1
Surgery
For
4
th
stage
http://goo.gl/rjRf4F
I
LOKA
©
http://www.muhadharaty.com/surgery
I

2
Content
Topics:
Page:
Lump & Ulcer
3
Trauma
5
Hernia
10
P.R examination
14
I.V fluid
16
Stoma & Drains
18
Acute abdomen
20
Acute appendicitis
25
Intestinal obstruction
30
Splenomegaly
35
Chest Trauma & Chest Tube
37
Death in Chest Trauma
43
The Breast
47
Vascular Trauma
53
Head injury
60
Neck swellings
62
Thyroid gland
65
Salivary glands
71
3
Part1
: General surgery
(Lump & Ulcer)
1- The History of a Lump or an Ulcer
Duration: when was it first noticed? When it was first appeared?
First symptom: what brought it to the patient’s notice? when washing, pain,
someone else noticed it
Other symptoms: What symptoms does it cause?
o Lump: Interfere with movement, respiration, or swallowing.
o Ulcer: bleeding, discharge, smell, interference with walking, eating, or defecation.
Progression: How has it changed since it was first noticed?
o Lump: Size: enlarged, got smaller, fluctuated in size.
o Ulcer: size, shape, discharge and pain.
Persistence: Has it ever disappeared or healed?
o Lump: may disappear on lying down, or during exercise, and yet be irreducible at
the time of examination.
o Ulcer: has it healed or broken down? Record the history of each period.
Multiplicity: Has (or had) the patient any other lumps or ulcers? Obtain a complete
history of any other lumps or ulcers.
Cause: What does the patient think caused it? Following injuries (record type &
severity), or systemic illnesses.
2- The Examination of an Ulcer
Site
Size (Depth: in millimeters, and by describing
the structures it has penetrated)
Shape
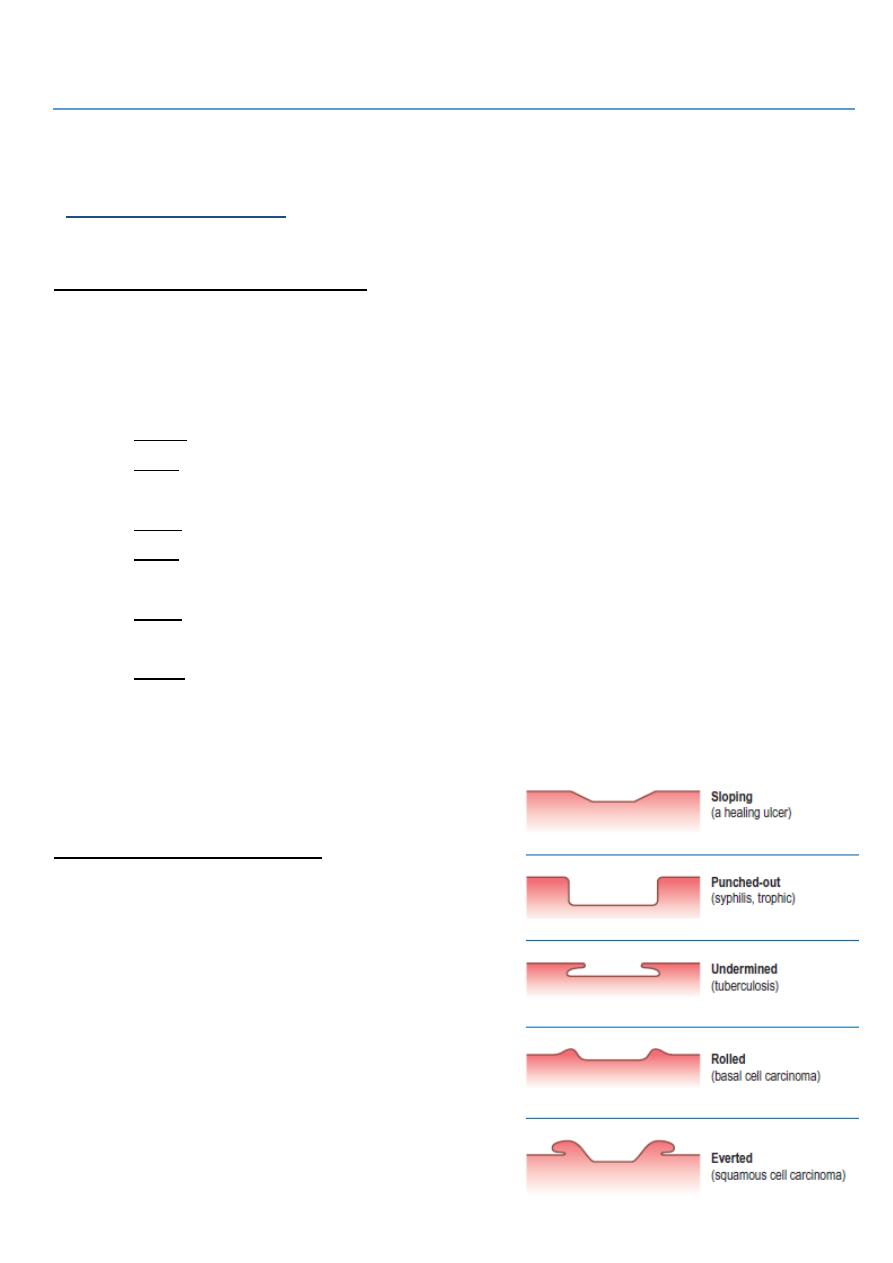
Edge: (sloping, punched out, undermined,
rolled, everted)
Floor: consists of slough, granulation tissue,
tendon or bone
Discharge: serous, sanguineous,
serosanguinous or purulent

4
Mobility/fixity: Move the ulcer and inspect skin for movement. Ask the patient to
tens the underlying muscle and then test mobility.
Inspect surrounding skin color. Palpate for temperature, tenderness.
Palpate the edge of ulcer: soft (healing), firm (non healing), hard (malignancy)
State of the local tissues: local blood supply, innervation of the adjacent skin, and
regional lymph nodes.
General examination.
3- The Examination of a Lump
Site: described in exact anatomical terms, using distances measured (by tape
measure) from bony points
Size: width, length & depth. Irregular lumps may need a diagram.
Shape: spheres, hemispheres, & asymmetrical outline (pear shaped or kidney
shaped)
Overlying skin: discolored, smooth, rough.
Temperature: hot or of normal, assess by the dorsum of the hand.
Tenderness: watch the patient’s face for signs of discomfort as you palpate. Always
try to feel the non-tender part before feeling the tender area.
Surface: smooth, irregular (cobblestones=bosselated) or rough. Large lumps have
mixture of surfaces.
Consistence: stony hard, firm, rubbery, spongy soft.
Edge: clearly defined or indistinct.
Fluctuation: Pressure on one side of a fluid-filled cavity makes all the other surfaces
protrude. Fluctuation can only be elicited by feeling at least two other areas of the
lump whilst pressing on a third.
Compressibility: vascular malformations and fluid collections can be compressed
until they disappear, but when left the lump re-forms.
Reducibility: hernia and some vascular lumps can be compressed so that it gets
smaller and then move into another place (disappears). Ask the patient to cough, the
lump may return (cough impulse), or it may tense on child’s cry.
Move: to test mobility/fixity
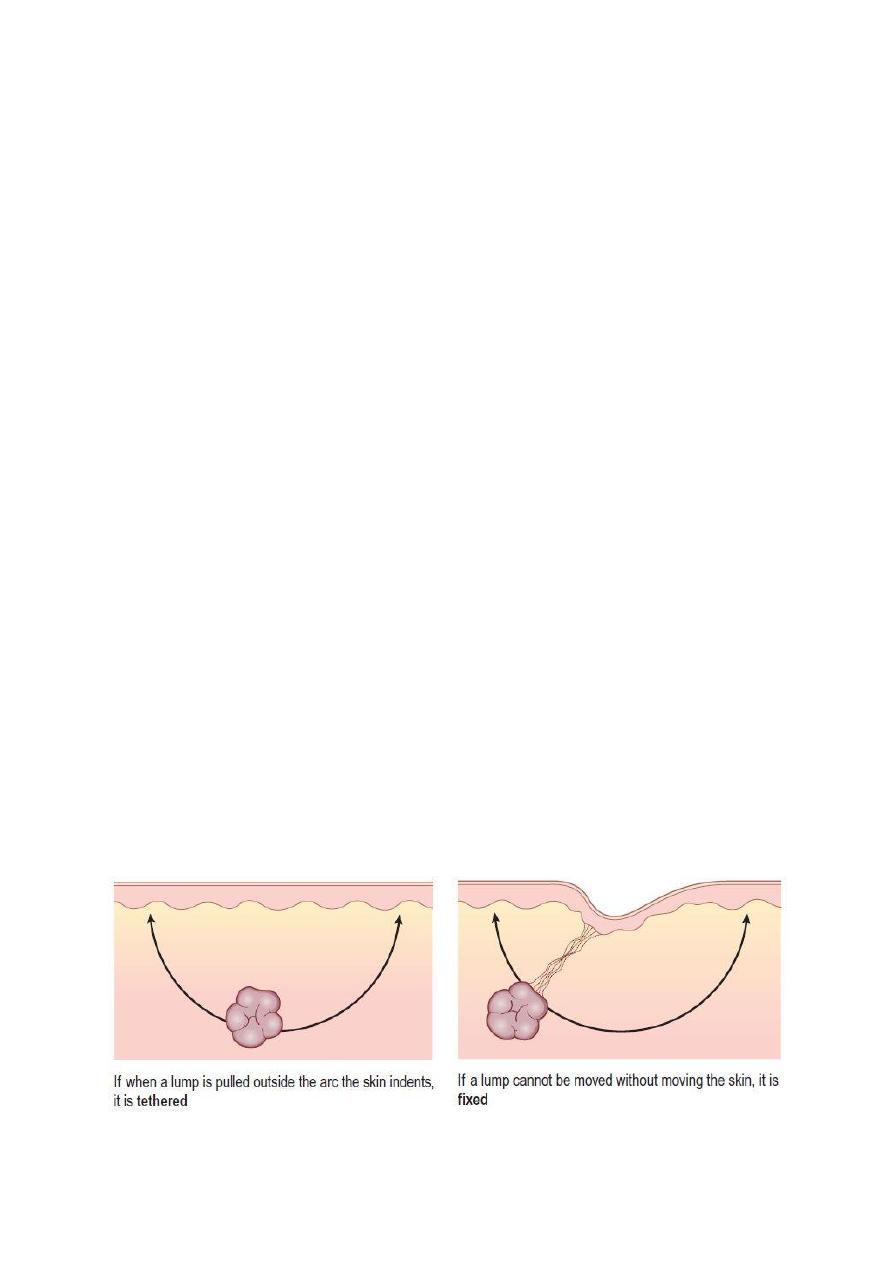
o Pinch the skin overlying the lump. Immovable skin indicates skin attachment.
o Move the lump and inspect skin for movement or puckering.
o Underlying muscles must be tensed: if it is still mobile then it is not attached to
the muscle. If it is less mobile, it is attached to the muscle. If it disappears then it
arises from below the muscle.
5
o Lumps that are attached to or arising from vessels or nerves may be moved from
side to side across the length of the vessel or nerve, but not up and down along
their length.
Palpate with both hands (Pulsatility):
Let your hand rest still for a few seconds on every lump to discover if it is pulsating.
Place the fingers of each hand on opposite sides of the lump. Expansile pulsation:
aneurysms and very vascular tumors push upwards and outwards. Transmitted
pulsation: lump is near to an artery and are moved by its pulsations upward.
Flick the lump (Fluid thrill): Large fluid collection easily conduct a percussion wave.
Percuss: Dull note indicates solid and fluid-filled lumps. Resonant notes in gas-filled
lumps.
10-Auscultate: Vascular lumps that contain an arteriovenous fistula may have a
systolic bruit. Hernia containing bowel may have audible bowel sounds.
Illuminate: Translucence or Trans illumination requires a bright pinpoint light source
and a darkened room. The light should be placed on one side of the lump, not
directly on top of it. The light should be seen in an area distant from the site in
contact with the light source.
o Positive for water, serum, lymph, or highly refractile fat.
o Negative for Blood and other opaque fluids do not transmit light.
State of local tissues: artery (weak distal pulse), vein (distended veins & edema),
nerve (paresis, loss of sensation), muscles (wasting), bone (erosion), and joints
(movement of proximal and distal joint).
General examination
Surgical scar: see the type – site – length – position (linear –
oplique – transverse) – stretch marks – discharge – bleeding –
ulcer
Symptoms with lump that indicate malignancy:
wasting
weight loss
anemia
fatigue
pressure symptoms

6
(Trauma)
Trauma is the major cause of death in the first 40 years of life
Trauma has 3 peaks of death:
1- Death at time of accident (seconds to minutes)
2- Death duo to life threatening trauma (minutes to hours)
3- Death after leaving the hospital (days to weeks)
Triage: is the process of determining the priority of patients treatments based on the
severity of their condition.it comes from French word and it mean to separate
BLS = basic life support: يتم تعليمها للناس العاديين للتقليل من أضرار اإلصابة
CLS = cardiac life support like CPR, giving drugs like dopamine and other things
important to save patients with emergency heart problem
ATLS = advanced trauma life support that divide in to primary /secondary/tertiary:
1- Primary survey: (ABCDEF)
A: airway patency: cervical spine stability – chin lift technique to avoid tongue
swallow
B: breathing: chest tube – nasal tube
C: circulation: check the vital sign – blood group – clotting screen – give worm fluid –
pressure on the site of bleeding, Put Two wide bore cannula, Give 1000cc of Ringer
lactate, should be warm to avoid hypothermia which may cause 1-Coagulopathy 2-
Acidosis.
D: disability: neurological problems - use Glasgow Coma Scale (form 3-15 score) or
AVPU system (A alert - V verbal - P pain - U unresponsive)
E: Exposure and Environment: rapidly check the pt. from head to toe and keep warm
environment to avoid hypothermia.
F: Fracture: do backslap or POP
Adjunct to primary survey:
o Foley's catheter (if no urethral bleeding)
o NG tube (if no fracture of the base of the skull)
o Intubation either: Endotracheal tube through mouth or through opening of
tracheostomy
o Monitoring of vital signs: PR, BR and oximetry
o Radiological investigation as X-ray (Chest, abdomen and pelvis), FAST (Focused
Assessment with Sonography in Trauma) and CT.
o ECG and cardiac markers (Troponin I and CK-MB) in cases of suspected cardiac
trauma.
o Diagnostic peritoneal lavage (examine peritoneal fluid).
o Diagnostic and therapeutic laparotomy or thoracotomy.
2- Secondary survey:
examination of patient from top to toe

7
take rapid history: AMPLE (A allergy – M medications – P past medical or
surgical or pregnancy – L last meal – E event or environment)
3- Tertiary survey: in special centers
History of trauma ((from doctor))
1- Duration of present illness (trauma): from the start of trauma until now
2- Pre-operative phase: describe the accident event:
Type of accident ( road traffic accident RTA – Fall from height – bullet)
Type of instrument or type of ground
Loss of conscious
Pain
Wound
Bleeding
Vomiting
3- Pre-hospital phase:
Time of arrival to the hospital
I.V fluid
Bandage
Antibiotics
Stop of bleeding
4- Hospital phase
History of trauma ((from Browse’s))
1. Cognitive function: ask who they are, where they live and their occupation.
2. History of the accident: ask the patient what they remember of the accident, and useful
if they can describe what happened. It is often helpful to know about:
-Gunshot
Type of machine: low velocity (pistol), high velocity (gun)
Number of bullets
Distance from shooter
Site of inlet and outlet
-Road traffic accident:
Was he the walker (on the street, sidewalk), driver, passenger (front or back seats),
protection (seat belts, airbags)
Others in accident: injured, dead.
Type of car and its speed (low or high velocity)
Damage to the vehicle: collision, rolling

8
-Fall from a height:
Height of fall
Did the patient hit anything on his way?
What position was the body at time of impact?
3. Walking after accident: to exclude pelvic and lower limb injuries.
4. Associated symptoms: Loss of consciousness, bleeding, vomiting, urination, cough,
dyspnea .
5. Transportation: car, ambulance
6. The distance of the hospital
7. What resuscitation and procedures done? What organs was damaged.
Examination of the Trauma
While doing general examination, palpate for symptomless swelling, laceration, bony
depression and distortion (especially in the head).
Post-operative Examination
1. General appearance of the patient
2. Input & output: IV fluid, drain (amount, color)
3. Wound:
Get permission
Inspection:
Dressing(clean, soaked with discharge)
Stitches (silk, nylon)
Color: red
Shape: healed
Discharge: (pus, blood, serum)
Bulging: fluid or something else
Palpation: Induration (indicates healing)
4. Examine the system involved.

9
#Fluid replacement after trauma:
Start as 2000 ml of crystalloid.
One unit of blood loss = three units of crystalloid replacement.
Increase the hematocrit as: one unit of hematocrit = one unit of blood.
#Blood gases test:
Ph., O2, CO2 saturation, electrolytes and every gas.
#Cardiopulmonary resuscitation (CPR):
CABC:
C = compression (100/ min) and ventilation (1 breath/ 8 sec),, depth of compression =
5 cm.
A = airway patency.
B = breathing.
C = circulation.

