
Medicine
Dr. Ghyath
Neurology
“
Ataxia
”
Dr. Ghyath
LECTURE 17

Ataxia Dr. Ghyath
3
Ataxia
Ataxia: is a Greek word mean disorder
Symptoms and signs of ataxia consist of:
Gait impairment
Unclear ("scanning") speech
Visual blurring due to nystagmus
Hand incoordination
Tremor with movement.
These result from the involvement of the cerebellum and its afferent and
efferent pathways.
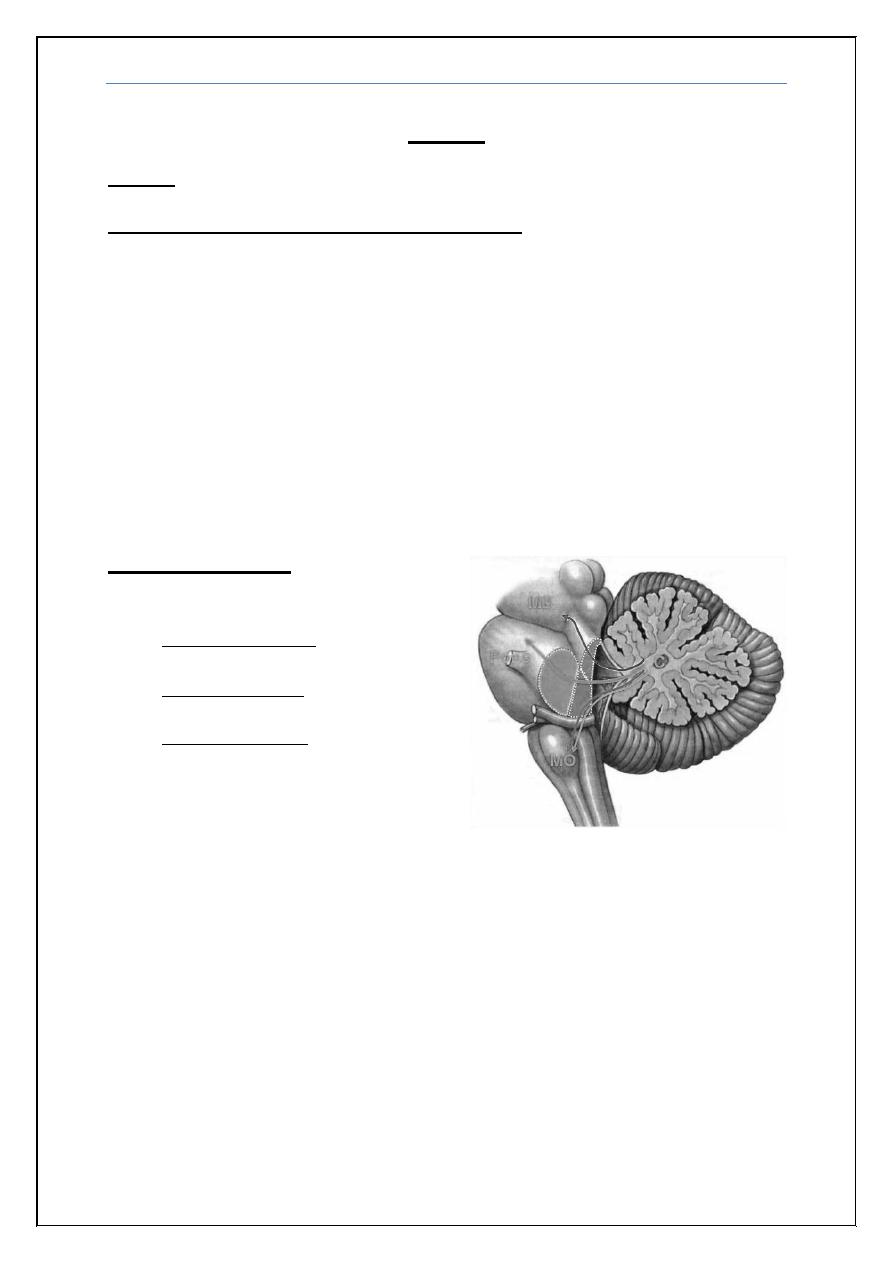
Cerebellar Ataxia
Cerebellar peduncles:
Superior peduncle connects
cerebellum with midbrain.
