For second grade
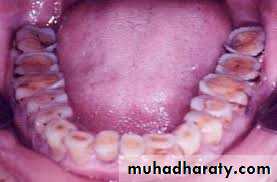
Caries of the Exposed RootCaries of the exposed root has shown increased prevalence over the past few years, particularly among the elderly.
Development of root caries relies on the expo-
sure of root areas, mostly due to gingival recession, andthe accumulation of plaque.

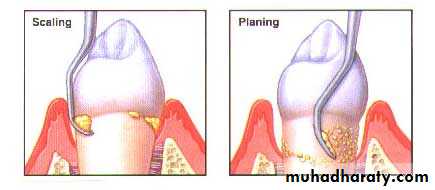
The cementum layer may cover the outer surface of the
exposed root. This layer can be removed with time byTooth brushing or dental therapeutic removal of tartar,
polishing, or periodontal treatment (scaling and root
planing).


It is known that dentin is more vulnerable to
demineralization than enamel, and the same applies tothe cementum layer . In most cases root caries spreads across the cementum or dentin surface to a certain extent, while initially its depth is limited.
The dentin of the root has fewer dentinal tubules than coronal dentin, It has been observed that bacteria are already able to penetrate the cementum layer in an early state of root caries development, while bacteria penetrate into the underlying dentin at a later state of lesion development.
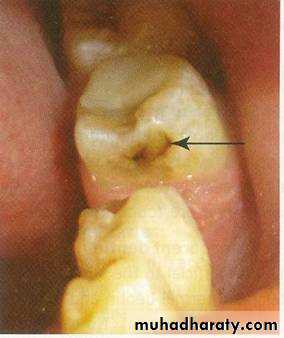
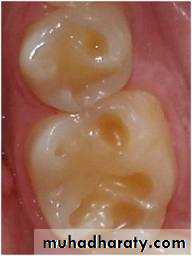
Arrested carious lesion is a lesion that may have formed
earlier and then stopped. It usually presents as a largeopen cavity which no longer retains food and becomes
self-cleansing.
Arrest Caries and Remineralization


Arrested carious lesions are most commonly seen on
lingual and labial aspects of teeth and less commonlyinterproximally.
On the proximal surface, it appears as
brown-stained area just below contact point of retained
tooth. Here, the caries process is arrested because prox imal surface becomes self-cleansing due to extraction of adjacent teeth.
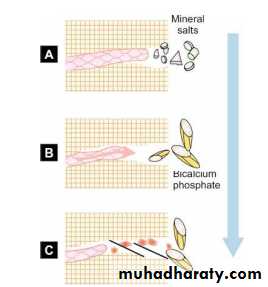
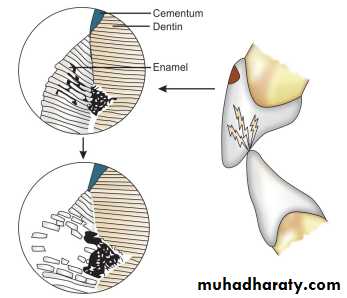
First Stage
•The acids produced by bacteria dissolve the minerals of the surrounding intertubular dentin• The tubule fluid becomes saturated with calcium magnesium and phosphate ions
• If less acid is produced then the second stage can occur.
Stages of Development of Arrested Caries
Second Stage
Large crystals of tricalcium phosphate are formed byprecipitation of saturated crystals.
Third Stage
• The odontoblast process secretes collagen into the
dentin tubule.
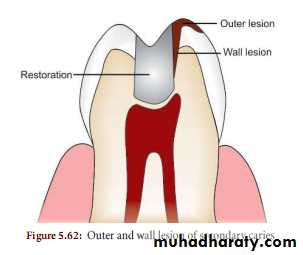
Secondary or recurrent caries can be defined as contact caries, which refers to caries on the tooth surface which is in contact with the restoration.
RECURRENT CARIES/SECONDARY CARIES


Though restorations are placed to restore a damaged
tooth to its form, functions and esthetics but none of therestorations can last for ever.
Most of the restorations are replaced because of the clinical diagnosis of recurrent caries which is thought to be within a range of 45 to 55 percent. The recurrent caries are seen more often in resin-based composite restorations than the amalgam restorations.




