Dermatoses Resulting from Physical Factors

Heat injuries

The body requires a certain amount of heat, but beyond definite
limits, insufficient or excessive amounts are injurious. The local action of excessive heat causes burns or scalds; on the other hand, undue cold causes chilblains, frostbite. The solar spectrum has been divided into different regions by wavelength. The parts of the solar spectrum important in photomedicine include UV radiation (below 400 nm), visible light (400–760 nm), and infrared radiation (beyond 760 nm). UVA, 320–400 nm; UVB, 280–320 nm; and UVC, 200–280 nm..a- First-degree burns of the skin result merely in an active congestion of the superficial blood vessels. Ordinary sunburn is the most common example of a first-degree burn. The pain and
increased surface heat may be severe, and it is not rare to have some constitutional reaction if the involved area is large
B-Second-degree burns are subdivided into superficial and deep forms.
In the 1- superficial second-degree burn, there is a transudation of serum from the capillaries, which causes edema of the superficial tissues. Vesicles and blebs are formed by the serum gathering beneath the outer layers of the epidermis. Complete recovery without scarring is usual in patients with superficial burns.2-The deep second-degree burn is pale and anesthetic. Injury to the reticular dermis compromises blood flow and destroys appendages, so healing takes more than 1 month and results in scarring.
sunburn
Sunburn is the normal cutaneous reaction to sunlight in excess of an erythema dose. UVB erythema becomes evident at around 6 h after exposure and peaks at 12–24 h,
The minimal amount of a particular wavelength of light capable of inducing erythema on an individual’s skin is called the minimal erythema dose (MED). Although the amount of UVA radiation is 100 times greater than UVB radiation during midday hours, UVB is up to 1000 times more erythemogenic than UVA, and so essentially all solar erythema is caused by UVB
Treatment
1-Immediate first aid for minor thermal burns consists of prompt cold applications (ice water, or cold tap water if no ice is available), which are continued until pain does not return on stopping them. 2-The vesicles or blebs of second-degree burns should not be opened but should be protected from injury because they form a natural barrier against contamination by microorganisms.sunburn

sunburn

Miliaria, the retention of sweat as a result of occlusion of eccrine sweat ducts, produces an eruption that is common in hot, humid climates, such as in the tropics and during the hot summer. Staphylococcus epidermidis,
which produces an extracellular polysaccharide substance,
induces miliaria in an experimental setting. This
polysaccharide substance may obstruct the delivery of sweat
to the skin surface. The occlusion prevents normal secretion
from the sweat glands, and eventually pressure causes rupture
of the sweat gland or duct at different levels. The escape of
sweat into the adjacent tissue produces miliaria
.
Types of miliaria
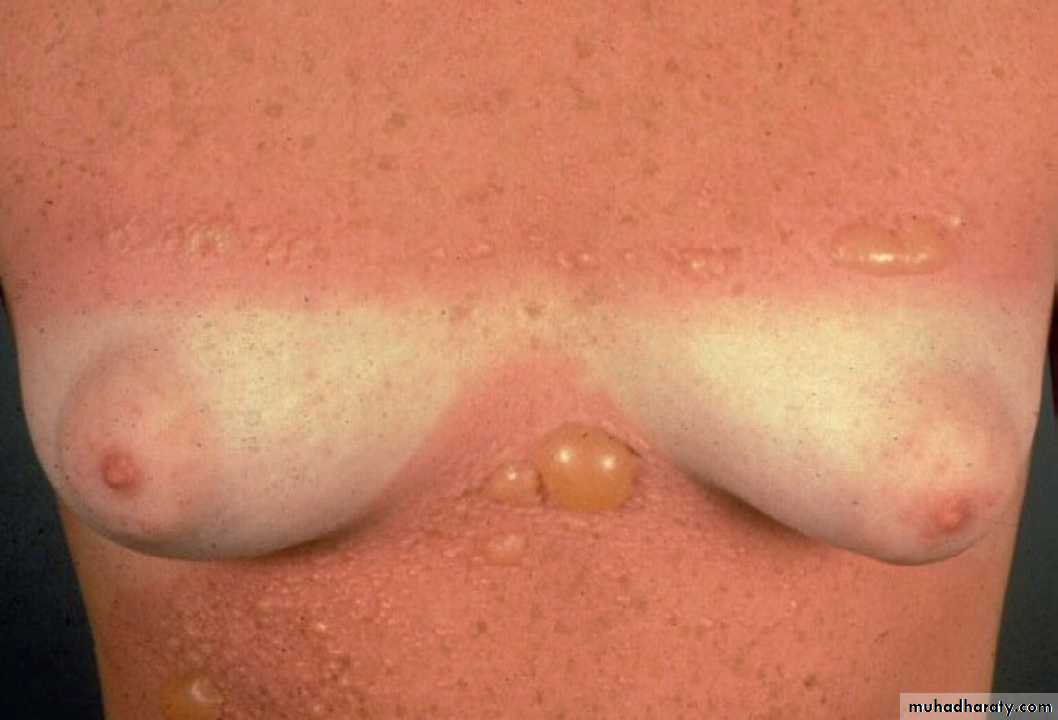
1. Miliaria crystallina:is characterized by small, clear,superficial vesicles with no inflammatory reaction. It appears
in bedridden patients in whom fever produces increased perspiration
or in situations in which clothing prevents dissipation
of heat and moisture, as in bundled children. The lesion are generally asymptomatic and their duration is short-lived
because they tend to rupture at the slightest trauma
Miliaria crystallina

