1
Third stage
Medicine
Lec-3
د
.
عبدالحق
1/1/2014
HYPOKALEMIA
3.5-5.2 mmol/L)
)
Potassium
Only 2% is found outside the cells and of this only 0.4% of your K+ is found in the plasma.
Thus as you can see serum K+ measurements have limitations in reflecting TOTAL body K+
stores.
A 1 mEq/L drop in K+ reflects between 200-400 mEq total body K+ deficit
3.5-5.2 mmol/L)
)
Pottasium
*Major intracellular cation
*ICF conc. = 150- 160 mEq/ L
*Resting membrane potential
*Regulates fluid, ion balance inside cell
*Contribute to pH balance
Pathophysiology of Hypokalemia
Decrease in K+ causes decreased excitability of cells, therefore cells are less responsive to
normal stimuli
Hypokalemia can only occur for four reasons:
Decreased intake
Shift into cells
Extra-renal losses..GIT
Renal losses
*Spurious - i.e. K+ is falsely low..cases of Hyperleukocytosis
Decreased intake normal intake 40-120 daily.
Shift into cells:
1. Alkalosis
2.Insulin
3. Beta adrenergic drugs or epinephrine
there will be shift
hypoinsulinemia
: because of
mechanism of Hypokalemia
–
Ketoacidosis
*
(polyuria)
lost in urine
, which is
+
replaces K
+
to ECC, H
+
of K
Examples of increased potassium entry into cells
Hypokalemic periodic paralysis:
typically oriental men with thyrotoxicosis; ? abnormal Ca++ channel; ? Increased Na/K atp
ase activity.
2
Increased RBC uptake:
e.g. after treatment with B12, folate.
Gastrointestinal losses of potassium
Gastric juice contains 5 – 10 mEq K+/L.
Intestinal fluids contain 20 – 50 mEq/L
.
Hypokalemia from loss of gastric fluid
).
Alkalosis
ion increases plasma bicarbonate(
Loss of hydrogen
*
.
increases aldosterone secretion
pletion
volume de
*Coexisting
levels, sodium is retained and potassium
increased aldosterone
* In the setting of
excreted.
Potassium loss is most prominent early.
Actual losses in gastric juice are relatively small.
Diarrheal losses are usually accompanied by metabolic acidosis
1.Villous adenoma
.Laxative abuse
2
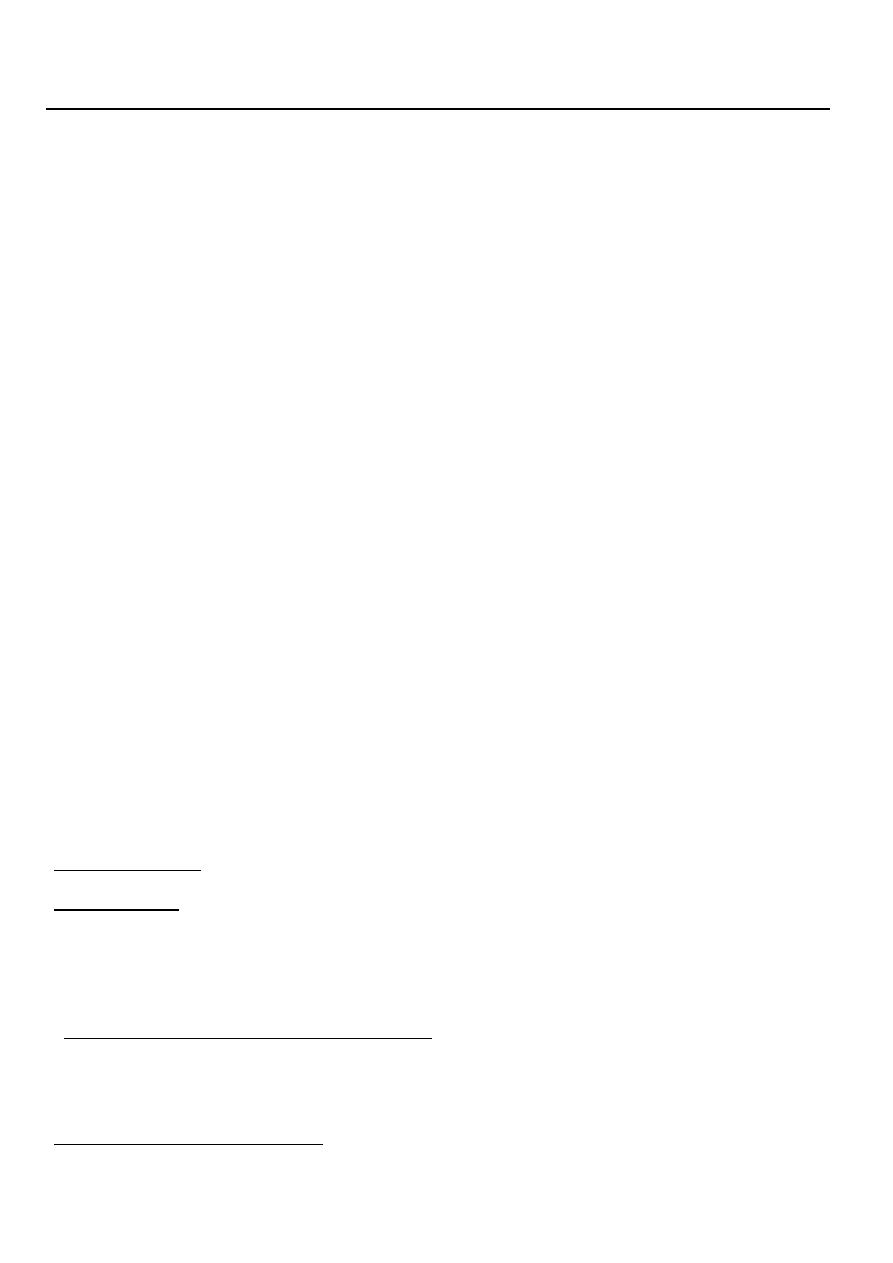
The kidney and potassium
Renal K+ Loss
Urine K+ >20 mEq/24 hours
or spot urine K+ of > 30
*Nearly all potassium filtered at the glomerulus is reabsorbed in the proximal nephron.
