
1
Third stage
Medicine
Lec-2
د
.
اسماعيل
1/1/2014
Presenting problems in GIT diseases (part 2)
LOWER GIT BLEEDING
Severe acute lower gastrointestinal bleeding
:
This is an unusual medical emergency. Patients
present with profuse red or maroon diarrhoea and with shock.
1. Diverticular disease is the most common cause. Acute bleeding is due to erosion of an artery
within the mouth of a diverticulum and bleeding almost always stops spontaneously. If
bleeding continues, the diseased segment of colon will need to be resected after confirmation
of the site (by angiography or colonoscopy).
2. Angiodysplasia is a disease of the elderly in which vascular malformations develop in the
proximal colon. Bleeding can be acute and profuse; it usually stops spontaneously but
commonly recurs. Diagnosis is often difficult. Colonoscopy reveals characteristic vascular
spots which are reminiscent of spider naevi. In acute bleeding, visceral angiography shows
bleeding into the intestinal lumen and an abnormal large, draining vein. In some patients
diagnosis is only achieved by laparotomy with on-table colonoscopy..
The treatment of choice is endoscopic thermal ablation, but resection of the affected bowel may be
required if bleeding continues.
3. Ischaemia is due to occlusion of the inferior mesenteric artery and presents with abdominal
colic and rectal bleeding. It should be considered in patients (particularly the elderly) who have
evidence of generalised atherosclerosis. Diagnosis is made at colonoscopy. Resection is
required only in the presence of peritonitis.
4. Meckel's diverticulum with ectopic gastric epithelium may ulcerate and erode into a major
artery. The diagnosis should be considered in children or adolescents who present with
profuse or recurrent lower gastrointestinal bleeding. A Meckel's 99mTc-pertechnate scan is
sometimes positive but the diagnosis is commonly made only by laparotomy, at which time the
diverticulum is excised.
Subacute or chronic lower gastrointestinal bleeding
This is extremely common at all ages and is usually due to haemorrhoids or anal fissure.
Haemorrhoidal bleeding is bright red and occurs during or after defecation. Proctoscopy is used to
make the diagnosis but in subjects who also have altered bowel habit and in all patients
presenting at over 40 years of age, colonoscopy or barium enema is necessary to exclude
coexisting colorectal cancer. Anal fissure should be suspected when fresh rectal bleeding and
anal pain occur during defecation.
chronic/subacute,
Other causes: Inflammatory bowel disease, Carcinoma, Large polyps, Angiodysplasia
Radiation enteritis, Solitary rectal ulcer\syndrome (SRUS).
2
OBSCURE MAJOR GASTROINTESTINAL BLEEDING:
In some patients who present with major gastrointestinal bleeding, upper endoscopy and
colonoscopy fail to reveal a diagnosis. When bleeding continues, urgent mesenteric
angiography is indicated. This will usually identify the site if the bleeding rate exceeds 1 ml/min
and embolisation can sometimes be used to stop the bleeding. If angiography is negative,
enteroscopy can be used to visualize the proximal small intestine and treat the bleeding source.
Wireless capsule endoscopy is also used to define a source of bleeding and, unlike push
enteroscopy, the jejunum and ileum are visualized. When all else fails, laparotomy with on-table
endoscopy is indicated.
OCCULT GASTROINTESTINAL BLEEDING :
'Occult' means that blood or its breakdown products are present in the stool but cannot be
seen. Occult bleeding may reach 200 ml per day, cause iron deficiency anaemia and signify
serious gastrointestinal disease. Any cause of gastrointestinal bleeding may be responsible but
the most important is colorectal cancer, particularly carcinoma of the caecum which may have no
gastrointestinal symptoms. In clinical practice, investigation of the gastrointestinal tract should be
considered whenever a patient presents with unexplained iron deficiency anaemia. Testing the
stool for the presence of blood is unnecessary and should not influence whether or not the
gastrointestinal tract is imaged because bleeding from tumours is often intermittent and a
negative faecal occult blood (FOB) test does not exclude important gastrointestinal
disease. Many colorectal cancer patients are FOB-negative at presentation, and the only value
of FOB testing is as a means of screening for colonic disease in asymptomatic populations
.