•The main causative factor for recurrent caries is
marginal leakage around the restorations• Factors which predispose to recurrent caries are
ditching or fracture of the restoration at the edges
• Fracture of the marginal tooth structure, microleakage.
• Presence of overhangs
• Rough surface of the restoration along with poor oral
hygiene
• An improper tooth preparation
• Unpolished enamel surfaces.
Etiology
Non-carious lesions
Non- carious lesions
1- Erosion2- Abrasion
3- Abfraction4- Attrition
Erosion

1-Erosion
Definition: It is defined as a loss of tooth substance caused by a chemical process that does not involve known bacterial action.In general, erosion appears as sharply defined wedge shaped or irregular depression caused by chemicals in the cervical area usually on the facial tooth surface
It is classified according to the source of the acid, either INTRINSIC or EXTRINSIC.
Intrinsic sources of acids originate in the stomach and are associated with eating disorders, such as anorexia and bulimia nervosa, or with acid reflux and regurgitation.
Extrinsic sources are acids contained in dietary components, such as carbonated soft drinks and fruit and fruit juices.
EXTRINSIC FACTORS
– Environmental erosioni. Professional wine tasters, battery, electroplating
Chemical manufacture.
ii. Swimmers


– Dietary origin: High intake of
i. Citrus fruit and juicesii. Carbonated beverages
iii. Acidic fruit flavored candies
iv. Pickled foods



– Medicinal origin
i. Aspirin
ii. Vitamin C
iii. Iron tonicsiv. Acidic mouthwashes



Intrinsic factor
It occurs due to involvement of endogenous acids, mainly due to regurgitation of gastric acid into the oral cavity. This may occur in certain conditions such as:– Eating disorder
i. Anorexia nervosa
ii. Bulimia nervosa

– Vomiting
i. Recurrent vomitingii. Psychogenic vomiting syndrome
iii. Drug induced vomiting
– Pregnancy morning sickness
– Gastrointestinal disorder– Chronic alcoholism

Abrasion
Definition: It is defined as the loss of tooth substance induced by mechanical wear other than that of mastication.

Etiology of abrasion: Various etiological factors are:
A) Faulty oral hygiene practice:– Horizontal brushing technique or improper brushing technique

– Use of toothbrush with hard bristles
– Use of abrasive toothpaste– Excessive time, force and frequency of brushing
– Excessive use of interproximal brush



B) Abnormal oral habits:
– Use of toothpicks.– Finger nail biting.

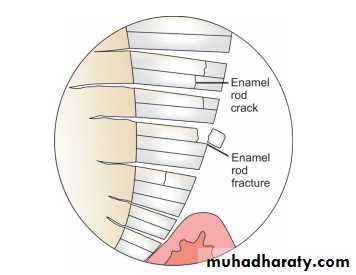
Abfraction


Abfraction Lesion
These are wedge type defects usually occur in cervical areas of tooth due to excessive occlusal stresses or parafunctional habits such as bruxism.Abfractions are the microfractures which appear in the enamel on cervical area of tooth, and flexed under heavy loads. Abfraction lesion appears as a wedge shaped defect with sharp line angles
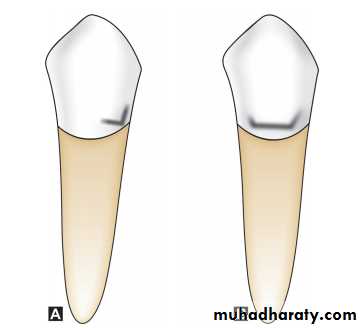
Abfractions are commonly found in cases where mal-aligned canines cause initial lateral guidance forces to be exerted on the lingual incline of the buccal cusp of the maxillary premolar.
Attrition

ATTRİTİON
It is defined as a physiological, continuous, process resulting in loss of tooth structure from direct frictional forces between contacting teeth.It occurs both on occlusal and approximal surfaces. Attrition is accelerated by parafunctional mandibular movements, especially bruxism.