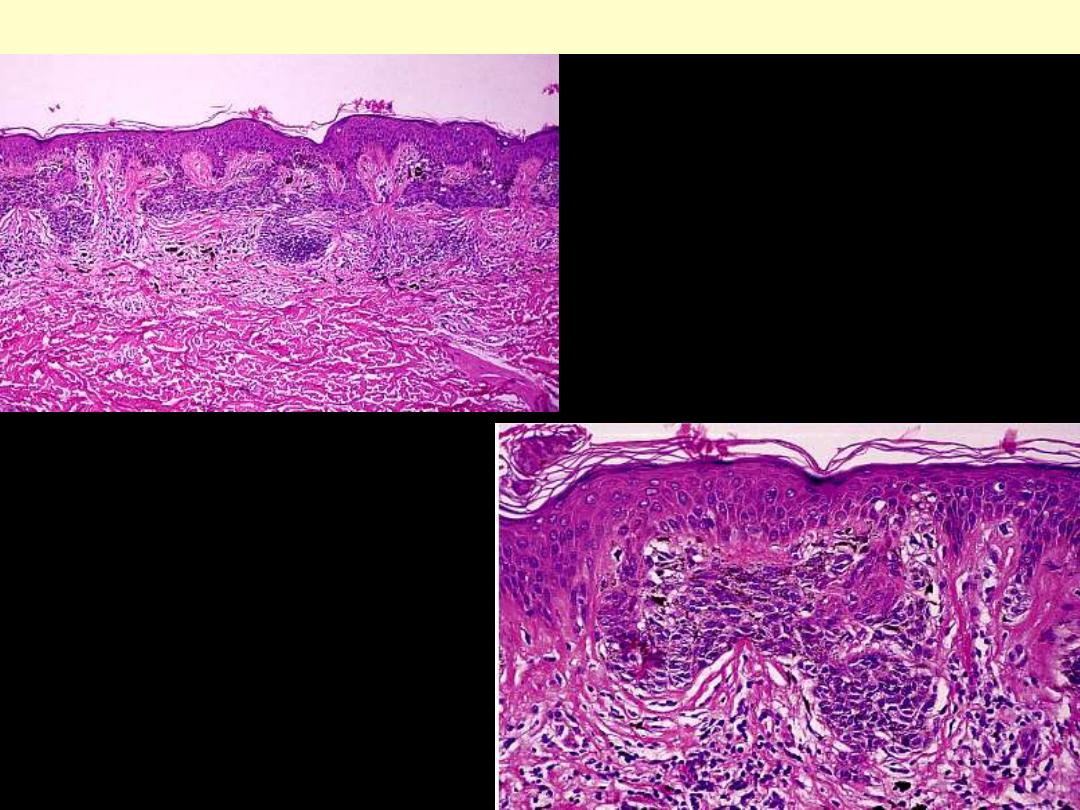
There is dermal fibrosis, inflammation, and a
proliferation of melanocytes at the dermo-
epidermal junction, with bridging of rete
ridges.
Dysplastic nevus
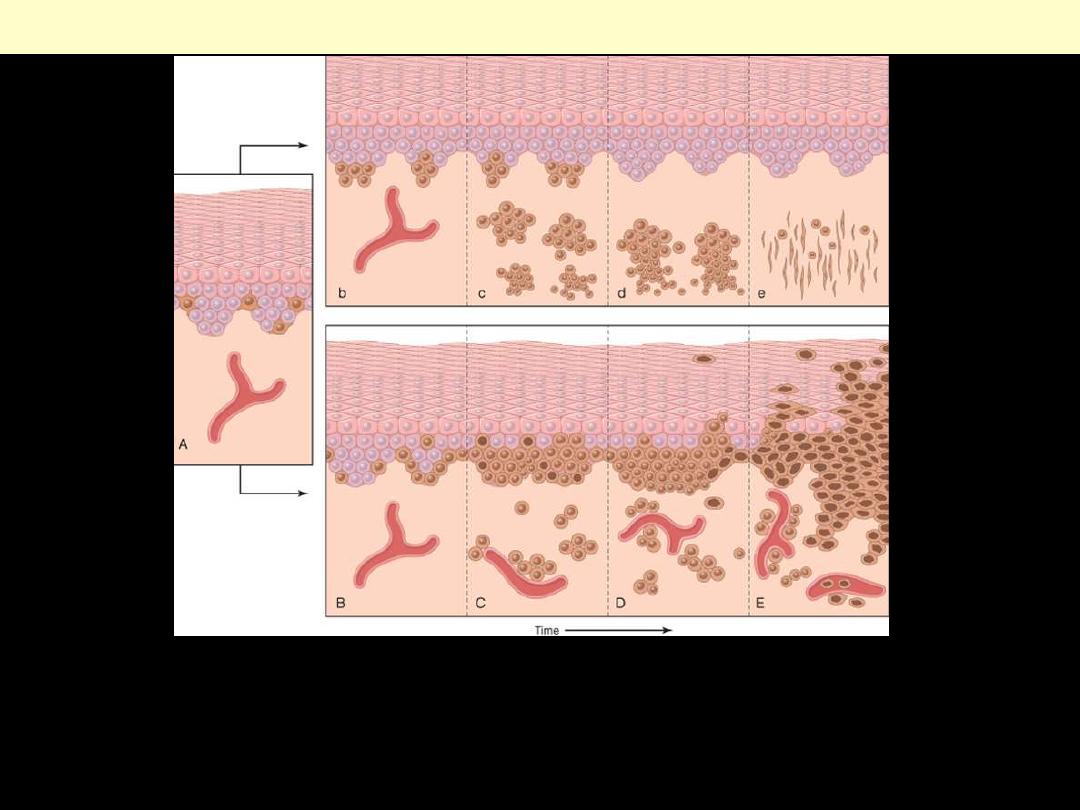
A, Normal skin shows only scattered melanocytes. Top row: b, Junctional nevus. c, Compound nevus. d, Intradermal
nevus. e, Intradermal nevus with neurotization (extreme maturation). Bottom row: B, Lentiginous melanocytic
hyperplasia. C, Lentiginous compound nevus with abnormal architecture and cytologic features (dysplastic nevus). D,
Early or radial growth-phase melanoma (large dark cells in epidermis) arising in a nevus. E, Melanoma in vertical
growth phase with metastatic potential. Note that no melanocytic nevus precursor is identified in most cases of
melanoma. They are believed to arise de novo, perhaps using the same pathway.
