ACUTE DISC HERNIATION LUMBO-SACRAL
Lec-1+2Prof.DR.SADEQ AL-MUKHTAR
CONSULTANT ORTHOPAEDIC SURGEON
Historical review
Sciatica used by GreeksIschias =Pain arising from or around the hip and thigh.
Hippocrates (460-370 B.C) noted that ischiatic pain mainly affected men aged 40-60 years and that in younger men it usually lasted for 40 days.
Development ”Embryology” :
Started in the 3rd week of gestation to3rd decade of life.During the 4th week of development the cells of sclerotomes shift their position to surround the spinal cord and notochord then the caudal portion of each sclerotome segment proliferates extensively and condenses and the caudal half of one sclerotome binds the cephalic half of the next sclerotome
In the fetus, the spinal cord extends to the lower limit of the spinal dura mater at the level of the 2nd sacral vertebra.
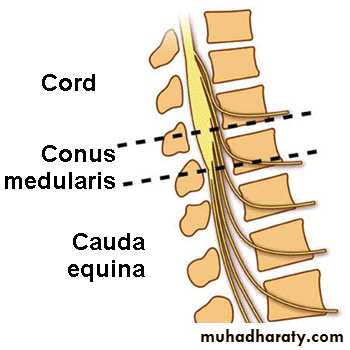
At birth the conus medullaris lies opposite the 3rd lumbar vertebra and does not reach its permanent level opposite the 1st or 2nd vertebra until the age of twenty.
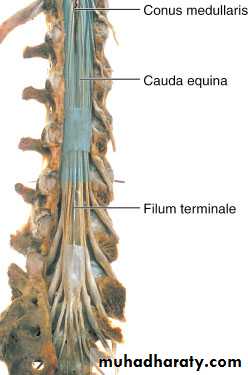
Below L1 the anterior and posterior roots pass almost vertically downward through the subarachnoid space and form with the centrally disposed filum terminale of pia mater ,the cauda equina
The peripheral lumbar roots usually leaves the dural sheath opposite a disc level e.g L3-4 and then passes distally within the canal to leave it through intervertebral foramen one segment lower e.g L4-5.
BIOMECHANICS OF LUMBAR SPINE
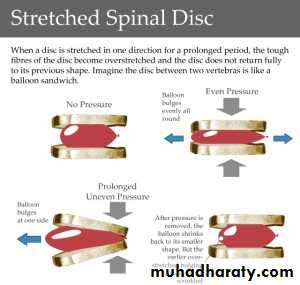
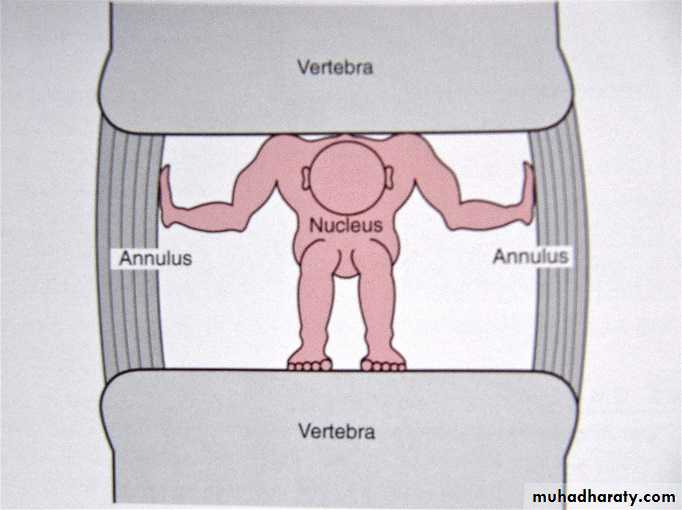
Human vertebral column is exposed to both DYNAMIC and STATIC forcesThe nucleus pulposus act like a fluid-filled ballon distributing the axial pressure equally over the cartilage plates and over the annulus fibrosus, the fibers of which become elongated.
In SYMMETRIC and AXIAL LODING: The expanding nucleus pulposus will be pressed against the elastic annulus fibrosus. As soon as the pressure relieved the nucleus retains its form and position.
In ASYMMETRIC LOADING: The central part of the disc containing the nucleus pulposus will migrate towards the area of least load.
ANATOMY
The bodies of adjacent vertebrae are held together by :1-Strong intervertebral disc.
2-Anterior longitudinal ligament.
3-Posterior longitudinal ligament
The intervertebral disc as a secondary cartilaginous joint .It consist of:
a-The cartilage plate.
b-The annulus fibrosus.
c-The nucleus pulposus.
Disc pressure is related to the body position;
the lumber disc pressure is higher in sitting position compared with standing .This is due to increase in muscular activity in the back in sitting and leaning forward, the intra-discal pressure increases as the center of the body is not as in lordotic posture in the center of the disc but is move anteriorly.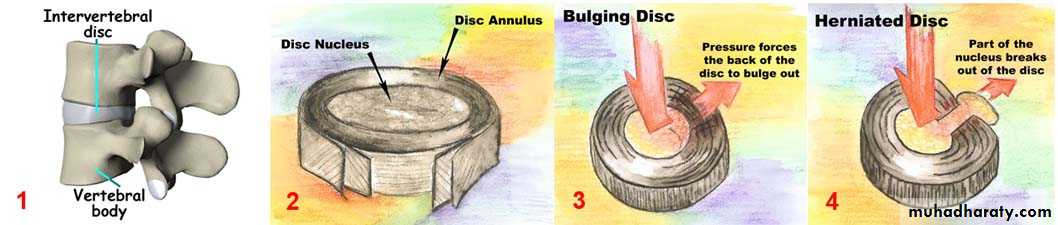
It has been shown that when anaesthetized and supine patient, weighing 70 kg has loading of 20 kg in his 3rd lumbar disc. This increases to a maximum loading of 270 kg when the individual is sitting and leaning forward with an additional 20 kg in his hands.
