
1
Third stage
Medicine
Lec-7
د
.
اسماعيل
1/1/2014
Worm infestation
1- Nematodes or roundworms:
Intestinal human nematodes: Ancylostoma duodenale,
Necator americanus, Strongyloides stercoralis, Ascaris lumbricoides, Enterobius
vermicularis, Trichuris trichiura
Tissue-dwelling human nematodes: Wuchereria bancrofti, Brugia malayi, Loa loa, etc.
2- Trematodes or flukes
: e. g.Schistosoma haematobium, S. mansoni, S.
japonicum,
3- Cestodes or tapeworm
: Intestinal tapeworms: Taenia saginata, T. solium,
Diphyllobothrium latum, Hymenolepis nana.Tissue-dwelling cysts or worms: Taenia solium,
Echinococcu
s
Intestinal human nematodes
Diseases are caused by adult nematodes living in the human gut.
There are two types:
• The hookworms, which have a soil stage in which they develop into larvae that then
penetrate the host
• a group of nematodes which survive in the soil merely as eggs that have to be ingested for
their life
The hookworms Ancylostomiasis
ANCYLOSTOMIASIS (HOOKWORM)
Ancylostomiasis is caused by parasitisation of the small intestine with Ancylostoma
duodenale or Necator americanus.
It is one of the main causes of anaemia in the tropics. In the early stages of infection
eosinophilia is common. The adult hookworm is 1 cm long and lives in the duodenum and
upper jejunum.

2
Eggs are passed in the faeces. In warm, moist, shady soil the larvae develop into the
filariform infective stage; they then penetrate human skin and are carried to the lungs . After
entering the alveoli they ascend the bronchi, are swallowed and mature in the small intestine,
reaching maturity 4-7 weeks after infection.
Hookworm infection is widespread in the tropics and subtropics.
A. duodenale is endemic in the Far East and Mediterranean coastal regions and is also
present in Africa, while N. americanus is endemic in West, East and Central Africa and
Central and South America, as well as in the Far East.
MORPHOLOGY AND LIFE CYCLE
The larvae may cause allergic inflammation at the site of entry through the skin. When
infection is heavy, the passage through the lungs may cause pulmonary eosinophilia. The
worms attach themselves to the mucosa of the small intestine by their buccal capsule and
withdraw blood. The mean daily loss of blood from one A. duodenale is 0.15 ml and from N.
americanus 0.03 ml. The degree of iron and protein deficiency which develops depends not
only on the load of worms but also on the nutrition of the patient and especially on the iron
stores. In a light infection there may be no anaemia.
Clinical features: Dermatitis, usually on the feet (ground itch), may be experienced at the
time of infection. The passage of the larvae through the lungs in a heavy infection causes a
paroxysmal cough with blood-stained sputum, associated with patchy pulmonary
consolidation. When the worms have reached the small intestine, vomiting and epigastric
pain resembling peptic ulcer disease may occur. Sometimes frequent loose stools are passed.

3
Iron deficiency anaemia, protein-losing enteropathy and hypoproteinaemia may develop in
the undernourished. High-output cardiac failure may result from the chronic iron deficiency
anaemia. The mental and physical development of children may be retarded. A well-
nourished person with a light infection may be asymptomatic.
Investigations
There is eosinophilia. The characteristic ovum can be recognised in the stool. If hookworms
are present in numbers sufficient to cause anaemia, faecal occult blood testing will be
positive and many ova will be present.
Management
single-dose treatment albendazole (400 mg) is the best choice but Mebendazole 100 mg 12-
hourly for 3 days is preferred. Anaemia associated with hookworm infection responds well
to oral iron even when severe; blood transfusion is rarely required and should only be used
with great care in very severely anaemic patients (< 40 g/l). . The management of anaemic
heart disease is best accomplished by treatment with antihelmintics and iron.
ASCARIS LUMBRICOIDES (ROUNDWORM)
This pale yellow nematode is 20-35 cm long. Humans are infected by eating food
contaminated with mature ova. Ascaris larvae hatch in the duodenum, migrate through the
lungs, ascend the bronchial tree, are swallowed and mature in the small intestine. This tissue
migration can provoke both local and general hypersensitivity reactions with pneumonitis,
eosinophilic granulomas, bronchial asthma and urticaria.
Normally, the adult worms are located in the small intestine. In unusual circumstances, such
as fever, irritation due to drugs, anaesthesia, and bowel manipulation during surgery, the
worms may migrate to ectopic sites where they may give rise to severe disease.