Possible steps in development of melanocytic nevi and melanoma
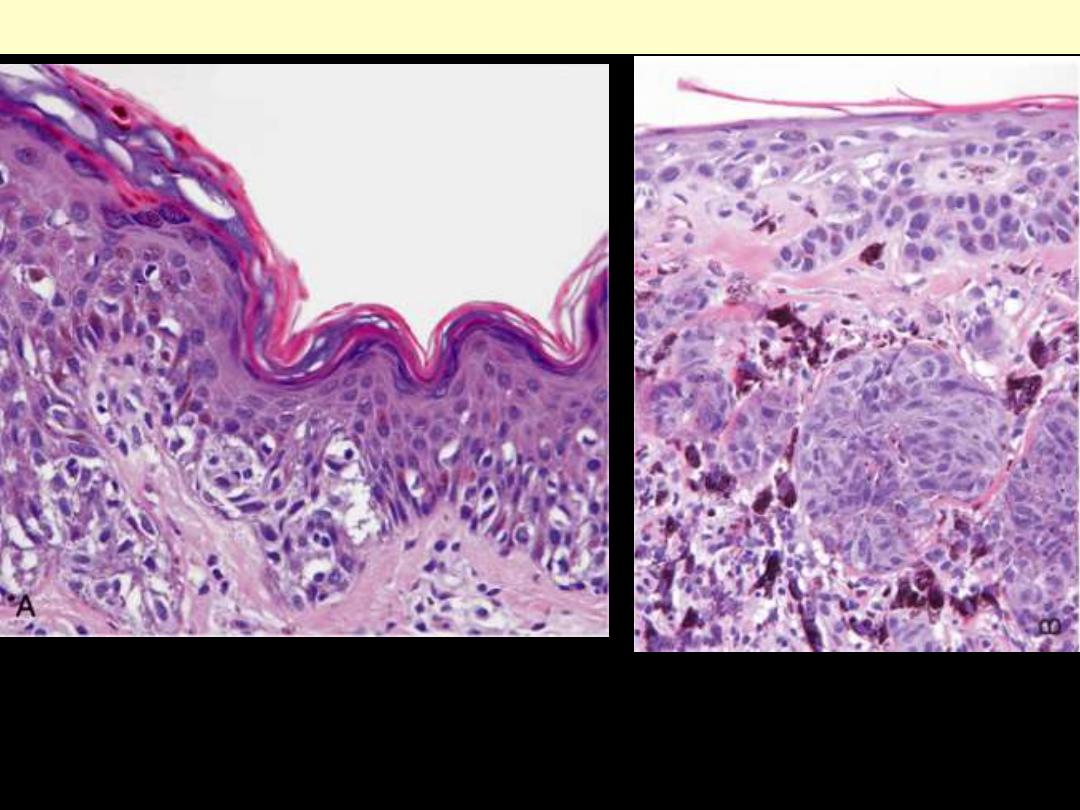
A, Radial growth, showing irregular nested and single-cell spread of melanoma cells in the epidermis.
B, Vertical growth showing nodular aggregates of malignant cells extending deeply within the dermis.
Melanoma
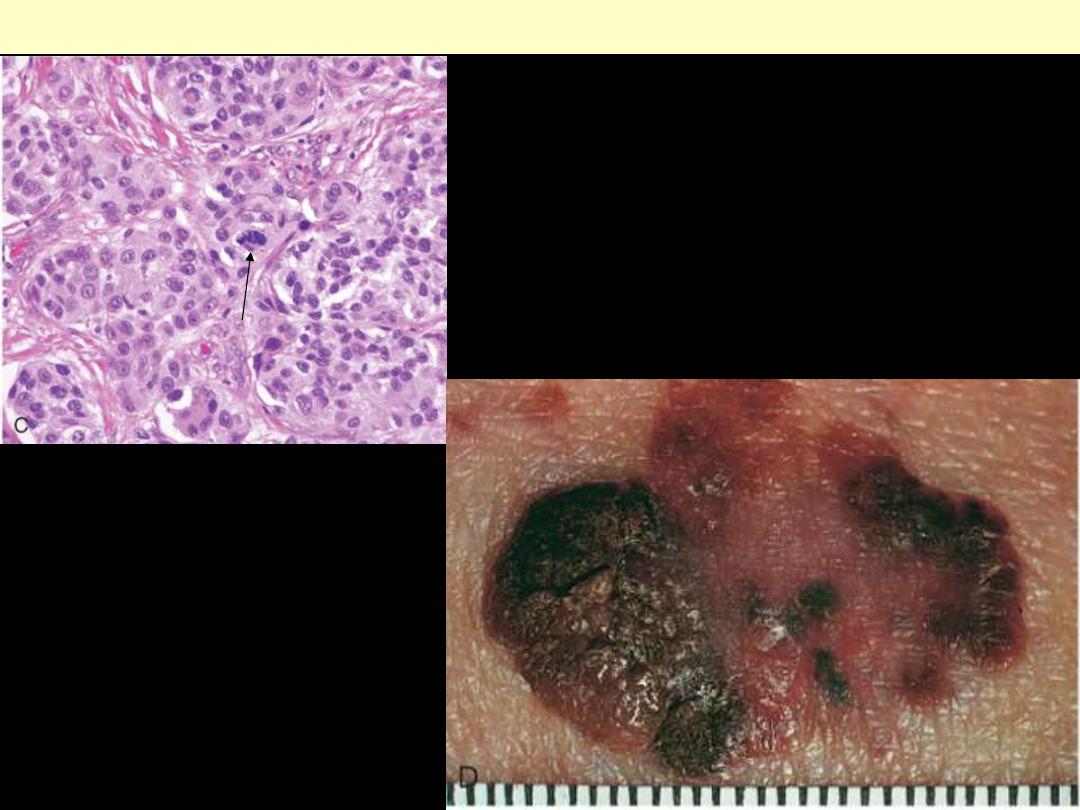
C, Melanoma cells have hyperchromatic nuclei of
irregular size and shape with prominent nucleoli. Mitoses,
including atypical forms (arrow), are often encountered.
D, Lesions clinically tend to be larger than nevi, with
irregular contours and pigmentation. Macular areas are
early superficial (radial) growth, while elevated areas
often indicate dermal invasion (vertical growth).
