
Endocrine
Dr. Moneeb
“ Diabetes Mellitus ”
Total Lec: 42

Diabetes mellitus
The contents of this lecture:
1. Definition
2. Types
3. Aetiology
4. Pathology and pathophysiology
5. Clinical presentations
6. Diagnosis
7. Treatment
8. complications
Introduction and Classification
Diabetes mellitus (DM) is a common, chronic, metabolic syndrome characterized by
hyperglycemia as a cardinal biochemical feature.
DM is not a single entity but rather a heterogeneous group of disorders.
Three major forms of diabetes and several forms of carbohydrate intolerance are
identified.
Aetiologic Classifications of Diabetes Mellitus
Type I diabetes
(
β-cell destruction, usually leading to absolute insulin deficiency)
Immune mediated, Idiopathic
Type 2 diabetes
(may range from predominantly insulin resistance with relative
insulin deficiency to a predominantly secretory defect with insulin resistance)
Dominant, type 2 due to sulfonylurea receptor 1 mutation.
Other specific types
•
Genetic defects of
β-
cell function
Chromosome 20, HNF-4α (MODY1)
Chromosome 7, glucokinase (MODY2)
Chromosome 12, HNF-1α (MODY3)
Insulin promotor factor–1 (MODY4)
HNF-1β (MODY5)
NEUROD1 (MODY6)
•
Genetic defects in insulin action
Type A insulin resistance, Lipoatrophic diabetes
•
Diseases of the exocrine pancreas
Pancreatitis, Trauma, pancreatectomy, Neoplasia, Cystic fibrosis , Hemochromatosis
•
Endocrinopathies
Acromegaly, Cushing disease, Pheochromocytoma, Hyperthyroidism
•
Drug-or chemical-induced
Pentamidine, Nicotinic acid, Glucocorticoids, Thyroid hormone, Diazoxide, β-
Adrenergic agonists, Thiazides, β-Interferon, cyclosporine
•
Infections
Congenital rubella, Cytomegalovirus
•
Other genetic syndromes sometimes associated with diabetes
Down syndrome, Klinefelter syndrome, Turner syndrome, Wolfram syndrome
, Friedreich ataxia Huntington chorea, Laurence-Moon-Biedl syndrome,, and Prader-
Willi syndrome
•
Gestational diabetes mellitus
•
Neonatal diabetes mellitus
Transient—without recurrence
Transient—recurrence 7–20 yr later
Permanent from onset
TYPE 1 DIABETES MELLITUS
(Immune Mediated)
Previously called insulin-dependent diabetes mellitus (IDDM) or juvenile diabetes.
T1DM is the most common endocrine-metabolic disorder of childhood and
adolescence, with important consequences for physical and emotional development
T1DM is characterized by low or absent levels of endogenously produced insulin and
dependence on exogenous insulin to prevent development of ketoacidosis, an acute
life-threatening complication of T1DM.
The natural history includes 4 distinct stages:
(1) Preclinical β-cell autoimmunity with progressive defect of insulin secretion,
(2) Onset of clinical diabetes,
(3) Transient remission “honeymoon period,”
(4) Established diabetes associated with acute and chronic complications and
decreased life expectancy.
EPIDEMIOLOGY:
The incidence of T1DM is rapidly increasing in specific regions and shows a trend
toward earlier age of onset.
sex & socioeconomic status
Girls and boys are almost equally affected; there is no apparent correlation with
socioeconomic status.
Age at onset:
Peaks of presentation occur in 2 age groups:
The 1st peak (at 5–7 years of age) may correspond to the time of increased exposure
to infectious agents coincident with the beginning of school;
the 2nd peak (at the time of puberty) may correspond to the pubertal growth spurt
induced by gonadal steroids and the increased pubertal growth hormone secretion
(which antagonize insulin).
A growing number of cases are presenting between 1 and 2 years of age.
Genetic basis:
The genetics of T1DM cannot be classified according to a specific model of
inheritance.
Inheritance of HLA-DR3 or -DR4 antigens appears to confer a 2- to 3-fold increased
risk for the development of T1DM.
When both DR3 and DR4 are inherited, the relative risk for the development of
diabetes is increased by 7- to 10-fold.
Inheritance of HLA-DR2 appear to be protective against diabetes.
The concordance rate among identical twins is only 30–50%, suggesting either the
participation of environmental triggering factors or other genetic factors
The risk to offspring of a diabetic parent is 2–5%, with the higher risk occurring in the
offspring of a diabetic father.