Middle peduncle connects
cerebellum with pons.
Inferior peduncle connects
cerebellum with medulla
oblongata.
True cerebellar ataxia must be distinguished from ataxia associated with
vestibular nerve or labyrinthine disease, as the latter results in a disorder
of gait associated with a significant degree of dizziness, light-headedness.
True cerebellar ataxia is devoid of these vertiginous (dizziness and light-
headedness) complaints and is clearly an unsteady gait due to imbalance.
Sensory disturbances can also on occasion simulate the imbalance of
cerebellar disease; with sensory ataxia (due to involvement of joint position),
imbalance dramatically worsens when visual input is removed (Romberg
sign).
Ataxia Dr. Ghyath
4
Ataxia is classified into:
Acute, sub acute and chronic
Hereditary and acquired
Acute (Hours to Days)
Vascular: cerebellar infarction, hemorrhage,
Intoxication: alcohol, lithium, phenytoin barbiturates
Acute cerebellitis eg: (varcilla, polio & caosaki) virus
Cerebellar abscess.
Post infection syndrome especially after varcilla
Subacute (Days to Weeks)
Intoxication: mercury, solvents, gasoline, glue; cytotoxic chemotherapy,
Degeneration of the cerebellar vermis: may be due to the combined
effects of alcoholism and malnutrition, particularly with deficiencies of
vitamins B1 and B12.
Tumour: cerebellar glioma or metastatic tumor
Demyelinating: multiple sclerosis
Chronic (Months to Years)
Paraneoplastic cerebellar ataxia is associated with a number of different
tumors (and autoantibodies) such as :
Breast and ovarian cancers (anti-Yo)
Small-cell lung cancer (anti-PQ type voltage-gated calcium
channel)
Inherited diseases
Amiodarone, phenytoin
Ataxia Dr. Ghyath
5
The Inherited Ataxias
These may show autosomal dominant, autosomal recessive or maternal
(mitochondrial) modes of inheritance:
1) Autosomal Dominant Ataxias
The autosomal dominant spinocerebellar ataxias (SCAs) include SCA types 1
through SCA 30.
2) Autosomal Recessive Ataxias
Friedreich's Ataxia
This is the most common form of inherited ataxia, comprising one-half of all
hereditary ataxias. It can occur in a classic form or in association with a
genetically determined vitamin E deficiency syndrome; the two forms are
clinically indistinguishable.
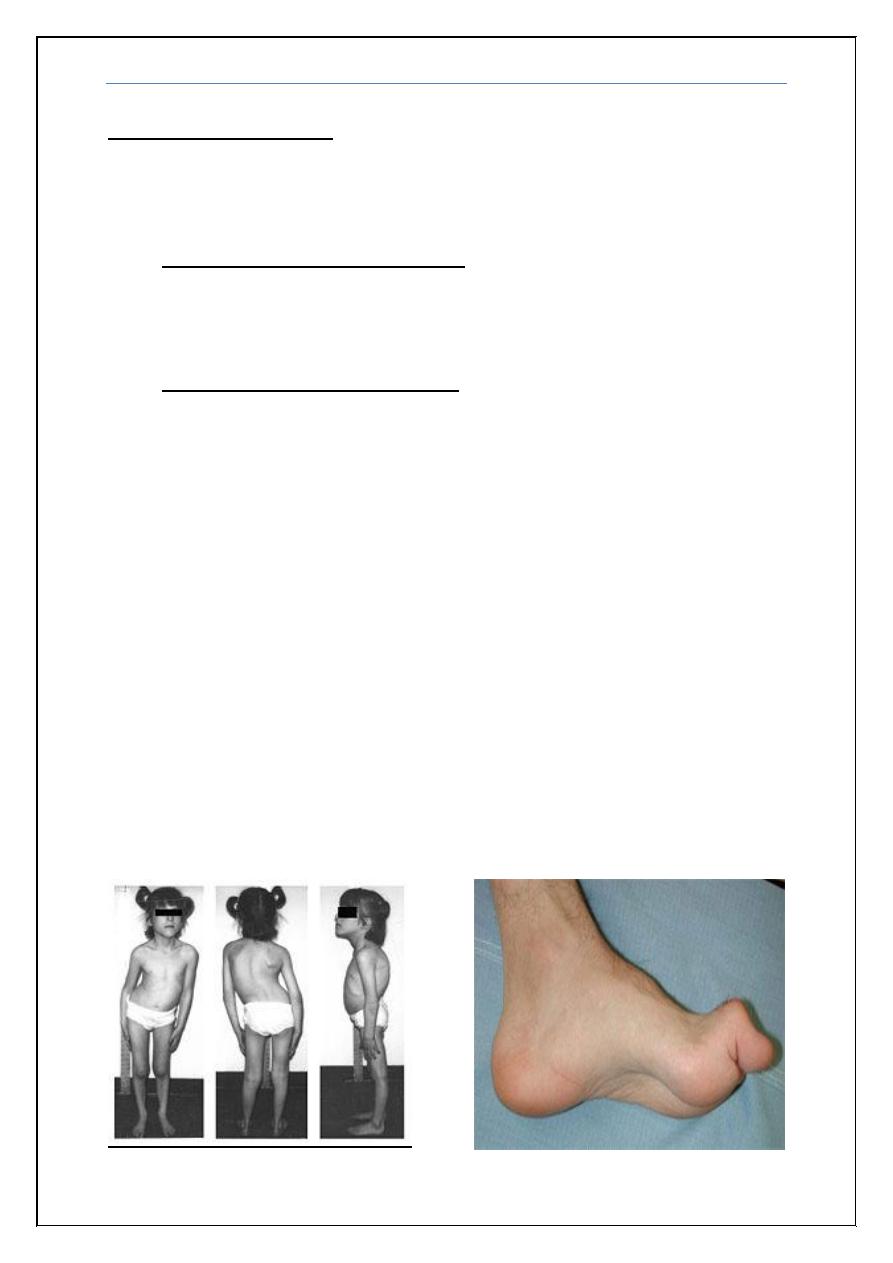
Symptoms and Signs
Friedreich's ataxia presents before 25 years of age with:
Progressive ataxia, the lower extremities are more severely involved than
the upper ones.
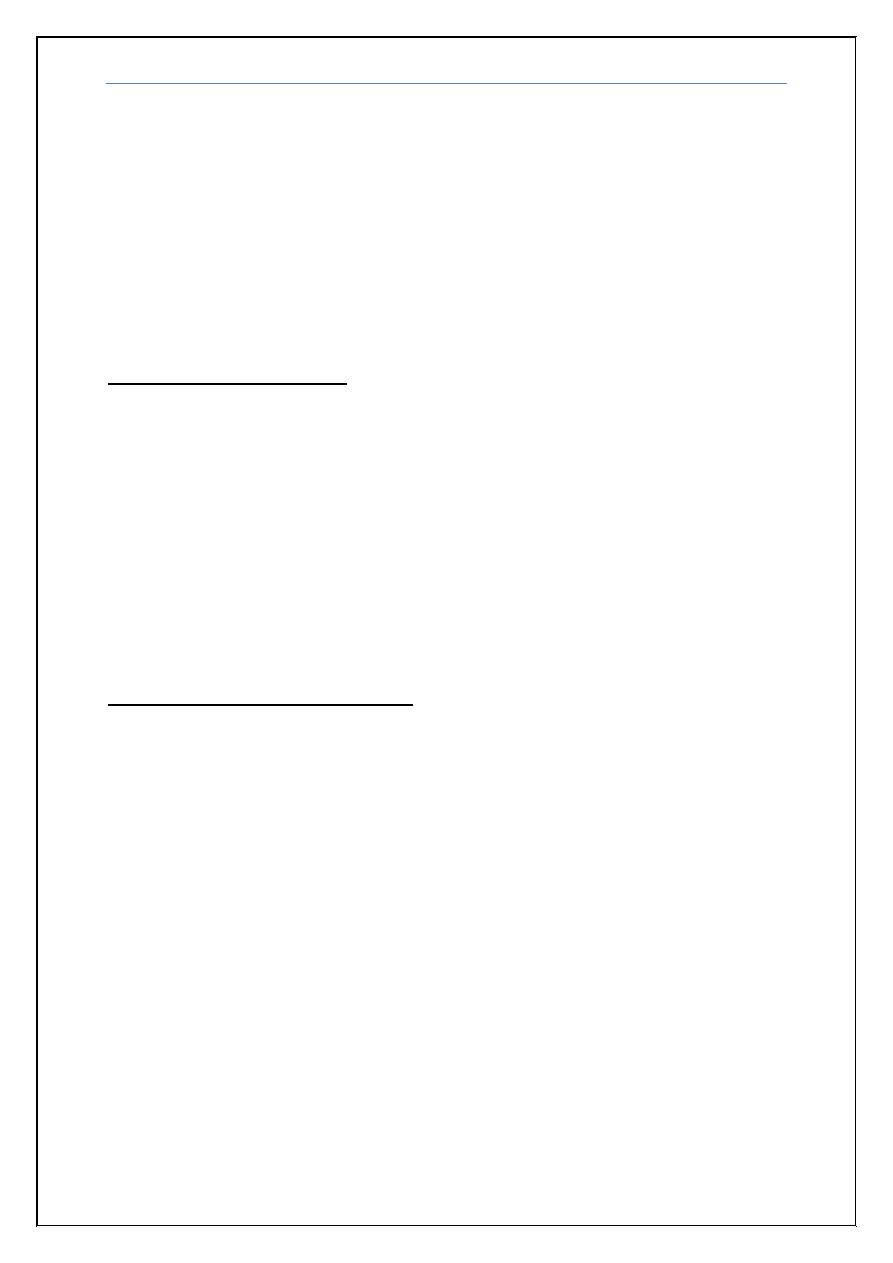
Musculoskeletal deformities: progressive scoliosis, foot deformity pes
cavus or pes equinovarus.
Extensor plantar responses, absence of deep tendon reflexes, and
weakness (greater distally than proximally) are usually found.
Loss of vibratory and proprioceptive sensation occurs.
Ataxia Dr. Ghyath
6
Cardiac involvement occurs in 90% of patients; cardiomegaly, symmetric
hypertrophy, murmurs, and conduction defects are reported.
Moderate mental retardation or psychiatric syndromes are present in a
small percentage of patients.
A high incidence of diabetes mellitus (20%) is found and is associated
with insulin resistance and pancreatic B-cell dysfunction.
The median age of death is 35 years. Women have a significantly better
prognosis than men, MRI of the spinal cord shows atrophy also slight
atrophy of the cerebellum may occur.
Investigation for ataxia
Blood Studies: CBP, alcohol level, anticonvulsant drug levels, vitamin E
levels and paraneoplastic antibody panel.
Neuroimaging: Brain imaging is useful for demonstrating posterior fossa
tumors or malformations, cerebellar infarction or hemorrhage, and
cerebellar atrophy associated with degenerative disorders and Brain (MRI)