11
(Hernia)
Definition:
It is the protrusion of an intra-abdominal organ (intestine, …) through a defect in the
abdominal wall
Causes:
Congenital: such as vessel or viscous enters or leaves the abdomen
Acquired: Alongside structures penetrating the abdominal wall, Acquired weakness from
trauma or disease, Associated with raised intra-abdominal pressure
Types:
inguinal
femoral
umbilical
incisional
epigastric
Physical signs:
occur at congenital or acquired weakness in the abdominal wall
most hernias can be reduced
most hernias have an expansile cough impulse
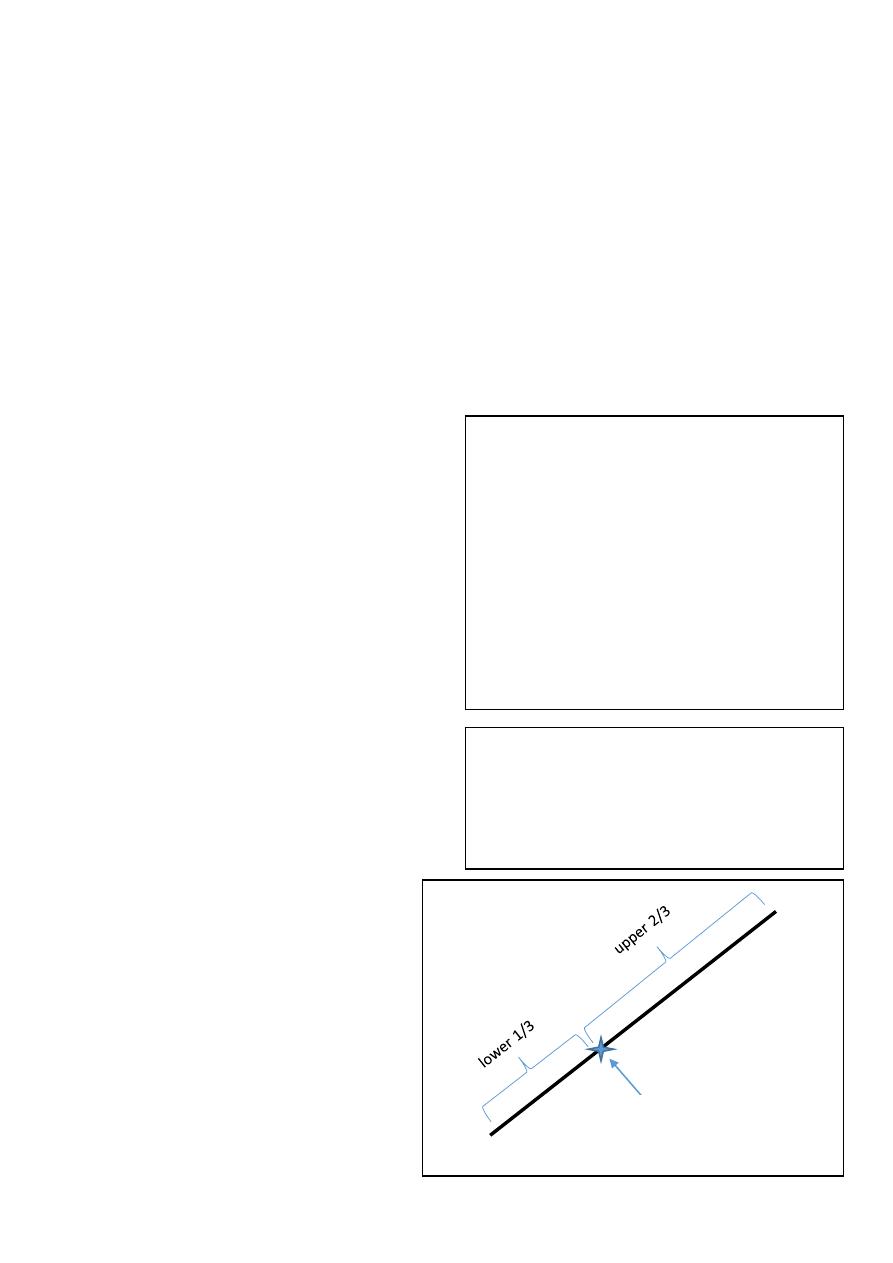
Inguinal hernia
Surface anatomy:
The inguinal ligament located between anterior superior iliac spine and pubic
tubercle (2-3 cm from midline)
11
The inguinal ligament is the lower inwardly folded edge of the aponeurosis of the
external oblique muscle
The external or superficial inguinal ring is an extension of the same aponeurosis
The internal or deep inguinal ring is the point of entrance of vas deference,
testicular artery and inferior epigastric artery. And it is a common site of hernia.
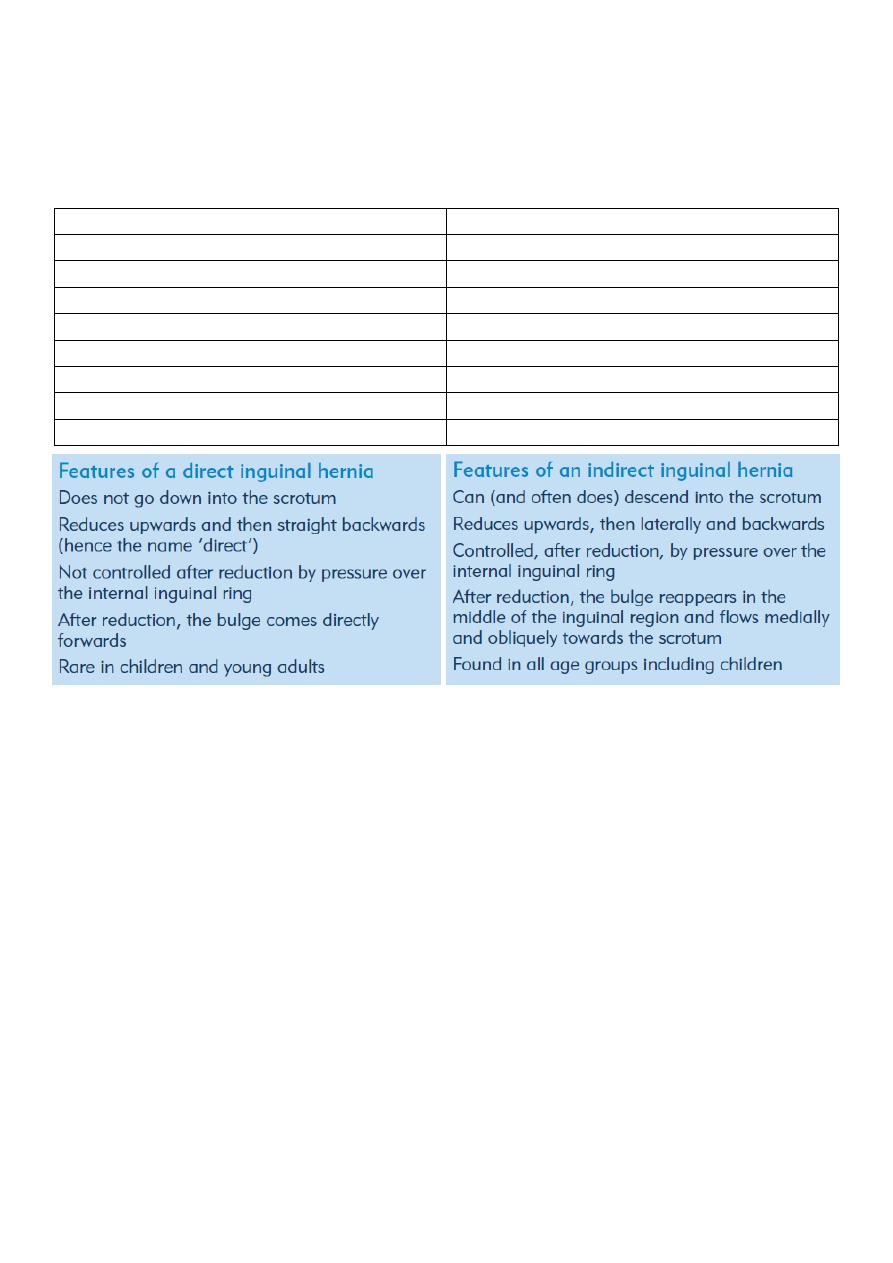
Direct inguinal hernia
Indirect inguinal hernia
Outside the spermatic cord
inside the spermatic cord
Not or rarely extend to the scrotum
usually extend to the scrotum
Wide neck of the hernia sac
narrow neck of the hernia sac
Medial to the inferior epigastric artery
lateral to the inferior epigastric artery
Less common
More common
Occur in old age
Occur in babies and adult
Not enter from the deep ring
Enter from the deep ring
Go out from the superficial ring
Go out from the superficial ring
Examination: ((from the book))
1- While the patient is standing upright.
Inspect: the inguinal and femoral canals and the scrotum for any lumps or bulges.
Ask the patient to cough; look for an impulse over the femoral or inguinal canals and
scrotum.
Identify the anatomical relationships between the bulge, the pubic tubercle and the
inguinal ligament to distinguish a femoral from an inguinal hernia.
Palpate
Form front: Examine the scrotum to decide whether the lump is a hernia or a true
scrotal lump (you can’t get above a hernia) .
Form side: Stand by the side of the patient with one hand on patient’s back to
support him, and your examining hand on the lump to define its characteristics.
2- Now ask the patient to lie down and establish whether the hernia reduces
spontaneously. If so, press two fingers over the internal inguinal ring at the mid-inguinal
point and ask the patient to cough or stand up while you maintain pressure over the
12
internal inguinal ring. If the hernia reappears, it is a direct hernia. If it can be prevented
from reappearing, it is an indirect inguinal hernia.
Examination of both direct and in direct inguinal hernia: ((from doctor))
1- Setting
Ask the patient to stand up
Always examine both inguinal regions.
2- Inspection:
Look at the lump from in front and assess:
the exact site and shape of the lump.
whether the lump extends down into the scrotum, if there are any other scrotal
swelling
any swelling on the ‘normal’ side.
3- Lying position: ask the patient to lie down then cough => you will see the hernia by
inspection
4- Standing position: exposure the inguinal region then stand in front of the patient and ask
him to cough and you will see hernia in the left or right side, if there is right hernia go
laterally from the right and put your hand on the hernia then make reduction of the hernia
then ask the patient to lie down and ask him to cough, now if you see the protrusion of the
hernia it is direct hernia but if you don't see it that means it is indirect hernia.
Femoral hernia: it is not reducible hernia so easily diagnosed
The differential diagnosis of an inguinal hernia
Femoral hernia
Hydrocele of the cord or the canal of Nuck
Undescended testis
Lipoma of the cord
The differential diagnosis of femoral hernia
Inguinal hernia
Enlarged lymph gland
Saphena varix
Ectopic testis
Note:
Put your hand on the hernia in the following manner:
Thumb: put it on the deep inguinal ring
Index: put it on the superficial inguinal ring (above pubic tubercle)
Middle finger: put it lateral to the pubic tubercle and 4 cm below it

13
Psoas abscess
Psoas bursa
Lipoma
The differential diagnosis of a lump in the groin
Inguinal hernia
Femoral hernia
Enlarged lymph glands
Saphena varix
Ectopic testis
Femoral aneurysm
Hydrocele of the cord or hydrocele of the canal of Nuck
Lipoma of the cord
Psoas bursa
Psoas abscess
14
(P.R examination)
1- Ask the patient about the pain: if there is pain you should give general anesthesia at first
then do PR exam
2- Privacy of the patient
3- Position:
Left lateral position
Dorsal position
Elbow-knee flexion position
4- Inspection: see the following: skin – hair – pilonidal sinus – perianal abscess – ulcer-
discoloration – hygiene – external hemorrhoids (position-size-color-thrombosis) – anal
fissure (acute, chronic – most common site in male and female is posterior) – fistula in ano (
single or multiple – above or below midline – anterior or posterior – distance from anus)
5- Sterile gloves
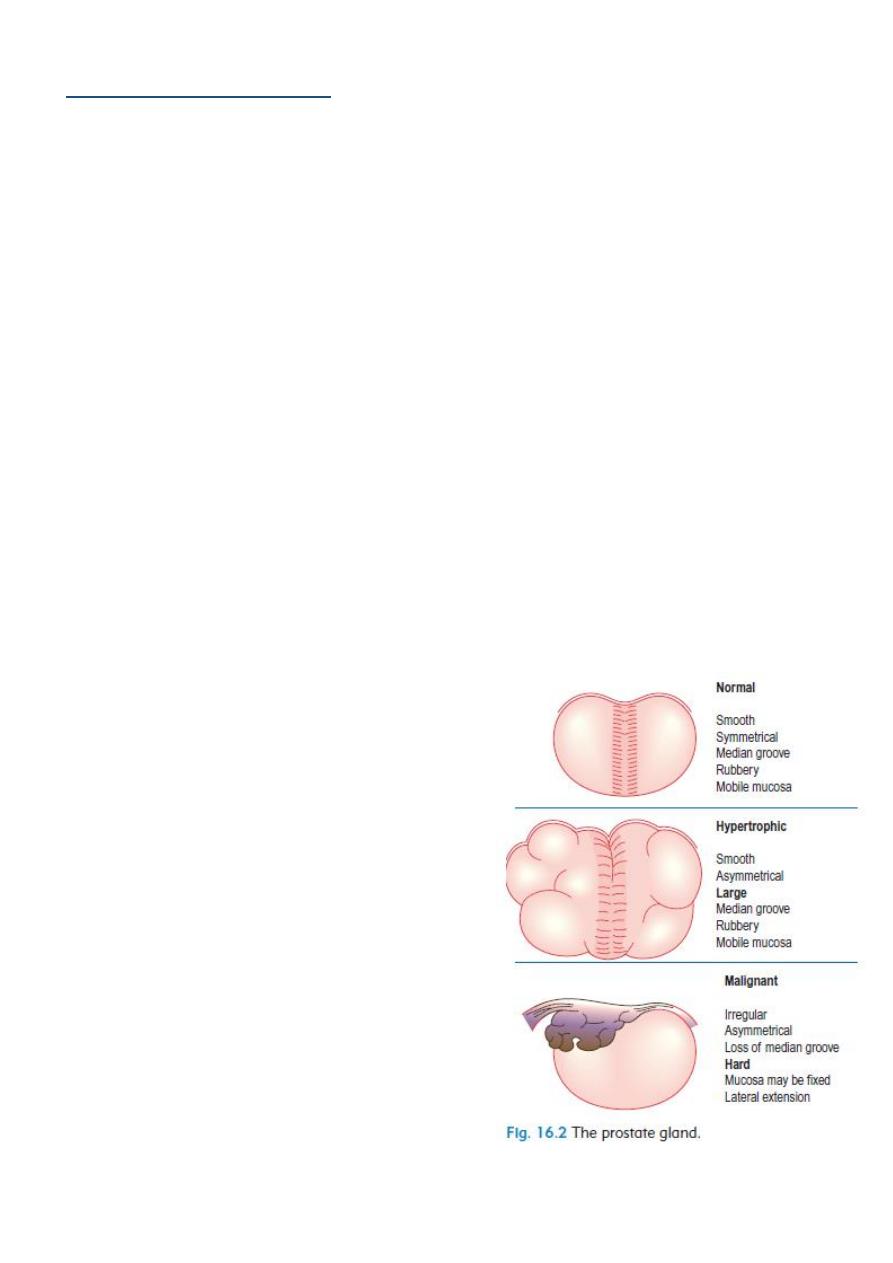
6- Introduce finger: feel the rectum and anal canal then feel the prostate (size-mucus above
it-fixed or mobile) feel the wall (soft-hard-ulcer-mass)
7- Tell the patient to squeeze: sometimes touch mass descent from above
8- In female feel: cervix – uterus – vaginal wall –
cervical excitation – Krukenberg tumor on the
ovary - The recto-vesical/recto-uterine pouch
9- Thank and cover the patient
Important note: virgin female do PR instead of
per vaginal
Indication of PR exam:
Suspected appendicitis
PR bleeding
Change bowel habits
Part of abdominal examination
Genitourinary problem
Pelvic or spinal trauma

15
Ano-Rectal Diseases
Bleeding: only blood passed by its self (diverticular disease, angiodysplasia), mixed
with feces (or on surface of feces), after defecation (hemorrhoids), on toilet paper
(hemorrhoids or fissure).
Tenesmus: intense desire to defecate with either nothing or small amount of mucous
and loose stool. Caused by anal or rectal carcinoma, IBD, IBS.
Pain on defecation
Straining on defecation
Pruritus
Incontinence and soiling: amount, color, consistency, frequency. Due to sphincter
failure, impaction with overflow, extreme urgency, neurological impairment.
Prolapse: with bowel action, during standing or walking. Fecal and urinary
incontinence may coexist.
Changed bowel habit

16
(I.V fluid)
1-
Crystalloid
: water + electrolytes
Normal saline ( NaCl 0.9% ) = 154 mql Na + 154 mql Cl: it is isotonic, not
pyrogenic, not immunogenic, used as volume expander in shock, trauma, burn
and dehydration.
Ringer's solution: NaCl + K + Ca + lactate that correct acid-base balance
Dextrose-water (glucose-water) = 5%, 10%, 25%, 50% : it is used in
nourishment of patient and in hypoglycemic state, but not used in shock and
burn because it can lead to hypotension
Dextrose-saline (dextrose-water + normal saline) = 1/3, 1/5
Ringer's solution and Ringer's lactate used in burn and trauma
2-
Colloids
: high molecular weight solutions like:
Protein ( albumin )
Polysaccharide
Glycine
Plasma
Hematin
Gelatin
Dextran
Take blood sample for cross-matching before give these solutions, and they could
lead to infections transmission like malaria and hepatitis
Post-surgical fluid
There is neuro-hormonal response to trauma (like increase ADH and increase aldosterone
that lead to edema and hypertension due to Na retention) so we give fluid according to this
response.
1- First day:
Type of fluid: glucose-water // Amount of fluid:
Ongoing Loss: IN diarrhea, sweating, drain, nasogastric tube, dehydration. Depend
on conscious state and urine output (400-500 ml normally) (calcium needed). Give
fluid according to type of trauma, surgery and patient.
Deficit: give fluid according to type of trauma, surgery and patient.
Maintenance:
o Minimum requirement of patient is 5% dextrose water
17
o One liter of dextrose water = 50g of glucose
o BMR = 500 Kcal
o Rough method minimum 2-3 liters fluid in 70 kg patient
o Calculate like the following
For example: 70 kg adult first 10 kg = give 100 ml/kg = 1000 ml
Second 10 kg = give 50 ml/kg = 500 ml
Reminding kg = give 20 ml/kg = 1000 ml
So we will give 2500 ml of iv fluid to this patient
Not give K in the first day because the trauma make the effect on aldosterone so
there are sodium and potassium retention so not give K.
2- Second day:
Give glucose-saline in same amount (or) glucose saline + normal saline + electrolytes
3- Third day:
Give K
1 ml/kg = 60-80 ml of K
K is given with fluid, Normal range of K = 3.5-5.0 (mEq/L)
4- After 3 days: change the type of nutrition from IV fluid to other types of parenteral
nutrition

18
(Stoma & Drains)
Stomas
A colostomy (or ileostomy) stoma is an artificial opening made in the colon
(or small intestine) to divert feces and flatus outside the abdomen where they can be
collected in an external appliance. Depending on the purpose for which the diversion
has been necessary, a stoma may be temporary or permanent. Temporary or
defunctioning stomas are usually fashioned as loop stomas, while end stomas usually
as a result of surgical removal of distal bowel.
Ileostomy: Formed from any part of the mid- or distal small bowel. Ileostomies (loop
or end) are usually spouted, have prominent mucosal folds, tend to be dark pink/red
in color, and are most common in the right side of the abdomen. Ileostomy effluent is
usually liquid; patients are more likely to develop fluid and electrolytes problems.
Colostomy: Formed from any part of the large bowel. Colostomies (loop or end) are
usually flush, have flat mucosal folds, tend to be light pink in color. A colostomy
effluent is usually solid and they are most common in the left side of the abdomen.
Stoma complications
o Skin irritation
o Prolapse
o Retraction
o Ischemia
o Stenosis
o Parastomal hernia
o Bleeding
o Fistulation
When you see a stoma (during abdominal examination) examine it.
o Inspect:
- Site.
- Shape (spouted, flush)
- Type.
- Effluent.
- Complications: prolapse, retraction, necrosis of the distal end, fistula, stenosis,
hernia, bleeding, colostomy diarrhea, contact dermatitis.
o Ask the patient to cough: stomal hernia, parastomal hernia.
o Examine perineum:
- Closed by abdominoperinial resection in permanent colostomy.
- Intact in temporary colostomy.

