1
Third stage
Medicine
Lec-3
د
.
جاسم
محمد
1/1/2014
FEVER
DEFINITION OF FEVER
Fever is an elevation of body temperature that exceeds the normal daily variation, in
conjunction with an increase in hypothalamic set point
NORMAL BODY TEMPERATURE
Maximum normal oral temperature
At 6 AM : 37.2
At 4 PM : 37.7
Temperature Classification
Hypothermia
<35.0 °C
Normal
36.5–37.5 °C
Fever
>37.5–38.3 °C
Hyperthermia
>37.5–38.3 °C
Hyperpyrexia
>40.0–41.5 °C
Note: The difference between fever and hyperthermia is the mechanism
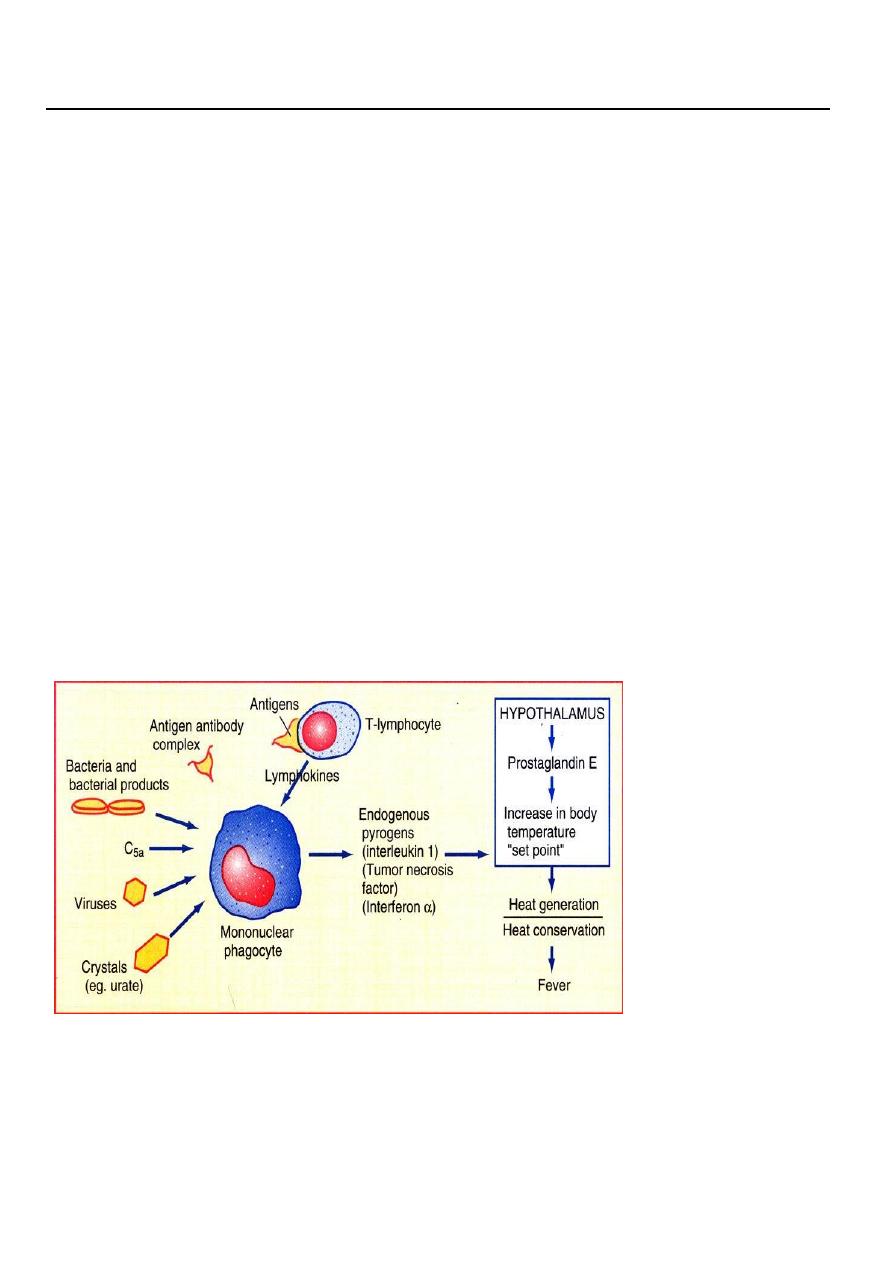
PATHOGENESIS OF FEVER
CAUSES OF FEVER
Infection
Tissue injury - infarction, trauma
Malignancy
Drugs

2
Immune-mediated disorders
Other inflammatory disorders
Endocrine disorders
Factitious of self-induced fever
Infections presenting as fever
without localizing signs or symptoms
Viral
Rhinovirus, adenovirus, parainfluenza
Enterovirus Influenza
Bacterial
Staphylococcus aureus
Salmonella thyphi, S. parathyphi
Streptococci
Post animal exposure
Coxiella burneti (Q fever)
Leptospira interrogans
Brucella species
Granulomatous infection Mycobacterium tuberculosis
Histoplasma capsulatum
Infections with Fever and Lymphadenomegaly
(generalized)
Viral
Measles,Rubella
Bacterial
Brucellosis,Tuberculosis,Syphilis
(regional)
Pyogenic infection
Sta. aureus, Stre.
Tuberculosis
Scrofula (tbc. Cervical adenitis)
Inguinal lymphadenopathy Syphilis, herpes
Plague
Yersinia pestis
DISCOMFORT DUE TO FEVER
For each 1 °C elevation of body temperature:
Metabolic rate increase 10-15%
Insensible water loss increase 300-500ml/m2/day
O2 consumption increase 13%
Heart rate increase 10-15/min
HYPERTHERMIA
Heat production exceeds heat loss, and the temperature exceeds the individuals set point.
Heat stroke ,drugs
Hyperpyrexia
Hyperpyrexia is a fever with an extreme elevation of body temperature greater than or
equal to 41.5 °C . Such a high temperature is considered a medical emergency as it may
3
indicate a serious underlying condition or lead to significant side effects. The most
common cause is an intracranial hemorrhage. Other possible causes include