Melanoma
Tumors
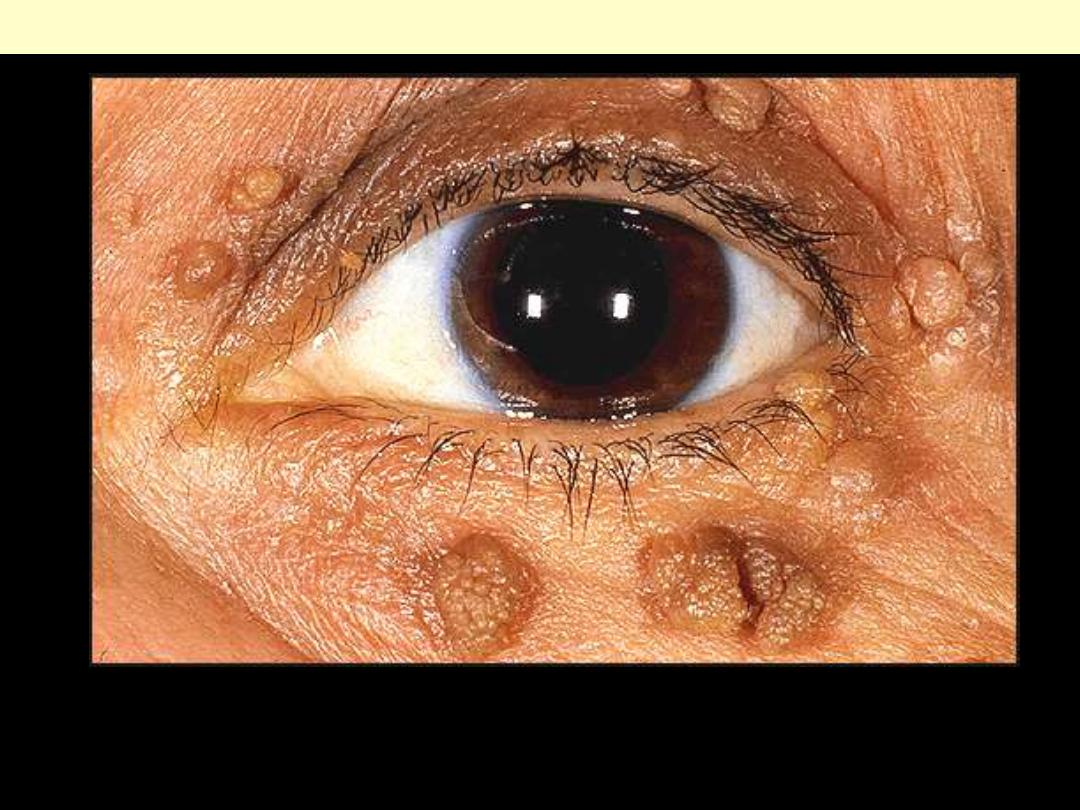
Seborreic keratosis appears to be "stuck onto" the surface of the skin. commonly it has a complex
surface with numerous grooves. it may be pigmented and this should not be confused with melanoma.
SK is common.; the sudden appearance of multiple, large seborrheic keratoses may be a
dermatological marker of malignancy.
Seborrheic keratosis eyelid
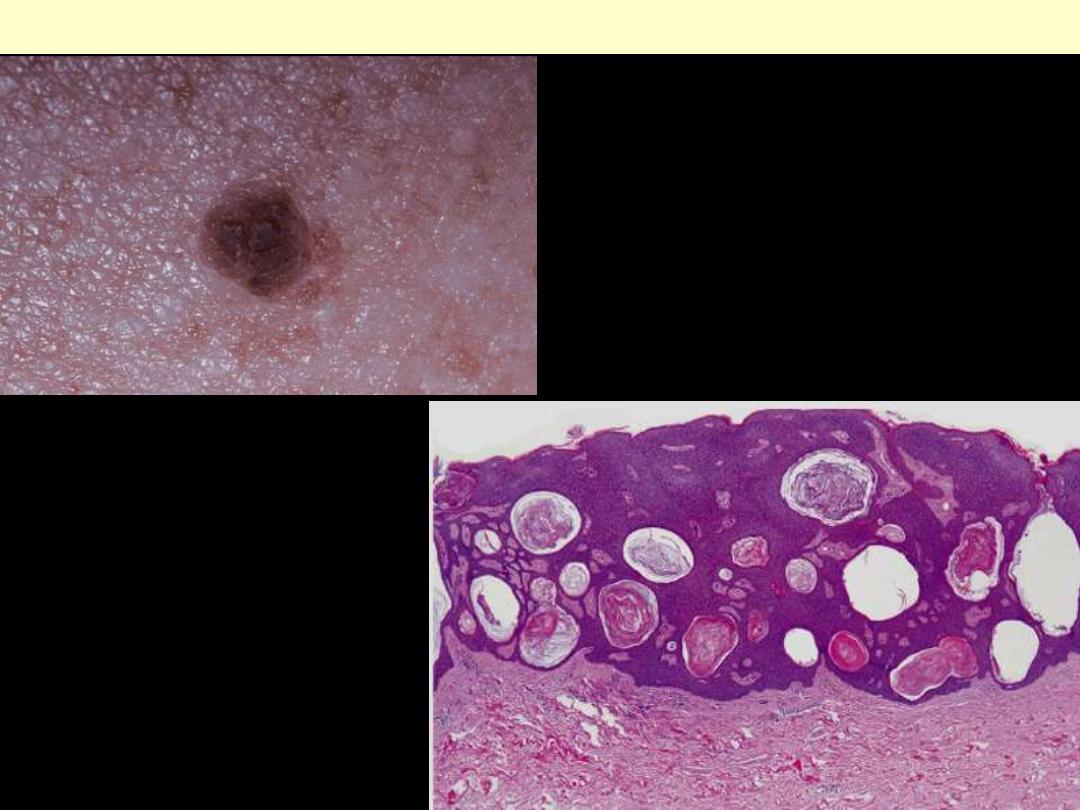
A. This roughened, brown, waxy lesion almost
appears to be "stuck on" the skin.
B. The lesions consist of an orderly proliferation
of uniform, benign basaloid keratinocytes with a
tendency to form keratin microcysts (horn cysts).