19
Colostomy bag ((from doctor))
1- Site of colostomy: in the left iliac fossa it is related to the colon (colostomy) but in the
right iliac fossa it is related to the small intestine (ileostomy)
2- Stool ( color – amount - ………… )
3- Types of colostomy: permanent colostomy – temporal colostomy – terminal
colostomy – loop colostomy – double burl colostomy
4- Types of ileostomy: temporal ileostomy – permanent or terminal ileostomy
Drains
Types of drainage:
1- Closed drainage system: tubes with bags (( the tubes should be flexible and rubber but
we don't have this proper type of tubes ))
2- Open drainage system: only tubes without bags
3- Active drainage: maintained under suction
4- Passive drainage: have no suction
Indication:
1- To evacuate (drain) existing abnormal collections of fluid or gas, To remove pus, blood,
serous exudates, chyle or bile
2- To help eliminate dead space
3- To form a controlled fistula
4- To prevent buildup of normal or abnormal body fluid
5- To warn or prevent serious complications
Complications:
1- Damage to structures during insertion
2- Damage after insertion
3- Route for infection from external environment
4- Failure of drainage (Poor Drain Selection, Poor Drain Placement, Poor Post-operative
Management) or false sense obscurity
5- Pain/discomfort
6- Insufficient drainage
7- Incision dehiscence / hernia
8- Premature Removal
9- Accumulation of fluid
Types of tubes:
1- T tube
2- Foley catheter
3- NG tube
21
Part2
: Abdomen
(Acute abdomen)
#Causes of acute abdomen:
1- Most common causes:
Acute appendicitis
Acute cholecystitis
Pancreatitis
Inflammatory disease
Ectopic pregnancy
2- Other causes:
Acute Small Bowel Obstruction
Mesenteric Vascular Occlusion
Perforated Duodenal Ulcer
Acute peptic ulcer
Peritonitis
Pyelonephritis
Abdominal aortic aneurysm
3- Extra abdominal causes:
pleurisy
4- Non-surgical causes:
Diabetic ketoacidosis
Uremia
SLE
Hematological disorders
#patient with acute abdomen need:
History taking
Physical examination
Investigations
Laparoscope : to see the cause of acute abdomen + for definitive diagnosis
#Peritonitis features:
Inspection: No abdominal movement on respiration

21
Palpation: Tenderness, rebound tenderness, guarding, and rigidity.
Percussion: tenderness on percussion
Auscultation: Absence of bowel sound.
Associated: Pyrexia and tachycardia
.
#Examination of Acute Abdomen:
Inspection:
Usual inspection of the abdomen
Ask the patient to cough (this elicits pain, you may find a hernia)
Palpation: only superficial, using 1 or 2 fingers to score pain;
Mild: tenderness
Moderate: guarding
Sever: rigidity
Auscultation for bowel sounds : rule of three (Auscultate 3 areas for 3 minutes)
Right iliac fossa for 1 minute
The right side of umbilicus for 1 minute
Lower abdomen for 1 minute
Percussion: At the end of procedure because it elicits pain that may decreases bowel
sounds.
#Investigations:
1- Investigations in acute Cholecystitis:
Hematological: TSB (total serum bilirubin) – WBC count – Alkaline phosphatase (
obstructive jaundice) – serum amylase (indicate acute pancreatitis) – GUE (general
urine examination)
Radiological: US (gold standard) – X ray ( erect and supine abdomen x-ray) – CT scan
(highly sensitive to peritonitis)
2- Biliary tree: gold standard investigations are U.S + X ray
3- Pancreatitis: gold standard investigations are CT scan + contrast test
#surgery:
Patient with acute abdomen need surgical intervention in the following conditions:
Tachycardia + Tachypnea + Hypotension + Fever + Abdominal distention
22
#Cardinal signs of some disease of acute abdomen:
1- Cardinal signs of intestinal obstruction:
Site of obstruction above the pyloric region:
1- Pain
2- Vomiting: watery and acidic
3- Distention: no distention
4- Absolute constipation: not absolute
Site of obstruction mid-intestinal region:
1- Pain
2- Vomiting: bile content
3- Distention: mild distention
4- Absolute constipation: little absolute
Site of obstruction left colon region:
1- Pain
2- Vomiting: little amount of vomiting
3- Distention: obvious distention
4- Absolute constipation: absolute
2- Cardinal signs of acute Cholecystitis:
Febrile
Nausea
Colic abdominal pain if there is biliary obstruction but if there is inflammation it will
spread to make constant referral pain
Post-meal pain (30 min)
Fatty meal will increase the pain
The pain is sudden, severe, continuous, radiated to tip of right scapula, aggravated
by moving and coughing, relieved by analgesics and the site is right hypochondrium.
3- Cardinal signs of chronic Cholecystitis:
Some signs of acute cholecystitis
Distention
Fibrosis seen in imaging studies like U.S
Thickness
4- Cardinal signs of acute on chronic Cholecystitis:
Picture of acute abdomen
Note:
Types of abdominal pain:
1- Constant griping pain: could
contracting pain, it is due to
inflammation
2- Colic pain: due to muscular
tube obstruction
Note:
The constipation could be
relieved easily without surgery
but the obstruction very
difficult to be relieved
23
Fever
Hypertension
Abdominal pain
Loss of apatite
Signs of septicemia
5- Cardinal signs of diverticulitis:
The most common type of diverticulitis is sigmoid diverticulitis and it is caused by fiber
full food and it is acquired type of diverticulitis and not occur in developing countries
Lead to inflammation acute abdomen
Diarrhea
Bleeding per rectum
Nausea
Pain
Vomiting
6- Cardinal signs of sigmoid volvulus:
Sign of acute abdomen
Acquired or congenital
Occur in developing countries
7- Cardinal signs of Meckel's diverticulum:
Congenital
Sign of acute abdomen
Pain in right iliac fossa
Nausea
Vomiting
8- Cardinal signs of Acute appendicitis:
History: Nausea, vomiting, central abdominal pain which later shifts to the right iliac
fossa
Examination
:
Peritonitis features, palpable mass in the right iliac fossa. Rovsing’s sign
(Palpation in the left iliac fossa produces pain in the right iliac fossa). Iliopsoas test
(for Retroileal appendicitis, iliopsoas abscess): Ask the patient to flex the thigh
against the resistance of your hand; a painful response indicates an inflammatory
process involving the right psoas muscle.
9- Cardinal signs of Perforated peptic ulcer with acute peritonitis:
History: history of dyspepsia, ulcer disease, NSAIDs or corticosteroid therapy.
Vomiting at onset associated with severe acute onset abdominal pain, previous
Examination: Peritonitis features

24
10- Cardinal signs of Acute pancreatitis:
History: alcohol abuse/cholelithiasis, Anorexia, nausea, vomiting, constant severe
epigastric pain
Examination: Peritonitis features, epigastric tenderness, periumbilical bruising
(Cullen’s sign) or loin bruising (Grey
–Turner’s sign, fever)
11- Cardinal signs of Ruptured aortic aneurysm:
History: history of vascular disease and/or high blood pressure. Sudden onset of
severe, tearing back/loin/abdominal pain.
Examination: Shock and hypotension, pulsatile, tender, abdominal mass,
asymmetrical femoral pulses, Grey–Turner’s and Cullen’s sign.
12- Cardinal signs of acute mesenteric ischemia:
History: Anorexia, nausea, vomiting, bloody diarrhea, constant, abdominal pain,
previous history of vascular disease and/or high blood pressure
Examination: Atrial fibrillation, heart failure, asymmetrical peripheral pulses, absent
bowel sounds, variable tenderness
and guarding
13- Cardinal signs of Intestinal obstruction:
History: Colicky abdominal pain, vomiting, distention and constipation
Examination: Surgical scars, hernias, mass, distension, visible peristalsis, increased
bowel sounds
Murphy's sign
is tested for during an abdominal examination; it is performed by asking the patient
to breathe out and then gently placing the hand below the costal margin on the right
side at the mid-clavicular line (the approximate location of the gallbladder). The
patient is then instructed to inspire (breathe in). Normally, during inspiration,
the abdominal contents are pushed downward as the diaphragm moves down
(and lungs expand). If the patient stops breathing in (as the gallbladder is tender and,
in moving downward, comes in contact with the examiner's fingers) and winces with a
'catch' in breath, the test is considered positive. In order for the test to be considered
positive, the same maneuver must not elicit pain when performed on the left
side. Ultrasound imaging can be used to ensure the hand is properly positioned over
the gallbladder.
25
(Acute appendicitis)
Definition: defined as an inflammation of the inner lining of the vermiform appendix that
spreads to its other parts. Despite diagnostic and therapeutic advancement in medicine,
appendicitis remains a clinical emergency and is one of the more common causes of acute
abdominal pain.
Causes: Obstruction of the appendiceal lumen by:
lymphoid hyperplasia secondary to inflammatory bowel disease (IBD)
infections (bacteria, parasites)
fecal stasis and fecaliths
foreign bodies
neoplasms (carcinoid tumor)
strictures
swollen peyer's patches
History of acute appendicitis (clinical presentation)
1- shifting pain: start as visceral pain (around the umbilicus) then shift to parietal pain (
in the R.I.F )
2- Sudden onset of sever pain in the R.I.F (( in 1/3 of patients ))
3- Nausea
4- Vomiting (( one or two times per day – and usually start after the pain ))
5- Loss of appetite
6- Diarrhea or constipation (( in 18% of patients ))
Investigations:
Acute appendicitis is diagnosed from history and clinical examination but we do
many investigations for differential diagnosis and complications
There are a lot of investigations in acute appendicitis like: WBC count, General urine
analysis, X-ray, U.S, C.T scan, Laparoscopy and pregnancy test.
Note:
There are two types of pain:
1- Viseral pain: ((generalized pain – not localized)) occur in the epigastric, suprapubic
regions and around the umbilicus.
2- Parietal or somatic pain: ((localized pain – not generalized)) occur when an inflamed
organ touch the parietal peritoneum. Like pain in the right iliac fossa (R.I.F)
26
1- Patient with R.I.F pain: we do WBC count and General urine analysis for differential
diagnosis of 1- Acute appendicitis 2- Urinary Tract Infection (UTI) 3- Stone formation
4- irritation of the urinary bladder wall
2- Use Ultra Sound (U.S) for differential diagnosis of:
ectopic pregnancy
overian cyst in female, and presented with: menstrual irregularity
salpingitis and hirsutism and obesity.
ureteric stone
Pyelonephritis in male
3- Use Abdominal X ray (A.X.R) for differential diagnosis of:
Intestinal obstruction
ureteric stone
Pyelonephritis (radio-opaque)
4- Use C.T scan for differential diagnosis of:
Tumor
Perforated appendix
Perforated viscous
Pancreatitis
5- Use laparoscopy ((diagnostic and therapeutic)) for differential diagnosis of:
Gynecological complications
Advantage for obese
Clinical signs of patient with acute appendicitis:
1- Rovsing's sign: pressure on left iliac fossa and the pain will appear in Right iliac fossa
2- McBurney's sign: deep tenderness at the McBurney's point
3- Obturator sign: pain due to contact between the inflamed appendix and obturator
muscle.
4- Psoas sign: The pain results because the psoas borders the peritoneal cavity, so
stretching (by hyperextension at the hip) or contraction (by flexion of the hip) of the
muscles causes friction against nearby inflamed tissues like appendix.
5- Aaron's sign: is a referred pain felt in the epigastrium upon continuous firm pressure
over McBurney's point. It is indicative of appendicitis
هام جدا
27
6- Blumberg's sign: A positive sign is indicated by presence of pain upon removal of
pressure on the abdominal wall. It is very similar to rebound tenderness
7- Cough sign: increase pain with cough because of parietal pain
8- Shifting pain
9- Shifting tenderness: pressure on left iliac fossa and the pain will appear in Right iliac
fossa
10- R.I.F Tenderness
11- Rebound tenderness: lead to sever pain after sudden release of the hand above
appendix
12- percussion tenderness: percussion on McBurney's point lead to sever tenderness
13- guarding sign: The tensed muscles of the abdominal wall automatically go into
spasm to keep the tender underlying tissues (apeendix) from being disturbed.
Right iliac fossa pain differentials:
1- For child:
Acute appendicitis
Cystitis (UTI)
Torsion of testes
Intestinal obstruction
Enteritis
Intussusception
Mesenteric lymphadenoma
Meckel's diverticulum
Gastroenteritis
2- For young adult male:
Acute appendicitis
Acute pyelonephritis
Ureteric stone
Cancer
UTI
Inflammatory bowel disease
3- For female:
Ectopic pregnancy
UTI
Complication of pregnancy
Sigmoid
4- For elderly:
Cancer
Note:
To differentiate between acute
appendicitis and Meckel's diverticulum:
rotate the baby to the left side then
exam the pain if the pain is still in the
R.I.F it is acute appendicitis but if the
pain disappear it is Meckel's
diverticulum
both have the same clinical characters
Note:
To differentiate between acute
appendicitis and Mesenteric
lymphadenoma : via shifting pain
Umbilicus
Ant. Sup. Iliac spine
McBurney's point = base
of the appendix
28
Inflammatory bowel disease
Sigmoid
Surgery:
1- General anesthesia
2- Appendectomy
3- Type of surgery: conventional and laparoscopic
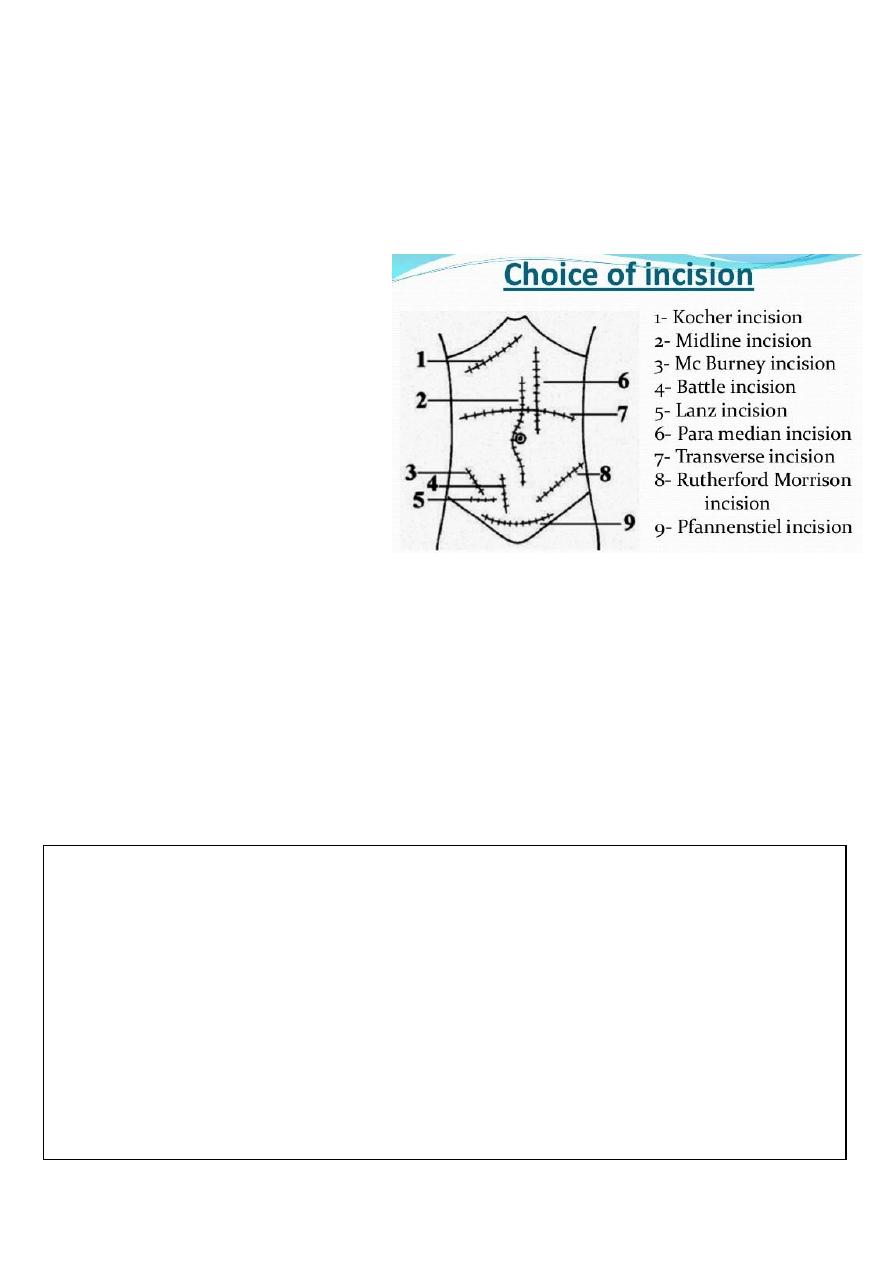
4- Types of incisions:
Lanz incision
Gridiron incision
Muscle splitting incision
Rutherford incision
Middle line surgery
Right para-median
5- Size of incisions is 6-7 cm
Complications of acute appendicitis:
1- Appendicular abscess
2- Appendicular mass
3- Generalized peritonitis
4- Perforation:
Predisposing factors: delayed diagnosis – immunocompromised patient – two
extreme of age.
Site: occur in the tip of appendix lead to appendicular abscess pelvic
abscess generalized peritonitis.
Need surgery + drainage of abscess + aspiration under U.S guide.
Note:
Ochsner sherren regimen:
Is an expected management giving to apatient with appendicular mass
Aim: treatment of infections + pain relief + fluids and electrolytes supplement
Period: 48-72 hours
The regimen is: Nothing by mouth + fluids and electrolytes supplement + antibiotics +
analgesics + chart ( contain pulse measure + pressure measure + general examination +
measure input and output of fluids )
For more information visit: http://www.medimag.com.ng/ochsner-sherren-regimen-
and-appendix-mass/

