
1
Fifth stage
Pediatric
عملي
-
كتابة الطالب
.د
ربيع
2/11/2015
Development:
Definition:
development is the acquisition of new skills &maturation of organs function.
Examples:
Development of hand function:
o At birth hands has reflex grasp (you can hold the baby by his grasp to your fingers)
this has no importance.
o At 4
th
months
active grasp: by his intention he will couch the objects.
o At 8
th
month
scissor grasp or radial assisted grasp (with thumb and fingers).
o At 10
th
month
pincer grasp with thumb and forefingers.
o At 1
st
year
like adult he couch objects.
Development of speech:
o In the beginning
throaty sound.
o After 4 months
vowels.
o After 8 month
s
consonants.
o 1 year
2words.
o 2 years
200 words.
o 4 years
all speech must be compressible.
Developmental history:
Four questions to be asked in developmental History:
1. Gross motor roll over? Sit? Crawl? Walk? Going up stairs?
2. Fine motor movements of fingers, couching objects, shoe tie, buttoning,
unbuttoning.
3. Social adaptation smile, knows his mother, clapping, bye-bye, annoyed when
being taken from his mother, control his urination & defecation.
4. Language or speech.
Examples:
o Social smile → smile in response to social contact (not during sleep) at 3-6 weeks
"21days" if delayed serious CNS problem.
o Head control → 12-16 weeks.
o Active grasp → 4 months
o At 5.5 months → transfer object from one hand to another , roll over "supine,
prone"

2
o At 7 month → sit with support
o At 8 month → sit without support
o At 9 month → waving bye – bye, creeping and crawling الزحف كالدودة
o At 10 month → respond to his name
o At 1 year → says few word beside mama , baba & Drink by bottle
o At 9 month - 2 year separation anxiety
o At 12 month Walk assisted
o At 20 month Walk Without assisting
Important steps in general examination of a child:
1. Position
2. Consciousness
3. Orientation
4. Respiration
5. State of nutrition & hydration.
6. Vital signs
7. Measurements
8. Special things if present
#Position:
Flexed with fisted hands "as the patient we saw in the ward".
Extended posture "frog like".
Opisthotonous "his head & his heels on the bed while his body is arched commonly
seen in kernicterus "bilirubin encephalopathy"
Tetanus neonatorum, decerberate & decorticate posture.
#Consciousness: conscious, lethargic, comatose, lethargic with crying on examination only
(implying serious problem).
#Orientation: in child of more than 4-5 years old >> ask about (place, time, person)
#Respiration:
Regular or not, seek about sign of respiratory distress if present (infrasternal or
intercostals recession).
Chyne stokes breathing hyperpnea + pauseindicates severe brain insult
"Respiratory failure or heart failure" type 1 hypoxia is imminent, PO2 <92% while
type 2:- PCO2>45mmHg + hypoxia.
Chyne stokes breathing pattern is normal in premature or in neonate (1 week) old age.

