1
Third stage
Medicine
Lec-1
د
.
فاخر
1/1/2014
Major manifestations of lung diseases
Objectives
1-to enumerate the main respiratory features .
2-to discuss each one of them .
3-to make approach of diagnosis .
Respiratory diseases share the same manifestation from simple diseases like flu to the more
serious disease like bronchiogenic carcinoma. So we have to concentrate on these
manifestation to differentiate between them.
1- cough 2- sputum 3- haemoptysis
4-chest pain 5- dyspnea 6-cyanosis
7-clubbing
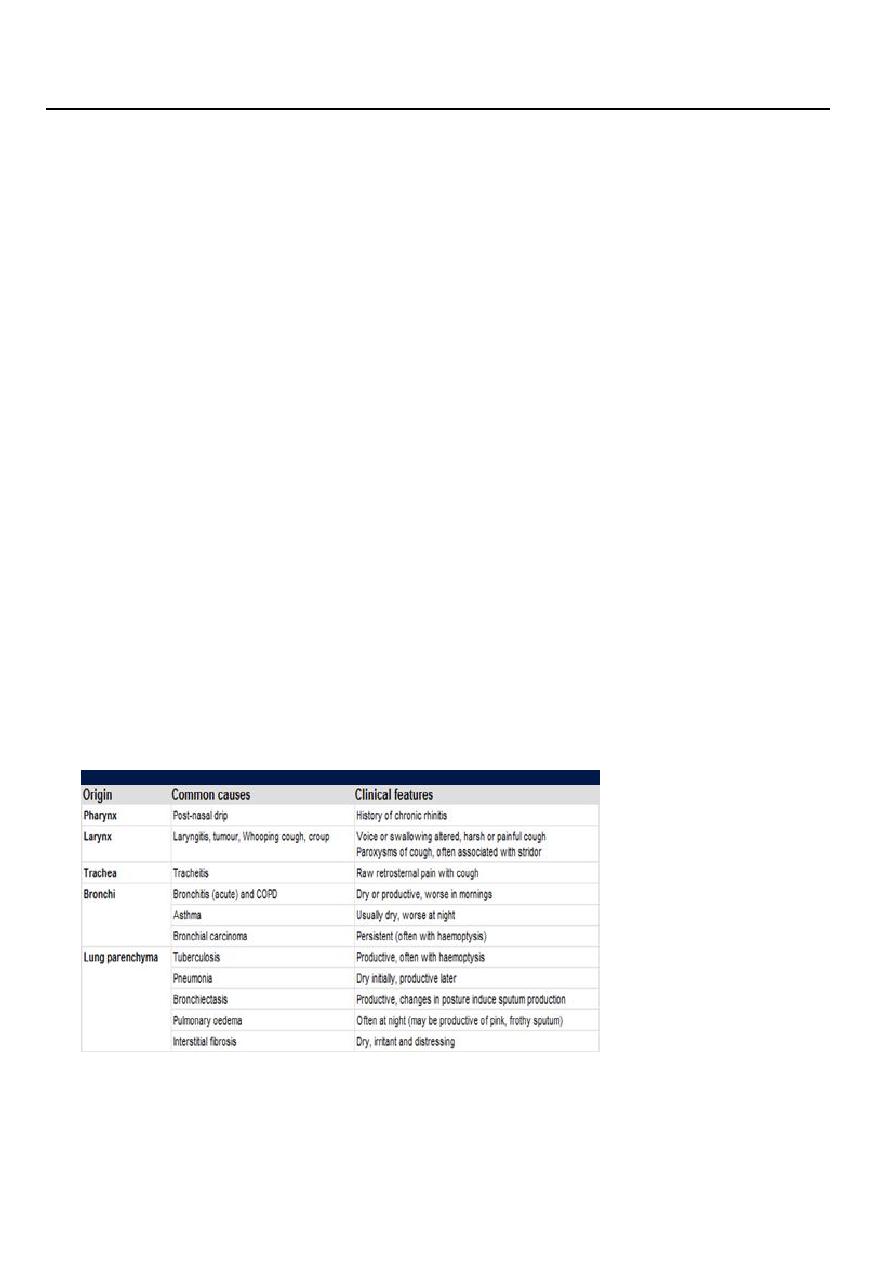
1- Cough
Dry or productive:
Dry bronchitis
Productive smoker, chronic bronchitis
Painful or painless:
change in the pattern of cough example from normal to
bovine and the patient has horsiness of voice
If the cough persists for more time 2-3weeks the patient should be send to the chest
x-ray (CXR).