Clinical features
Intestinal ascariasis causes symptoms ranging from occasional vague abdominal pain
through to malnutrition. The large size of the adult worm and its tendency to aggregate and
migrate can result in severe obstructive complications. In endemic areas ascariasis causes up
to 35% of all intestinal obstructions, most commonly in the terminal ileum. Obstruction can
be complicated further by intussusception, volvulus, haemorrhagic infarction and
perforation. Other complications include blockage of the bile or pancreatic duct and
obstruction of the appendix by adult worms.

4
Investigations
The diagnosis is made microscopically by finding ova in the faeces. Adult worms are
frequently expelled rectally or orally. Occasionally, the worms are demonstrated
radiographically by a barium examination. There is eosinophilia.
Management
Mebendazole 100 mg 12-hourly for 3 days. Albendazole 400 mg or piperazine 4 g or
ivermectin (150–200 μg/kg) as a single dose is effective for intestinal ascariasis. Patients
should be warned that they may expel numerous whole, large worms. Obstruction due to
ascariasis should be treated with nasogastric suction, piperazine and intravenous fluids.
Prevention
Community chemotherapy programmes have been used to reduce Ascaris infection. The
whole community can be treated every 3 months and over several years. Alternatively,
schoolchildren can be targeted; treating them lowers the prevalence of ascariasis in the whole
community.
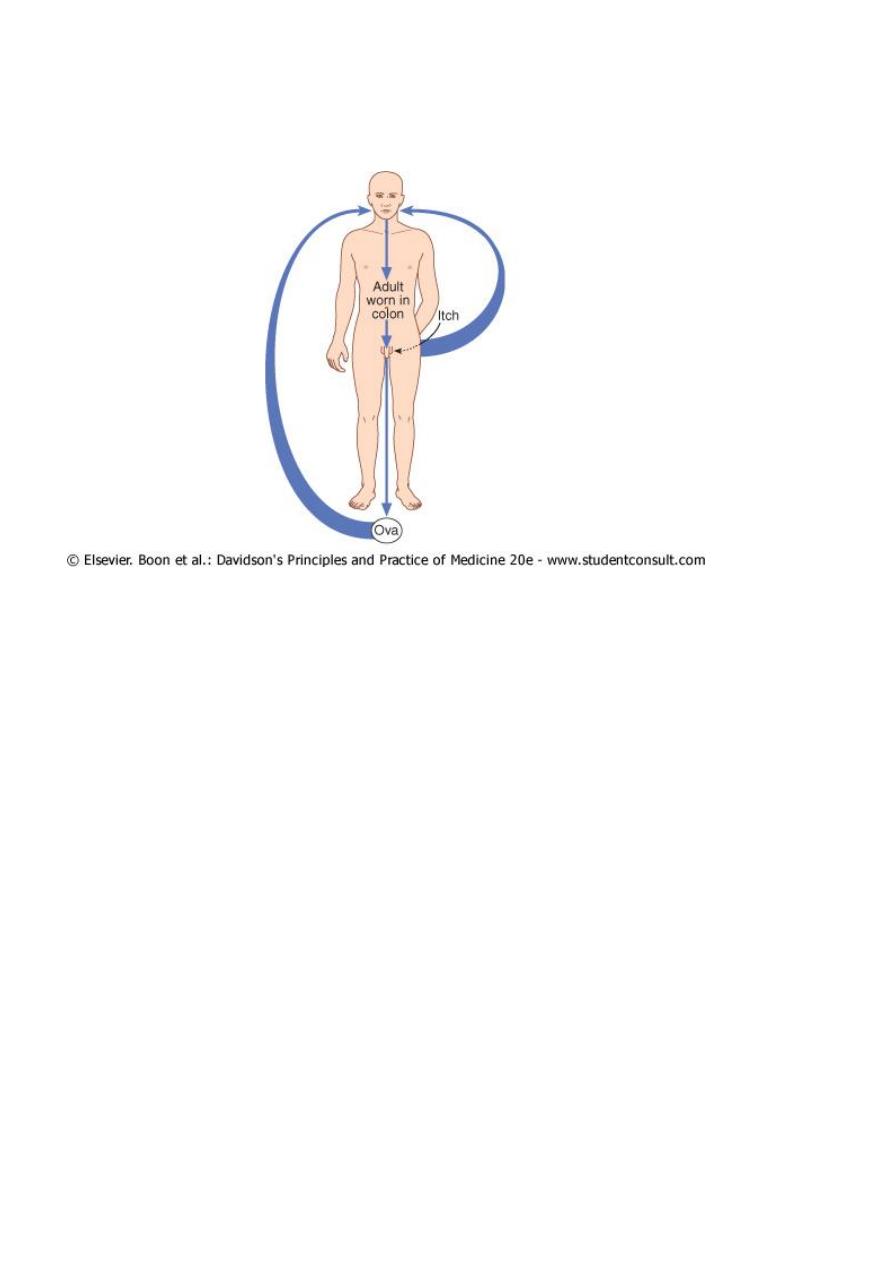
Enterobiasis
Enterobiasis is a disease caused by Enterobius vermicularis infestation.