Environmental basis:
No dominant environmental agent responsible for triggering T1DM Environmental
risk determinants can be classified as : Viral infections: coxsackie B3, coxsackie B4,
cytomegalovirus, rubella, and mumps can infect human β cells.
Only congenital rubella infection is associated with diabetes in later life (10–12%)
Seasonal association:
Seasonal variations occur in the incidence of T1DM with greater frequency in autumn
and winter months
Puberty:
pubertal changes may contribute to accelerated onset of T1DM. The pubertal peak in
onset of type 1 DM occurs earlier in girls than boys.
Dietary factors:
Dietary factors have been implicated in the pathogenesis of T1DM, but the role of
dietary factors in induction of islet autoimmunity remains controversial.
cow's milk & initial exposure of infants to cereals before 4 months of age has been
suggested to increase the risk of islet cell autoimmunity
Body mas index:
There may be a greater risk of T1DM among individuals who were heavier as young
children.
Insulin resistance is a function of fat mass, Therefore, limiting excessive weight gain
may be as important for children susceptible to T1DM as for those at genetic risk for
T2DM.
Chemicals & drugs:
Drugs such as alloxan, streptozotocin (STZ), and pentamidine are directly cytotoxic to
β cells and cause diabetes in experimental animals and humans.
Psychosocial stress
may constitute a trigger mechanism for T1DM or the autoimmune process behind
the disease.(uncover latent cases of DM)
PATHOGENESIS
Autoimmune Injury:
•
T1DM is a chronic, T cell–mediated autoimmune disease that results in the
destruction of the pancreatic islets.
•
Genetic predisposition and environmental factors lead to initiation of an
autoimmune process against the pancreatic islets which leads to a gradual and
progressive destruction of β cells, with loss of insulin secretion.
* at the onset of clinical diabetes, 80–90% of the pancreatic islets are destroyed.
Regeneration of new islets has been detected at onset of T1DM, and it is thought to
be responsible for the honeymoon phase (a transient decrease in insulin requirement
associated with improved β-cell function).
* In young diabetic children, especially those of DR3/DR4 haplotypes, the
destruction of β cells is almost complete during the 1st 3 yr after the onset of
hyperglycemia, whereas in older patients complete β-cell destruction may take up to
10 yr.
*most individuals progressing to overt diabetes express multiple anti–islet cell
antibodies (GAD65, ICA512/IA-2, and IAA) before the onset of diabetes.
PATHOPHYSIOLOGY
In normal metabolism, there are regular swings between the postprandial, high-
insulin anabolic state and the fasted, low-insulin catabolic state that affect liver,
muscle, and adipose tissue .
T1DM is a progressive low-insulin catabolic state in which feeding does not reverse
but rather exaggerates these catabolic processes.
With moderate insulinopenia, glucose utilization by muscle and fat decreases and
postprandial hyperglycemia appears.
At even lower insulin levels, the liver produces excessive glucose via glycogenolysis
and gluconeogenesis, and fasting hyperglycemia begins.
Hyperglycemia produces an osmotic diuresis (glycosuria) when the renal threshold is
exceeded (180 mg/dL;= 10 mmol/L).
The resulting loss of calories and electrolytes, as well as the persistent dehydration,
produce a physiologic stress with hypersecretion of stress hormones (epinephrine,
cortisol, growth hormone, and glucagon).
These hormones, in turn, contribute to the metabolic decompensation:
• by further impairing insulin secretion (epinephrine),
• by antagonizing insulin action (epinephrine, cortisol, GH),
• by promoting glycogenolysis, gluconeogenesis, lipolysis, and ketogenesis
(glucagon, epinephrine, growth hormone, and cortisol)
• by decreasing glucose utilization and glucose clearance (epinephrine, growth
hormone, cortisol).
The combination of insulin deficiency and elevated plasma values of the counter-
regulatory hormones is also responsible for accelerated lipolysis and impaired lipid
synthesis, with resulting increased plasma concentrations of total lipids, cholesterol,
triglycerides, and free fatty acids.
The hormonal interplay of insulin deficiency and glucagon excess shunts the free
fatty acids into ketone body formation; the rate of formation of these ketone bodies,
principally β-hydroxybutyrate and acetoacetate, exceeds the capacity for peripheral
utilization and renal excretion.
Accumulation of these keto acids results in metabolic acidosis (diabetic ketoacidosis,
DKA) and compensatory rapid deep breathing in an attempt to excrete excess CO2
(Kussmaul respiration).