.
Urinary potassium is the result of distal potassium secretion
*
,
adequate number of nephrons
* To excrete potassium, the kidney requires an
adequate to provide adequate distal delivery of sodium for
circulation
, and a
aldosterone
sodium/potassium exchange.(Na-K-ATPase)
Causes of Renal loss of potassium
Primary hyperaldosteronism ( Conns syndrome),
Cushing syndrome and increased steroids.
Diuretic therapy :Thiazides, loop diuretics and *Diuretics- activate the renin-angiotensin-
aldosterone cascade.
Cabonic anhydrase inhibitor
DKA
Renal tubular acidosis (RTA)
Proximal RTA type 1 and 2 ,Some distal types
(
(Type IV RTA patients are typically hyperkalemic
3
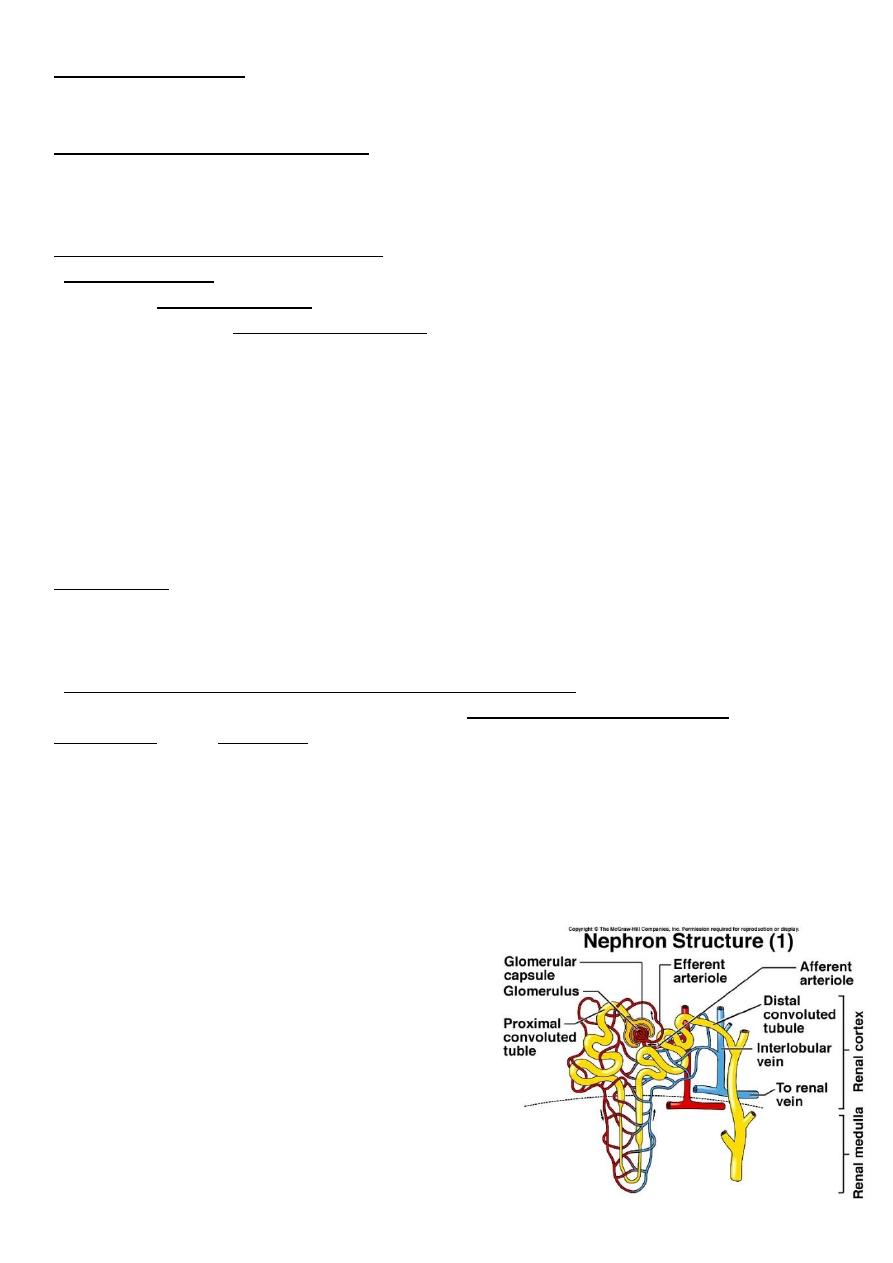
Clinical manifestations of Hypokalemia
s
Neuromuscular disorder
Muscle Weakness, flaccid paralysis, respiratory arrest,
:nuasia , constipation paralytic ileus
GIT
DI( Polyuria,polydypsia)
Acquired Nephrogenic
: Arrhythmias, Postural hypotension
Heart
ECG Changes: Flat T-wave appearance of U wave
Cardiac arrest
Management
*treat underlying cause
*correction of alkalosis
*Oral…KCL Tabs
exceed 10mmol per
….DO NOT
slowly
KCL should be
infusion of
…….beware……
Parenteral
*
hour