Children are more often involved than adults. It occurs in groups such as families living
together, and in army camps.
This helminth is common throughout the world. It affects children especially. After the ova
are swallowed, development takes place in the small intestine, but the adult worms are found
chiefly in the colon. The male is approximately 5 mm long with a diameter of 0.1 to 0.2 mm.
The female is approximately 13 mm long.
Clinical features
The gravid female worm lays ova around the anus, causing intense itching, especially at
night. The ova are often carried to the mouth on the fingers and so reinfection takes place. In
females the genitalia may be involved. The adult worms may be seen moving on the buttocks
or in the stool.
5
Enterobius vermicularis
Investigations
Ova are detected by applying the adhesive surface of cellophane tape to the perianal skin in
the morning. This is then examined on a glass slide under the microscope. A perianal swab,
moistened with saline, is an alternative method for diagnosis.
Management
A single dose of mebendazole 100 mg, albendazole 400 mg or piperazine 4 g is given and
may be repeated after 2 weeks to control auto-reinfection. Where infection constantly recurs
in a family, each member should be treated as above. During this period all nightclothes and
bed linen are laundered. Fingernails must be kept short and hands washed carefully before
meals. Subsequent therapy is reserved for those family members who develop recurrent
infection.
Tapeworm Infestation (Cestoda)
Cestodes are ribbon-shaped worms which inhabit the intestinal tract.
They have no alimentary system and absorb nutrients through the tegumental surface. The
anterior end, or scolex, has suckers for attaching to the host. From the scolex arises a series

6
of progressively developing segments, the proglottides, which when shed may continue to
show active movements. Cross-fertilisation takes place between segments.
Ova, present in large numbers in mature proglottides, remain viable for weeks and during
this period they may be consumed by the intermediate host. Larvae liberated from the
ingested ova pass into the tissues.
Humans acquire tapeworm by eating undercooked beef infected with Cysticercus bovis, the
larval stage of Taenia saginata (beef tapeworm), undercooked pork containing the larval
stage of T. solium (pork tapeworm), or undercooked freshwater fish containing larvae of
Diphyllobothrium latum (fish tapeworm). Usually only one adult tapeworm is present in the
gut but up to ten have been reported.
CESTODA (TAPEWORMS) TYPES
The most important cestoda that infest humans are:
1. Taenia saginata
2. Taenia solium
3. Echinococcus
4. Diphyllobothrium (fish tapeworm)
5. Hymenolepis
1. Primary host:
Humans are the primary host in all (adult live in intestine) except Echinococcus, in which
the human is intermediate host (larva within tissues) and dogs are primary host (final host).
2. Intermediate Hosts:
Cattle: T. Saginata, Pigs: T. Solium, Fishs: Diphyllobothrium, Human, sheep and others:
Echinococcus.
3. Rarely the human becomes intermediate host for T. solium if he/she ingest eggs
accidently.
1. The primary host (human or others) passes the mature segments containing ova which
remain viable for Ws in the soil and may be consumed by intermediate hosts (cattle,
sheep, pig, fishes) and change to larva in their tissues.
2. When humans are the primary host, the adult cestode is limited to the intestinal
tract. When humans are the intermediate hosts, the larvae are within the tissues,
migrating through the different organ systems.

7
T. saginata
Most worms are solitary (AL- DODDA AL-WAHEDA), and worms may live 30 years and
may reach 20 meters in length
Taenia saginata
Infection with T. saginata occurs in all parts of the world. The adult worm may be several
metres long and produces little or no intestinal upset in human beings, but knowledge of its
presence, by noting segments in the faeces or on underclothing, may distress the patient. Ova
may be found in the stool. The ova of T. saginata and T. solium are indistinguishable
microscopically.