Seborrheic keratosis
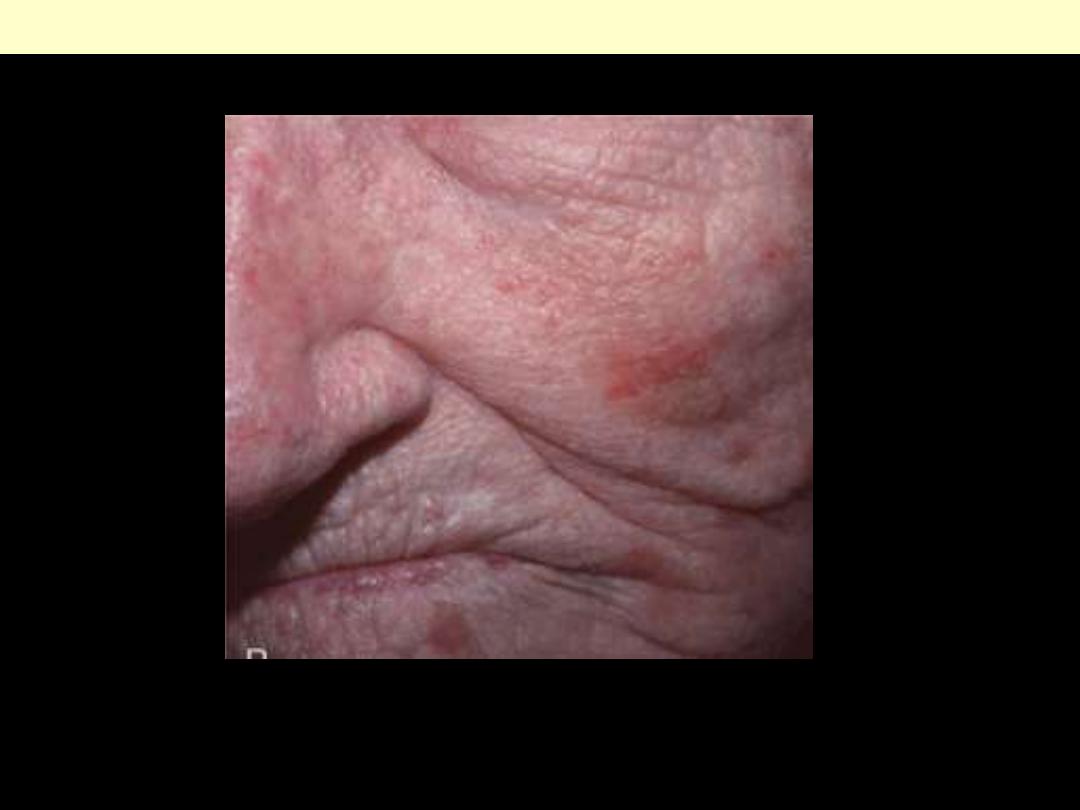
Most lesions form subtle zones of redness or sandpaper-like keratinization as seen in the lesions on the
cheek, nose, and chin of this woman
Actinic keratosis
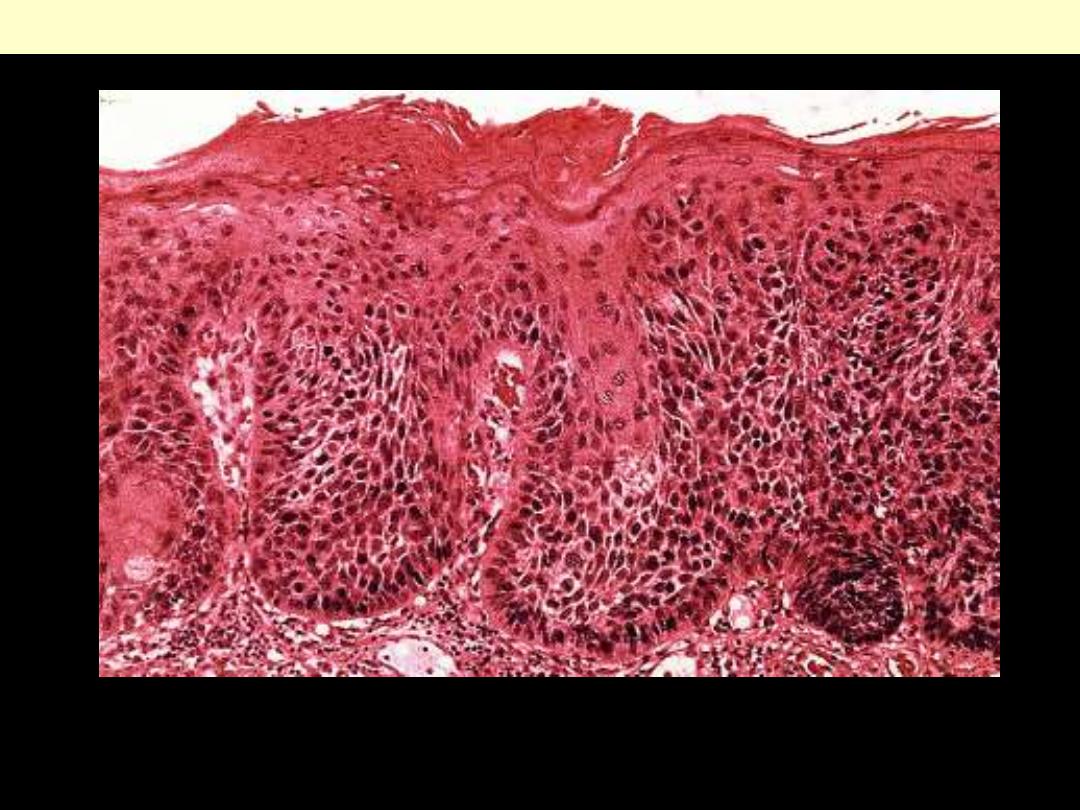
Actinic keratosis with moderate dysplasia
The lower portions of the epidermis show cytologic atypia, often with hyperplasia of basal cells with