Types of miliaria

2.Miliaria rubra (prickly heat) appear as discrete , extremely pruritic, erythematous papulovesicles accompanied
by a sensation of prickling, burning, or tingling. They later
may become confluent on a bed of erythema The sites most frequently affected are the antecubital and popliteal fossae,
trunk, infra-mammary areas (especially under pendulous
breasts), abdomen (especially at the waistline), and inguinal
regions; these sites frequently become macerated because
evaporation of moisture has been impeded. Exercise-induced
itching may also be caused by miliaria rubra.
Miliaria rubra

miliaria
3.Miliaria pustulosa
is preceded by another dermatitisthat has produced injury, destruction, or blocking of the sweat
duct. The pustules are distinct, superficial, and independent
of the hair follicle. The pruritic pustules occur most frequently
on the intertriginous areas, flexure surfaces of the extremities,
scrotum, and back of bedridden patients
Miliaria pustulosa

treatment
1-The most effective treatment for miliaria is to place the patient in a cool environment. Even a single night in an air-conditioned room helps to alleviate the discomfort. Next best is the use of circulating air fans to cool the skin. 2-Anhydrous lanolin resolves
the occlusion of pores and may help to restore normal swe
secretions. 3-Hydrophilic ointment also helps to dissolve keratinous
plugs and facilitates the normal flow of sweat.
4-cooling baths containing colloidal oatmeal or cornstarch are
beneficial if used in moderation. Mild cases may respond to
dusting powders, such as cornstarch or baby talcum powder
Erythema ab igne
Erythema ab igne is a persistent erythema—or the coarsely
reticulated residual pigmentation resulting from it—that isusually produced by long exposure to excessive heat Erythema ab igne occurs on the legs as a result of habitually
warming them in front of open fireplaces, space heaters, or car
heaters. Similar changes may be produced at sites of an electric
heating pad application such as the low back, or the upper
thighs with laptop computers. The condition occurs also in
cooks, silversmiths, and others exposed over long periods to
direct moderate heat.
treatment
The use of emollients containing α-hydroxy acids or a cream
containing fluocinolone acetonide 0.01%, hydroquinone4%, and tretinoin 0.05% may help reduce the unsightly pigmentationEpithelial atypia, which may lead to Bowen’s disease and
squamous cell carcinoma, has rarely been reported to occur
overlying erythema ab igne. Treatment with 5-fluorouracil
(5-FU) or imiquimod cream may be effective in reversing this
epidermal alteration
Erythema ab igne

Cold injuries
Exposure to cold damages the skin by at least three mechanisms.
•1. Reduced temperature directly damages the tissue, as infrostbite and cold immersion foot.
•2. Vasospasm of vessels perfusing the skin prevents
adequate perfusion of the tissue and causes vascular
injury and consequent tissue injury (pernio, acrocyanosis,
and frostbite).
•3. In unusual circumstances, adipose tissue is predisposed
to damage by cold temperatures due to fat composition
or location. Outdoor workers and recreationalists, the armed forces,
alcoholics, and the homeless are particularly likely to suffer
cold injuries.
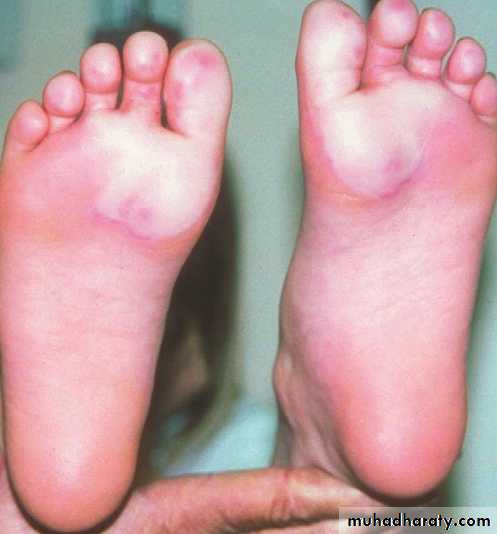
Chilblains (pernio)
Chilblains constitute a localized erythema and swelling caused
by exposure to cold. Blistering and ulcerationsmay developin severe cases. In people predisposed by poor peripheral circulation,
even moderate exposure to cold may produce chilblains.
chilblain

Chilblains occur chiefly on the hands, feet, ears, and face,
especially in children; onset is enhanced by dampness
chilblain
Patients with chilblains are often unaware of the cold injury
when it is occurring, but later burning, itching, and rednesscall it to their attention. The affected areas are bluish-red, the
color partially or totally disappearing on pressure, and are
decidedly cool to the touch. Sometimes the extremities are
clammy because of excessive sweating.

