1
Third stage
Surgery
Lec-3
.د
سعدالله الزكو
1/1/2014
Malignant Skin Tumors
Basal cell carcinoma (BCC)
Most common, 75% of skin tumors.
Affects white skin, Male: Female=3:2 .
Commonly Caucasian male older than 60 years
Occurs on exposed parts: face, neck, scalp.
Arise from basal layer of epidermis.
No metastasis.
Etiological factors:
1-chronic exposure to sun light
2-chemicals: arsenic, hydrocarbons
3-ionizing radiation
4-xeroderma pigmentosa
5-basal cell nevus syndrome
6- low immunity (AIDS, renal transplant)
7- smoking
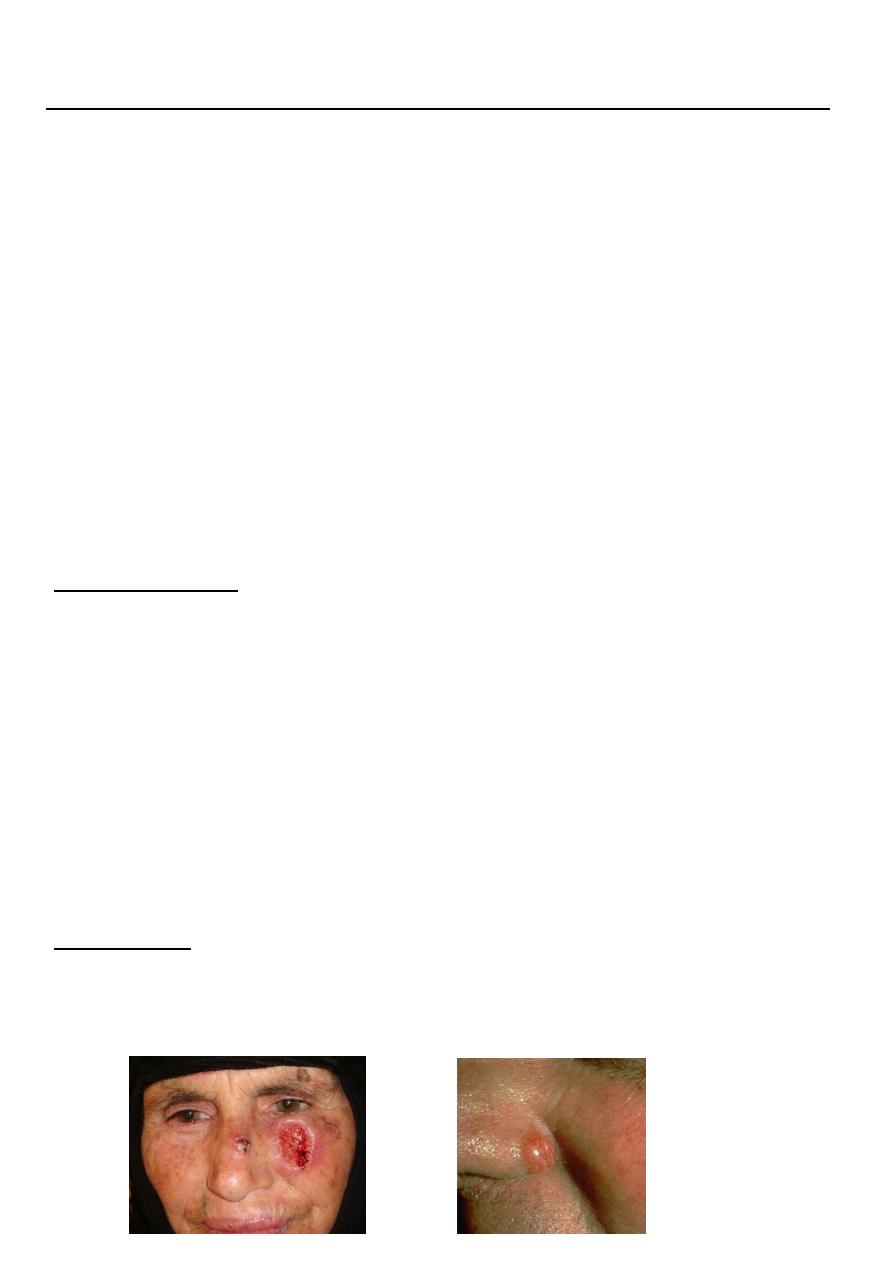
Clinical types:
1-Nodulo-ulcerative : commonest type, usually single lesion, as pearly or translucent
nodule with raised borders and telangiectasias, grow slowly, tend to ulcerate, giving rise
“rodent ulcer”.