The decreases in inter-vertebral distance will diminish the intra-foramenal space by 1/5th and also inflammation and swelling of the peri-neural tissue in disc prolapsed or with osteophyte reaction of the articular facets, the space will decrease considerably.
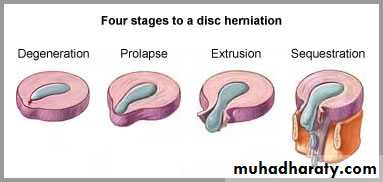
TYPE OF DISC HERNIATION:
Vertical HerniationSchmorls nodes
Horizontal Herniation
Protrusion
Extrusion
Sequestration
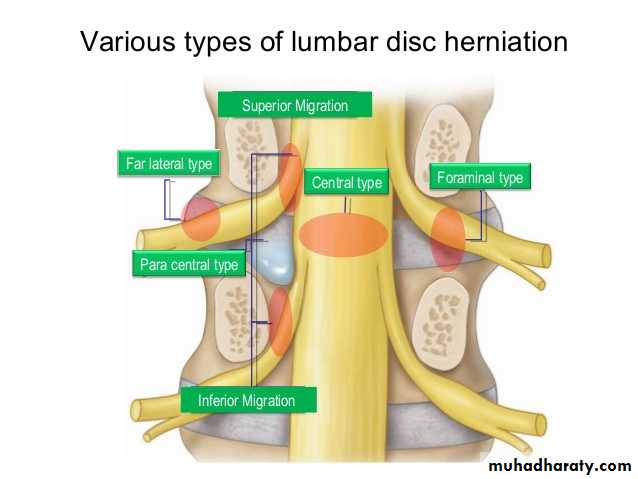
Site of Herniation
Central Herniation:Small Central
Massive Central
Lateral Herniation:
Intermediate Hermiation:
Intraforaminal
Clinical Features
63% of working adults, age 45-49 years had low back pain.37% of above having had Sciatica.
History:
Pain-acute/chronic.Site-Type-Radiation
Intermittency of symptoms
Paresthesia
Loss of sensation or Motor Power
Urgency or Frequency of Micturation
EXAMINATION
Walking and Standing-undressed
Gait
Supine position-SLR-Test
Confirm the test:
Bragards test-Dorsiflexion of Ankle.
Compression of common P.N.
Flexion of Cervical Spine.
Contralateral SLR-Test “Well Test”
Neurological Examination
Muscle weakness and AtrophyTendon Reflexes:
Depressed Ankle (S1,2) Reflex in L5,S1 LEVEL-Examin both Ankles.
Compression of L5 Root most commonly cause no reflex change ,but sometime causes increased Knee jerk because of weak antagonists.
L4 Root lesion result in depressed patellar tendon reflex(L2-4).
Differential Diagnosis
Bony Abnormalities: Spondylolisthesis / Spondylosis / Spinal canal stenosis.
Inflammatory: Discitis/T.B/Acute extradural abscess/Viral radiculitis.
Tumors: Ependymoma of filum terminale or conus medullaris/Neuroma/Meningioma.
Degenerative: Degenerative lesions of spinal cord and peripheral neuropathies/D.M.
Bony nerve Entrapment: Subluxation of facet joints/Narrowing of root canal.
Vascular: Peripheral vascular occlusive diseases.
INVESTIGATIONS
Plain X-Rays
Radiculography-Colored Water soluble material injection intrathecal.
CT-Scan
MRI
Haematological test: ESR/Wbc count/Brucella test ….etc. to exclude other differential diagnosis
Treatment
Conservative:Bed rest-Skin traction for 3 weeks.Surgical:
Full Laminectomy.
Partial hemi-laminectomy.
Fenestration.
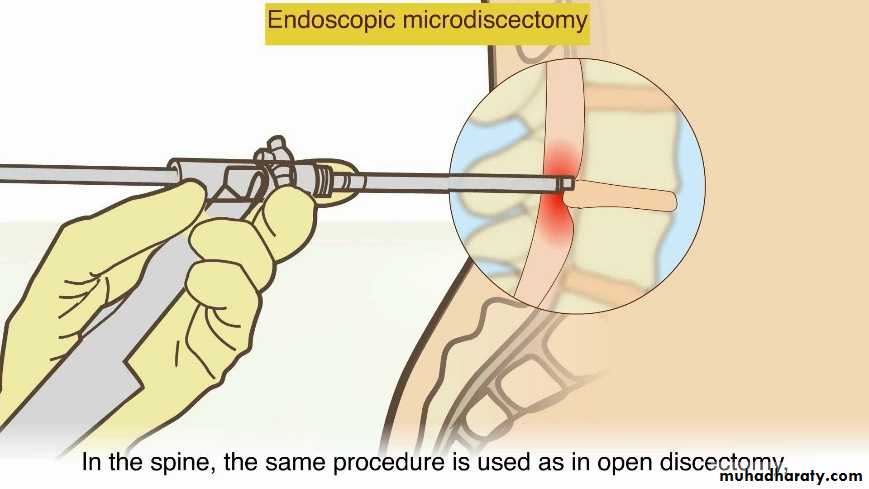
Micro discectomy-Endoscopic.
Chemonucleolysis