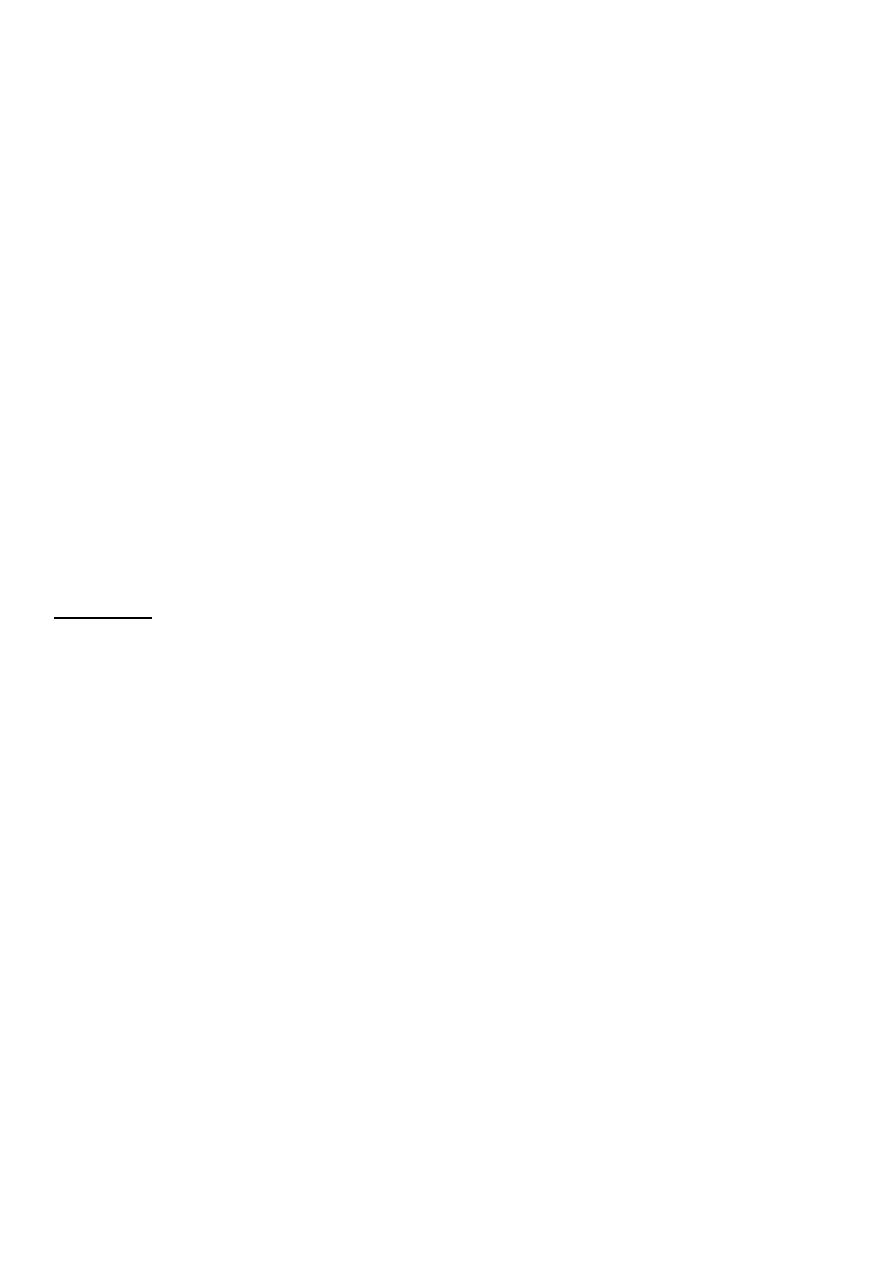
Vomiting:
Vomiting is usually associated with nausea, retching, salivation, anorexia or
dyspepsia. It is important to distinguish true vomiting from regurgitation and to elicit whether the
vomiting is acute or chronic (recurrent), as the underlying causes may differ. Associated
symptoms of abdominal pain, fever, diarrhoea, relationship to food, drug ingestion, headache,
vertigo and weight loss should be sought.
Examination may reveal:
signs of dehydration, fever and infection.
Evidence of abdominal masses, peritonitis or intestinal obstruction.
Neurological signs including papilloedema, nystagmus, photophobia and neck stiffness.
Other findings may suggest alcoholism, pregnancy or bulimia as the underlying diagnosis.