moderate dysplasia. There is hyper- and parakeratosis. Lymphocytes are present in superficial dermis
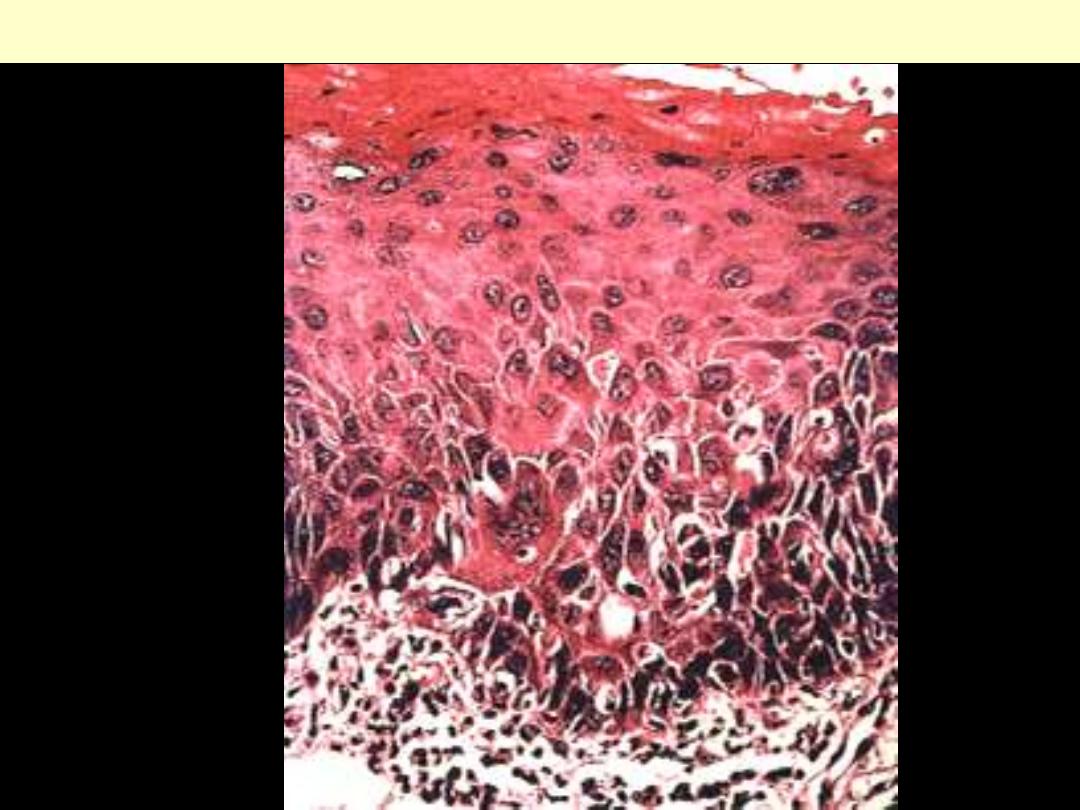
Actinic keratosis with Severe dysplasia
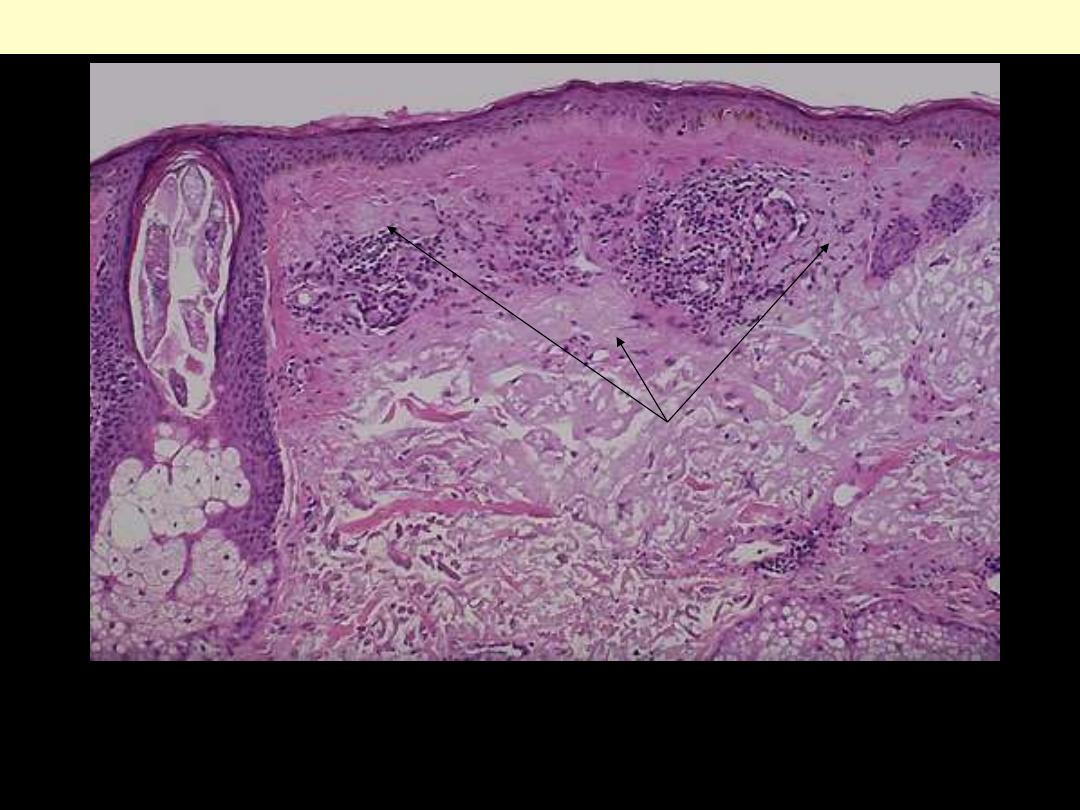
Sun exposure damages the skin, primarily as the result of ultraviolet light. This actinic damage is seen
as a collection of abnormal collagen fibers in the upper dermis, seen here with a pale bluish appearance
(basophilic degeneration) (arrows). Note the epidermal atrophy.