29
Differential diagnosis of appendicular mass:
1- T.B peritonitis
2- Hematoma
3- Crohn's disease
4- Tumor
5- Abscess
6- Ovarian cyst
7- Ectopic kidney
8- Lymphoma
9- Tissue mass
Differential diagnosis of appendicular mass (other source)
1- appendicular mass
2- ileocaecaltuberculosis (hyperplastic type)
3- Intussusception
4- Crohn`s disease
5- carcinoma caecum
6- Tubo-ovarian mass, e.g. abscess
7- undescended testis
8- transplanted kidney
9- ectopic kidney
10- psoas abscess
11- non-Hodgkin lymphoma
Complications of appendectomy:
1- Septicemia
2- D.V.T
3- Inconel hernia
4- Respiratory complications
5- Intestinal obstruction
6- Infections
31
(Intestinal obstruction)
#Types of intestinal obstruction:
1- complete (total blockage of the lumen) - incomplete (partial blockage)
2- small intestine obstruction - large intestine obstruction
3- Dynamic (mechanical) obstruction - Adynamic obstruction (paralytic ileus) due to loss
of transmission of peristalsis and hypokalemia
4- Acute intestinal obstruction - Chronic intestinal obstruction
#Causes of intestinal obstruction
:
1- In neonate:
Congenital anomalies (like congenital pyloric stenosis)
Atresia
Hirschberg disease
Hernia
Family history of intestinal obstruction
2- In infant:
Meconium ileus
Perforated anus
Hirschberg disease
Causes of Dynamic (mechanical) obstruction
Extra-mural
Intra-mural
Intra-luminal
Adhesions
Bands
Internal hernia
external hernia
tumor
Tumor (cancer-lymphoma)
Strictures
Inflammatory disease like
Crohn's disease
Fecal material
Foreign bodies
Bezoars
Gallstone
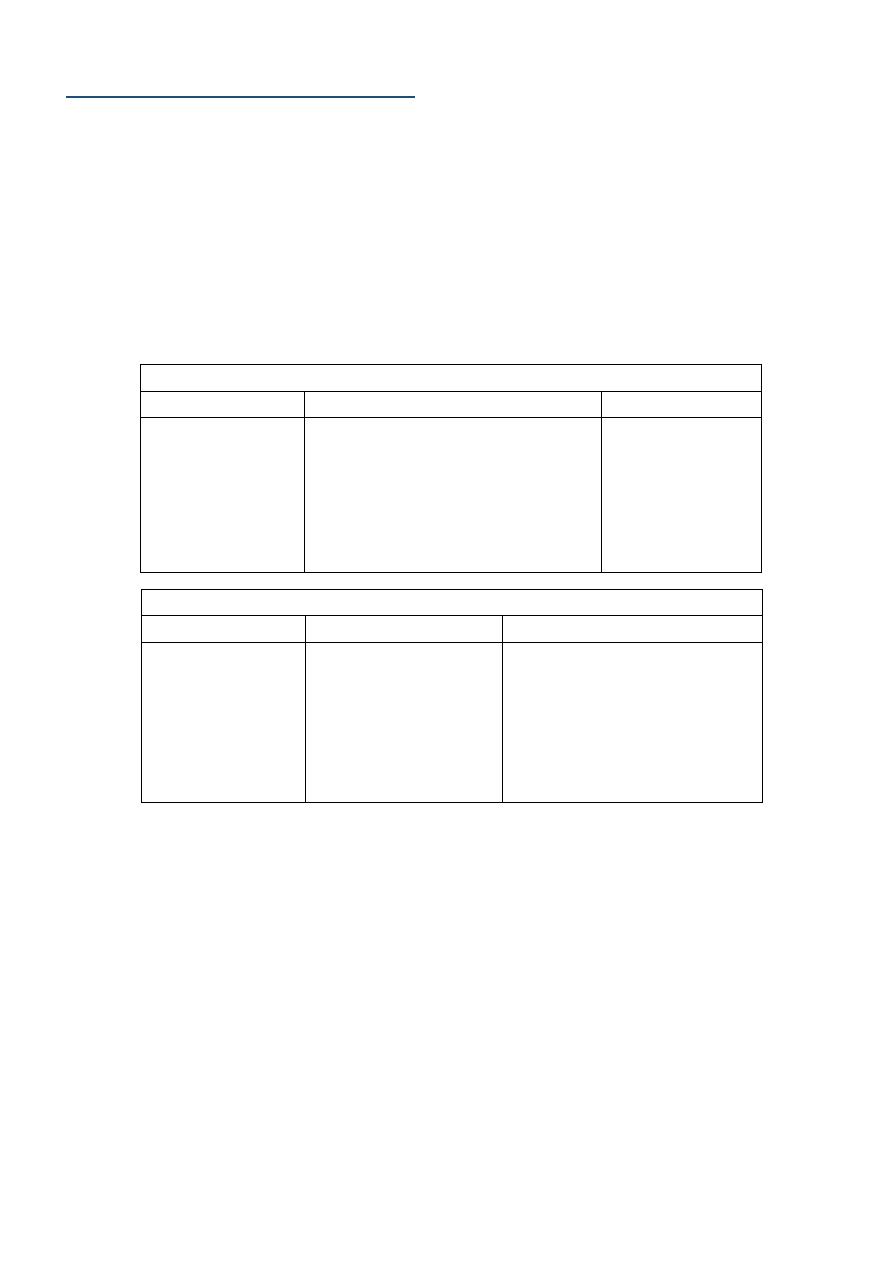
Acute and chronic intestinal obstruction
Duration
Site
Symptoms
Acute: less than
2 weeks
Chronic: more
than 2 weeks
Acute: in the small
and large intestine
Chronic: only in the
large intestine
Acute: start as abdominal
pain then vomiting then
distention then constipation
Chronic: start as
constipation then distention
then pain then vomiting
31
Congenital anomalies
3- In children:
Volvulus
Tumor
Adhesion
Intussusception
4- In adult and elderly:
Hernia
Tumor
Adhesion
#Clinical features of intestinal obstruction:
1- Vomiting: start green, yellow then feculent color. More proximal obstruction lead to
increase vomiting and distention
2- Abdominal pain: colicky (in paralytic ileus is less pain)
3- Abdominal distention: Gas Nitrogen (produced by swallow of air and bacterial
fermentation) Fluid (produced by secretions and dietary source)
4- Constipation : but in some condition there is diarrhea
5- Extra-intestinal features: fever – dehydration – electrolyte disturbance
#Management of intestinal obstruction:
resuscitation-investigations-treatment
=Resuscitation:
I.V fluid (wide bore cannula): ringer lactate ((lower intestinal obstruction is acidic but
upper intestinal obstruction is alkaline so not give ringer lactate in upper intestinal
obstruction like gastric outlet obstruction and give normal saline with potassium
instead))
Blood sample for investigations
Nasogastric tube
Foley's catheter
Antibiotics: against gram negative and anaerobic bacteria
Analgesia
Note: هام
Intestinal obstruction with diarrhea:
Richter's hernia
Gallstone ileus: called ball valve mechanism يوم مسدود ويوم إسهال– called
aerobilia (air in the biliary tree)
Pelvic abscess
Fecal impaction
Mesenteric vascular occlusion
32
Check vital signs
=Investigations:
X-ray:
Erect and supine supine give earlier diagnosis
See air/fluid level 5cm is normal – above 5 cm is abnormal
Small intestine: central – small diameter- diameter more than 6 cm
Large intestine: peripheral – large diameter – diameter more than 8 cm. if more
than 10 cm it indicate perforation.
=Treatment:
Treat underlying cause
Surgery
#Closed loop syndrome:
Obstruction in two sides
May lead to dilatation and green vomiting and perforation
Occur in colon: CA colon or incompetent ileocecal valve
Occur in small intestine: volvulus of small intestine
Occur in sigmoid volvulus (anti clock wise obstruction)
#Sigmoid volvulus:
Resuscitation: like that of intestinal obstruction
Deflating rectal tube
Sigmoidoscope (diagnostic and therapeutic)
#Intussusception:
Occur in the ileum – cecum – colon
Occur from 9 months of age to 10 years
Clinical features: vomiting – abdominal pain – blood per rectum – palpable
abdominal mass – lethargy – red current jelly – scream
Etiology: idiopathic – viral gastrointestinal pathogens like rotavirus, echovirus,
reovirus
Diagnosis: history – physical examination– radiographic studies – abdominal plain X-
ray – abdominal films – U.S – barium or air contrast enema (gold standard –
therapeutic and diagnostic)
Differential diagnosis: rectal prolapse
Treatment: IV line + nasogastric tube + IV antibiotics + hydrostatic barium enema or
pneumatic enema + surgery
Note:
Sigmoid colon: is the
commonest site of
volvulus, tumor and
diverticulosis
because of its shape
and fecal material
storage

33
# Causes of chronic intestinal obstruction (Intestinal Pseudo-Obstruction
)
1- The 3 most common associations are the following:
Trauma (especially retroperitoneal)
Serious infection
Cardiac disease (especially myocardial infarction and congestive heart failure)
2- Other conditions commonly associated with colonic pseudo-obstruction are:
Recent surgery (abdominal, urologic, gynecologic, orthopedic, cardiac, or
neurologic)
Spinal cord injury
Old age
Neurologic disorders
Hypothyroidism
Electrolyte imbalances
(hyponatremia ,hypokalemia ,hypocalcemia,hypercalcemia ,
orhypomagnesemia )
Respiratory disorders
Renal insufficiency
Medications (eg, narcotics, tricyclic antidepressants, phenothiazines,
antiparkinsonian drugs, and anesthetic agents)
Severe constipation
3- The condition may also observed in patients with the following:
Intestinal hypoperistalsis syndrome
Megacystis megacolon
Amyloidosis
GI carcinoma
Guillain-Barré syndrome
Multiple myeloma
Alcohol abuse
#Mesenteric vascular occlusion:
Causes: High cholesterol - Blood clots - Cocaine and methamphetamine use –
surgery
Symptoms include: abdominal pain and tenderness - bloating or a sense of
fullness – diarrhea – nausea – vomiting - fever
Diagnosis: CT – U.S – MRI - MRA (magnetic resonance angiography) -
Arteriogram
34
Treatment: Angioplasty + Lifestyle adjustments + medications (antibiotics -
vasodilator drugs - heparin or warfarin)
#Hypokalemia:
Potassium normal range : 3.5-5.2 mmol/L
Causes: Decreased intake - Shift into cells - Extra-renal losses (GIT) - Renal losses -
Spurious
Clinical manifestations: Neuromuscular disorders (Muscle Weakness, flaccid
paralysis, respiratory arrest) GIT (nausea , constipation paralytic ileus)
Acquired Nephrogenic DI ( Polyuria,polydypsia) Heart (Arrhythmias, Postural
hypotension)
ECG Changes: Flat T-wave - appearance of U wave - Cardiac arrest
Management: treat underlying cause + correction of alkalosis + Oral KCL Tabs
#Notes#
History of jaundice:
1- Obstructive jaundice due to benign cause: painful + fluctuating jaundice like
gallstone
2- Obstructive jaundice due to Malignant cause: painless + constant jaundice like
cancer
How to ask patient about bowel motion:
Ask about: frequency – color – amount – content – odor – timing – blood – mucus)
Diarrhea
:
More than 3 bowel motion/day or more than 300 mg/day
It is important to ask the patient if there are changes in the bowel motion
because it differs from person to person
Early morning diarrhea = malignancy (like CA colon )
35
(Splenomegaly)
Causes
:
1- Infections:
Viral: infectious mononucleosis
Bacterial: brucellosis – syphilis – T.B
Protozoal: malaria - kala azar
2- Hematological: leukemia, lymphoma
3- Metabolic: Gaucher's disease
4- Vascular malformations
5- Liver disease: cirrhosis
6- Portal hypertension
7- Hemolytic anemia
8- Tumor and secondary metastasis
Indications of splenectomy:
1- Trauma
2- Hereditary spherocytosis
3- Portal hypertension
4- Malignancy (CA stomach - lymphoma)
Complications of splenectomy
1- Respiratory complications:
Basal atelectasis: cough after splenectomy due to lung collapse
Plural effusion
Empyema
2- Increase susceptibility to infections like
H.influenzae (pneumonia) , N.meningitidis (meningitis)
3- D.V.T
4- Thrombocytosis ( can lead to thrombosis )
5- Acute gastric dilatation
6- Bleeding
7- Injury to adjusent organs
8- Pancratits
9- Septicemina ( by streptococcus – haemophilus )
Note:
There is conservative
management instead
of splenectomy
Note:
After splenectomy
give antibiotics and
vaccines
36
37
Part3
: Chest
(Chest Trauma & Chest Tube)
((Chest Trauma))
#Mechanism of trauma of the chest
Penetrating trauma
o causes:
1. Bullet injury (the tract is straight) (may result in shock wave and cavitation)
2. Shell injury (the tract is zigzag like)
3. Stab wound
o penetrating trauma (has inlet only) perforating trauma (has inlet and outlet)
o Penetrating trauma may lead to laceration of the lung, pneumothorax,
hemothorax, heart injury.
Blunt trauma
o Crushing chest wall between two blunt objects
o Causes:
1. RTA (Road Traffic Accident)
2. FFH (Fall From Height)
3. Blunt object trauma
o Blunt trauma may lead to Ecchymosis, bruising, rib fracture, flail chest,
pneumothorax, hemothorax.
Blast trauma
o It is due to explosion of a bomb, which lead to formation of intense positive
wave followed by negative wave collectively known as ~Shock Wave~ which may
result in an injury to the micro-structures in the lungs as alveoli and capillaries.
o May lead to:
1. Interstitial hemorrhage
2. Intra alveolar hemorrhage
3. Diffuse capillary hemorrhage
4. lung edema
5. ARDS (acute respiratory distress syndrome)
6. Pneumothorax and hemothorax

38
#Components of chest trauma
Chest wall (skin – subcutaneous tissue – intercostal muscles – neurovascular bundle –
ribs) may lead to open pneumothorax or fracture of the ribs.
Parietal and visceral pleura may lead to pneumothorax, hemothorax, empyema.
The lung may lead to laceration of the lung, pneumothorax, hemothorax, collapse,
respiratory distress, hemoptysis.
The heart and great vessels may lead to massive bleeding, massive cardiac
tamponade, constrictive pericarditis, ventricular aneurysm, VSD, ASD, valve injury.
Thoracic duct may lead to chylothorax (milky color) which need surgery and
conservative management (bed rest + no fatty meal + total parenteral nutrition TPN).
Esophagus may lead to mediastinitis and sepsis.
Trachea and bronchus may lead to tracheal laceration, rapture of the trachea,
rapture of the bronchus, pneumothorax, emphysema, hemoptysis, obstruction.
Diaphragm may lead to herniation of abdominal content into the chest and it is
diagnosed by barium meal.
Spinal cord may lead to injury in the spinal cord.
#Effects of chest Trauma
Chest trauma may effects:
1-Breathing
2-Blood flow
Thoracic inlet includes structure that pass into the chest medial to the clavicle
Thoracic outlet includes structures that pass out of the chest superlateral to the
clavicle.
Trauma to the chest could cause:
o Insult without fracture Manage by: Analgesia, breathing, high flow O2 (ABO).
o Fracture of ribs If only one or two ribs treat conservatively (ABO).
o Flail chest mostly treated conservatively but may need chest tube or
mechanical ventilation in severe cases, with/without surgical intervention.
o Loss of part of the chest wall needs surgical intervention.
o Lung injury:
a. Contusion: hazy area on CXR
b. Direct injury: damage to tissues that may cause bleeding.
o Cardiac injury especially if the trauma associated with fractured sternum
(indicated severity of trauma); could be assessed by;
1-Trponin I and CK-MB monitoring
2-ECG, suspect:
a-BBB (bundle branch block) b-1st degree heart block c-tachyarrhythmia.
Most commonly associated with tamponade
39
#General principles in treatment of chest trauma
Resuscitation from shock restoration of blood volume and relief of pain
Restoration of normal cardiopulmonary function:
o Relief of upper airway obstruction (remove forging body + lateral position +
tracheostomy)
o Decompression of pleural cavity (drainage by chest tube)
o Relief pericardial tamponade
o Stabilization of chest movement (in flail chest injury)
Prevention of infection
#Management of Chest Trauma in general
ABC
Blood tests, blood gases, blood group and matching and preparing 2 pints of blood.
CXR (chest X-ray)
ECG and Echo (Esophageal echo is the best investigation to reveal cardiac injury).
Endoscopy: to check for esophageal perforation, also you can use water soluble
contrast which can be swallowed + fluoroscopy.
Bronchoscopy: to look for bleeding or damage to bronchi.
#Patient with chest trauma is treated by
85% by chest tube
15% by thoracotomy
#Indication of Thoracotomy:
Initial gush of 1500 cc of blood or 250cc/hr. for the first 3 hours (Suggests continuous
bleeding which needs repair)
Heavy air leak in pneumothorax (suggests bronchial injury)
Thoracic duct injury
Late complication like: Empyema, Fibrosis, Lung abscess, Broncho-pleural fistula.
Esophageal injury
Tracheal fracture: causes stridor, managed by thoracotomy and repair.
Great vessel injury or cardiac injury
o Most pt. with aortic injury don’t reach ER (95%) only 5% reach with high risk of
death during surgical intervention.
o If aortic injury is small causing an aneurysm its presentation will be late and
managed by elective thoracotomy and repair.