The diagnostic approach will be dictated by the history and examination.
3
Causes of vomiting:
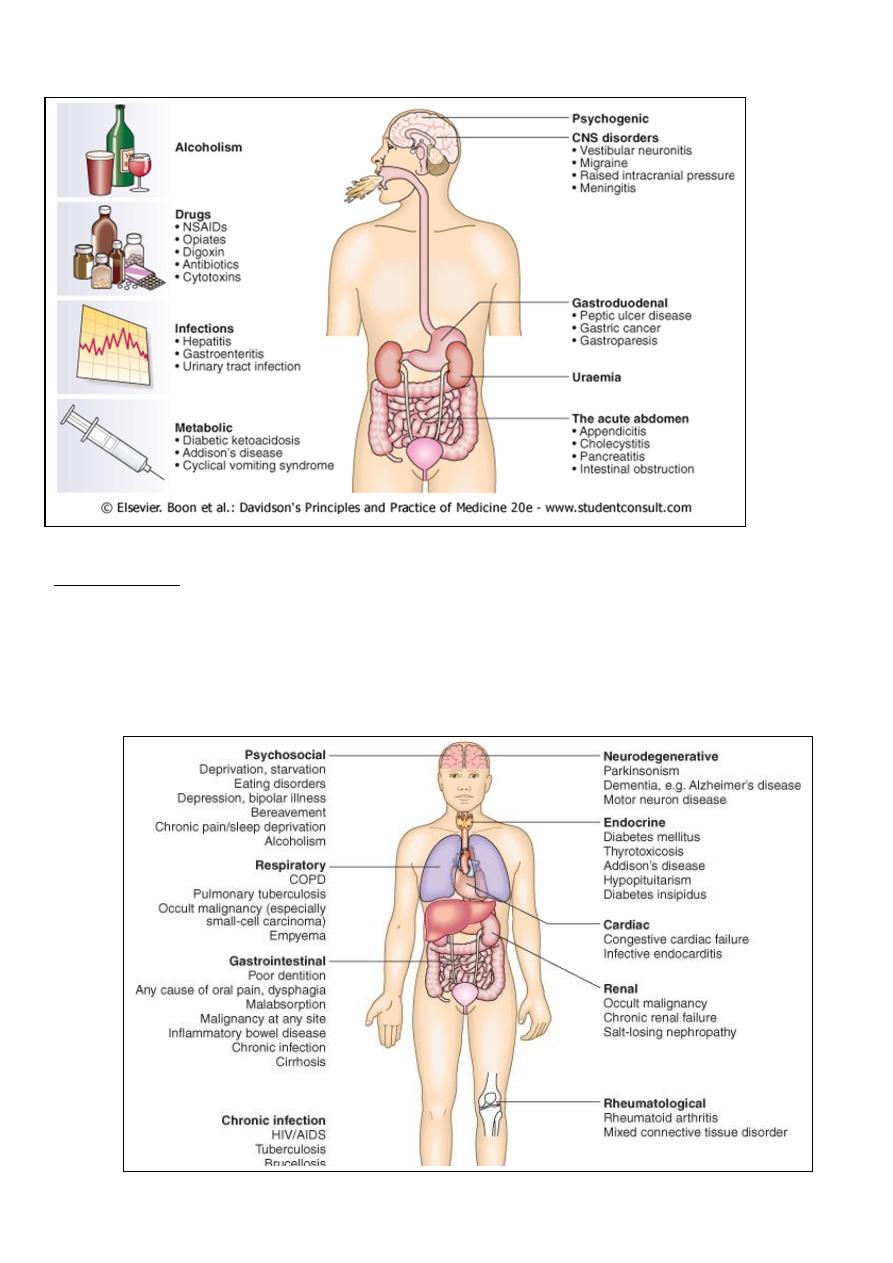
Weight loss:
Weight loss may be 'physiological' due to dieting, exercise, starvation, or the
decreased nutritional intake which accompanies old age. Alternatively, weight loss may signify
disease; a loss of more than 3 kg over 6 months is significant. Hospital and general practice
weight records may be valuable, as may reweighing patients at intervals, as sometimes weight is
regained or stabilises in those with no obvious cause.
Pathological weight loss can be due to psychiatric illness, systemic disease, gastrointestinal
causes or advanced disease of any specific organ system.

