
1
Third stage
Medicine
Lec-2
د
.
م
زاحم
الجيتجي
1/1/2014
CHEST PAIN
Objectives
To learn common causes of chest pain and the character of each type (description of
clinical features)
Chest pain is a common presentation of cardiac disease, but can also be a manifestation
of anxiety or of disease of the lungs, the musculoskeletal system or the gastrointestinal
system . Some patients deny 'pain' in favour of 'discomfort' but the significance remains
the same.
COMMON CAUSES OF CHEST PAIN
• Cardiac
o Mycocardial ischaemia(angina)
o Myocardial infarction
o Myocarditis
o Pericarditis
o Mitral valve prolapse
• Aortic
o Aortic dissection
o Aortic aneurysm
• Oesophageal
o Oesophagitis
o Oesophageal spasm
o Mallory-Weiss syndrome
• Lungs/pleura
o Bronchospasm
o Pulmonary infarct
o Pneumonia
o Tracheitis
o Pneumothorax
o Pulmonary embolism
o Malignancy
o Tuberculosis
o Connective tissue disorders (rare
• Musculoskeletal
o Osteoarthritis
o Rib fracture/injury
o Intercostal muscle injury
o Costochondritis (Tietze's syndrome)
o Epidemic myalgia (Bornholm disease)
2
• Neurological
o Prolapsed intervertebral disc
o Herpes zoster
o Thoracic outlet syndrome.
• Psychogenic/Anxiety
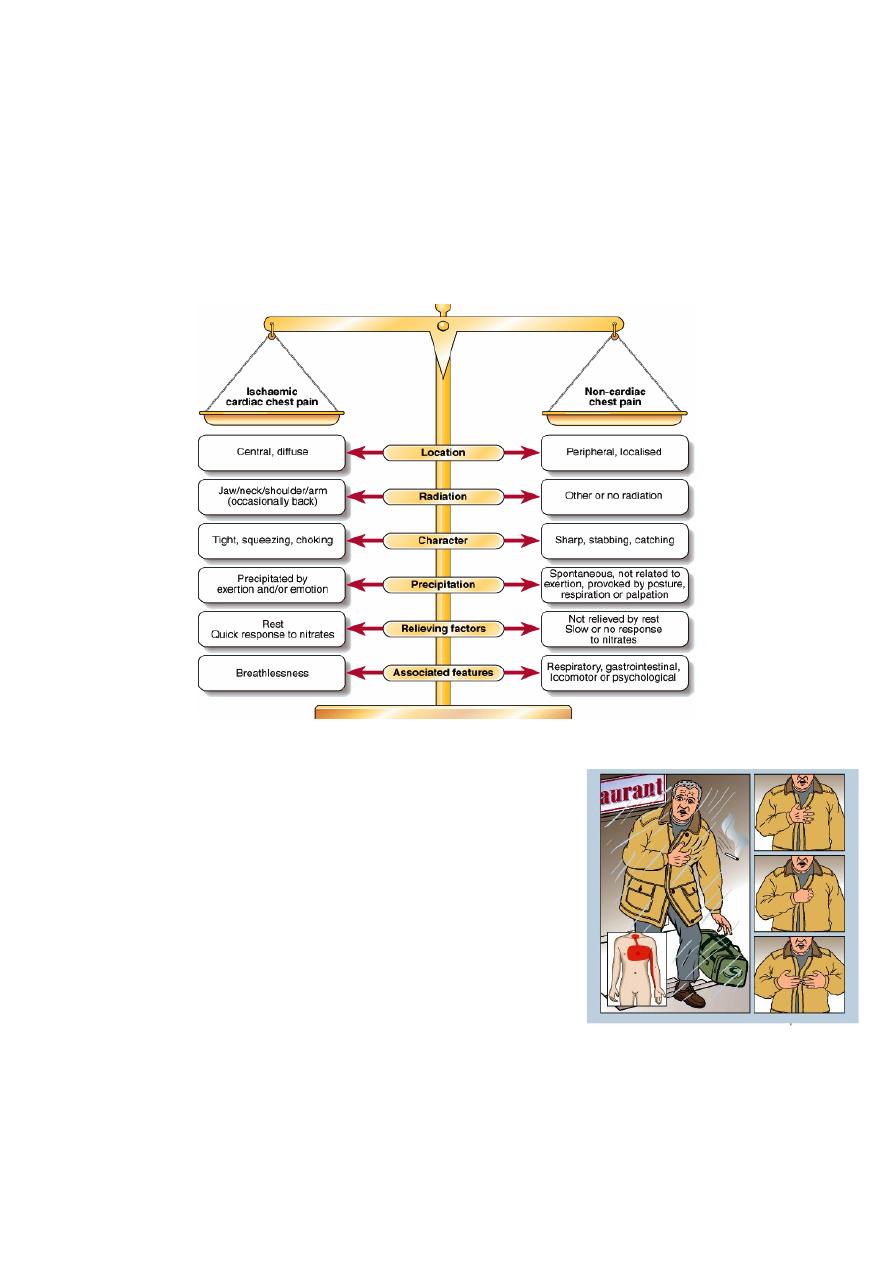
A number of key characteristics help to distinguish cardiac pain from that of other causes.