Acetone, formed by nonenzymatic conversion of acetoacetate, is responsible for the
characteristic fruity odor of the breath.
Ketones are excreted in the urine in association with cations and thus further
increase losses of water and electrolyte.
With progressive dehydration, acidosis, hyperosmolality, and diminished cerebral
oxygen utilization, consciousness becomes impaired, and the patient ultimately
becomes comatose.
↓ insulin → ↑ s. glucose → glucosuria → polyuria → thirst → dehydration
↓
↓ IC glucose
↓
↑ adrenaline, noradrenaline
GH , cortisol , glucagon
↓
↑ lipolysis → wt loss
↓
↑ ketone bodies → ketoacidosis → kussmaul respiration
↓ ↓
Ketonuria coma
Clinical presentations:
1. Classical presentation: (60-80%)
polyuria, polydipsia, polyphagia and Wt. loss.
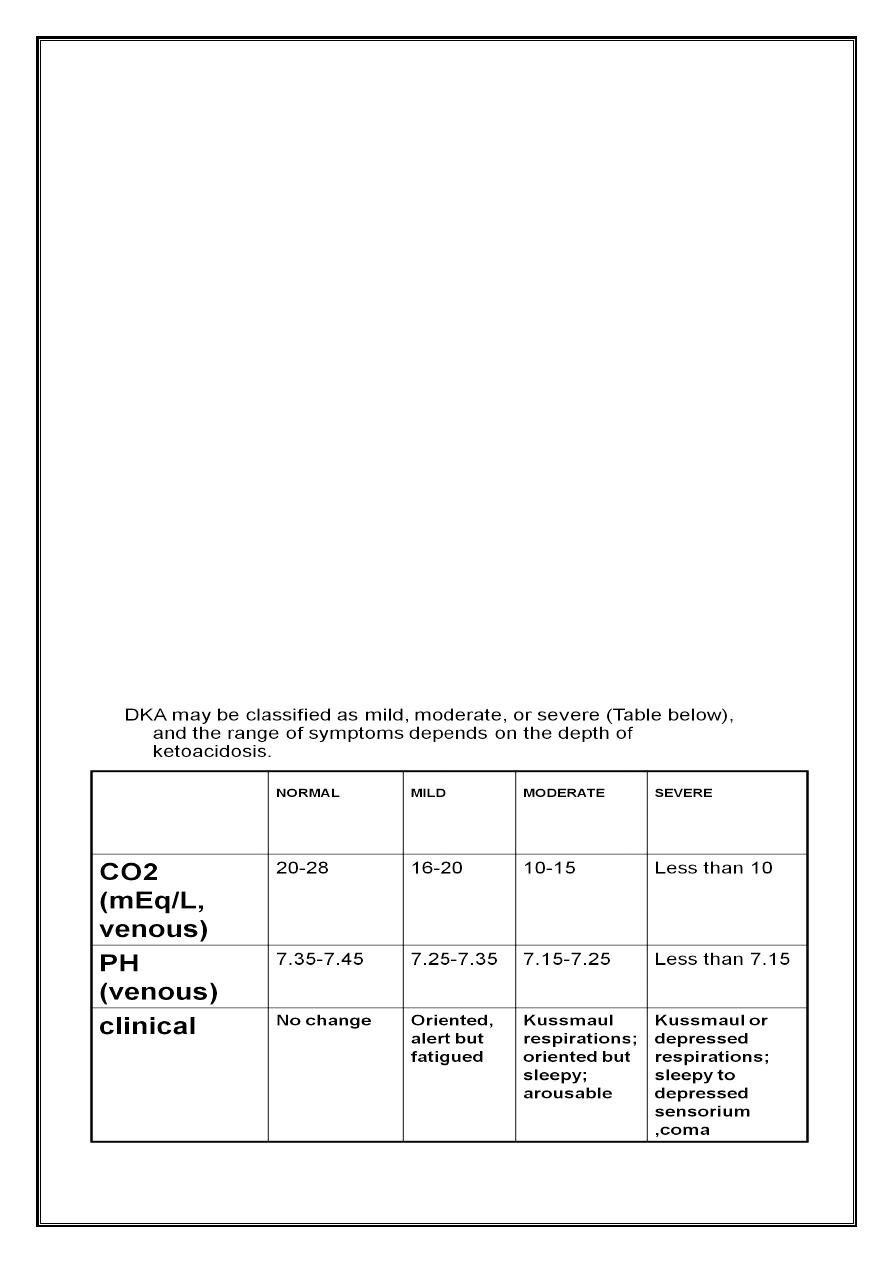
2. Diabetic ketoacidosis (DKA): (20–40%)
abdominal discomfort, nausea, vomiting, sever dehydration with persistent polyuria
(the degree of dehydration may be clinically underestimated because intravascular
volume is conserved at the expense of intracellular volume).