Praziquantel is the drug of choice, and prevention depends on efficient meat inspection and
the thorough cooking of beef. Niclosamide is an alternative .
T. Ova
The ova of T. saginata and T. solium are indistinguishable microscopically.
T. Saginata
The adult worm may be several meters long
Cattles intermediate host for T. saginata
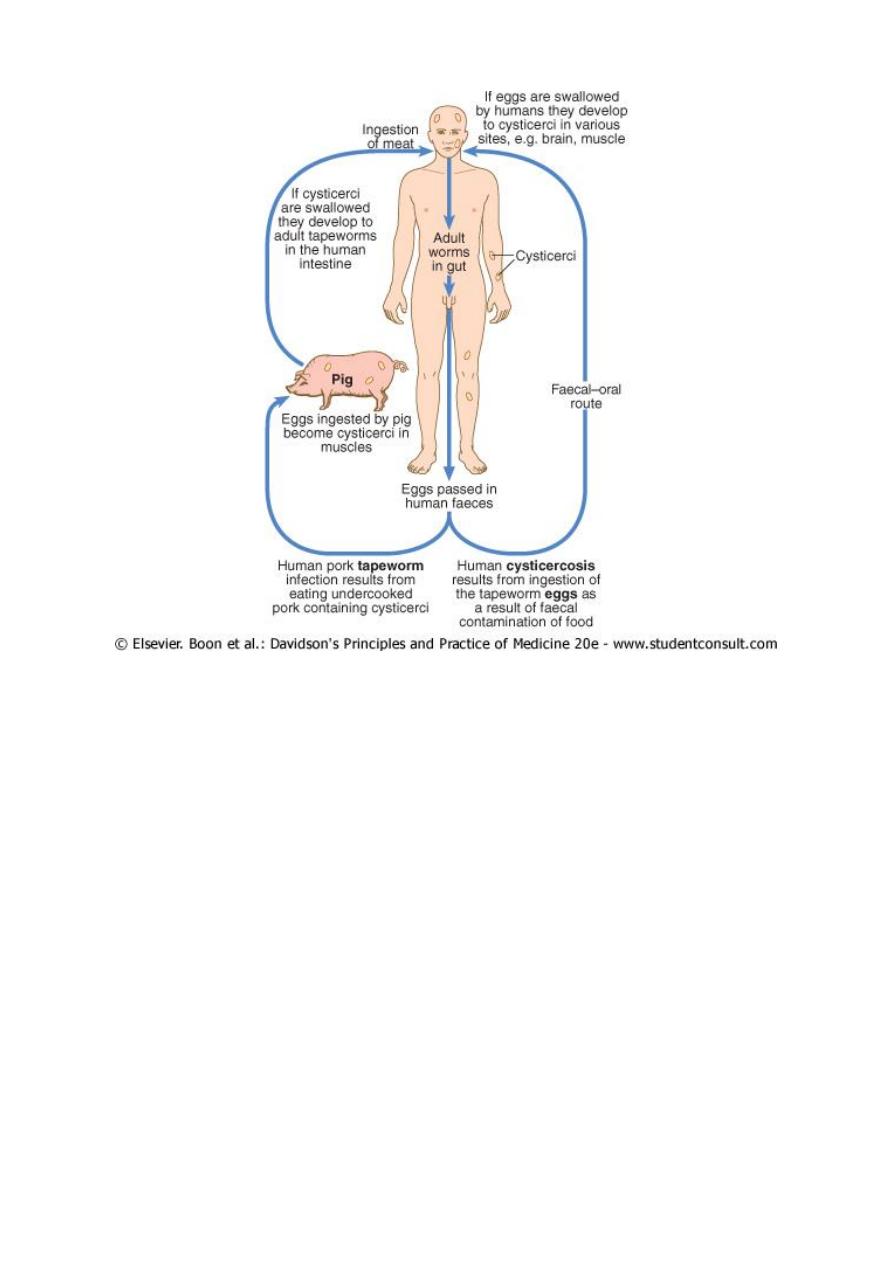
Taenia solium
T. solium, the pork tapeworm, is common in central Europe, South Africa, South America
and parts of Asia. It is not as large as T. saginata. The adult worm is found only in humans
following the eating of undercooked pork containing cysticerci.