sepsis, Kawasaki syndrome, neuroleptic malignant syndrome, drug effects, serotonin
syndrome, and thyroid storm and infections like viral.
TREATMENT OF FEVER
Most fevers are associated with self-limited infections, most commonly of viral origin.
Treatment of underlying cause
Treatment Strategies
Acetaminophen is generally a first-line antipyretic due to being well tolerated with
minimal side effects.
Pediatric dose: 10-15mg/kg q4-6h (2400mg/day); adult: 650mg q 4 h(4000mg)
Can be hepatotoxic in high doses; can upset stomach
Clinical Pearls
Don’t give aspirin to children under 18 years (Reye’s Syndrome)
Try water sponge bath; remove blankets and heavy clothing; keep room at
comfortable temp
DRUG FEVER
PATHOGENEGIS
Contamination of the drug with a pyrogen or microorganism
Pharmacologic action of the drug itself
Allergic (hypersensitivity) reaction to the drug
Onset and duration:
Onset: 1-3 weeks after the start of therapy
Duration: remits 2-3 days after therapy is stoped
Fever out of proportion to clinical picture
Associated findings:
Rigor (43%), Myalgia (25%), Rash (18%), Headache (18%),
Leukocytosis (22%), Eosinophilia (22%), Serum sickness,Proteinuria Abnormal liver
function test
APPROACH TO THE PATIENT WITH FEVER
ACUTE FEBRILE ILLNESS
History:
Personal History:
o Age
o Occupation
o Place of origin,Travel History
o Habits
Sexual Practices
4
Injection Drug Abuse
Excessive Alcohol Use
Consumption of Unpasteurized Dairy Products
Underlying Diseases:
o Splenectomy
o Surgical Implantation of Prosthesis
o Immunodeficiency
o Chronic Diseases:
Cirrhosis
Chronic Heart Diseases
Chronic Lung Diseases
Drug History:
o Antipyretics
o Immunosuppressants
o Antibiotics
Family History:
o TB in the Family
o Recent Infection in the Family
Associated Symptoms:
o Shaking chills
o Ear pain,Ear drainage,Hearing loss
o Visual and Eye Symptoms
o Sore Throat
o Chest and Pulmonary Symptoms
o Abdominal Symptoms
o Back pain, Joint or Skeletal pain
PATTERN OF FEVER
Continuous fever: Temperature remains above normal throughout the day and does
not fluctuate more than 1 °C in 24 hours, typhoid.