Ketoacidosis exacerbates prior symptoms & leads to Kussmaul respirations (deep,
heavy, rapid breathing), fruity breath odor (acetone), diminished neurocognitive
function, and possible coma.
Others : candidal vaginitis, secondary enuresis.
This entire progression happens much more quickly (over a few weeks) in younger
children.
In infants, most of the weight loss is acute water loss and there will be an increased
incidence of DKA at diagnosis.
In adolescents, the course is usually more prolonged (over months), and most of the
weight loss represents fat loss due to prolonged starvation. Additional weight loss
due to acute dehydration may occur just before diagnosis.
In any child, the progression of symptoms may be accelerated by the stress of an
intercurrent illness or trauma, when counter-regulatory (stress) hormones secretion
increased.
DIAGNOSIS
The diagnosis of T1DM is usually easy.
Although most symptoms are nonspecific, the most important clue is an
inappropriate polyuria in any child with dehydration.
Hyperglycemia, glycosuria, and ketonuria can be determined quickly.
In the obese child, T2DM must be considered.
DIABETES MELLITUS (DM)
Symptoms of DM plus Fasting plasma glucose ≥126 mg/dL (7.0 mmol/L)
or
Symptoms of DM plus random plasma glucose ≥200 mg/dL (11.1 mmol/L)
Or
2-hr plasma glucose during the OGTT ≥200 mg/dL
IMPAIRED GLUCOSE TOLERANCE (IGT)
Fasting glucose: 110–125 mg/dL (6.1–7.0 mmol/L)
2-hr plasma glucose during the OGTT: ≥ 140 mg/dL<200 mg/dL (11.1 mmol/L)
Once hyperglycemia is confirmed, it is important to determine whether DKA is
present (presence of ketonuria, an increased ion gap, a decreased serum bicarbonate
(or total CO2) and pH, and an elevated effective serum osmolality, indicating
hypertonic dehydration. and to evaluate electrolyte abnormalities—even if signs of
dehydration are minimal.
A baseline hemoglobin A1C (HbA1c) allows an estimate of the duration of
hyperglycemia and provides an initial value by which to compare the effectiveness of
subsequent therapy.
In the obese child, testing for autoimmunity to β cells is necessary ( because the
possibility of T2DM) but it is not necessary in thin diabetic patients.
Other autoimmunities associated with type 1 diabetes should be checked for
including: celiac disease (by tissue transglutaminase IgA and total IgA) thyroiditis (by
antithyroid peroxidase and antithyroglobulin antibodies).
Because significant physiologic distress can disrupt the pituitary-thyroid axis, free
thyroxine (T4) and TSH levels should be checked after the child is stable for a few
weeks.
TREATMENT
Therapy depends on the degree of insulinopenia at presentation.
Most children with new diabetes (60–80%) have mild to moderate symptoms, have
minimal dehydration with no history of emesis, and have not progressed to
ketoacidosis. ( ie: classical presentation or non ketotic onset)
Once DKA has resolved in the newly diagnosed child, therapy is transitioned to that
described for children with non ketotic onset.
Children with previously diagnosed diabetes who develop DKA are usually
transitioned to their previous insulin regimen.
New-Onset Diabetes Without Ketoacidosis.
Excellent diabetes control involves many goals:
1.to maintain a balance between tight glucose control and avoiding hypoglycemia,
2.to eliminate polyuria and nocturia,
3.to prevent ketoacidosis,
4.to permit normal growth and development with minimal effect on lifestyle.
Insulin Therapy
Children with long-standing diabetes and no insulin reserve require about:
0.7 U/kg/d if pre pubertal,
1.0 U/kg/d at mid puberty,
1.2 U/kg/d by the end of puberty.
A reasonable dose in the newly diagnosed child, then, is about 60–70% of the full
replacement dose based on pubertal status.
The optimal insulin dose can only be determined empirically, with frequent self-
monitored blood glucose levels and insulin adjustment by the diabetes team.
Residual β-cell function usually fades within a few months and is reflected as a
steady increase in insulin requirements.
Types of insulin and their regimens used are:
Actrapid (soluble) , monotard (lente), & mixtard.