2- Sputum
expectorated secretions which are produced out by coughing.
quantity: small or large.
quality: thin or thick(purulent).
color: white , yellow (mean there is infection) or green (must serious one).
2
If the sputum mixed with blood called Haemoptysis.
How we deal with sputum?
1.Gross examination.
2. Microscopical examination.
Investigation:
1. Gram stain: for bacterial examination.
2.AFB(acid fast bacillus) :for tuberculosis.
3.Cytology: for bronchiogenic carcinoma.
3-Haemoptysis
it is coughing of blood whether mixed with the sputum or pure. It may be small in
amounts or large in amounts.
The causes of large amounts of haemoptysis:
1. Bronchiectasis.
2. Lung abscess.
3. Tuberculosis.
4-CHEST PAIN
Chest pain is a frequent manifestation of both cardiac and respiratory disease and is
considered in detail on. Pleural or chest wall involvement by lung disease gives rise to
peripheral chest pain which is exacerbated by deep breathing or coughing). Central
chest pain suggests heart disease but occurs with tumours affecting the
mediastinum, oesophageal disease) or disease of the thoracic aorta).
Massive pulmonary embolus may cause ischaemic cardiac pain as well as severe
breathlessness. Tracheitis produces raw upper retrosternal pain which is worse on
coughing. Musculoskeletal chest wall pain is usually exacerbated by movement and
associated with local tenderness
Cardiac
o Myocardial ischaemia (angina)
o Myocardial infarction
o Myocarditis
o Pericarditis
o Mitral valve prolapse syndrome
Aortic
o Aortic dissection
o Aortic aneurysm
Oesophageal
o Oesophagitis
o Oesophageal spasm
o Mallory-Weiss syndrome
Massive pulmonary embolus
Mediastinal
o Tracheitis
o Malignancy
3
Lungs/pleura
o Pulmonary infarct
o Pneumonia
o Pneumothorax
o Malignancy
o Tuberculosis
o Connective tissue disorders
Musculoskeletal
o Osteoarthritis
o Costochondritis (Tietze's
o Rib fracture/injury syndrome)
o Intercostal muscle injury
o Epidemic myalgia (Bornholm disease)
Neurological
o Prolapsed intervertebral disc
o Herpes zoster
o Thoracic outlet syndrome
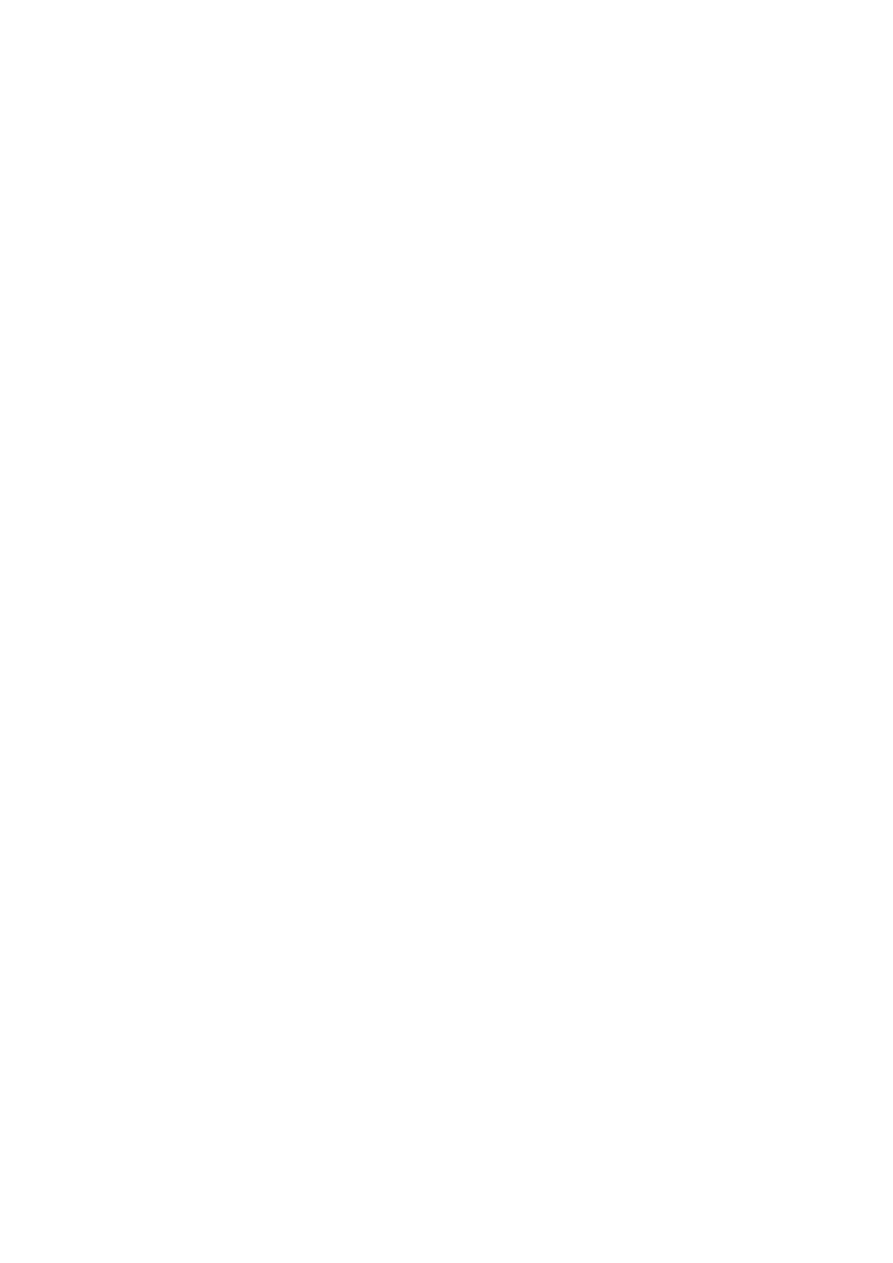
Breathlessness or dyspnea
Can be defined as the feeling of an uncomfortable need to breathe. It is unusual
among sensations in having no defined receptors, no localised representation in the