2
2. Pigmented BCC: second most common type, combines features of nodulo-ulcerative
&deep brown to lack brown to black nodule.
3-Superficial BCC: lightly pigmented erythematous patch, may be scaly, with areas of
scarring, mistaken for eczema ,often multiple, on trunk.
4-Sclerosing BCC: yellowish-white, ill-defined border, resemble scar ,it showes peripheral
growth with central scarring.
5-BC nevus syndrome: genetically determined (autosomal dominant), multiple BCC, skin
pits on palms & soles, jaw cyst, rib anomaly.
Diagnosis:
by biopsy (FNA, incisional biopsy , excisional biopsy)
Treatment:
Surgery: excision with 2-5 mm. healthy margin, & repair defect by skin graft or flap.
Radiotherapy: in large lesion, oldman, refusing operation.
Cryotherapy: for primary lesion < 2 cm., but hypopigmentation, scarring are
disadvantages.
3
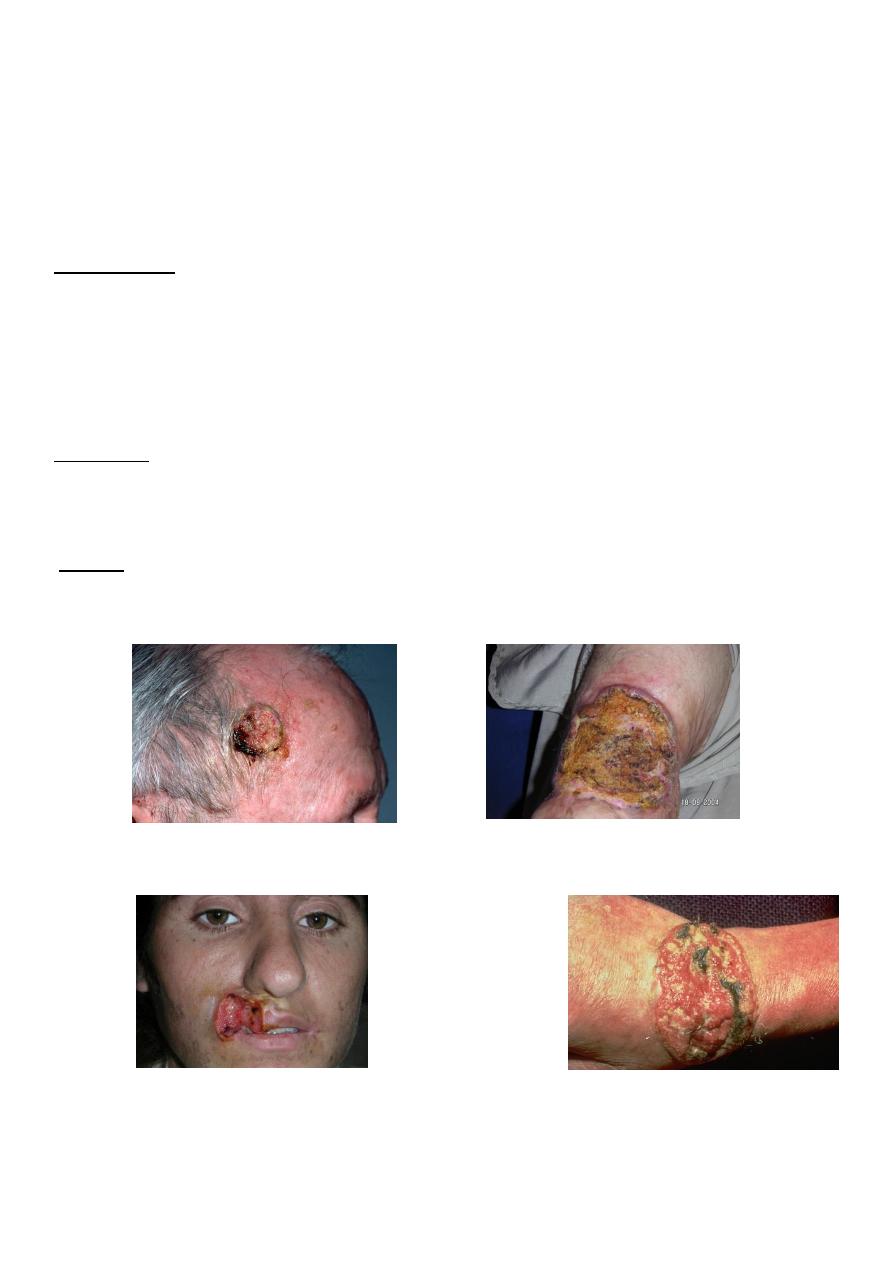
Squamous Cell Carcinoma
(SCC) is second most common skin cancer.
Arises from the malignant transformation of keratinocytes in the epidermis.
Arise either in normal skin or in preexisting lesion as (actinic keratosis, leukoplakia,
radiation keratosis, scars ( where called Marjolin ulcer).
Risk factors:
1- UV radiation exposure is the most important (common in farmers, sailors)