provides better visualization of posterior fossa lesions, including tumors,
and is superior to CT scanning for detecting the lesions of multiple
sclerosis.
CSF: in case of infection e.g. Cerebellitis.
Genetic studies: in case of hereditary ataxia
Treatment of ataxic disorders
The most important goal in management of patients with ataxia is to identify
treatable disease entities. Mass lesions must be recognized promptly and
treated appropriately. Paraneoplastic disorders treated by removal the primary
cancer or by immunotherapy.
Malabsorption syndromes leading to vitamin E deficiency may lead to
ataxia. The vitamin E deficiency form of Friedreich's ataxia must be considered,
and serum vitamin E levels measured. Vitamin E therapy is indicated for these
rare patients. Vitamin B1 and B12 levels in serum should be measured, and the
vitamins administered to patients having deficient levels.
Ataxia Dr. Ghyath
7
Wernicke’s encephalopathy
Wernicke–Korsakoff syndrome:
The presentation of Wernicke’s encephalopathy (ophthalmoplegia, ataxia and
confusion) can progress to the irreversible deficits of Korsakoff’s syndrome
(severe short-term memory impairment) resulting from an acquired
nutritional deficiency of thiamine (vitamin B1). Thiamine (and other B
vitamins) is a co-enzyme in glucose and lipid metabolism, amino acid
production and neurotransmitter synthesis. Because thiamine stores are
relatively small and there is a large daily turnover, deficiency may occur within
2–3 weeks of low intake.
Causes
Alcohol
Hyperemesis of pregnancy
Systemic malignancy
Haemo- or peritoneal dialysis
Gastrointestinal surgery
Prolonged intravenous feeding
Anorexia
AIDS
Treatment
Is by thiamine given immediately commencing at 50–100 mg parenterally in the
acute stage may continue for several days
END