Intermittent fever: The temperature elevation is present only for a certain period,
later cycling back to normal, e.g. malaria,
Remittent fever: Temperature remains above normal throughout the day and
fluctuates more than 1 °C in 24 hours, e.g., infective endocarditis.
Pel-Ebstein fever: A specific kind of fever associated with Hodgkin's lymphoma, being
high for one week and low for the next week and so on
Physical Examination:
Vital Signs
Neurological Exam.
Skin Lesions,Mucous Membrane
Eyes
ENT
Lymphadenopathy
5
Lungs and Heart
Abdominal Region (Hepatomegaly,Splenomegaly)
Musculoskeletal
LABORATORY STUDY:
IN PATIENT WITH FEBRILE ILLNESS
Assess the extent and severity of the inflammatory response to infection
Determine the site(s) and complications of organ involvement by the process
Determine the etiology of the infectious disease
FUO (FEVER OF UNKNOWN ORIGIN)
Classic FUO
Fever of 38.3 C or higher on several occasions
Fever of more than 3 weeks duration
Diagnosis uncertain, despite appropriate investigations after at least 3 outpatient
visits or at least 3 days in hospital
Nosocomial FUO
Fever of 38.3 or higher on several occasions
Infection was not manifest or incubating on admission
Failure to reach a diagnosis despite 3 days of appropriate investigation in hospitalized
patient
Neutropenic FUO
Fever of 38.3 or higher on several occasions
Neutrophil count is <500/mm3 or is expected to fall to that level in 1 to 2 days
Failure to reach a diagnosis despite 3 days of appropriate investigation
HIV-Associated FUO
Fever of 38.3 or higher on several occasions
Fever of more than 3 weeks for outpatients or more than 3 days for hospitalized
patients with HIV infection
Failure to reach a diagnosis despite 3days of appropriate investigation
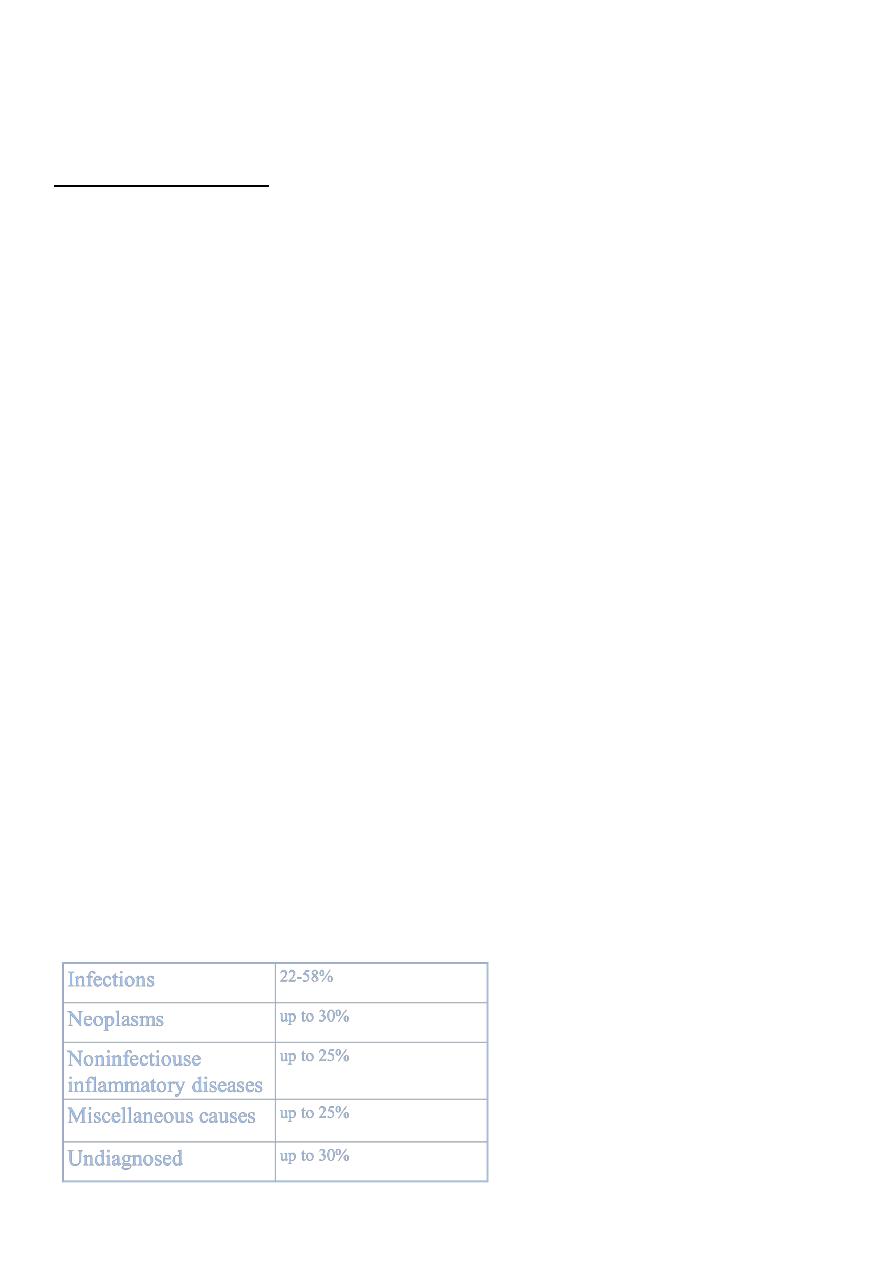
Causes of classical FUO
6
Infections commonly associated with FUO
Localized pyogenic infections
Intravascular infections
Systemic bacterial infections (Tuberculosis, Brucellosis,…)
Fungal infections
Viral infections
Parasitic infections
Malignancies commonly associated with FUO
Hodgkin’s disease
Non-hodgkin’s lymphoma
Leukemia
Renal cell carcinoma
Hepatoma
Colon carcinoma
Atrial myxoma
Noninfectious inflammatory diseases with FUO