Diagnosis may be difficult and it is often helpful to classify pain as possible, probable or
definite ischaemic cardiac pain, based on the balance of evidence
CHARACTERISTICS OF ISCHAEMIC CARDIAC PAIN
• Site of origin of pain. Cardiac pain is typically located
in the centre of the chest because of the derivation of
the nerve supply to the heart and mediastinum.
• Radiation. Ischaemic cardiac pain, especially when
severe, may radiate to the neck, jaw, and upper or
even lower arms. Occasionally, cardiac pain may be
experienced only at the sites of radiation or in the
back. Pain situated over the left anterior chest and
radiating laterally may have many causes, including
pleural or lung disorders, musculoskeletal problems
and anxiety.
• Character of the pain. Cardiac pain is typically dull, constricting, choking or 'heavy',
and is usually described as squeezing, crushing, burning or aching but not sharp,
stabbing, pricking or knife-like. The sensation can be described as breathlessness.
Patients often emphasise that it is a discomfort rather than a pain. They typically use

3
characteristic hand gestures (e.g. open hand or clenched fist) when describing
ischaemic pain
• Provocation. Anginal pain occurs during (not after) exertion and is promptly relieved
(in less than 5 minutes) by resting. The pain may also be brought on or exacerbated
by emotion and tends to occur more readily during exertion, after a large meal or in a
cold wind. In crescendo or unstable angina, similar pain may be precipitated by
minimal exertion and may occur at rest. The increase in venous return or preload
induced by lying down may also be sufficient to provoke pain in vulnerable patients
(decubitus angina). The pain of myocardial infarction may be preceded by a period of
stable or unstable angina but may occur de novo.
In contrast, pleural or pericardial pain is usually described as a 'sharp' or 'catching'
sensation that is exacerbated by breathing, coughing or movement. Pain associated
with a specific movement (bending, stretching, turning) is likely to be musculoskeletal
in origin.
• Pattern of onset. The pain of myocardial infarction typically takes several minutes or
even longer to develop; similarly, angina builds up gradually in proportion to the
intensity of exertion. Pain that occurs after rather than during exertion is usually
musculoskeletal or psychological in origin. The pain of aortic dissection, massive
pulmonary embolism or pneumothorax is usually very sudden or instantaneous in
onset.
• Associated features. The pain of myocardial infarction, massive pulmonary embolism
or aortic dissection is often accompanied by autonomic disturbance including
sweating, nausea and vomiting.
Breathlessness, due to pulmonary congestion arising from transient ischaemic left
ventricular dysfunction, is often a prominent and occasionally the dominant feature
of myocardial infarction or angina (angina equivalent).
Breathlessness may also accompany any of the respiratory causes of chest pain and
may be associated with cough, wheeze or other respiratory symptoms.
Classical gastrointestinal symptoms (oesophageal reflux, oesophagitis, peptic
ulceration or biliary disease) may provide the clue to the source of non-cardiac chest
pain but effort-related 'indigestion' is usually due to heart disease.

4
Emotional distress is a very common cause of atypical chest . This diagnosis should be
considered if there are features of anxiety or neurosis, and the pain lacks a predictable
relationship with exercise.
However, it is important to remember that the prospect of heart disease is a frightening
experience, particularly when it has been responsible for the death of a close friend or
relative; psychological and organic features therefore often coexist.
Anxiety may amplify the effects of organic disease and can create a very confusing picture.
Patients who believe they are suffering from heart disease are sometimes afraid to take
exercise and this may make it difficult to establish their true effort tolerance; assessment
may also be complicated by the impact of physical deconditioning.
Myocarditis and pericarditis These conditions may cause pain that is characteristically felt
retrosternally, to the left of the sternum, or in the left or right shoulder, and typically varies
in intensity with movement and the phase of respiration. The pain is usually described as
'sharp' and may 'catch' the patient during inspiration or coughing; there is occasionally a
history of a prodromal viral illness.
Mitral valve prolapse Sharp left-sided chest pain that is suggestive of a musculoskeletal
problem may be a feature of mitral valve.
Aortic dissection This pain is severe, sharp and tearing, often felt in or penetrating through
to the back, and is typically very abrupt in onset
Oesophageal pain Oesophageal pain can mimic that of angina very closely, is sometimes
precipitated by exercise and may be relieved by nitrates; however, it is usually possible to
elicit a history relating chest pain to supine posture or eating, drinking or oesophageal
reflux. It often radiates to the back.
Bronchospasm Patients with reversible airways obstruction, such as asthma, may describe
exertional chest tightness that is relieved by rest. This may be difficult to distinguish from
ischaemic chest tightness. Bronchospasm may be associated with wheeze, atopy and
cough.
Musculoskeletal chest pain This is a common problem that is very variable in site and
intensity but does not usually fall into any of the patterns described above. The pain may
vary with posture or movement of the upper body and is sometimes accompanied by local
tenderness over a rib or costal cartilage. There are numerous causes of chest wall pain,
including arthritis, costochondritis, intercostal muscle injury and Coxsackie viral infection
(epidemic myalgia or Bornholm disease). Many minor soft tissue injuries are related to
everyday activities such as driving, manual work and sport.