1
Third stage
Medicine
Lec-4
د
.
عبدالحق
1/1/2014
Hyperkalemia
Hyperkalemia
Severe: above 6.5 mmol/l carry
Risk of cardiac stand still in diastole
c/p: progressive muscular weakness or no symptoms
Of Hyperkalemia
Causes
1.(spurious) Pseudohyperkalemia
2.Excessive intake (diet, iv therapy..)
3.Redistribution out of cells
4.Endogenous increase K Load
(
5.Medications(ACEI,B-BLOCKER,K-sparingD
:
6.Renal retention of K
(
Renal failure or Tubular secretary failure
)
1.Spurious Hyperkalemia
Hemolysis (in tube )
Delay in processing of blood
Severe leukocytosis or thrombocytosis
2. Redistribution out of cells
1.Metabolic acidosis
2.Insulin deficiency
3.B-BLOCKERS
4.Hyperkalemic periodic paralysis
3. Exogenous(diet,K therapy)
2
4. Endog enous K load
Rhabdomyolysis
Hemolysis
Tumor lysis syndrome
Severe exercise
:
5. Renal Retention of K
In renal failure(especially when S.Cr >500 mic mol/L) ie with decrease GFR
A. Sever Acute Renal Failure , esp with Hemolysis , Rhabdomyolysis , Acidosis))
B. Chronic Renal Failure(Advanced)
(esp with oliguria /K load)
Conditions with Hyperkalemia due to Renal Tubular Secretary Failure ie with preserved GFR
1.Addison disease
2.Congenital adrenal enzyme defect
3. Drugs : ACEIs , B-blockers ,NSAIDs and K Sparing Diuretics..Amiloride,Spironolactone
4.Tubulointerstial disease…no response to the Aldosteron by tubules..(SLE , transplant
(,Amyloidosis, Obstructive Uropathy
Investigations
Serum Electrolytes
Renal Function tests (B. urea ,S. Cr ), bicarbonate level
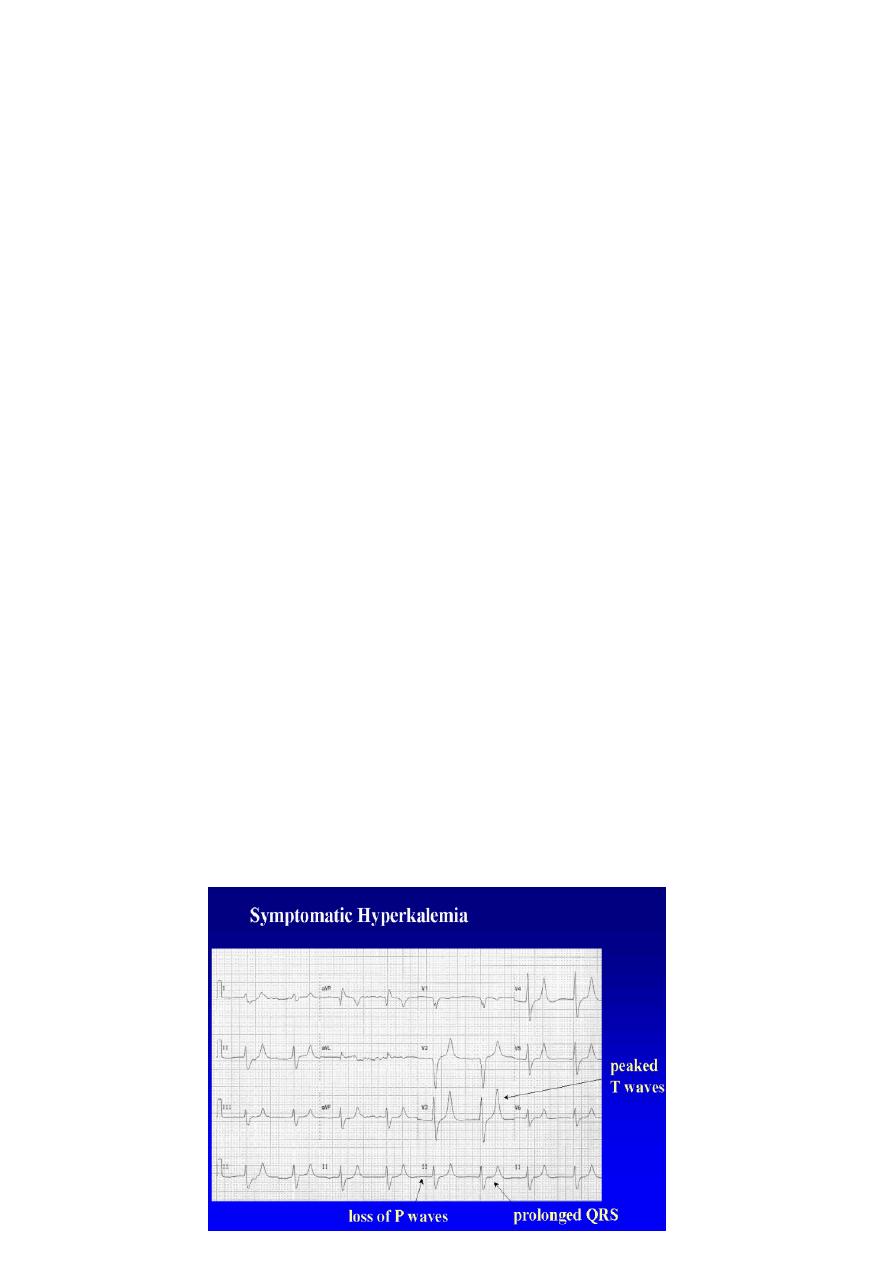
ECG
3
Treatment of Hyperkalemia
1- Stabilize myocardial membrane
2- Drive extracellular potassium into the cells
3- Removal of Potassium from the body
Stabilize myocardial cell membrane
3 min ,repeated if no reversal changes in ECG
-
10 ml 10% IV. Over 2
Calcium Gluconate
within 5-10 min
Drive extracellular potassium into the cells
10mg nibulized Salbutamol inhaler over 10 min, it will lower K
-
: or 5
Agonists
2
Inhaled
-
1
by 0.5-1.5 mmol/L started after 30 min ,action remain for 2-4 hours.
10 u with 25 gm of Glucose(Glucose50ml of 50% concentration) infusion
-
5
Soluble Insulin
-
2
within 10 min :
it will lower K by 0.5-1.5 mmol/L started after 15-30 min ,action remain for several hours.
*infusion of10-20%Dextrose 500ml within4-6hrs to minimize rebound increase in K
8.4%.
100ml of
If Acidosis , IV Sodium Bicarbonate
-
3
Removal of Potassium from the body
1.Frusemide IV with Normal Saline if renal function is normal
2.Ion Exchange Resin(eg. Calsium Resonium binds K+ in exchange for Ca++) given orally 15-
30 g or rectally 30g, which remove K from GIT.
and binds it in gut, primarily in large intestine, decreasing
+
for K
+
Exchanges Na
Resin
-
K
*
total body potassium
3.Dialysis if significant renal impairment