brain, and multiple causes both in health (e.g. exercise) and in diseases of the lungs,
heart or muscles.
Pathophysiology Physiological stimuli to breathing are summarised in. Respiratory
diseases can stimulate breathing and dyspnoea by stimulating intrapulmonary
sensory nerves (e.g. pneumothorax, interstitial inflammation and pulmonary
embolus), by increasing the mechanical load on the respiratory muscles (e.g. airflow
obstruction or pulmonary fibrosis) or by causing hypoxia, hypercapnia or acidosis,
stimulating chemoreceptors. In cardiac failure, pulmonary congestion reduces lung
compliance and can obstruct the small airways.
Dyspnea:
o Heart failure
o Respiratory failure
o Pneumonia
o Asthma
o Metabolic :diabetic
ketoacidosis –renal
failure
4
Asthma
Dyspnoea in asthma is associated with episodes of wheeze or chest tightness, varying in
severity over time, but usually worse in the morning and often waking the patient
overnight. There may be a history of childhood wheeze, or of wheeze or rhinitis provoked
by pollens, dusts, household pets or occupational allergens. In exercise-induced asthma,
wheeze and chest tightness typically come on immediately after exercise.
Heart disease
Impaired left ventricular function can cause exertional dyspnoea. Orthopnoea, cough and
wheeze may also be present, as in lung disease. A history of angina or hypertension may be
useful in implicating a cardiac cause. On examination, an increase in heart size as judged by
a displaced apex beat, a raised JVP and cardiac murmurs may indicate cardiac disease
(although these signs can occur in severe cor pulmonale). The chest X-ray may show
cardiomegaly
Cyanosis
Is an abnormal bluish discoloration of the skin resulting from an increase in the level
of reduced hemoglobin in the blood, and, in general, reflects an arterial oxygen
saturation of 85% or less (normal arterial oxygen saturation ≥95%). Central cyanosis
presents as cyanosis of the lips or trunk and reflects right-to-left shunting of blood
owing to structural cardiac abnormalities (e.g., atrial or ventricular septal defects) or
pulmonary parenchymal or vascular disease (e.g., chronic obstructive pulmonary
disease, pulmonary embolism, pulmonary arteriovenous fistula).