treatment
1.The affected parts should be protected against further exposure
to cold or dampness. If the feet are affected, woolen socksshould be worn at all times during the cold
Months
2. Nifedipine, 20 mg three times a day, has been effective.
Vasodilators such as nicotinamide, 500 mg three times a day,
or dipyridamole, 25 mg three times a day, or the phosphodiesterase
inhibitor sildenafil, 50 mg twice daily, may be used
to improve circulationSpontaneous resolution occurs without treatment in 1–3 weeks.
frostbite
When soft tissue is frozen and locally deprived of blood
supply, the damage is called frostbite. The ears, nose, cheeks,fingers, and toes are most often affected. The frozen part painlessly
becomes pale and waxy. Various degrees of tissue
destruction similar to those caused by burns are The degree of injury is
directly related to the temperature and duration of freezingencountered
frostbite
frostbite

frostbite
Treatment
Early treatment of frostbite before swelling develops shouldconsist of covering the part with clothing or with a warm hand
or other body surface to maintain a slightly warm temperature
so that adequate blood circulation can be maintained. Rapid rewarming in a water bath between 37 and 43°C (100–110°F)
is the treatment of choice for all forms of frostbite. Rewarming
should be delayed until the patient has been removed to
an area where there is no risk of refreezing. Slow thawing
results in more extensive tissue damage.
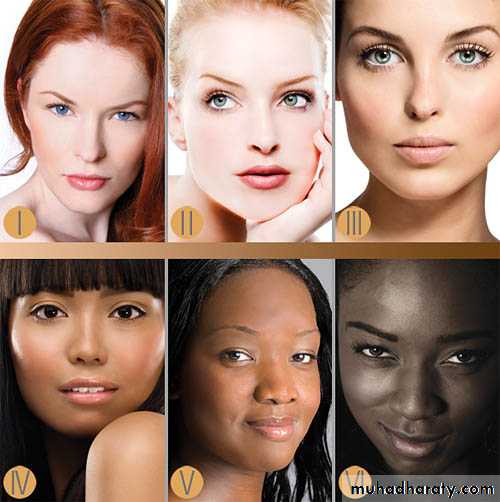
Skin type Baseline skin color Sunburn and tanning history
I White Always burns, never tans
II White Always burns, tans minimally
III White Burns moderately, tans
gradually
IV Olive Minimal burning, tans well
V Brown Rarely burns, tans darkly
VI Dark brown Never burns, tans darkly
Skin types
Polymorphic light eruption
A common acquired sunlight-inducedPolymorphous light eruption (PLE, PMLE) is the most common form of photosensitivity, a history of PLE can be elicited in between 5% and 20% of the adult population.disorder typically presenting in the spring.
Clinical presentation: a pruritic,
erythematous, symmetrically distributed,
papulovesicular eruption, usually on
exposed areas, within hours of exposure
to ultraviolet radiation A change in the amount of sun exposure appears to be more critical than the absolute amount of radiation. The lesions of PLE appear most often 1–4 days after exposure to sunlight, most commonly
sunlight, with full resolution in days to
several weeks.
Polymorhic light eruption
Genetics: most likely a genetically
determined delayed-type hypersensitivity
reaction against UVR-induced cutaneous
antigen(s).
Therapy: responds to broad-spectrum
sunscreen use, oral or topical steroids, and
prophylactic low-dose immunosuppressive
Phototherapy
Polymorphic light eruption


COMPLICATIONS. A very few patients with PMLE
may develop LE, as there is a higher than normal prevalenceof prior PMLE in patients with LE. However,
the presence of autoantibodies does not portend development
of LE. Patients with PMLE may also experience
significant disease-related psychosocial morbidity. The
rate of both anxiety and depression in patients with
PMLE are twice that of the general population, and
these rates are similar to those observed in patients
with psoriasis and atopic dermatitis
PREVENTION. PMLE may often be avoided by moderating
sunlight exposure, wearing protective clothing
and applying broad-spectrum high-protection-factor
sunscreens regularly. Sunscreens with UVA and UVB
protection may prevent PMLE eruptions in photoprovocable
patients, but sunscreens without UVA
protection are generally ineffective. Prophylactic phototherapy
each spring or before sunny vacations tends
to prevent attacks.
Selection of Diseases Sometimes Exacerbatedby Ultraviolet Irradiation
Acne
A topic eczemaCarcinoid syndrome
Cutaneous T-cell lymphoma
Dermatomyositis
Disseminated superficial actinic porokeratosis
Erythema multiforme
Familial benign chronic pemphigus (Hailey–Hailey disease)
Keratosis follicularis (Darier disease)
L ichen planus
L upus erythematosus
Pellagra
Pemphigus foliaceus (erythematosus)
Pityriasis rubra pilaris
Psoriasis
Reticulate erythematous mucinosis syndrome
Rosacea
Seborrheic eczema
Transient acantholytic dermatosis (Grover disease)
Viral infections