41
((Chest Tube))
#General information
It is closed drain.
To isolate the atmospheric pressure from the pleural pressure the tube should be
placed in an underwater seal of about 200-300 cc of normal saline, so the air can`t
return back into the pleural cavity.
We do under water seal and not emptying the pleura directly and completely to
avoid rapid lung expansion.
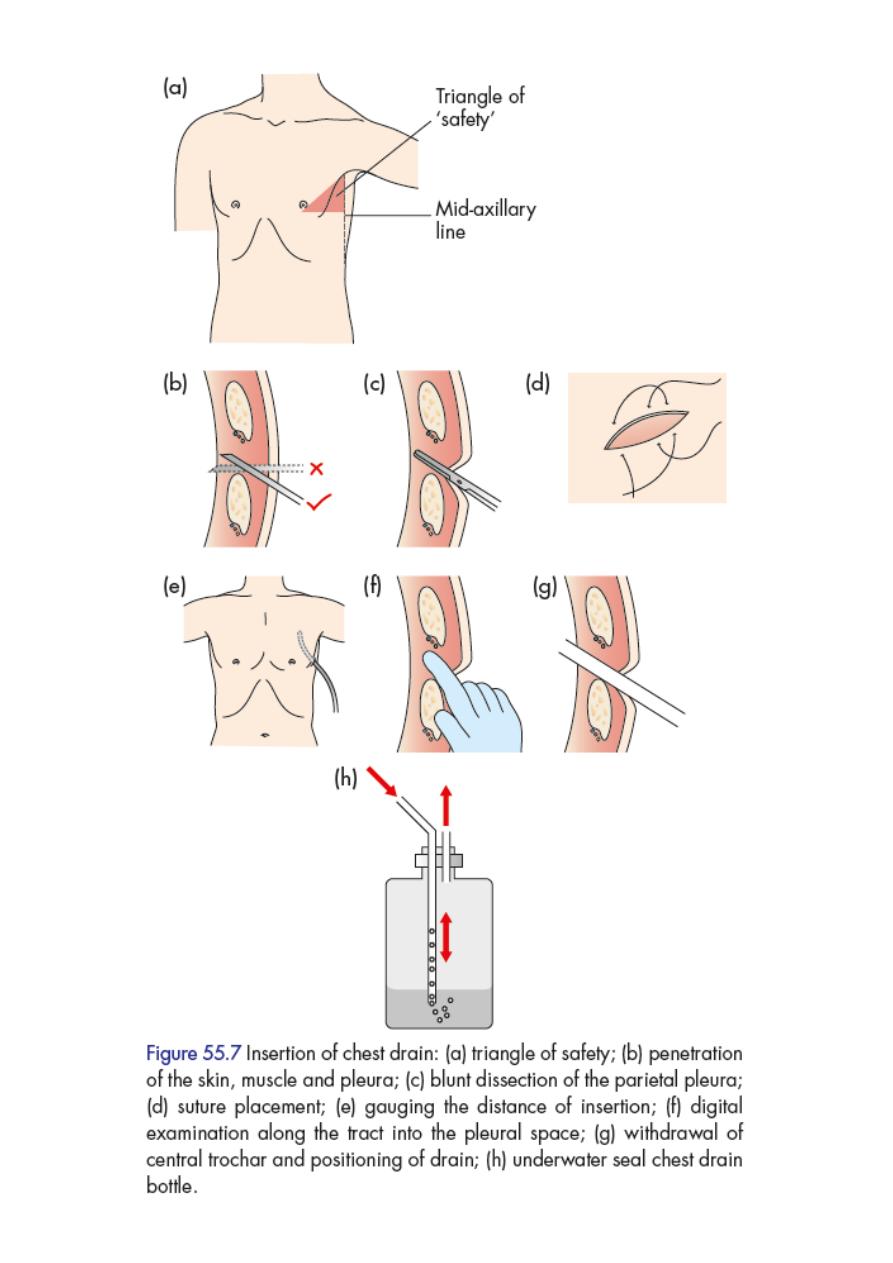
In aspiration and insertion of chest tube we should insert in the upper border of
the rib to avoid injury to neurovascular bundle.
#Indications
Complex pneumothorax
Pneumothorax on positive-pressure ventilation
Hemothorax
Large plural Effusion
Empyema
Chylothorax
#Contraindications
Bleeding diathesis
Coagulopathy
#Site of insertion
It is inserted in the Triangle of safety which has the following boundaries:
1. Anteriorly posterior border of pectoralis major muscle.
2. Posteriorly anterior border of latissimus dorssi.
3. Inferiorly (base) the 5
th
intercostal space.
4. Superiorly (apex) the base of axilla.
A line is made in the triangle at the mid-axillary line and the tube is inserted at the
level of this line in the 4
th
or 5
th
intercostal space.
41
#We should know the followings:
Contents of the tube and bottle.
Amount of the contents.
If the chest tube is functioning or not:
o Swinging movement of fluid in the tube, if not ask the patient to cough.
o Air bubbles.
#when we should remove chest tube?
A-In pneumothorax
1. If there is no air bubbles or air leak.
2. If there is no swinging movement.
Clump the tube for 24 hr. and do X-ray, if the lung expanded open the clump and ask
pt. to cough if there are air bubbles leave the tube , if not, remove it.
B-In hemothorax or chylothorax or pyothorax
No discharge for 24-48 hr.
C-In effusion
If there is Small amount of fluid we can remove the tube (large amount
not
remove it).
Depend on the fluid collection in the bottle and the X-ray.
Normal plural fluid is 50-100 cc.
#Complications
bleeding
Organ perforation
Intercostal neuralgia
Tube blockage
Subcutaneous emphysema
Re-expansion pulmonary edema
Local infection and empyema
>> For more information see the following videos <<
http://www.muhadharaty.com/lecture/1677
http://www.muhadharaty.com/lecture/1678
42
43
(Death in Chest Trauma)
Causes of early death in patient with chest trauma:
Upper airway obstruction
Massive hemothorax
Tension pneumothorax
Open pneumothorax
Flail chest injury
Pericardial tamponade
(1) Upper airway obstruction
#Causes
Direct injury leads to edema, hematoma or blood clots obstructing the airways.
Foreign body aspiration
Secretions in unconscious patients
Tongue swallowing
External compression
#Management
Position: left lateral position with traction of the angle of mandible anteriorly
Sucking: any forging body or secretion by the sucker
High flow O2
Endotracheal tube: placement from the mouth
Tracheostomy with use of endotracheal tube: when approach from the mouth is not
possible due to fascial trauma or other causes.
Laryngoscope: sometimes used to open the upper airway.
(2) Massive hemothorax
When 1000-2000ml (or 1.25-1.5 L in other reference) of blood is collected in the pleural
cavity initially
It is called massive hemothorax.
#Causes
Laceration of the lung
Injury of great blood vessels
Note:
Simple pneumothorax:
Simple symptoms or may
be asymptomatic
Mostly occurs in patient
with Marfan`s syndrome
Normal vital sign
44
Injury to intercostal artery
Injury to bronchial artery
#Management
Give blood + I.V fluid.
Put the chest tube.
Do Thoracotomy done if there is continuous bleeding of 300 cc of blood in 3-4
hours, thoracotomy will stop the bleeding.
Note: 85% of all chest trauma need chest tube only.
15% of all chest trauma may need thoracotomy.
(3) Tension pneumothorax
Presence of air under tension (high pressure) in the plural cavity due to one way valve
mechanism. It lead to lung collapse and pressure on the other lung and mediastinal
structures and push them. It comprise inferior and superior vena cava (lead to shock) and
pressure on right and left atrium (lead to hypotension).
#Causes
Trauma
Disease or (spontaneous)
o Tuberuclous
o Non-Tuberculous:
a. Rupture of emphysematous bullae (diameter= 2 cm or more)
b. Rupture of emphysematous bleb
c. Rupture of solitary lung cyst
d. Honeycomb lung or cystic lung
e. Idiopathic in young smoker patient
f. In patient with Marfan's syndrome (usually simple pneumothorax that progress
to tension)
#Diagnosis:
History:
o The patient present with severe sudden dyspnea
o Sometimes chest pain
o Healthy young patient
o Previous attack
Clinical examination:

45
o Hyper-resonant on percussion.
o Asymmetrical chest movement.
o Tracheal deviation and mediastinal shifting toward opposite side.
o Vocal fremitus (tactile fremitus) is decreased or absent.
o Absence of breath sounds.
o Hypotension or shock (CVP is 10-15mmHg) and engorged neck veins due to
compression of large vessels that impair venous return.
Do Needle aspiration
#Management
Needle puncture or needle decompression (wide bore needle): in the 2
nd
intercostal
space at the level of mid-clavicular line, converting it into open pneumothorax
allowing air to escape into atmosphere thus temporarily relief the tension
pneumothorax.
Chest tube: with underwater seal is done after needle decompression.
Thoracotomy: according to indication.
(4) Open pneumothorax
Associated with external trauma (Sucking wound) the air enter through the defect in the
chest wall during inspiration and go out with expiration. Patient presented with dyspnea.
#Management
Closure of the wound by either suturing or gauze
Chest tube
(5) Flail chest injury
Characterized by paradoxical movement of segment of the chest with respiration:
In inspiration
the lung go in (collapse)
In expiration
the lung go out (expansion)
#Cause:
Blunt or penetrating trauma lead to Fracture of ribs:
1-Multiple (more than 3 ribs)
2-Successive
3-Fracture at least in two sites in each rib
#Management
Rest and immobilization (no movement of the chest).
Intubation may be needed with high flow oxygen.
46
Fixation of the segment by :
o Plaster
o Traction
o Suturing the ribs by using steel wire
o Thoracotomy
Chest tube
Mechanical ventilation (IPPV) in severe cases (anesthesia + endotracheal tube).
#Flail chest may be accompanied by
Interruption in respiration, leads to respiratory compromise.
Lung contusion.
Disease in the lung, mediastinum, pneumothorax, hemothorax.
(6) Pericardial tamponade
It is characterized by presence of blood in the pericardium.
Acute form of pericardial effusion clinically characterized by Becks triad:
o Hypotension
o Engorged neck veins (elevated JVP)
o Muffled heart sounds
To improve the diagnosis
do CXR Echo study of the heart
#Cause:
Trauma.
Infection mainly in Iraq due to TB, or other causes as uremia or hypoproteinemia.
Disease (pericarditis, bacterial, inflammatory, malignant, TB) with presence of fluid in
all of these diseases.
#Amount of blood:
Acute tamponade 100 cc of blood
Chronic tamponade 700-1000 cc of blood (chronic tamponade occur in
pericarditis due to TB, renal failure, liver failure, heart failure, tumor)
#Management
Pericardiocentesis with echo guidance. (using needle or catheter for few days)
Thoracotomy if bleeding is continuous or if recur
.
In chronic case: do aspiration + continuous catheter in the pericardium take blood
for investigations (culture + chemical)
47
(The Breast)
#General information
The breasts are modified sweat glands.
Composed from lobes lobules lactiferous duct
Pigmented skin covers the areola and the nipple, which
is erectile tissue.
The openings of the lactiferous ducts are on the apex of
the nipple.
The nipple is in the fourth intercostal space in the mid-
clavicular line, but accessory breast/nipple tissue may
develop anywhere down the nipple line (axilla to groin).
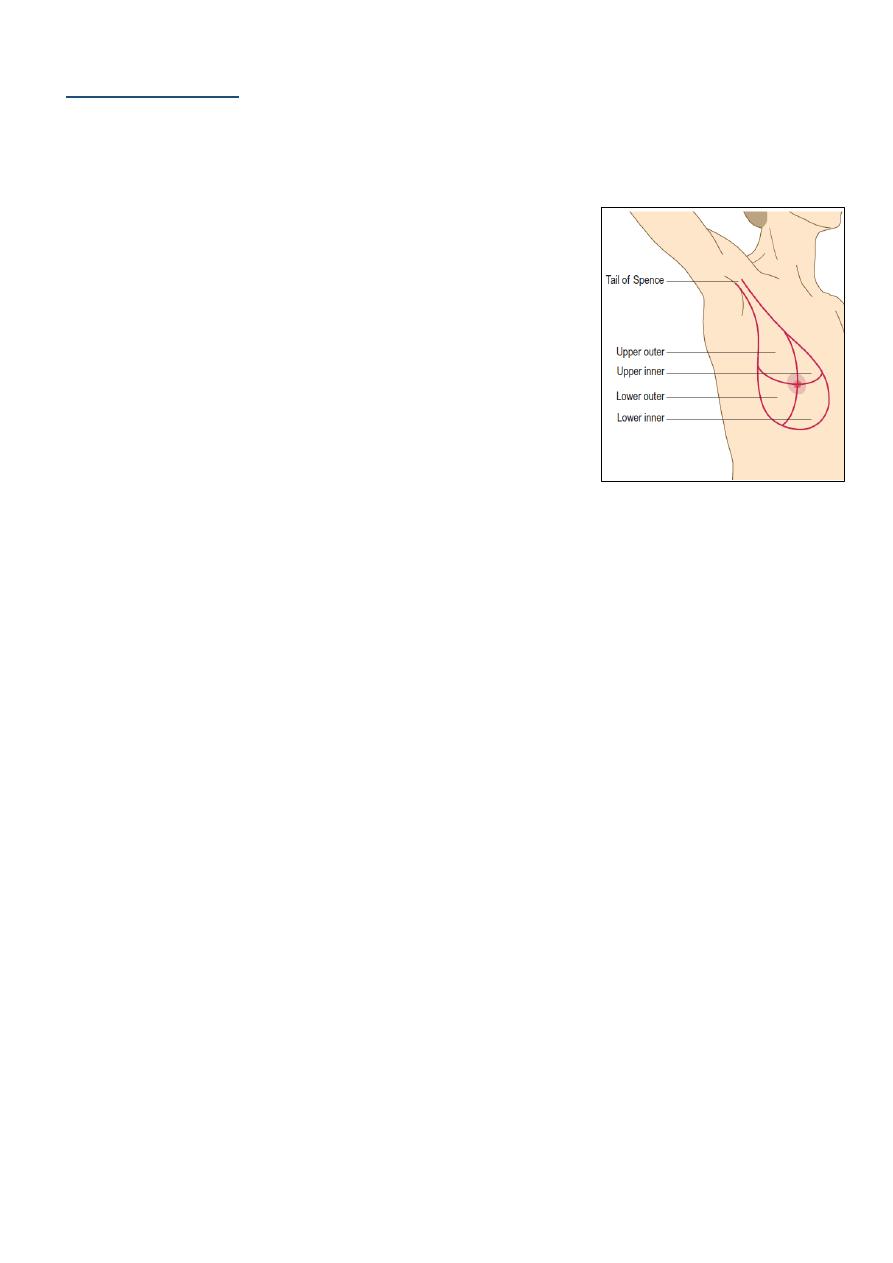
The adult breast is divided into the nipple, the areola and four quadrants, upper and
lower, inner and outer, with an axillary tail projecting from the upper outer quadrant.
upper lateral quadrant the most quadrant that affect by malignancy
99% of breast cancer occur in female and only 1% in male (more aggressive in male)
The breast is bounded by the clavicle superiorly, the lateral border of the latissimus
muscle laterally, the sternum medially, and the infra-mammary fold inferiorly.
Conservative breast surgery radiotherapy + removal of the breast.
If there is metastases to the spine there will be tenderness and pain on raising the leg
and absent knee jerk due to damaging effects on the nerves.
#Lymph nodes
Lymph drainage of the breast:
o 70% to the axillary LN
o 20% to the supraclavicular LN or along the internal mammary vessels
o 10% to the abdominal LN
Axillary L.N divided into five groups:
o Anterior (Pectoral)
o Posterior (Subscapular)
o lateral
o Medial (Sub-clavicular)
o Central (intermediate)
Surgical levels of axillary L.N:
o Level I bottom level, below the lower edge of the pectoralis minor muscle
o Level II lies underneath/posterior the pectoralis minor muscle
o Level III above/medial the pectoralis minor muscle