Solar (actinic) keratosis

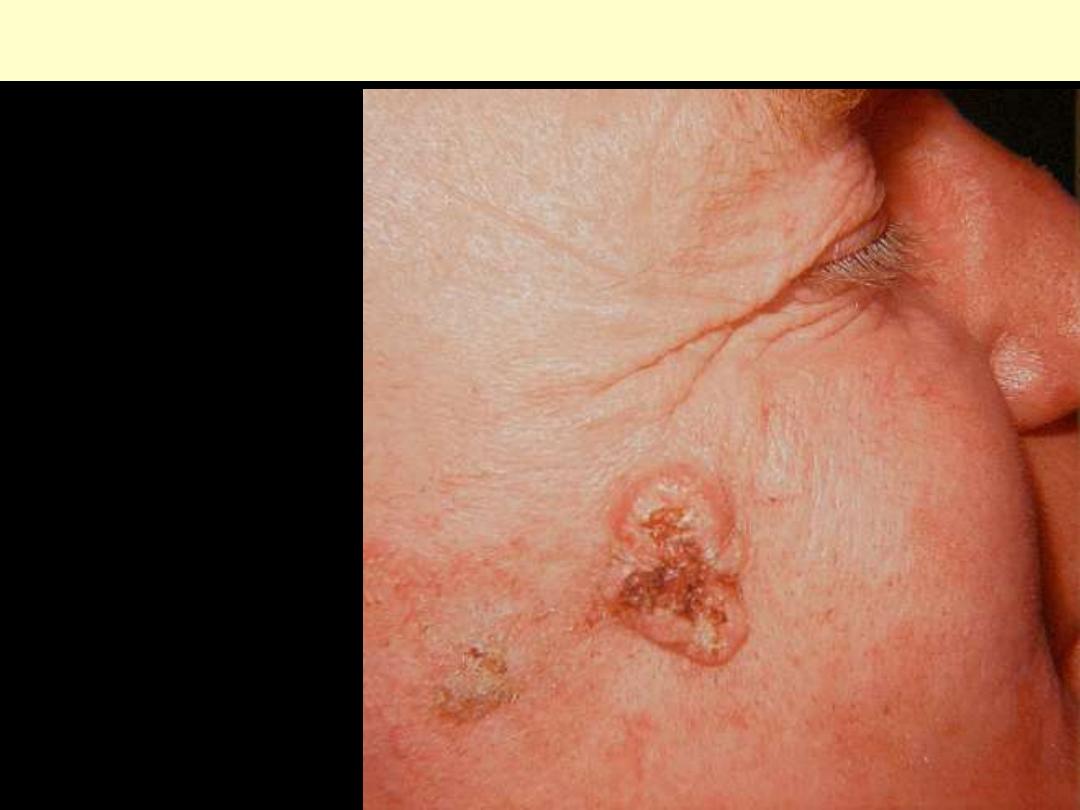
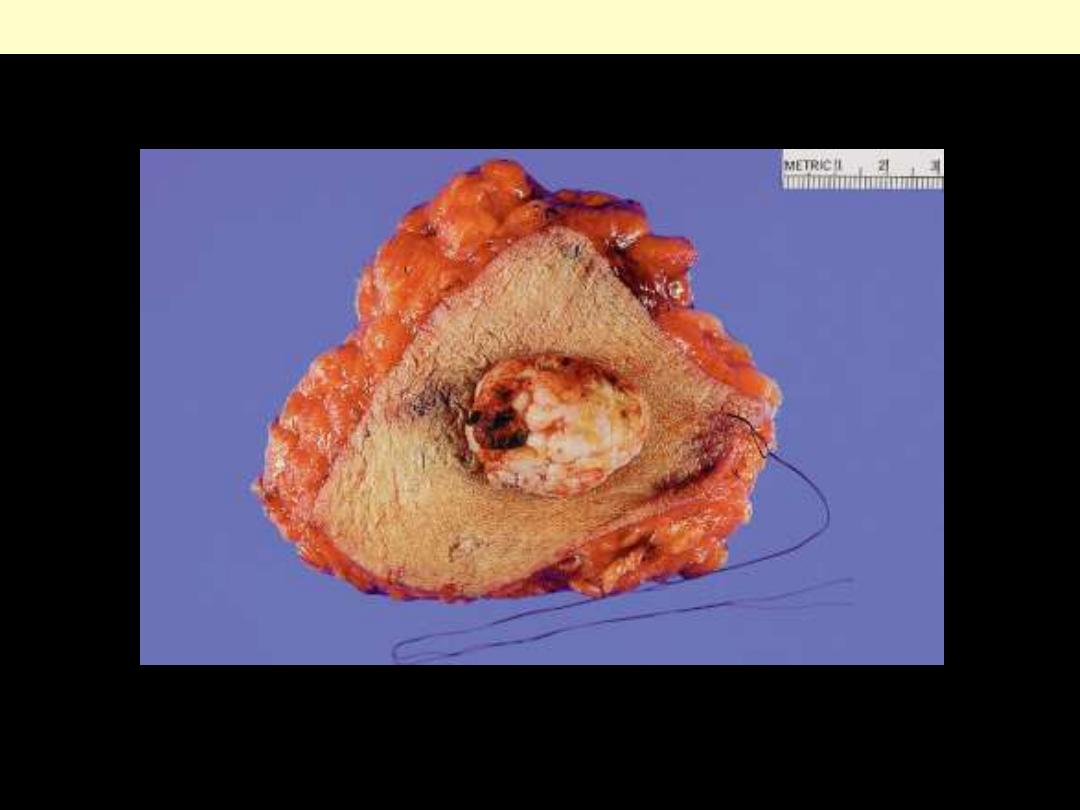
A nodular and hyperkeratotic lesion occurring on the ear, unfortunately with early metastasis to a
prominent postauricular lymph node (arrow).
Squamous cell carcinoma
Squamous cell ca skin
Tumor of the face with rolled
edges and depressed center.
SCC of the leg with exophytic appearance.

Well-differentiated SCC showing deep invasion
The tumor is formed by atypical squamous cells arranged in orderly lobules showing large zones of
keratinization.
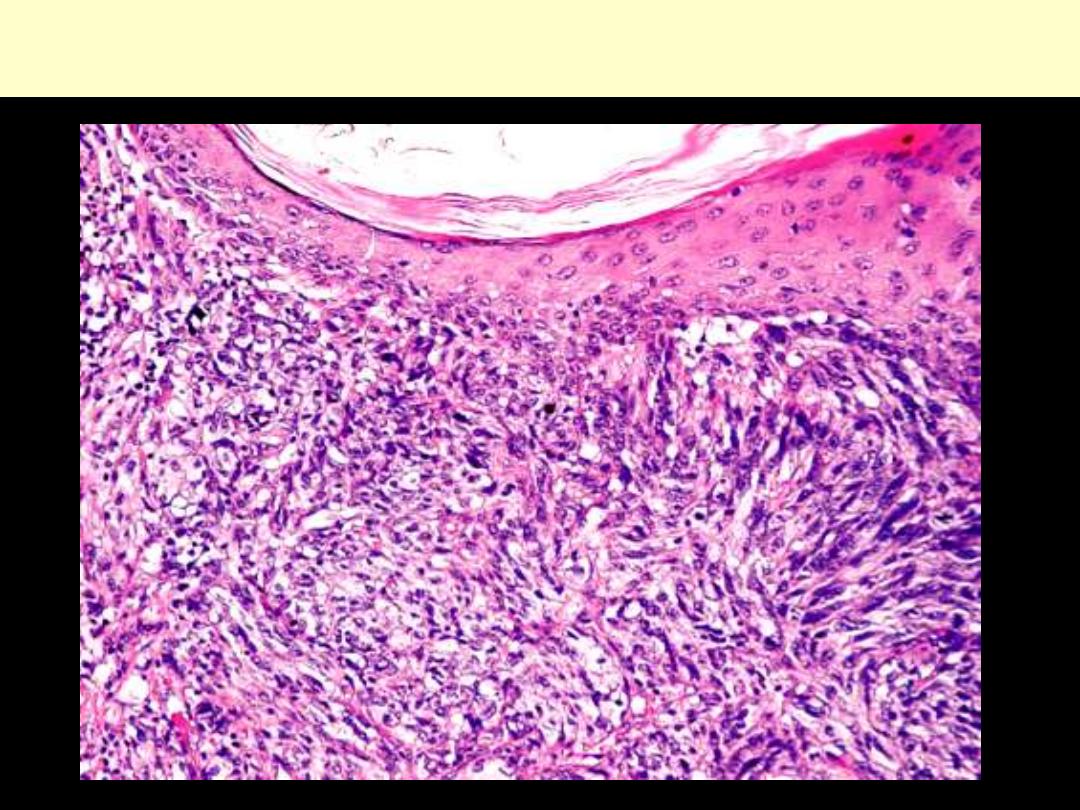
Poorly- differentiated Squamous cell carcinoma showing spindle
metaplastic features (sarcomatoid SCC)