1. Two doses regimen ( actrapid 1/3 and monotard 2/3) or mixtard only with 2/3
of the daily dose in the morning and 1/3 in the evening,
( sometimes we personalize the dose and the % of the combination).
However, such a schedule would provide poor coverage for lunch and early morning,
and would increase the risk of hypoglycemia at midmorning and early night.
2. Basal bolus regimen
insulin analogs (Lispro (L) and aspart) which are absorbed much quicker because
they do not form hexamers. their action started within 10 minutes with duration of
action of 2 hours without peak.
The long-acting analog glargine (G) creates a much flatter 24-hr profile, making it
easier to predict the combined effect of a rapid bolus (L or A) on top of the basal
insulin, producing a more physiologic pattern of insulin effect.
The basal insulin glargine should be 25–30% of the total dose in toddlers and 40–50%
in older children.
The remaining portion of the total daily dose is divided evenly as bolus injections for
the 3 meals .
Postprandial glucose elevations are better controlled, and between-meal and night
time hypoglycemia are reduced.
Frequent blood glucose monitoring and insulin adjustment are necessary in the 1st
weeks as the child returns to routine activities and adapts to a new nutritional
schedule, and as the total daily insulin requirements are determined.
Insulin Pump Therapy
Inhaled Insulin
Pre prandial inhaled insulin is being evaluated in adults with T1DM and T2DM.
Pre-meal oral insulin (Oralin) has been evaluated in comparison with oral
hypoglycemic agents, mostly in patients with T2DM. The clinical data appear
promising, but further evaluation of efficacy in T1DM is needed
Ketoacidosis
Reversal of DKA is associated with inherent risks that include hypoglycemia,
hypokalemia, and cerebral edema.
Any protocol must be used with caution and close monitoring of the patient
Hyperglycemia and Dehydration:
Insulin (0.1 unit/ kg/ hour) IV or IM must be given at the beginning of therapy to
accelerate movement of glucose into cells, to stop hepatic glucose production, and to
halt the movement of fatty acids from the periphery to the liver.
Rehydration also lowers glucose levels by improving renal perfusion and enhancing
renal excretion.
The combination of these therapies usually causes a rapid initial decline in serum
glucose levels.
Once glucose goes below 180 mg/dL (10 mmol/L), the osmotic diuresis stops and
rehydration accelerates without further increase in the infusion rate.
Repair of hyperglycemia occurs well before correction of acidosis. Therefore, insulin
is still needed to control fatty acid release after normal glucose levels are reached.
To continue the insulin infusion without causing hypoglycemia, glucose must be
added to the infusion, usually as 5% or 1/5 GS solution.
Glucose should be added when the serum glucose has decreased to about 250
mg/dL (14 mmol/L) so that there is sufficient time to adjust the infusion before the
serum glucose falls further.
The insulin infusion can also be lowered from the initial maximal rate once
hyperglycemia has resolved.
During repair of fluid deficits we must take in consideration the potential risk of
cerebral edema. All fluid intake and output should be closely monitored.
*Limited ice chips may be given as a minimal oral intake.
*Although patients with DKA have a total body potassium deficit, the initial serum
level is often normal or elevated.
This is due to the movement of potassium from the intracellular space to the
serum, both as part of the ketoacid buffering process and as part of the catabolic
shift.
*Mildly elevated creatinine or BUN is not a reason to withhold potassium therapy if
good urinary output is present.
Keto Acid Accumulation:
Low insulin infusion rates (0.02–0.05 units/kg/h) are usually sufficient to stop
peripheral release of fatty acids, thereby eliminate the production of ketone bodies
Bicarbonate buffers, regenerated by the distal renal tubule and by metabolism of
ketone bodies, and their excretion in the urine steadily repair the acidosis once
ketoacid production is controlled.
Bicarbonate therapy is rarely necessary and may even increase the risk of
hypokalemia and cerebral edema.
(only indicated in case of sever acidosis , ie :when the blood PH < 7.1)
Persistent acidosis may indicate inadequate insulin or fluid therapy, infection, or
rarely lactic acidosis.
Urine ketones may be positive long after ketoacidosis has resolved , Therefore,
persistent ketonuria may not accurately reflect the degree of clinical improvement
and should not be relied upon as an indicator of therapeutic failure.
Cerebral edema:
For all but the mildest cases, frequent neurologic checks for any signs of increasing
intracranial pressure, such as a change of consciousness, depressed respiration,
worsening headache, bradycardia, apnea, pupillary changes, papilledema, posturing,
and seizures.