CYSTICERCOSIS Human cysticercosis is acquired by ingesting tapeworm ova, either by
ingesting ova from contaminated fingers or by eating contaminated food. The larvae are
liberated from eggs in the stomach, penetrate the intestinal mucosa and are carried to many
parts of the body where they develop and form cysticerci, 0.5-1 cm cysts that contain the
head of a young worm. They do not grow further or migrate. Common locations are the
subcutaneous tissue, skeletal muscles and brain.
T. Solium scolex with hooks and suckers
Pigs intermediate host for T.solium
8
Clinical features
When superficially placed, cysts can be palpated under the skin or mucosa as pea-like ovoid
bodies. Here they cause few or no symptoms, and will eventually die and become calcified.
Heavy brain infections, especially in children, may cause features of encephalitis. More
commonly, however, cerebral signs do not occur until the larvae die, 5-20 years later.
Epilepsy, personality changes, staggering gait or signs of internal hydrocephalus are the most
common features.
Investigations
Calcified cysts in muscles can be recognised radiologically. In the brain, however, less
calcification takes place and larvae are only occasionally demonstrated radiologically;
usually CT or MRI will show them. Epileptic fits starting in adult life should suggest the
possibility of cysticercosis if the patient has lived in or travelled to an endemic area. The
subcutaneous tissue should be palpated and any nodule excised for histology. Radiological
examination of the skeletal muscles may be helpful. Antibody detection by fluorescent
antibody test, ELISA or immunoblotting is available for serodiagnosis.
9
Management and prevention
Niclosamide, followed by a mild laxative (after 1-2 hours) to prevent retrograde intestinal
autoinfection, is useful only for the intestinal infection. Praziquantel improves the prognosis
of cerebral cysticercosis; the dose is 50 mg/kg in three divided doses daily for 10 days.
Albendazole, 15 mg/kg daily for a minimum of 8 days, has now become the drug of choice
for parenchymal neurocysticercosis. Prednisolone, 10 mg 8-hourly, is also given for 14 days,
starting 1 day before the albendazole or praziquantel. In addition, anti-epileptic drugs should
be given until the reaction in the brain has subsided. Operative intervention is indicated for
hydrocephalus. Studies from India and Peru suggest that most small solitary cerebral cysts
will resolve without treatment.
Cooking pork well will prevent infection with T. solium. Cysticercosis is avoided if food is
not contaminated by ova or segments. Great care must be taken by nurses and other adults
while attending a patient harbouring an adult worm.
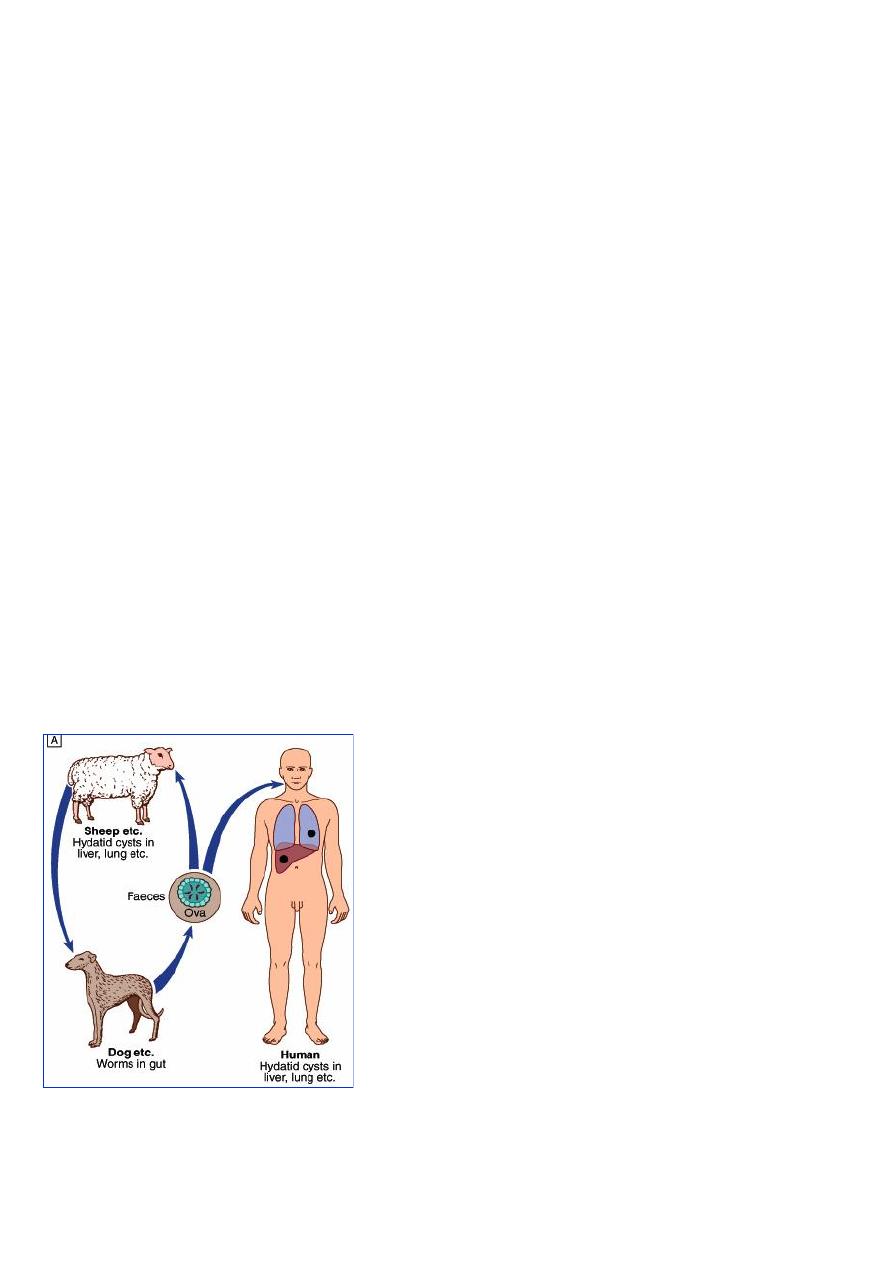
Echinococcus infestations
The disease is common in the Middle East, North and East Africa, Australia and Argentina.