48
When there is breast cancer and axillary L.N affected means metastatic and
systemic disease.
Sentinel L.N (first L.N adjacent to the cancer) to see if there is metastases make
injection of methylene blue or radioactive substance then take biopsy and examine
it.
#History
Questions:
o How long have symptoms been present?
o What changes have occurred?
o Is there any relationship to the menstrual cycle?
o Does anything make it better or worse?
Age:
o young patient (15-25 years) fibro-adenoma
o middle age (25-40 years) ANDI (Aberrations in the normal development and
involution) due to hormonal changes like prolactin and sex hormones
o old age (more than 40 years) cancer of the breast
Questions of lump (Cause - first symptoms - onset - duration - associated symptoms
– progression - multiplicity)
Presentation: discharge – lump – skin changes
History of trauma: lead to fat necrosis which appears as a mass
History of breast surgery and biopsy
Family history: 5-10% of breast cancer run in family
Risks that increase the probability of breast cancer occurrence:
o Number of menstruation (increased number more risk)
o Nulliparous (more risk)
o Unmarried (more risk)
o Lactation (protective)
Drug history: estrogen – progesterone
Obesity: increase the level of estrogen
Sex related hereditary diseases
Menstrual history:
Menarche, menopause, changes during the menstrual cycle,
pregnancies, lactation.
Social history: smoking – alcohol – diet (fat, animal meat, low fiber, pickles)
#We should examine the following for complete breast exam:
Both breasts
The axilla
The supraclavicular LN
The abdomen for a-Hepatomegaly b-Ascites

49
Do PR to check Douglas pouch for metastasis
Examine the spine for tenderness
Do knee jerk and straight leg raising test
#Breast clinical examination
1. Settings:
Position: The patient must be undressed to the waist, resting comfortably at 45
degree. Ask her to rest her hands on her thighs to relax the pectoral muscles.
Other positions: supine or setting 90 degree
Explain what to do to the patient
Always examine the patient with nurse or relatives
Clean your hand – good light – humidity – temperature
2. Inspection:
Face the patient and look at the breasts for: asymmetry, local swelling, dilated veins
skin changes (lump, ulcer, puckering, peau d’orange, scar, fungation), nipple changes
(discoloration, discharge, destruction, depression, deviation, displacement,
duplication)
Nipple discharge: one or two breast, single or multiple duct, type of discharge (serous,
blood, mixed)
Ask the patient to press her hands firmly on her hips to contract the pectoral muscles
and inspect again for invisible lumps.
Ask her to raise her arms above her head and then lean forward to expose the whole
breast and exacerbate skin dimpling.
Elevate the breast with your hand to uncover dimpling overlying a tumor which may
not be obvious on inspection.
Examine the arm
3. Palpation:
Ask her to lie with her head on one pillow and her hand under her head on the side to
be examined.
Hold your hand flat to her skin and palpate the breast tissue, using the palmar surface
of your fingers to compress the breast tissue firmly against her chest wall.
Begin with the symptomless side, or you can examine both sides simultaneously.
View the breast as a clock face. Examine each ‘hour of the clock’ from the outside
towards the nipple, including under the nipple. Examine all the breast tissue.
Compare the texture of one breast with the other.
Define the characteristics of any mass:

51
o Characteristics: site, size, shape, surface, edge, pain, temperature (raised in
inflammation)
o Content: Fibro-adenoma (rubbery) Cyst or glactocele (soft) Cancer (hard)
o Levels of the mass: attach to the muscle or skin (pinch the skin out), mobility,
tethering (mass sometimes fixed and sometimes mobile or mass move separately
from the skin)
o TNM staging (from lecture)
Relations to structures beneath the breast is tested by holding the mass between your
thumb and forefinger with the patient’s hands on her hips. Ask her to push her hands
against her hips (contract pectoralis muscle) and then push the examiners shoulder
(contract serratus anterior). If the lesion is less mobile, it is either fixed or tethered.
Examine the axillary tail between your fingers and thumb as it extends towards the
axilla.
Palpate the nipple by holding it gently between your index finger and thumb. If the
patient complains of discharge, try to express it by massaging the breast towards the
nipple & gently pressing the nipple to uncover any discharge. Note the color and
consistency of any discharge, along with the number and position of the affected
ducts. Test any nipple discharge for blood using urine-testing sticks.
4. Examine the supraclavicular fossa, looking for any visual abnormality.
5. Palpate the regional lymph nodes (axillary and neck)
6. Examination of axilla: right axilla examine by left hand and vice versa (we should make
relaxation of the patient hand)
7. Examine site of malignancy: back (spine tenderness) abdomen (hepatomegaly – ascites)
8. Do P.R examination: for krukenberg tumor
9. Back examination: metastasis of breast cancer to venous plexus
#Triple assessment of the mass
1- History and Examination
2- Radiology
Ultrasound: mass, cyst, abnormality
Mammography: it is X-ray, see soft tissue of the breast, do to 35 years old
patient or older, if done to young patient it will make more dense tissue (less
soft tissue), it has lateral view and medial oblique view, it used to see if there is
malignancy in the breast
3- Biopsy: incisional biopsy, excisional biopsy, fine needle aspiration, whole organ
biopsy
4- Extra: MRI, CBC, Others
51
#Notes
Clinical presentation of breast symptoms:
1. Painful lump (Abscess (postpartum or lactational), cyst, periductal mastitis (duct
ectasia), fibroadenosis, very rarely Ca)
2. Painless lump (Carcinoma, cyst, fibro-adenoma, fibroadenosis)
3. Pain without lump (mastalgia) cyclical or non-cyclical breast pain, very rarely
carcinoma.
Causes of Inversion or retraction:
1. Cancer slit like inversion of the nipple
2. Genetic
3. Puberty
4. Fungal infection
Retraction: circumference (benign or congenital) slit like retraction (cancer)
MOST common cause of nipple discharge is lactation
Discharge could be either:
1. Milky or serous (normal)
2. Bloody or pinkish in papilloma (most common cause) or carcinoma.
3. Purulent due to infection
4. Greenish, brownish or black in duct ectasia.
Question-Difference between fixity and tethering?
1. Fixity: When a lesion is fixed to the skin, it has spread into the skin and cannot be
moved or separated from it.
2. Tethering: A tethered lesion is one which is more deeply situated and distorts the
fibrous septa (the ligaments of Astley Cooper) that separate the lobules of breast
tissue. This puckers the skin, but the lesion remains separate from it and can be
moved independently.

53
(Vascular Trauma)
#General information
Vascular trauma trauma to the arteries or veins
Consequence ischemia or bleeding
Bleeding:
o Arterial: jetting + bright color
o Venous: continuous + dark color
o Concealed: internal in the cavities like pleura, peritoneum, pericardium
o Revealed: external
Unrecognized and untreated bleeding lead to loss of organ (death) or gangrene
Ischemia:
o Convert aerobic respiration to anaerobic lead to metabolic disturbances lead to
inflammatory response (SIRS)
o Signs of ischemia (5Ps) Pain – Pale – Paralysis – Paresthesia – Pulseless
o Acute ischemic limb is due to trauma, thrombus, embolus
o Chronic ischemia is due to ischemic disease like atherosclerosis lead to some
symptoms like claudication
Unrecognized and untreated ischemia lead to limb lose, stroke, bowel necrosis,
multiple organ failure
Clot (outside the vessel) Thrombus (inside the vessel)
Source of embolus:
o Heart (in atrial myxoma, septic embolus from infected endocarditis)
o Fat embolus
o Air embolus
o Tumor
Virchow’s triad:
o Endothelial dysfunction or damage
o Stasis
o Hypercoagulability
Venous injury, leading to bleeding and thrombosis.
#Mechanism of vascular trauma
1- Laceration:
As bullet or shell or stab wound.
Could be complete or partial cutting of the vessel.

54
o Partial: more bleed, less spasm, more dangerous, lead to retraction (increase
bleeding) // partial cut lead to expanding pulsating hematoma.
o Complete: less bleed, more spasm, less dangerous, contraction, spasm of both
end of the artery reduce bleeding or thrombus reduce bleeding or retraction
reduce bleeding
Partial cut produce more profuse bleeding than complete cut (Why?):
Because when there is complete cut, the proximal and distal ends of the vessel
undergo vasospasm and retraction in addition to compression from surrounding
tissues, while in partial cut the retraction of the vessel will increase the cut opening
and thus increases the bleeding. In addition bleeding into the surrounding tissues will
lead to formation of hematoma which it is pulsatile in partial cut (due to
communication with vessel lumen) and usually not pulsatile in complete cut.
2-Blunt:
As crush injury
Lead to thrombosis ischemia acute ischemia of the limb.
A blunt trauma to the artery cause injury to the intima that can end in:
o Exposure of the sub-endothelial collagen lead to activation of clotting mechanism
and thrombosis that lead to obstruction of blood flow lead to ischemia of the
distal tissues.
o The intima itself my flap and act as a valve in the artery, obstructing blood flow.
Pseudo-aneurysm: it is a pulsatile mass of clot surrounded by membrane or
surrounding tissue, it result from arterial hemorrhage within contained hematoma.
Artero-venous fistula:
o result from injury to adjacent artery and vein
o which may lead to subsequent rapture or cardiovascular compromise
o lead to dilated veins and thick wall veins and increase venous pressure
o lead to thrill and bruit
#Diagnosis of vascular trauma
1- Clinical diagnosis:
Hard sign of vascular injury:
o Pulsatile bleeding
o Expanding hematoma
o Absent distal pulses
o Cold, pale limb
o Palpable thrill
o Audible bruit
55
Absence of hard sign of vascular injury virtually excludes the presence of vascular
trauma.
Sometimes there is no hard signs but the patient has ischemia ((risk of old age,
history of bleeding))
Presence of hard signs mandates immediate operative intervention ((Time is only
6 hours)) if late lead to irreversible ischemia.
Signs that mean the limb is not dead yet: capillary refill + movement of the limb.
2- Investigations:
Doppler US (called duplex Doppler)
Angiography (done by catheterization)
CT angiography (less invasive, give I.V contrast)
#Management of vascular trauma
1- Arrest bleeding:
Pressure: especially venous bleeding.
Position: depend on the site of bleeding specific positions will reduce bleeding.
Packing: by using our hands or fingers! Or by using bandages or tourniquet, in
areas where bandage or tourniquet can’t be used as below the angle of mandible
we can use folly’s catheter, by inserting it in the wound as deep as possible then
inflate its balloon which will provide pressure on the bleeding vessel.
*** Time limit for tourniquet is 30-45 min, to prevent ischemia, and also we have
to write the time of application of the tourniquet so when the pt. reach the
hospital or special center, the doctor who will receive him will know the time of its
application.
2- I.V line:
Sample (blood group, cross matching).
Assessment of vital signs (PR, BP, urine output).
Volume replacement (give amount of fluid that keep blood pressure between 90
and 100 mmHg to avoid ischemia and hypertension.
Give normal saline or ringer lactate
Give blood and clotting factor as necessary are administered to correct
hypothermia, acidosis, coagulopathy, restore perfusion
Not give large amount of fluid to avoid:
o increase blood pressure
o dislodgment of clot or thrombus lead to bleeding
o hemodilution (affect clotting mechanism)
o hypothermia
o electrolyte dilution

56
3- Surgical treatment:
Vascular clamp: We apply tourniquet proximal to the arterial injury, then we close
the proximal and distal ends of the injured artery and stop bleeding, after this we
remove the tourniquet to allow blood flow through collateral vessels to the distal
tissue.
Trimming of the artery.
Saphenous vein graft: if there is gap, and we should reverse the direction of
saphenous vein because it contain valves, use saphenous vein because it is
available without infection and low complications.
End to end anastomosis: use prolyn (non-absorbable monofilament suture).
Not do anastomosis to irreversible ischemia to avoid ischemia perfusion
syndrome:
o Activation of cellular and humeral immunity
o Collection of toxic material like lactic acid and potassium
o Lead to cell edema
#Compartment syndrome:
Ischemia leads to cell membrane dysfunction and thus causes efflux of electrolytes
(mainly potassium) from the cells into surrounding tissues, thus increases the
osmolarity extracellularly leading to shifting of fluid into the interstitium, which lead
to formation of edema which compress the vessels more and causing more ischemia.
Clinical features:
o Severe pain
o Tenderness
o Weak or no pulse
o Tense calf area
o Homan's sign
Diagnosis:
o Clinically
o Probe: to measure the pressure in the compartment (30 mmHg)
Management:
o Opening the compartment by fasciotomy if the intracompartment pressure more
than 30mmHg, but we do it prophylactically regardless of the pressure inside it.
#Reperfusion Syndrome:
Ischemia leads to accumulation of the following:
1-Pottasium (efflux from cells due to membrane dysfunction)
2-Lactic acid (due to anaerobic metabolism)
3-Free radicals