2-ionizing radiation, arsenic, and certain other chemicals, also hereditary( xeroderma
pigmentosa)
3-fair- colored skin and red-hair are at higher risk
Clinically:
Present as irregular ulcer, everted edge, indurated base, attached deeply, blood-stained
discharge, frequent lymph N. positive.
Types:
1-Slow growing : is verrucous, may be deeply locally invasive, likely to metastasize, more
differentiated.
2-Rapid growing: more nodular & indurated, early ulceration with local invasion, greater
metastasis, less differentiated.

4
Treatment:
* biopsy done.
1- Excision
Surgical excision with 10-mm margin offers the advantages of histologic diagnosis, rapid
healing, and improved cosmesis.
If lymph n. positive: excise lesion with lymph n. dissection.
2-Radiation therapy
Radiation therapy is best used in older patients, who are poor surgical candidates It has a
high cure rate (90- 95% )
Malignant Melanoma:
result of the malignant transformation of melanocytes, the pigment forming cells.
Occurs mainly in skin, also in eye, mouth,anus, vagina .
Etiology/risk factors
1-Positive family history in 5-10% of patients.
2-Blue eyes, red hair, white skin, freckling.
3-Benign and/or dysplastic melanocytic nevi
4-Immunosuppression (in renal transplant).
5-High UV radiation .