Mannitol 10% (10gm /100ml) must be readily available for use at the earliest sign of
cerebral edema.
All patients with DKA should be checked for initiating events in order to avoid them
to prevent the recurrence of DKA.
Management of DKA
1. Admission to the emergency unit.
2. ABC if the patient is comatosed and O2 to be delivered via mask.
3. IV LINE and Aspiration of blood for RBS, B.urea, S.Cr, S.K, S.Na, S.Cl, CBP, B.C/S
,ASTRUP
4. Urine for ketone, sugar, pus cell.
5. Calculation of the deficit and maintenance of the fluids ; to be replaced over
36- 48 hours (hyperosmotic dehydration)
Oral fluid is stopped and only sucking of chips of ice is allowed .
IV fluid (0.9%N/S or RL bolus 10 - 20ml / kg /1
st
hour) and then rate of fluid
replacement from the 2
nd
hour till resolution of DKA calculated according to the
following formula :
( 85× Bwt + maintenance – bolus / 23 hours= rate / hour ).
Change the type of the fluid from N/S to G/S (1/2, 1/3,1/5) when RBS is less than 250
mg/dl . WHY?
6 KCl: the patient is hypokalemic even if S.K was normal .WHY?
20 - 40 meq/L (1 ml = 2 meq) and sometimes increased to 60 meq/L .
7. INSULIN : either IV continuous infusion via a separate IV line started at time
zero OR interrupted IM or IV dose started after one hour (the dose in both ways is
0.1 unit /kg/h)
Changed to SC insulin and start oral fluid when there are no emesis, or acidosis
with normal electrolytes. HOW ?
8. Sod. Bicarbonate : only used in sever acidosis (PH less than 7.1) in a dose of 20-
40 meq ( 1 ml = 1 meq) with the fluid. WHY?
9. Mannitol :10% if signs of cerebral oedema appear in a dose of 1 gm / kg IV
infusion.
10. Antibiotic : if infection is present.
11. checking for the initiating events should be done and treated & avoid to be
repeated
*NB: put 50 unit of soluble (actrapid) insulin in one pint (500 cc) NS = 0.1 u/cc & use
EVAC to control the rate of infusion OR
use micro-drip (burette) & put 10 unit of soluble insulin for every 100 cc NS.
In either ways you must flush 1cc/ Kg rapidly to saturate the insulin receptors & then
the rate will be:
1CC /Kg /hour = 60 micro drops /kg /hr
= one micro drop /kg/min.
The rate should be reduced to 1/2 if RBS is below 150 mg/dl
NEVER FORGET THE FLOW SHEET FOR DIABETIC KETOACIDOSIS
(name, age, date, time, BWt & SA, PR, BP,PH, RBS , S.electrolyte, Fluid input, output,
insulin dose, signs of cerebral oedema, and notes).
Basic Education
Therapy consists not only of initiation and adjustment of insulin dose but also of
education of the patient and family.
In the acute phase, the family must learn the “basics,” which includes:
*monitoring the child's blood glucose and urine ketones,
*preparing and injecting the correct insulin dose subcutaneously at the proper time,
*recognizing and treating low blood glucose reactions, and
*having a basic meal plan.
Most families are trying to adjust psychologically to the new diagnosis of diabetes in
their child and thus have a limited ability to retain new information.
Written materials covering these basic topics help the family during the 1st few days.
Nutritional Management
Nutrition plays an essential role in the management of patients with T1DM. This is of
critical importance during childhood and adolescence, when appropriate dietary
intake is required to meet the needs for energy, growth, and pubertal development.
The caloric mixture should comprise approximately 55% carbohydrate, 30% fat, and
15% protein.
Approximately 70% of the carbohydrate content should be derived from complex
carbohydrates such as starch; intake of sucrose and highly refined sugars should be
limited.
Carbohydrate counting has become a mainstay in the nutrition education and
management of patients with DM.
Each carbohydrate exchange unit is 15 g.
Patients and their families are provided with information regarding the carbohydrate
contents of different foods and food label reading.
The total daily caloric intake is divided to provide 20% at breakfast, 20% at lunch, and
30% at dinner, leaving 10% for each of the midmorning, midafternoon, and evening
snacks, if they are desired.
Emphasis should be placed on regularity of food intake and on constancy of
carbohydrate intake.
Monitoring
Success in the daily management of the diabetic child can be measured by the ability
of the family, and subsequently the child, in assuming responsibility for daily
“diabetic care.”