Peripheral cyanosis
May occur because of systemic vasoconstriction in the setting of poor cardiac output
or may be a localized phenomenon resulting from venous or arterial occlusive or
vasospastic disease (e.g., venous or arterial thrombosis, arterial embolic disease,
Raynaud's disease). When cyanosis presents in childhood, it usually reflects
congenital heart disease with right-to-left shunting of blood.
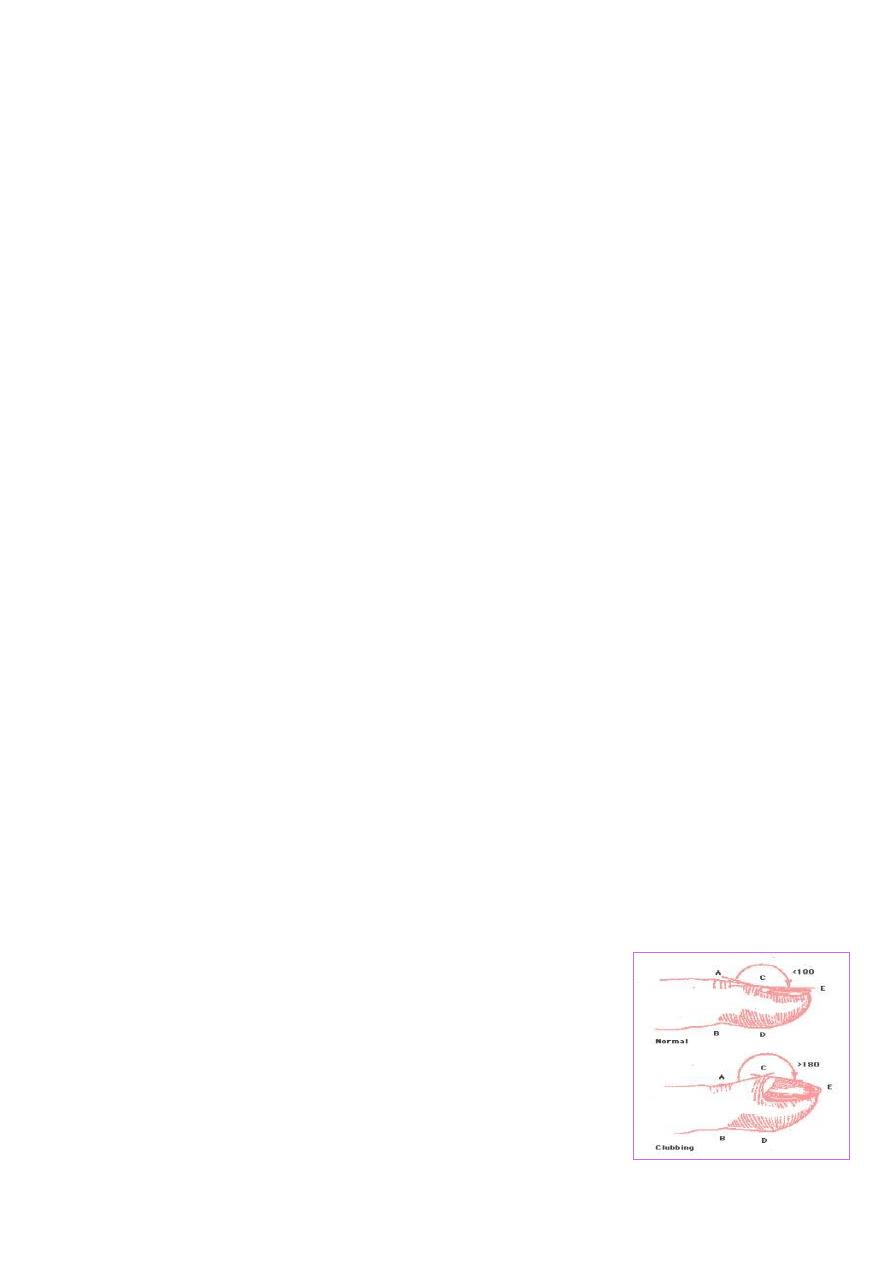
Clubbing
Loss of the angle between the nail and nail bed.
Normally the angle 175 (less than 180 ) and becomes 180 and more in clubbing.
So clubbing characterized by :
1. Increase curvature of the nail.
2. Swelling of the terminal phalanges (drumstick).
Causes of the clubbing:
1. Lung abscess.
2. Fibrosing alveoli.
3. Bronchiogenic carcinoma.