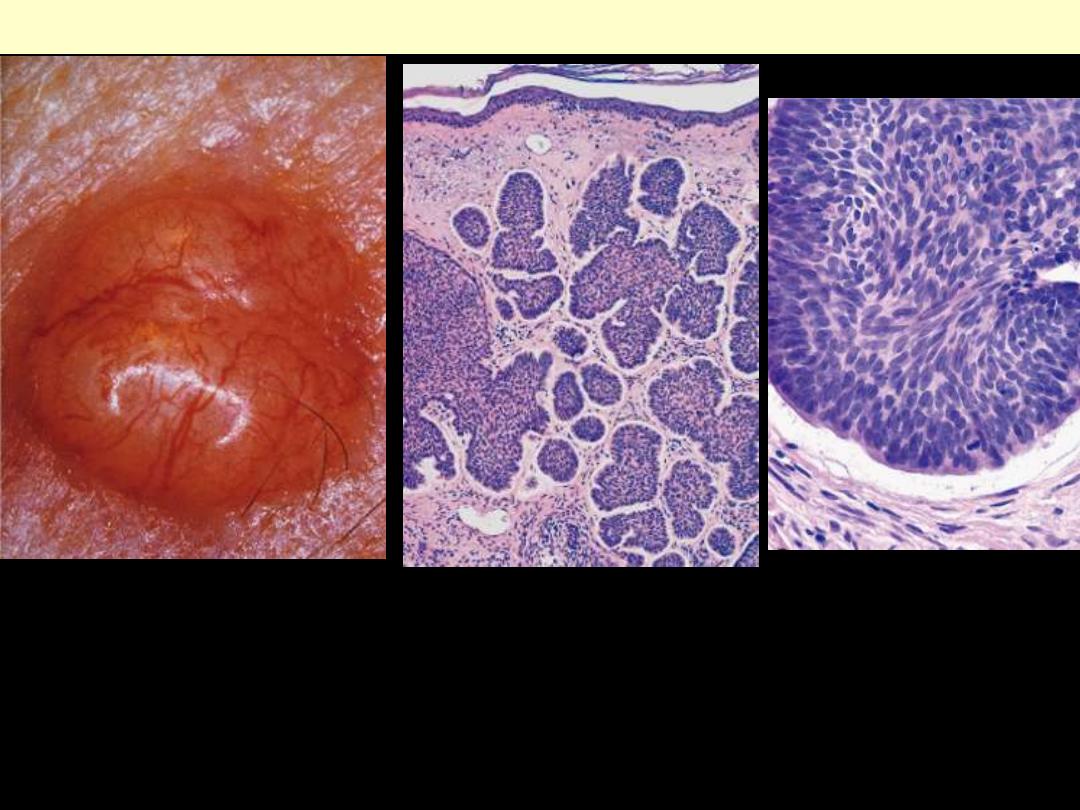
A.
This lesion is a prototypical pearly, smooth-surfaced papule with associated telangiectatic vessels
B.
The lesion is formed by multiple nodules of basaloid cells infiltrating a fibrotic stroma.
C.
The cells have scant cytoplasm, small hyperchromatic nuclei, and a peripheral palisade with
clefting from the stroma. Note the similarity of these cells to the basal cells of normal epithelium.
Basal cell carcinoma
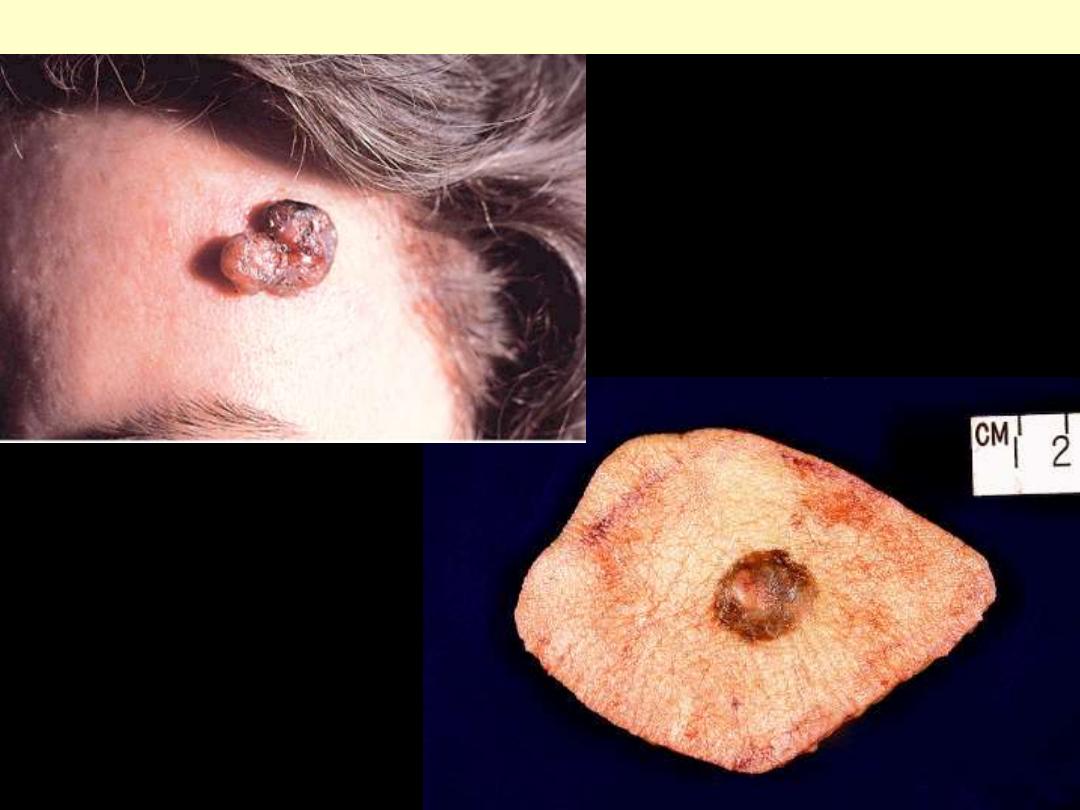
Nodular and pigmented basal cell carcinoma of forehead
Clinical appearance of pigmented
basal cell carcinoma. Melanin is
largely present in macrophages
located in the stroma between tumor
lobules.