3
#State of nutrition and dehydration:
CHO deficiency.
Protein deficiency >> edema
Fat deficiency >> medial aspect upper thigh & buttock "sites of storage of fat"
Vitamins and minerals:
1. B1 (thiamine) deficiency
beriberi "dry & wet"
2. B2 deficiency
normocytic anemia, cheilitis, stomatitis.
3. B3 (Niacin) deficiency
pellagra "diarrhea, dementia, dermatitis".
4. B7 (Biotin) deficiency
hypotonia, ataxia.
5. B9 (Folate) deficiency
anemia.
6. B12 (Cobolamin) deficiency
anemia with stomatitis & tongue soreness.
7. Vitamin A deficiency
dry & scaly skin.
8. Vitamin D Deficiency
rickets.
9. Vitamin K deficiency
bleeding.
Water and electrolytes (signs of dehydration) sunken eye, depressed fontanelle, dry
mouth, dry buccal cavity, absence of tear, poor skin turgor.
Note: wrinkling of skin in the area around the thigh is sign of wasting look for
abdominal distension + eversion of umbilicus.
#Vital signs:
Respiratory rate.
Pulse rate (if examined from any site other than the heart) >> for 1 minute
Heart rate (if taken from the heart) >> for 1 minute, difference between heart rate &
pulse rate pulse deficit.
Temperature (we must take the core temperature (rectally)) but usually taken from
axilla and corrected by adding 0.5 to it.
Blood pressure.
Capillary refill.
Pulse oximetry.
#Special things if present: Hydrocephalus, clubbing, cyanosis, down syndrome features.
#Measurements:
Height (if measured on ground) / length (if measured on bed)
Weight: 50 centile (ideal)
o Less than 1 year = (age in month + 9) /2
o 1-7 years = (age in year +4) * 2
o More than 7 years = (age in year) * 3
OFC: from most prominent area in the occiput to the 1 inch above glabella.
o At birth: 35 cm (in full term baby).
4
o At 1st year: 35cm +
o 2 months >> +4
o 4 months >> +3
o 6 months >> +2
o 8 months >> +1
o 10 months >> +1
o 12 months >> +1
o So at 1 year it will equal 49 cm
o At 2 years ( + 2.5 cm )
o Next 5 years ( + 0.5 cm / year )
o Next 5 years ( + 0.3 cm / year )
Tiny child vs. stunted growth:
o In tiny child the height and weight both decreased in a similar manner and often
there is a history of tinny child in family (seek about similar condition in family).
o While in stunted growth the height and weight are severely decreased and may be
not the same and there is no similar condition in the family and often associated with
other diseases.
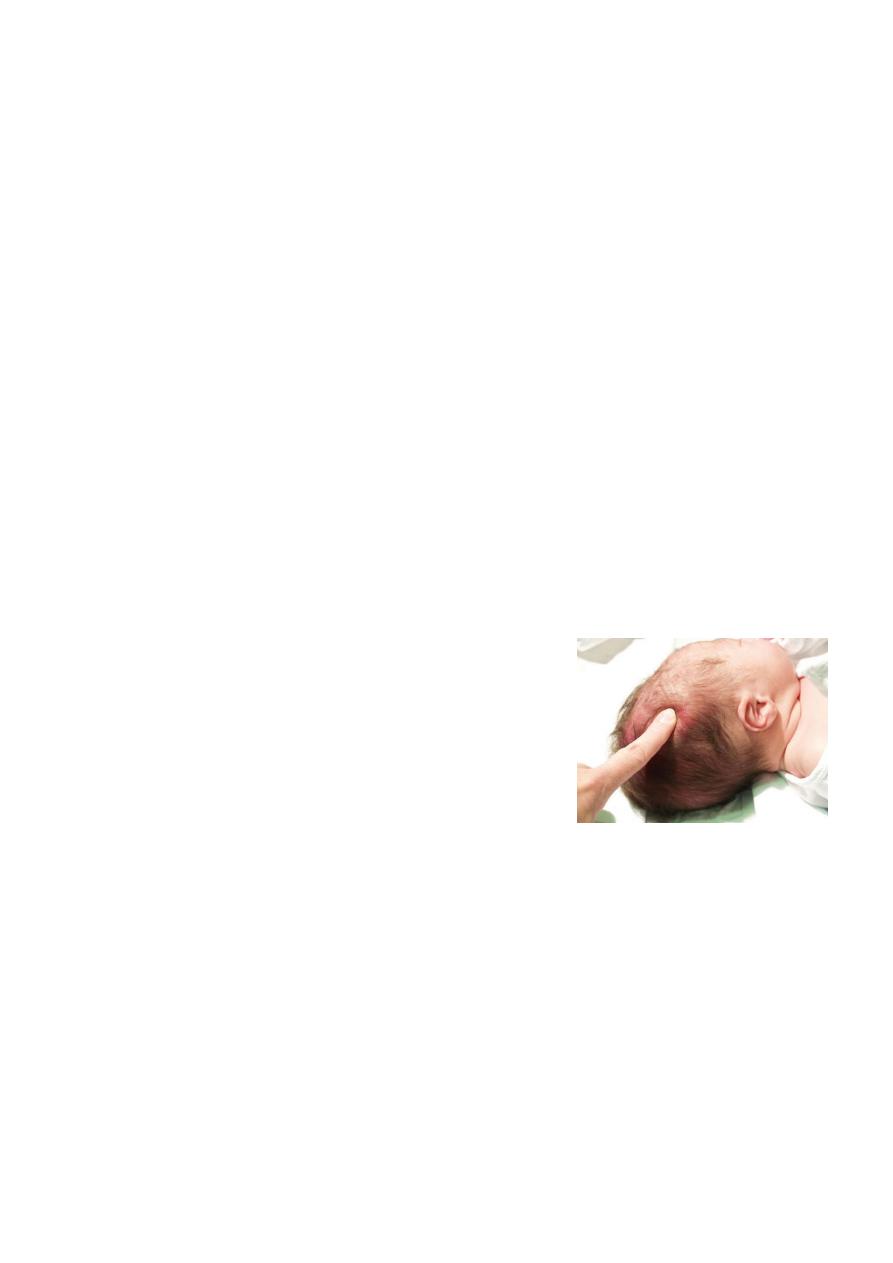
Craniotabes
Is a softening of the skull bones.
Can be a normal finding in infants, especially
premature infants.
It may occur in up to one third of all newborn infants.
It is harmless in the newborn, unless it is associated
with other problems these can include rickets and osteogenesis imperfecta (brittle
bones).
Maneuver press the bone along the area where the bones of the skull come
together "posterior parietal". The bone often pops in and out, similar to pressing on a
ping-pong ball if the problem is present. No testing is done unless osteogenesis
imperfecta or rickets is suspected.
.
Acidotic breathing in child with dehydration (causes of acidosis in children):

5
Gastroenteritis with dehydration → low renal perfusion → ↓GFR → ↓ excretion of
acids by kidney (pre-renal failure).
Gastroenteritis with diarrhea → loss of inlet juice → losing bicarbonate (HCO3) → no
compensatory loss of acids by kidney due to ↓ GFR (which is the only organ can
excrete acids from the body) → acidosis.
Renal failure due to diseased kidney:
o Congenital >> Horse shoe kidney, renal agenesis, duplication.
o Acquired >> Chronic glomerulonephritis, nephritic syndrome, nephritis.
Ketoacidosis → DM.
RTA → (renal tubular acidosis):
o Proximal RTA → problem in reuptake of HCO3. inefficient proximal tubulesno
recollection of CHO acidosis.
o Distal RTA → problem in excretion of H ion & retaining Na ions.
Notes:
Do not forget nutritional and hydration state during general examination.
Do not misdiagnose hyperventilation for dyspnea.
Respiratory failure type 1 → PO2 < 92 mmHg.
Respiratory failure type 2 → hypoxia + hypercapnia.
Bronchiolitis → not recurrent.
Asthma → recurrent.
Chyne stock respiration >> period of hyperventilation then period of apnea which is
normally seen in neonate especially if preterm.