57
After restoring perfusion the above will enter into the systemic circulation and
affects the body tissues and mainly the heart and it may cause:
1-Cardiac Arrhythmia or Arrest
2-Metabolic acidosis
Sometimes it is asymptomatic and these changes will reverse by physiological
mechanisms of the body.
Treatment: Steroids to prevent SIRS, NaHCO3 to prevent acidosis, Ca gluconate to
reverse the effect of potassium.
#History of ischemic limb
History of claudication
o intermittent pain on waking or exercise for distinct distance (differ from patient to
other)
o Relieved by rest
o occur in the calf, thigh, buttock, may occur in the arm
o Leriche's syndrome (claudication in the buttock)
Color changes (dusky, bluish, reddish, black)
Pain, Pale, Paresthesia, Paralysis
Night pain
previous amputation or loss of limb
#Vascular examination
Steps of assessment of arterial circulation:
1- Inspection
Check pressure area (heel, medial and lateral malleolus, tips of toes, below calf
muscles)
Check hidden area (popliteal fossa, between toes see laceration, cracks)
Skin changes (color, bleeding disorders)
Wasting and deformities
Hair distribution and loss
Gangrene and ulcers
Amputation and loss of toes
Guttering vein (groove)
2- Palpation
Skin temperature (in ischemia cold limb, in infection warm limb)
Tenderness
58
Edema (pitting, non-petting)
Thrill (in vascular lesion or mass)
Capillary filling test (more than 2 sec ischemia, test in the tips of finger nail)
Burger's angle or vascular angle (patient lie supine and elevate his leg 90 degree then
it will become pale if there is ischemia) (The angle decrease in severe disease)
Capillary refilling time (done after burger's test the limb become purple dusky in
color)
Ulcer examination
Mass examination
Amputation levels of amputation:
o Toe and head of metatarsal (Ray excision)
o Trans-metatarsal
o Through ankle
o Below knee
o Through knee
o Above Knee
o Head of femur (called disarticulation)
Palpate peripheral pulses
Allen's test: To determine which artery is not dominant, so we can remove it and put
it in the heart if needed.
3- Auscultation
Listen for bruits
Measure the blood pressure and index
4- Do investigations
Random glucose
Blood urea and nitrogen
Lipid profile
Bilirubin level
Doppler or Duplex
#Examination of arterial pulses
When examining any pulse, we should know:
1-Rate
2-Rhythm
3-Volume
4-Character
5-Consistency of arterial wall
Lower limb pulses:
1-Femoral pulse; can be felt in the midinguinal point midway between symphysis
Causes of Radio-femoral delay:
1- Coarctation of aorta
2- Aortic aneurysm
3- Aortic dissection
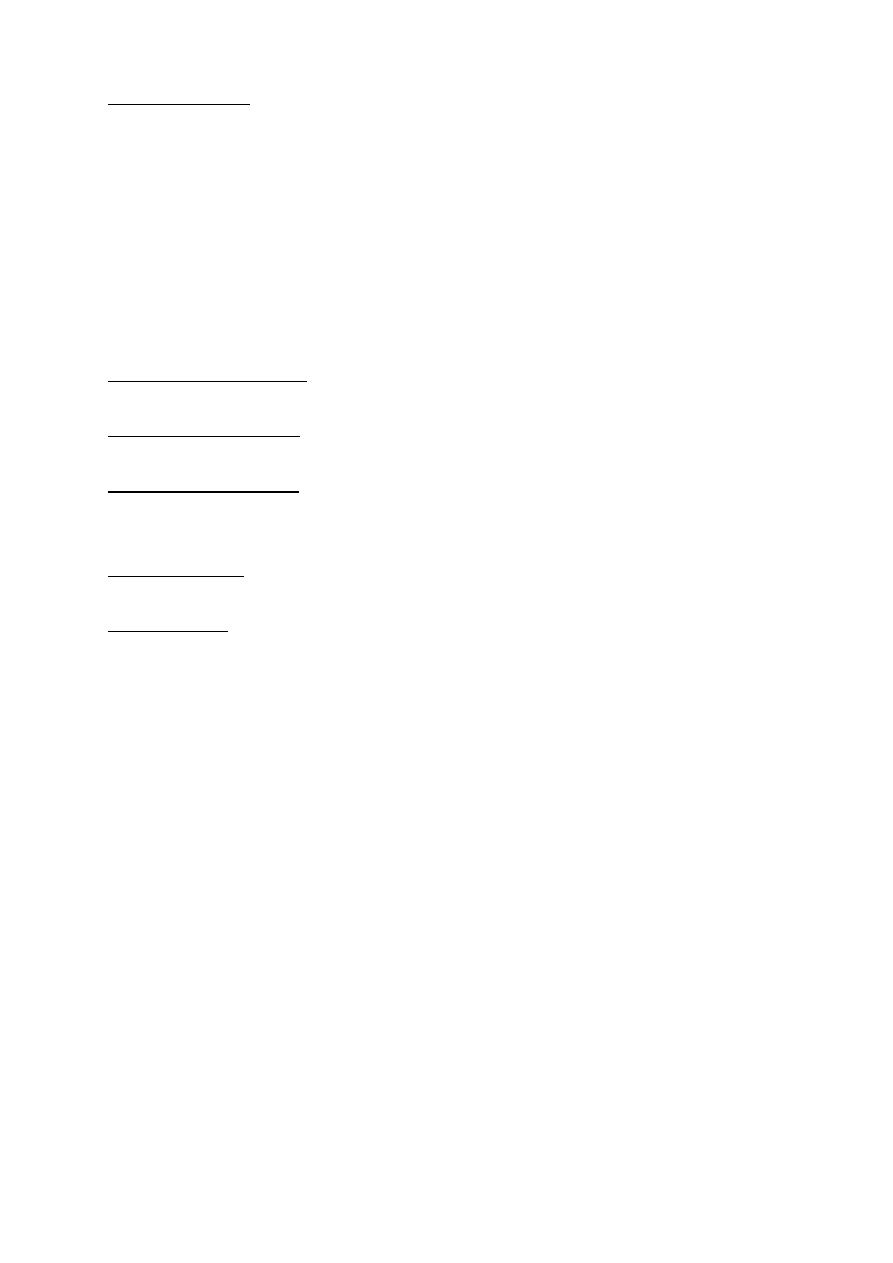
59
pubis and anterior superior iliac spine, just below the inguinal ligament.
2-Popliteal pulse; you can fell it by three maneuvers:
A- On supine position: either by flexion of knee joint 120 degree and by putting our
thumbs of the two hands on the tibial tuberosity and using other fingers palpating
deeply in the popliteal fossa. Or by hyperextension of the leg at knee joint and
pushing by one hand over the knee and palpating by the other hand.
B-On prone position.
C-Sitting position: by placing one leg over the other and look for leg movement from
pulsation (May be seen in popliteal aneurysm or in normal variant).
(Popliteal pulse usually it is hard to feel but if it is easily felt always suspect popliteal
artery aneurysm).
3-Posterior tibial artery; 2cm below the medial malleolus or midway between the
heel and medial malleolus.
4-Anterior tibial artery; at the ankle joint, midway between the medial and lateral
malleolus.
5-Dorsalis pedis artery; lies lateral the tendon of extensor halluces longus muscle or
between the 1st and 2nd metatarsal bones.
Upper limb pulses:
1-Brachial pulse; you can feel it by asking the pt. to contract his biceps and locate its
tendon, the artery lies medial to the tendon.
2-Radial pulse; lies lateral to tendon of flexor carpi radialis muscle.
#Examination of varicose veins
When there is suspected sapheno-femoral varix or perforating varices we can differentiate
between them by one of the following tests:
1-Trendelenberg test:
The patient is in supine position and the his/her legs above the level of the heart and
pressure is applied at the saphenofemoral junction and then ask the patient to stand up
and inspect if there is :
a-Refilling within 3-5 sec, this is normal
b-Refilling after 20 sec or no filling this indicate incompetent superficial veins
c-If there is rapid filling of the veins this indicate non-competent valves of the
communicating branches.
2-Tourniquet test:
Same as above, but the tourniquet is applied instead of the pressure and the same findings
are presented to determine whether the incompetency site:
1-above the knee, incompetence in the perforators of the thigh
2-below the knee, incompetence between the short saphenous and popliteal veins.
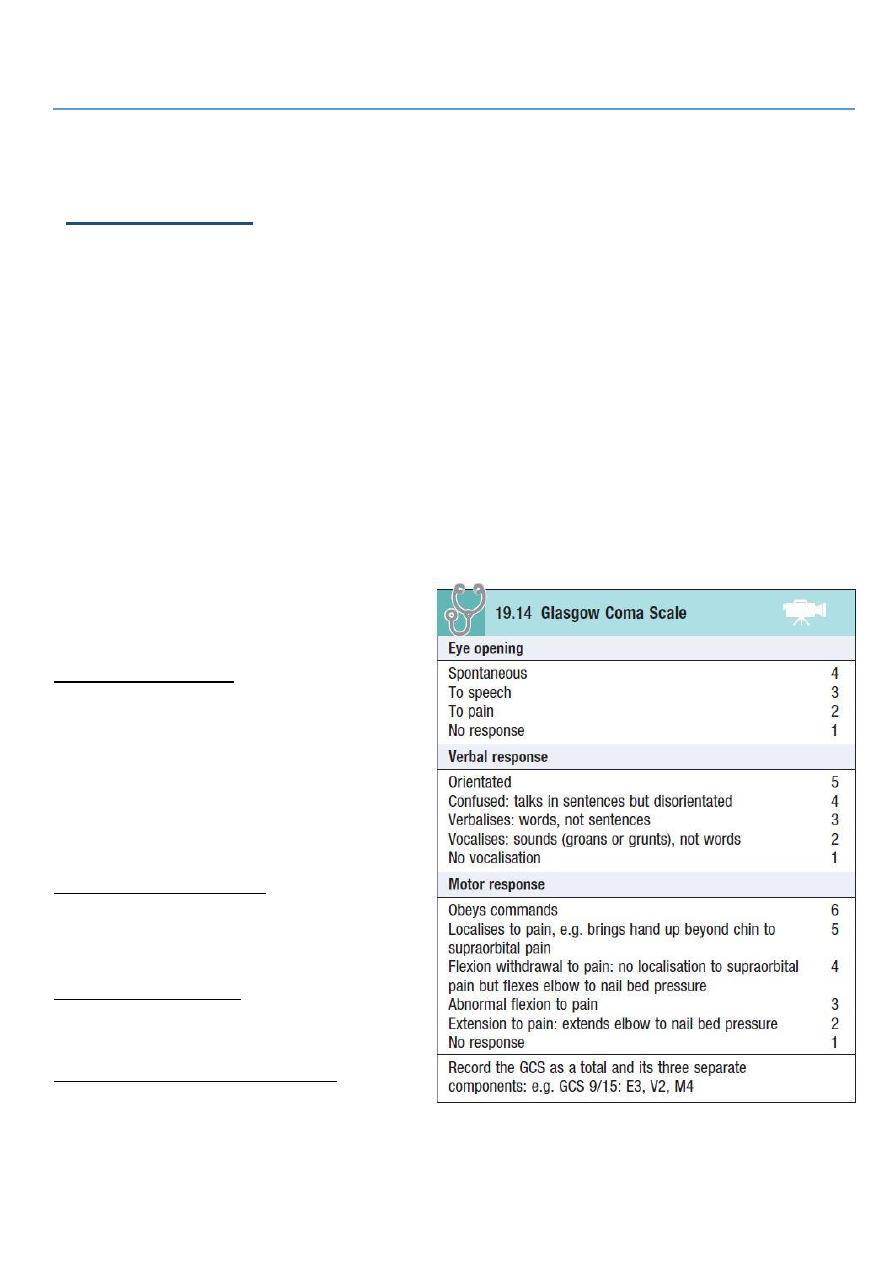
61
Part4
: Head & Neck
(Head injury)
Primary injuries: at accident (fracture, hematoma, hemorrhage).
Secondary injuries: later on:
1- Hyperthermia increase intracranial pressure.
2- Hypotension hypovolemia.
3- Seizure increase brain demand.
4- Hypoxemia.
5- Hypoglycemia.
Head injury bleeding hematoma closed space compression of brain
secondary brain insult we must do decompression.
Do the following examinations:
1- Glasgow coma scale.
2- Focal neurological signs.
3- Examination of pupil.
4- Signs of fracture at base of skull.
Glasgow coma scale:
From 0 to 3 dead person.
From 3 to 8 Severe.
From 8 to 13 moderate.
13 minimal.
14 and 15 normal.
8 or less patient need definitive
airway management.
Focal neurological signs:
Sensory examination.
Motor examination.
Reflexes examination.
Examination of pupil:
Dilatation of pupil in 3rd CN palsy.
Reactivity to the light.
Signs of fracture at base of skull:
Raccoon eye.
Bat sign.
Rhinorrhea and otorrhea.
Hemotympanum.

61
#Vital signs hypertension & bradycardia do CT scan see hematoma.
#Trait of increased intra-cranial pressure vomiting, hypertension, bradycardia.
#Indication of CT scan in head injury: (box in baily)
Low Glasgow coma scale.
Features of fracture of base of skull.
Focal neurological sings.
Deterioration of conscious level.
Age above 65.
Ante-grade amnesia.
Coagulopathy.
Seizure.
Alcoholic.
#Management:
First do primary and secondary survey of ATLS (ABCD).
High O2 flow.
Anticonvulsant foe seizure.
Glucose.
Fluid and electrolyte (but not give glucose water).
Correction of hyperthermia.
#Types of cranial hematomas:
Intra-axial hemorrhage: bleeding within the brain itself, or cerebral hemorrhage.
Extra-axial hemorrhage: bleeding that occurs within the skull but outside of the brain
tissue, falls into three subtypes:
o Epidural hematoma: rapidly accumulating hematoma between the dura mater and
the cranium.
o Subdural hematoma: occurs when there is tearing of the bridging vein between the
cerebral cortex and a draining venous sinus.
o Subarachnoid hemorrhage: is bleeding into the subarachnoid space (the area
between the arachnoid membrane and the pia mater surrounding the brain)
#Severity of head injury
Severe head injury (Glasgow Coma Scale score 3–8).
Moderate injury (Glasgow Coma Scale score 9–14).
Minor head injury (Glasgow Coma Scale score 15).
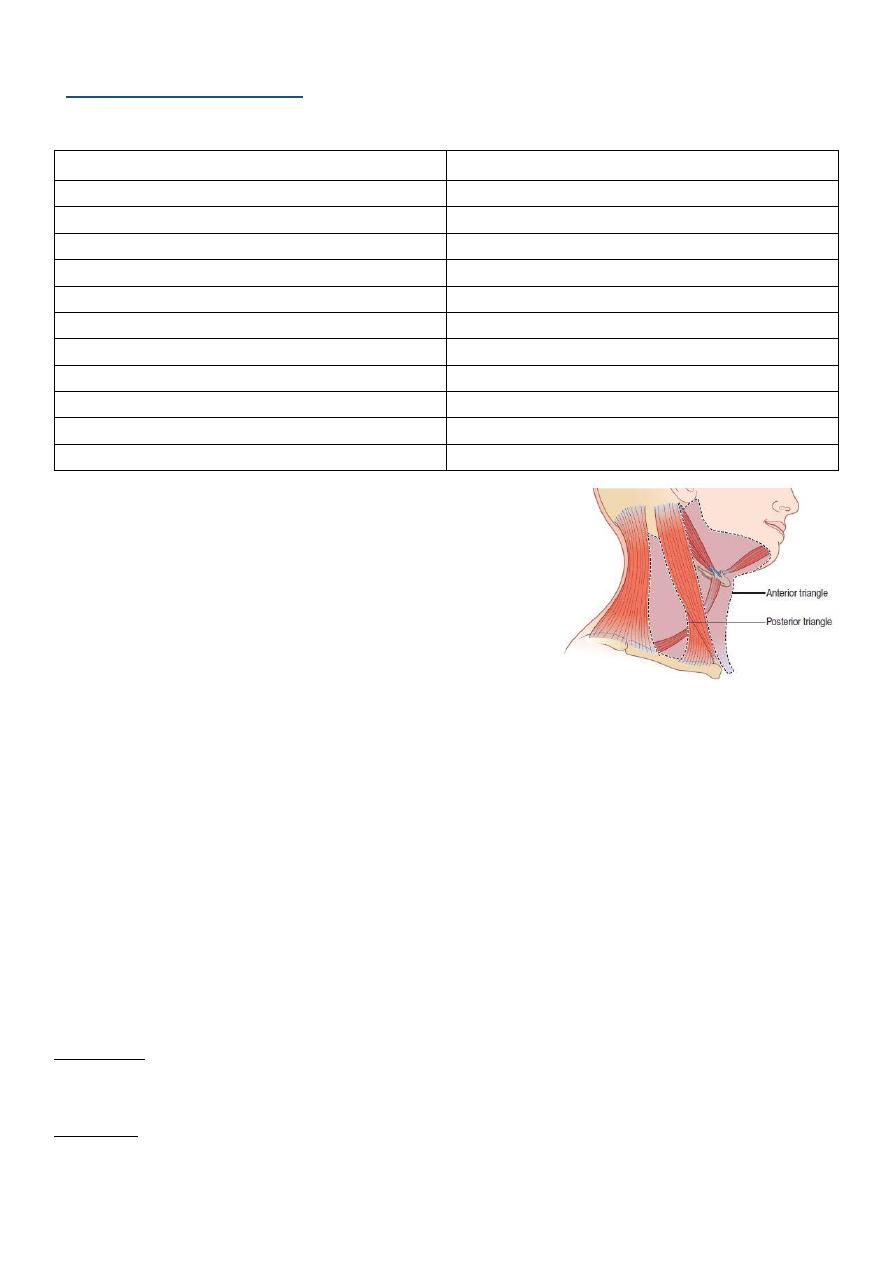
62
(Neck swellings)
Midline swelling
Lateral swelling
Thyroid enlargement
Branchial cyst
Thyroglossal cyst
Cystic hygroma
Peri-tracheal L.N enlargement
Sternocleidomastoid tumor
Single nodule in isthmus
Pharyngeal pouch
Chondroma of thyroid gland
Cervical lymphadenopathy
Sebaceous cyst
Lipofibroma
Thyroid cyst
Carotid body tumor
Mass related to skin
Thyroid enlargement
Dermoid cyst
Dermoid cyst
Lipoma
Sebaceous cyst, lipoma
Sub-hyoid bursa
Early stage of SCC
#History of neck swelling:
Onset, Duration, Possible cause, First symptom,
Associated symptoms, Progression, Persistent,
Multiplicity
Pain (10S), fever, weight change
Dysphagia, odynophagia, dysphonia, dyspnea, cough,
hemoptysis
Pain in the mouth, discomfort on eating, sore throats or ulceration, nasal discharge,
pain or blockage of the airway, pain in the throat or neck, changes in voice and
difficulty with breathing.
Family history, Personal history (Smoking, alcohol), Travel history
o Symptoms such as general malaise, fever and rigors and contact with people with
infectious diseases may indicate an infective cause of the swelling.
o Loss of appetite, loss of weight and pulmonary, alimentary or skeletal symptoms may
suggest a malignant cause.
o
Irritation of the skin associated with enlarged cervical lymph glands is often seen with
lymphoma
.
#Examination of neck swelling:
Inspection
Site (midline, anterior triangle, posterior triangle), Size, Shape, Surface, Skin over,
Surrounding, Scar, Other masses.
Palpation
Put gel on your hands.
Ask about pain.
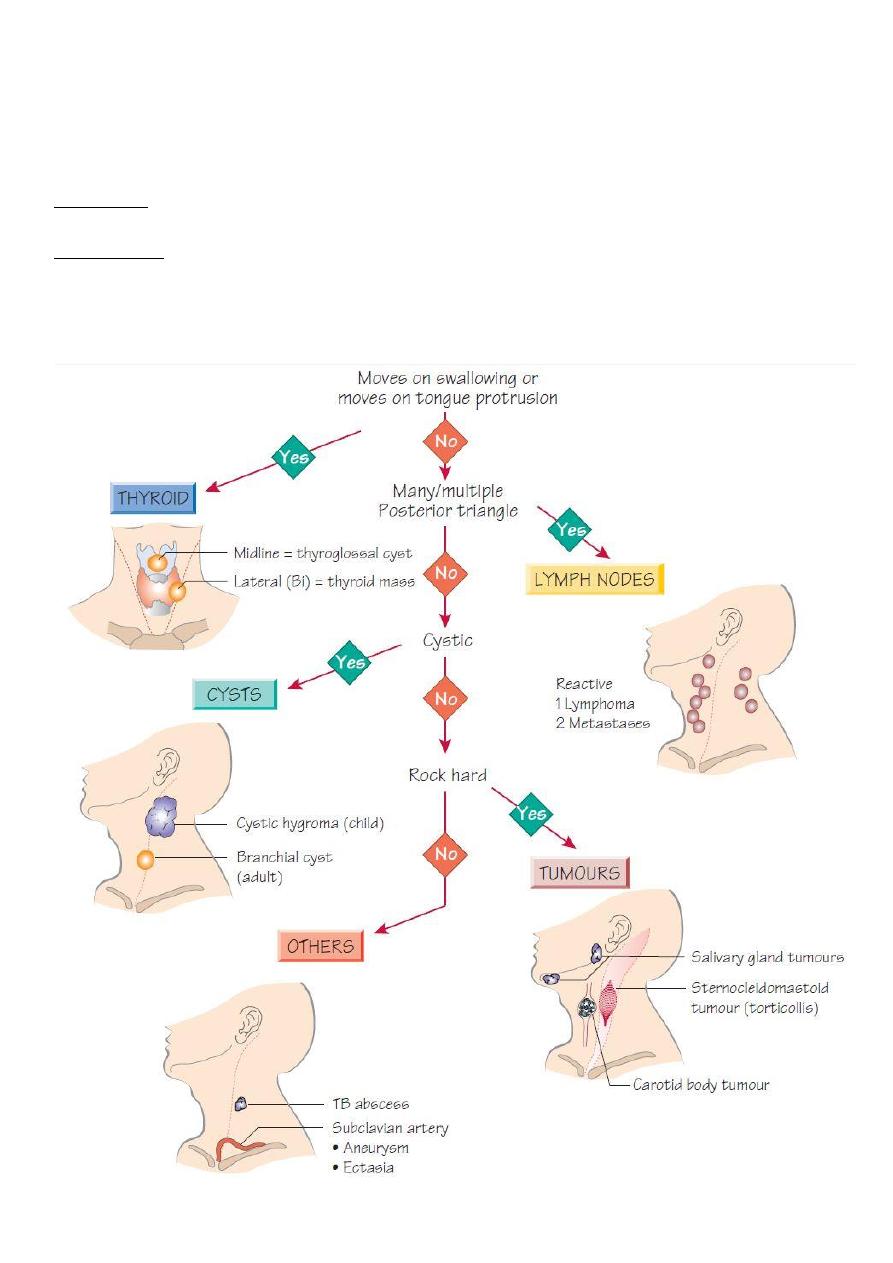
63
Start away from the mass.
Examine: temperature, fluctuation, consistency, margin, overlying skin, attachment to
underlying tissue (fixity), fluctuation, reducibility, compressibility, cough impulse (in
pharyngeal pouch), pulsation (carotid), translumination (cystic hygroma, thyroid cyst,
thyroglossal cyst).
Percussion
In retrosternal extension of goiter (percuss on sternum) become dull.
Auscultation
Thyroid bruit in thyroid tumor for example.
64
#Neck lymph nodes:
Information:
Lymph nodes in the neck are divided into anterior and posterior cervical groups:
Anterior cervical triangle is limited by the midline anteriorly, the clavicle below, and the
sternocleidomastoid muscle. It includes the submental, submandibular, jugular,
scalene, and supraclavicular lymph node groups.
Posterior cervical triangle is limited by midline, sternocleidomastoid, and trapezius
muscle. It includes the posterior cervical, post-auricular and the occipital groups.
Enlarged lymph nodes are examined for:
The lymph node areas involved.
Whether they are discrete or matted.
Approximate size of the lymph nodes.
Tender or not.
Consistency (Soft, rubbery, hard).
Mobile or fixed.
Abnormality of the overlying skin,
Levels of L.N:
Level 1 submental (1A) and submandibular (1B).
Level 2 Upper third of sternocleidomastoid.
Level 3 middle third of sternocleidomastoid.
Level 4 lower third of sternocleidomastoid.
Level 5 posterior triangle.
Level 6 peritracheal L.N.
Notes:
The anterior group is better examined from behind while the patient is sitting, and the
posterior group is examined from the front.
Examine the scalp if you find enlarged occipital and auricular L.N.
If the cervical L.N are enlarged, the axillary and inguinal L.N should be examined.
80% of enlarged L.N in adult is malignant.
Biopsy: used in case of solid mass or uncertain diagnosis.
Use FNA for diagnosis:
o If you find benign condition then do excisional biopsy.
o If you find limited malignant condition then do excisional biopsy.
o If you find extensive malignant condition then do radio or chemotherapy.
Causes of cervical lymphadenopathy:
Infection: Non-specific, Glandular fever, Tuberculosis, Syphilis, Toxoplasmosis, Cat-
scratch fever (Rochalimaea henselae)
Metastatic tumor: From the head, neck, chest and abdomen
Primary reticuloses: Lymphoma, Lymphosarcoma, Reticulosarcoma
Sarcoidosis