Collagen vascular/ hypersensitivity diseases
o Lupus
o Still’s disease
o Temporal arteritis (Giant cell arteritis)
Granulomatouse diseases
o Crohn’s disease
o Sarcoidosis
o Idiopathic granulomatouse disease
Miscellaneous causes of FUO
Drug fever
Factitious fever
FMF
Recurrent pulmonary emboli
Subacute thyroiditis
FACTITIOUS FEVER
Diagnosis should be considered in any FUO, especially in:
Young women
Persons with medical training
If the patients clinically well
Disparity between temperature and pulse
Absence of the normal diurnal pattern
7
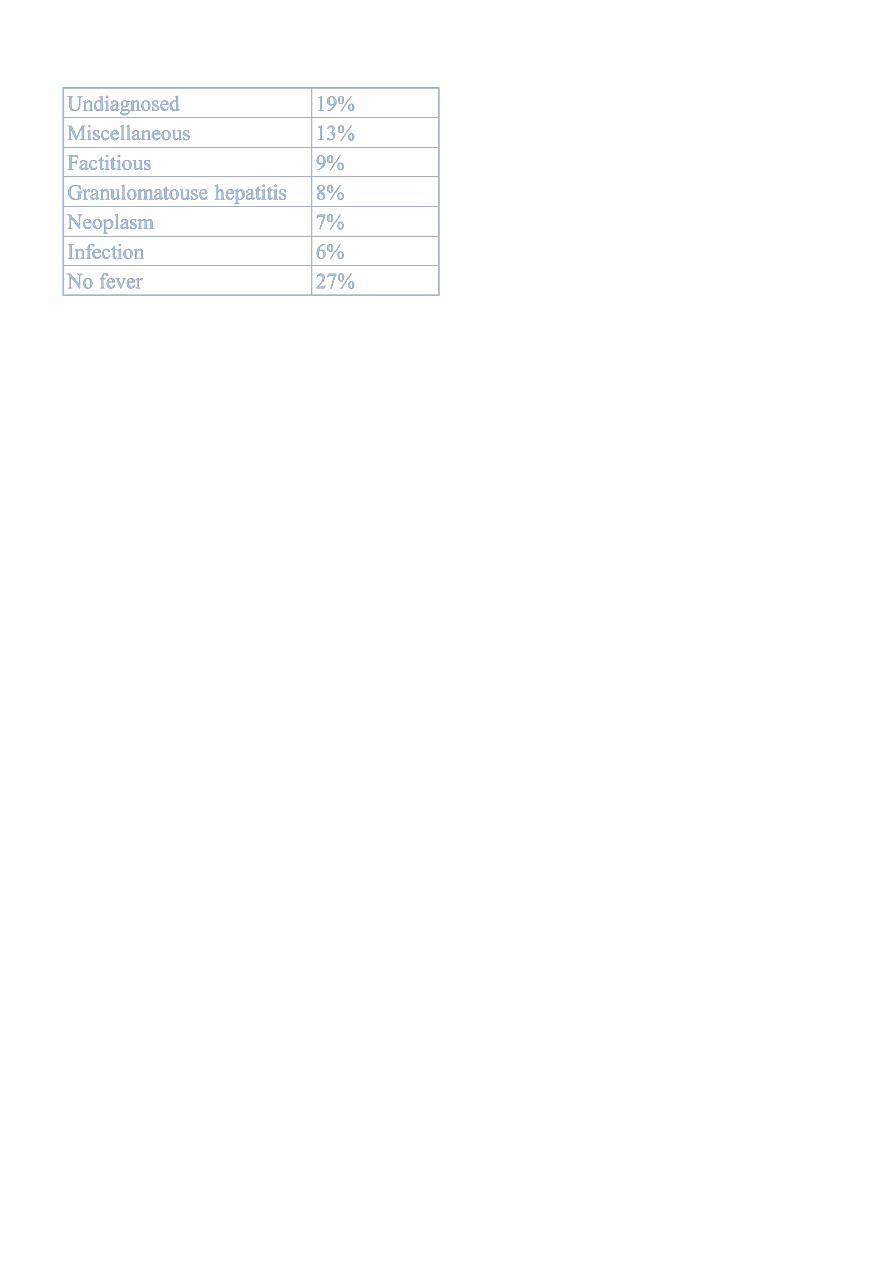
Causes of FUO lasting > 6 month
Approach to FUO
Determine whether the patient has a true FUO
Workup of true FUO:
o Careful history
Serial follow-up histories
o Careful physical examination
Physical examination should be repeated
Laboratory examination:
CBC(diff)
PBS
ESR
U/A
S/E
Culture of blood, urine,…
Skin test
Serology
ANA
Imaging:
CXR
Ultrasonography
Radiographic contrast study
Radioneuclide scan
CT or MRI
Invasive Procedures:
Biopsies:
Bone marrow
Skin lesion
Lymph node
Liver
Temporal artery