4
Physiological' weight loss: This may be obvious in cases of young individuals who
describe changes in physical activity or social circumstances. It may be more difficult to be
sure in older patients when a history of nutritional intake may be unreliable.
Psychiatric illness anorexia nervosa,bulimia and affective disorders.
Alcoholic patients lose weight as a consequence of self-neglect and poor dietary intake.
Systemic diseases
A. Chronic infections including tuberculosis , HIV, recurrent urinary or chest infections, and a
range of parasitic and protozoan infections should be considered.
B. Weight loss is a late feature of disseminated malignancy (carcinoma, lymphoma or other
haematological disorders).
C. Gastrointestinal disease Almost any disease of the gastrointestinal tract can cause weight
loss.
Dysphagia and gastric outflow obstruction cause defective dietary intake.
Malignancy at any site may cause weight loss by mechanical obstruction, anorexia
or cytokine-mediated systemic effects.
Malabsorption from pancreatic diseases or small bowel causes may lead to profound
weight loss with specific nutritional deficiencies.
Inflammatory diseases such as Crohn's disease or ulcerative colitis cause anorexia,
fear of eating and loss of protein, blood and nutrients from the gut.
D. Specific diseases of any major organ system.
Diagnosis:
When weight loss is due to serious organic disease a careful history, physical
examination , laboratory tests (biochemical or haematological) and relevant imaging will usually
define other features that lead to a specific diagnosis.
Diarrhea
The bowel frequency of the normal population ranges from three bowel movements per day to
one bowel action every third day, and a normal stool consistency ranges from porridge-like to hard
and pellety.
The term applied to: increased stool frequency and loose or watery stools.
Gastroenterologists define diarrhoea as the passage of more than 200 g of stool daily, and
measurement of stool volume is helpful.
The most severe symptom in many patients is urgency of defecation, and faecal incontinence is a
common event in acute and chronic diarrhoeal illnesses.
Acute diarrhea:
This is extremely common and usually due to faecal-oral transmission of
bacteria, their toxins, viruses or parasites. Infective diarrhoea is usually short-lived and patients
who present with a history of diarrhoea lasting more than 10 days rarely have an infective cause.
5
A variety of drugs, including antibiotics, cytotoxic drugs, proton pump inhibitors and NSAIDs, may
be responsible for acute diarrhoea.
Chronic or relapsing diarrhea:
The most common cause is irritable bowel syndrome ,which can present with increased frequency
of defecation and loose, watery or pellety stools. Diarrhoea rarely occurs at night and is most
severe before and after breakfast. At other times the patient is constipated and there are other
characteristic symptoms of irritable bowel syndrome. The stool often contains mucus but never
blood, and 24-hour stool volume is less than 200 g. Chronic diarrhoea can be disease of the colon
or small bowel, or malabsorption. Clinical presentation, examination of the stool, routine blood
tests and imaging reveal a diagnosis in many cases.
A series of negative investigations usually implies irritable bowel syndrome but some patients
clearly have organic disease and need more extensive investigations.
Colonic diarrhea:
Clinical features: Blood and mucus in stool. Cramping lower abdominal pain.
Some causes:Inflammatory bowel disease. Neoplasia. Ischaemia. Irritable bowel syndrome.
Investigations: Colonoscopy with biopsies.
Malabsorption:
Clinical features: Steatorrhoea. Undigested food in the stool. Weight loss and nutritional
disturbances.
Some causes:
Pancreatic (Chronic pancreatitis, cancer of pancreas, cystic fibrosis).
Enteropathy (Coeliac disease, tropical sprue, lymphoma, lymphangiectasia)
Obstructive Jaundice..
Investigations: (US, CT scan, MRCP, small bowel biopsy, barium follow through).
Small bowel diarrhea:
Clinical features: Large volume watery stool, abdominal bloating, cramping mid-abdominal pain.
Some causes: VIPoma. Drug induced (NSAIDs, Aminosalicylates, SSRIs).
Investigations: Stool volume, Gut hormone profile, Barium follow through.
ABDOMINAL PAIN
There are four types of abdominal pain:
1. Visceral. Gut organs are insensitive to stimuli such as burning and cutting but are sensitive
to distension, contraction, torsion and stretching. Pain from unpaired structures is usually
but not always felt in the midline.