Monitoring often include : insulin dose, unusual physical activity, dietary changes,
hypoglycemia, intercurrent illness, and other items that may influence the blood
glucose.
Self-monitoring of blood glucose (SMBG) is an essential component of managing
diabetes. Accu check devices to measure the B. glucose within one minute.
Parents and patients should be taught to use these devices and measure blood
glucose at least 4 times daily—before breakfast, lunch, and supper and at bedtime,
and records the results and other notes in special notebook to be reviewed with
doctor during follow up visit.
Ideally, the blood glucose concentration should range from approximately 80 mg/dL
in the fasting state to 140 mg/dL after meals.
A reliable index of long-term glycemic control is provided by measurement of
glycosylated hemoglobin.
HbA1C represents the fraction of hemoglobin to which glucose has been non
enzymatically attached in the bloodstream.
HbA1C measurement reflects the average blood glucose concentration from the
preceding 2–3 mo.
It is recommended that HbA1C measurements be obtained 3 to 4 times per year to
obtain a profile of long-term glycemic control. the HbA1C fraction:
in nondiabetic individuals, is usually less than 6%.
in diabetics:
•
values of 6–7.9% represent good metabolic control,
•
values of 8.0–9.9%, fair control,
•
values of 10.0% or higher, poor control.
Exercise:
•
No form of exercise, including competitive sports, should be forbidden to the
diabetic child. A major complication of exercise in diabetic patients is the
presence of a hypoglycemic reaction during or within hours after exercise.
•
glucoregulation is likely to be improved through the increased utilization of
glucose by muscles.
•
The major contributing factor to hypoglycemia with exercise is an increased
rate of absorption of insulin from its injection site.
•
Regular exercise also improves glucoregulation by increasing insulin receptor
number.
•
In patients who are in poor metabolic control, vigorous exercise may
precipitate ketoacidosis because of the exercise-induced increase in the
counter-regulatory hormones.
•
In anticipation of vigorous exercise, one additional carbohydrate exchange may
be taken before exercise, or the total dose of insulin may be reduced by about
10–15% on the day of the scheduled exercise.
•
It is also important to watch for delayed hypoglycemia several hours after
exercise.
Management During Infections
Although infections are no more common in diabetic children than in nondiabetic
ones, they can often disrupt glucose control and may precipitate DKA.
In addition, the diabetic child is at increased risk of dehydration if hyperglycemia
causes an osmotic diuresis or if ketosis causes emesis.
Counter-regulatory hormones associated with stress blunt insulin action and elevate
glucose levels.
If anorexia occurs, however, lack of caloric intake increases the risk of hypoglycemia.
Although children younger than 3 year tend to become hypoglycemic and older
children tend toward hyperglycemia, the overall effect is unpredictable.
Therefore, frequent blood glucose monitoring and adjustment of insulin doses are
essential elements of sick day guidelines.
One regimen is to add 10 -20% of the total dialy dose as actrapid before each meal in
addition to the usual daily dose if hyperglycemia developed ( two doses daily
regimen).
The overall goals are to maintain hydration, control glucose levels, and avoid
ketoacidosis.
complications of the management:
*Hypoglycemic Reactions:
Hypoglycemia is the major limitation to tight control of glucose levels.
Most children with T1DM can expect mild hypoglycemia each week, moderate
hypoglycemia a few times each year, and severe hypoglycemia every few years.
These episodes are usually not predictable, although exercise, delayed meals or
snacks, wrong dose and wide swings in glucose levels increase the risk.
Hypoglycemia can occur at any time of day or night.
Early symptoms and signs (mild hypoglycemia) may occur with a sudden decrease in
blood glucose to levels that do not meet standard criteria for hypoglycemia in non
diabetic children.
The child may show pallor, sweating, apprehension , hunger, tremor, and
tachycardia, all due to the surge in catecholamines as the body attempts to counter
the excessive insulin effect.
Behavioral changes such as tearfulness, irritability, and aggression are more
prevalent in children.
As glucose levels decline further, cerebral glucopenia occurs with drowsiness,
personality changes, mental confusion, and impaired judgment (moderate
hypoglycemia),progressing to inability to seek help and seizures or coma (severe
hypoglycemia).
Prolonged severe hypoglycemia can result in a depressed sensorium or stroke-like
focal motor deficits that persist after the hypoglycemia has resolved.
Although permanent squeale are rare, severe hypoglycemia is frightening for the
child and family and can result in significant reluctance to attempt even moderate
glycemic control afterward.