By handling a dog or drinking contaminated water, humans may ingest eggs . The embryo is
liberated from the ovum in the small intestine and gains access to the blood stream and thus
to the liver.
11
CLINICAL MANIFESTATION
A hydatid cyst is typically acquired in childhood and it may, after growing for some years,
cause pressure symptoms. These vary, depending on the organ or tissue involved. In nearly
75% of patients with hydatid disease the right lobe of the liver is invaded and contains a
single cyst. In others a cyst may be found in lung, bone, brain or elsewhere.
1. The patient remains asymptomatic until the cysts cause a mass effect on the organ, which
can be 5-20 years after the initial infestation.
2. These cysts do not metastasize, but they may be disseminated by accidental spillage.
3.Most patients have single organ
involvement and most will have a solitary cyst .
Hepatic form:
1. palpable R hypochondrial mass and jaundice can occur.
2. Rupture of liver hydatid cyst into peritoneal cavity may cause anaphylactic shock.
Pulmonary: 25%
1. Cystic rupture may result in symptoms of cough, chest pain, and hemoptysis.
2. Crape-like material may be coughed.
3. Rarely pneumothorax, with or without pleural effusion and anaphylaxis can occur
following cyst rupture.
Other organs: Brain, Kidney, Bone, Adrenal glands.
DIAGNOSIS
The diagnosis depends on the clinical, radiological and ultrasound findings in a patient who
has lived in close contact with dogs in an endemic area. Complement fixation and ELISA are
positive in 70-90% of patients.
MANAGEMENT
Hydatid cysts should be excised wherever possible. Great care is taken to avoid spillage and
cavities are sterilised with 0.5% silver nitrate or 2.7% sodium chloride. Albendazole (400 mg
12-hourly for 3 months) is used for inoperable disease, and to reduce the infectivity of cysts
pre-operatively. Praziquantel 20 mg/kg 12-hourly for 14 days kills protoscolices
perioperatively.

11
Prevention
Prevention is difficult in situations where there is a close association with dogs and sheep.
Personal hygiene, satisfactory disposal of carcasses, meat inspection and deworming of dogs
can greatly reduce the prevalence of disease.
Diphyllobothriasis
Is an infection that occurs from eating raw or undercooked fish infected with
Diphyllobothrium species.
Diphyllobothrium organisms are present in lakes, rivers, and deltas of freshwaters. Eskimos
in western Alaska and the West Coast of the United States are frequent hosts. Also in finland
The cestode is not invasive, but it does absorb a large amount of vitamin B-12 and
interferes with vitamin B-12 absorption from the ileum, producing a megaloblastic
anemia that resembles pernicious anemia (clinically and hematologically). Patients may
complain of neurologic symptoms resembling pernicious anemia (eg, paresthesias, difficulty
with balance, dementia or confusional states).