6
2. Parietal. The parietal peritoneum is innervated by somatic nerves, and its involvement by
disease processes, e.g. inflammation, infection or neoplasia, causes sharp, well-localised
and lateralised pain.
3. Referred pain. (For example, gallbladder pain is referred to the back or shoulder tip.)
4. Psychogenic. Cultural, emotional and psychosocial factors influence everyone's
experience of pain. In some patients, no organic cause can be found despite investigation,
and psychogenic causes ( e. g. depression) may be responsible.
CAUSES OF ACUTE ABDOMINAL PAIN ('SURGICAL'):
Inflammation:
Appendicitis,
Diverticulitis,
Cholecystitis,
Pelvic
inflammatory
disease
Pancreatitis, Pyelonephritis, Intra-abdominal abscess.
Perforation/rupture: Peptic ulcer, Diverticular disease, Ovarian cyst, Aortic aneurysm.
Obstruction: Intestinal obstruction, Biliary colic, Ureteric colic.
Other (rare)
'EXTRAINTESTINAL' CAUSES OF CHRONIC OR RECURRENT ABDOMINAL PAIN
Retroperitoneal:, Aortic aneurysm, Malignancy, Lymphadenopathy, Abscess.
Psychogenic: Depression, Anxiety, Hypochondriasis, Somatisation
Locomotor: Vertebral compression, Abdominal muscle strain.
Metabolic/endocrine: Diabetes mellitus, Addison's disease, Acute intermittent porphyria,
Hypercalcaemia.
Haematological: Sickle-cell disease, Haemolytic disorders
Neurological: Spinal cord lesions, Tabes dorsalis, Radiculopathy
IMPORTANT FACTORS IN THE ASSESSMENT OF ABDOMINAL PAIN
1. Duration 2. Site and radiation 3. Severity 4. Precipitating and relieving factors (food, drugs,
alcohol, posture, movement, defaecation) 5.Nature (colicky, constant, sharp or dull, wakes
patient at night) 6. Pattern (intermittent or continuous) 7. Associated features (vomiting,
dyspepsia, altered bowel habit). The initial choice of investigations will obviously depend on
the clinical features elicited during the history and examination:
o Epigastric pain, dyspepsia and relationship to food suggest gastroduodenal or biliary
disease. Endoscopy and ultrasound are indicated.
o Altered bowel habit, rectal bleeding or features of obstruction suggest colonic disease.
Barium enema and sigmoidoscopy, or colonoscopy are indicated.
o Pain provoked by food in a patient with widespread atherosclerosis may indicate
mesenteric ischaemia. Mesenteric angiography may be necessary.

7
o Persistent symptoms require exclusion of colonic or small bowel disease. However, young
patients with pain relieved by defecation, bloating and alternating bowel habit are likely to
have irritable bowel syndrome . Simple investigations (blood tests and sigmoidoscopy) may
be sufficient.
o Upper abdominal pain radiating to the back, a history of alcohol misuse, weight loss and
diarrhoea suggest chronic pancreatitis or pancreatic cancer. Ultrasound, CT and pancreatic
function tests are required.
o Recurrent attacks of pain in the loins or radiating to the flanks with urinary symptoms should
prompt investigation for renal or ureteric stones by ultrasound and intravenous urography.
o A past history of psychiatric disturbance, repeated negative investigations or vague
symptoms which do not fit any particular disease or organ pattern may point to a
psychological origin for the patient's pain . Careful review of case notes and previous
investigations, along with open and honest discussion with the patient, may reduce the
need for further cycles of unnecessary and invasive tests. Care must always be taken,
however, not to miss rare pathology or atypical presentations of common diseases.
CONSTANT ABDOMINAL PAIN Patients with chronic pain which is constant or nearly always
present will usually have features to suggest the underlying diagnosis, e.g. malignancy (gastric,
pancreatic, colonic, hepatic metastases), chronic pancreatitis or intra-abdominal abscess. In a
minority no cause will be found despite thorough investigation, leading to the diagnosis of 'chronic
functional abdominal pain'. In these patients a psychological cause is highly likely, and the most
important tasks are to provide symptom control, if not relief, and to minimise the effects of the pain
on social, personal and occupational life. Patients are best managed in specialised pain clinics
where, in addition to psychological support, appropriate use of drugs including amitriptyline,
gabapentin, ketamine and opioids may be necessary