Important counter-regulatory hormones in children include growth hormone,
cortisol, epinephrine, and glucagon. The latter two seem more critical in the older
child.
Many older patients with long-standing T1DM lose their ability to secrete glucagon in
response to hypoglycemia.
In the young adult, epinephrine deficiency may also develop as part of a general
autonomic neuropathy
This substantially increases the risk of hypoglycemia because the early warning
signals of a declining glucose level are due to catecholamine release.
Recurrent hypoglycemic episodes associated with tight metabolic control may
aggravate partial counter-regulatory deficiencies, producing a syndrome of
hypoglycemia unawareness and reduced ability to restore euglycemia (hypoglycemia-
associated autonomic failure).
Avoidance of hypoglycemia allows some recovery from this unawareness syndrome.
The most important factors in the management of hypoglycemia are:
*an understanding by the patient and family of the symptoms and signs of the
reaction and an anticipation of known precipitating factors such as sports activities.
Tighter glucose control increases the risk.
*A source of emergency glucose should be available at all times and places, including
at school and during visits to friends.
*If possible, it is initially important to document the hypoglycemia before treating,
because some symptoms may not always be due to hypoglycemia.
*Any child suspected of having a moderate to severe hypoglycemic episode should
be treated before testing.
*It is important not to give too much glucose;
5–10 g should be given as juice or a sugar-containing carbonated beverage or candy
and the blood glucose checked 15–20 minutes later.
*Patients, parents, and teachers should also be instructed in the administration of
glucagon when the child cannot take glucose orally.
An injection kit should be kept at home and school.
The intramuscular dose is 0.5 mg if the child weighs less than 20 kg and 1.0 mg if
more than 20 kg.
This produces a brief release of glucose from the liver.
Parents must then be prepared to take the child to the hospital for IV glucose
administration, if necessary.
*Somogyi Phenomenon, Dawn Phenomenon, and Brittle Diabetes:
blood glucose levels increase in the early morning hours before breakfast.
The dawn phenomenon is thought to be due mainly to overnight growth hormone
secretion and increased insulin clearance.
It is a normal physiologic process seen in most non diabetic adolescents, who
compensate with more insulin output.
A child with T1DM cannot compensate so we need to increase the evening lente
insulin.
the Somogyi phenomenon, a theoretical rebound from late night or early morning
hypoglycemia, thought to be due to an exaggerated counter-regulatory response.
so we need to decrease the evening insulin dose.
Continuous glucose monitoring systems may help clarify the cause of the elevated
morning glucose levels.
The term brittle diabetes has been used to describe the child, usually an adolescent
female, with unexplained wide fluctuations in blood glucose, often with recurrent
DKA, who is taking large doses of insulin (no physiological abnormality but usually
psychological cause)
*NONADHERENCE:
Family conflict, denial, and feelings of anxiety find expression in non adherence to
instructions regarding nutritional and insulin therapy and in noncompliance with self-
monitoring
*FEAR OF SELF-INJECTING AND SELF-TESTING:
Extreme fear of self-injecting insulin (injection phobia) is likely to compromise
glycemic control as well as emotional well-being.
Children and adolescents may either omit insulin dosing or refuse to rotate their
injection sites because repeated injection in the same site is associated with less pain
sensation.
Failure to rotate injection sites results in subcutaneous scar formation
(lipohypertrophy).
Insulin injection into the lipohypertrophic skin is usually associated with poor insulin
absorption and/or insulin leakage with resultant suboptimal glycemic control.
LONG-TERM COMPLICATIONS:
The increasingly prolonged survival of the diabetic child is associated with an
increasing prevalence of complications.
Limited joint mobility (LJM) (prayer sign) : highly correlated with micro vascular
complication of DM and can be used as rapid screening test in outpatient clinic.
Complications of DM can be divided into 3 major categories—
(1) microvascular complications, specifically, retinopathy and nephropathy;
(2) macrovascular complications, particularly accelerated coronary artery disease,
cerebrovascular disease, and peripheral vascular disease;
(3) neuropathies, both peripheral and autonomic, affecting a variety of organs and
systems.
In addition, cataract may occur more frequently.
PREDICTION AND PREVENTION
There is currently no known agent capable of preventing T1DM.
There are several obstacles to finding prevention strategy. These include
(1) ethical issues surrounding prediction,
(2) treatment dilemma,
(3) selection of populations at risk and treatment strategies, and
(4) finding new preventive agents.