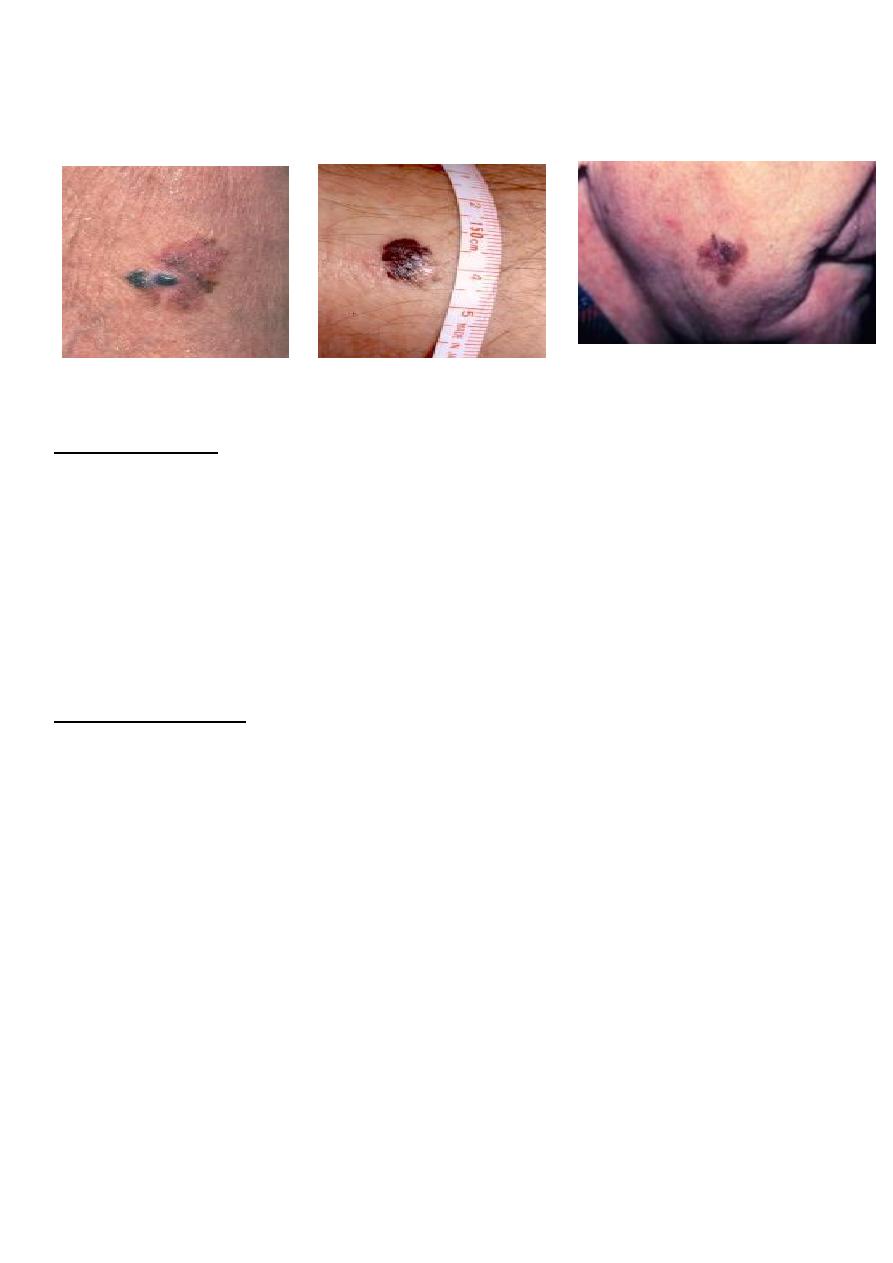
Malignant melanoma (MM) types:
1-Superficial spreading : 70% of MM, arise in a preexisting dysplastic nevus which changes
slowly over several months , usually flat, later become irregular and elevated.
2-Nodular melanoma : 15-30%, growth deeply into dermis .
3-Lentigo maligna: 4-10%, often larger than 3 cm, flat, tan, and begin as small, frecklelike
lesions. They occur in sun-exposed areas (eg, face and neck) of older individuals.
4-Acral lentiginous : 2-8% , in whites and 35-60% in dark-skinned ,occur on the palms,
beneath the nail beds, and soles.
5
5-Desmoplastic melanoma: 1% , tendency for perineural invasion, especially in the head
and neck
Breslow staging:
based on vertical thickness of the lesion from thickest point:
Stage 1 : Thickness of 0.75 mm or less
Stage 2: Thickness of 0.76-1.5 mm
Stage 3 :Thickness of 1.51-4 mm
Stage 4: Thickness greater than 4 mm
Surgical treatment:
-After diagnosis by biopsy, wide excision of primary lesion & removal of lymph node
involved or at high risk.
-Excision with 2-3 cm healthy margin.
-Elective L.N. dissection done in lesions 1-4 mm depth, but not <1mm or >4mm.
Superficial Spreading
Nodular Melanoma
Lentigo Maligna