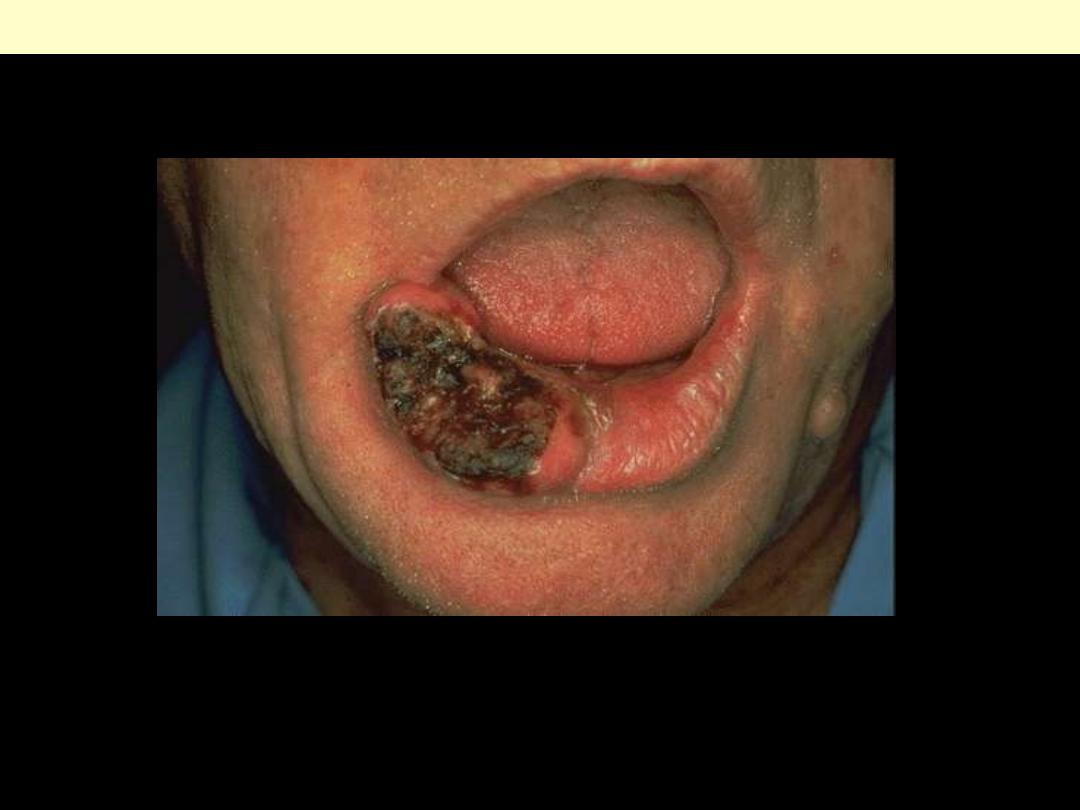
a pearly pink border and an ulcerated center.
Basal cell carcinoma lower lip
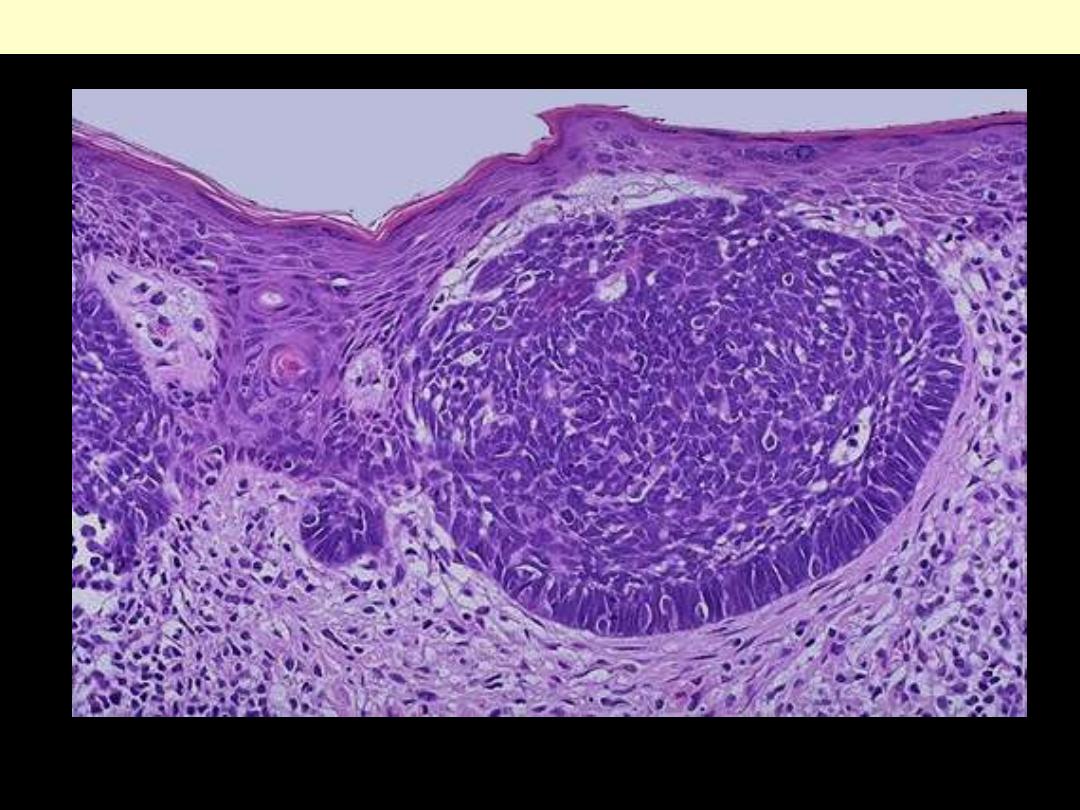
Nests of basaloid cells are dropping off into the upper dermis in this example of a basal cell carcinoma
of the skin.
Basal cell carcinoma solid