65
(Thyroid gland)
#Information:
Changes in hormone activity can be assessed by:
o Clinical examination.
o Measuring circulating tri-iodothyronine (T3) and thyroxine (T4) levels.
o Measuring the rate and quantity of radioactive iodine taken up by the gland.
Hormone secretion can be suppressed by:
o Iodine, which inhibits hormone release.
o Potassium perchlorate, which interferes with iodine trapping.
o Carbimazole and propylthiouracil, which inhibit the iodination of tyrosine and the
coupling of tyrosines to make thyronines.
o Destroying the gland surgically or with radiotherapy.
#Diagnosis of swellings in the neck:
History:
Is there one or more than one lump?
Where is the lump?
Is it solid or cystic?
Does it move with swallowing?
Multiple lumps: are invariably lymph glands.
A single lump:
In the anterior triangle that does not move with swallowing:
o Solid: Lymph gland, Carotid body tumor.
o Cystic: Cold abscess, Branchial cyst.
In the posterior triangle that does not move with swallowing:
o Solid: Lymph gland.
o Cystic: Cystic hygroma, Pharyngeal pouch, occasionally a secondary deposit of a
papillary thyroid carcinoma
o Pulsatile: Subclavian aneurysm.
In the anterior triangle that moves with swallowing:
o Solid: Thyroid gland, Thyroid isthmus lymph gland.
o Cystic: Thyroglossal cyst.
#Symptoms of thyroid disease:
The thyroid gland can cause two groups of symptoms and signs: those connected with the
swelling in the neck, and those related to the endocrine activity of the gland.
Neck symptoms:
o A lump in the neck: The majority of thyroid swellings grow slowly and painlessly.
o Discomfort during swallowing: This is not true dysphagia.
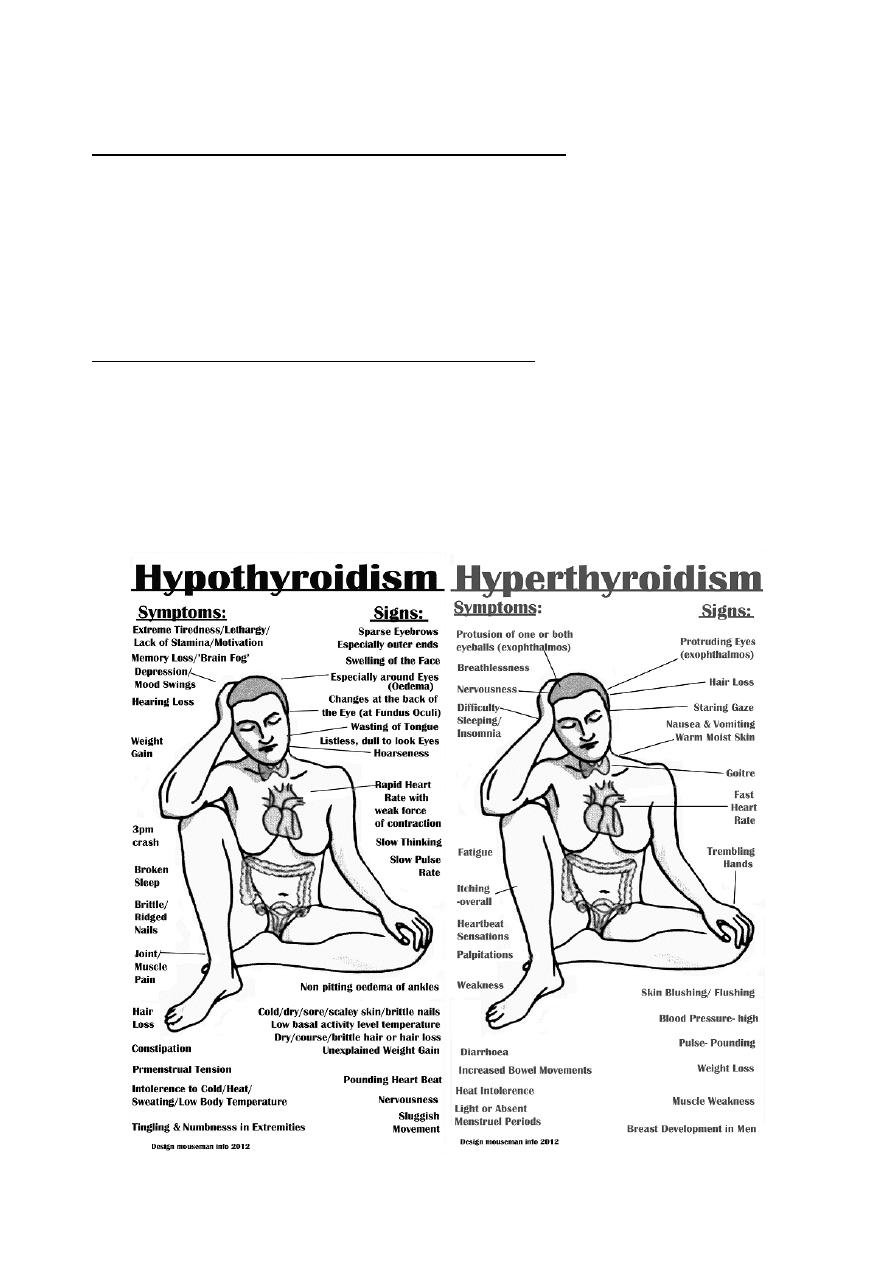
66
o Dyspnea: The whistling sound of air rushing through a narrowed trachea is stridor.
o Pain: occur in thyroiditis, Hashimoto’s disease, anaplastic carcinoma.
o Hoarseness: caused by a paralysis of one of the recurrent laryngeal nerves.
Symptoms and signs of hyperthyroidism/thyrotoxicosis:
o Nervous system: nervousness, irritability, insomnia, nervous instability, tremor of
the hands, full-blown thyrotoxic psychosis.
o Cardiovascular system: palpitations, breathlessness on exertion, swelling of the
ankles, chest pain, tachycardia, atrial fibrillation, dyspnea, peripheral swelling.
o Metabolic and alimentary systems: increase in appetite but loss of weight, diarrhea,
proximal muscle myopathies, preference for cold weather, excessive sweating,
intolerance of hot weather, amenorrhea.
Symptoms and signs of hypothyroidism/myxedema:
o Increase in weight, and constipation.
o Deposition of fat across the back of the neck and shoulders
o Slow thought, speech and action.
o Intolerance of cold weather.
o Loss of hair, especially the outer third of the eyebrows.
o Muscle fatigue.
o Dry skin and ‘peaches and cream’ complexion.

67
#History of thyroid gland:
Age, Sex, Geography, Diet, cause.
Local and general symptoms.
Duration of symptoms.
Family history.
Ask about: cold intolerance, sweating, appetite, sleep, menstrual problems.
Symptoms associated with malignancy: dyspnea, odynophagia, dysphagia, pain,
paresthesia, weight loss.
#Examination of thyroid gland:
Look at the whole patient:
o First confirm that the swelling in the neck is in the thyroid gland (move with
swallowing).
o Fast or slow movements and expressions, nervous and agitated.
o Thin or fat patient.
o What is the distribution of any wasting or fattening?
o Looks at thickness of cloths, sweating, feeling hot or cold.
o Pale or yellow lemon color occur in hypothyroidism.
o Loss of hair (in the outer third of the eyebrows) in hypothyroidism.
Look at the hands:
o Feel the pulse: Tachycardia (hyperthyroidism), bradycardia (hypothyroidism), atrial
fibrillation (thyrotoxicosis in middle or old age patient).
o Are the palms moist and sweaty?
o Is there a tremor? Thyrotoxicosis causes a fine, fast tremor.
o Look for finger clubbing, koilonychia, ecchymosis, wasting.
o Palmer erythema (hyperthyroidism) carpel tunnel syndrome (hypothyroidism).
Examine the eyes:
o Eye symptoms: double vision, pain in the eye if the cornea ulcerates.
o Eye signs: ecchymosis, bruises, sub-conjunctival hemorrhage, diversion sequence.
o Lid retraction and lid lag:
This sign is caused by over activity of the involuntary (smooth muscle) part of
the levator palpebrae superioris muscle.
Upper lid raised, Lower lid normal.
This is not exophthalmos.
o Exophthalmos:
The eyeball is pushed forwards by an increase in vretro-orbital fat, edema and
cellular infiltration.
Both lids moved away from center with sclera visible below or all-round the iris.
Because the eyes are pushed forwards, the patient can look up without
wrinkling the forehead.
In severe exophthalmos, the patient cannot close their eyelids and may develop
corneal ulceration
.
o Ophthalmoplegia:
It is weakness of the ocular muscles.

68
Caused by edema and cellular infiltration of the muscles themselves and of the
oculomotor nerves.
Particularly of the superior rectus and inferior oblique muscles (cannot look up
and out)
o Chemosis:
It is edema of the conjunctiva.
Caused by the obstruction of normal venous and lymphatic drainage of the
conjunctiva by the increased retro-orbital pressure.
Inspect the neck:
o Ask the patient to swallow: give a sip of water, all thyroid swellings ascend during
swallowing.
o Observe the general contours and surface of the swelling: the skin can be puckered,
tethered and pulled up by swallowing.
o Ask the patient to open their mouth and then to put out their tongue: If the lump
moves up as the tongue comes out, it is thyroglossal cyst.
o The neck veins will be distended if there is a mass obstructing the thoracic inlet.
o Is thyroid cartilage in the center of the neck or deviated to one side?
o See if there is scar (surgical or radiation scar).
Palpate the neck from the front:
o Confirm your visual impression of thyroid size, shape and surface, and to find out if
it is tender.
o Note the number, size, site, shape, nodularity, fixity, texture, consistency,
temperature, overlying skin for swelling.
o Can get below it or not? (Retrosternal extension).
o Check fixity by contraction of sternocleidomastoid muscle.
o Check the position of the trachea.
o Examine the position of thyroid cartilage.
Palpate the neck from behind the patient:
o Place your thumbs on the ligamentum nuchae and tilt the patient’s head slightly
forwards to relax the anterior neck muscles.
o Ask the patient to swallow while you are palpating the gland.
o With a retrosternal extension of the thyroid, it is important to assess whether you
can feel the lower border of the gland on swallowing or whether there is still a
significant extension lying behind the sternum.
o Feel the tenderness, shape, size, surface, consistency of thyroid gland or neck lump.
o Palpate the whole of the neck for any cervical and supraclavicular
lymphadenopathy.
Percussion:
o Used to define the lower extent of a swelling that extend below the suprasternal
notch.
o Percuss along the clavicles and over the sternum and upper chest wall.
o This can be done when standing in front of or behind the patient.
Auscultation:
o Listen over the swelling.
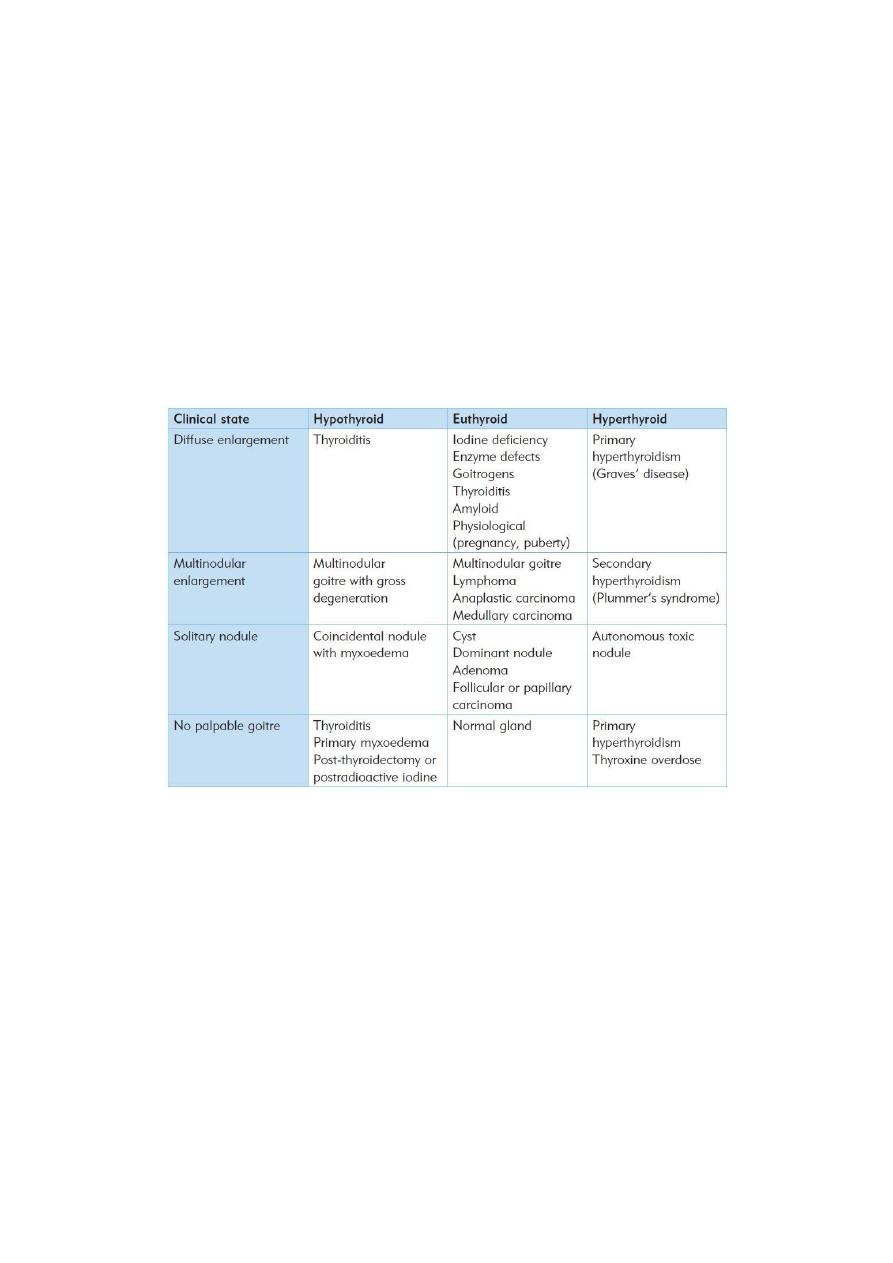
69
o Thyrotoxic and vascular glands and lumps may have a systolic bruit.
General examination:
o Examination of cardiovascular and nervous systems for any evidence of
hyperthyroidism or hypothyroidism.
o Examination of submental, submandibular, cervical, supraclavicular L.N.
o Reflexes: hyper reflexia (hyperthyroidism), slow relaxation phase (hypothyroidism).
#Examination of a patient with a goiter:
Look at the whole patient for agitation, nervousness or lethargy.
Examine the hands for sweating, tremor and tachycardia.
Examine the eyes for exophthalmos, lid lag, ophthalmoplegia and chemosis.
Examine the neck: always check that the lump moves with swallowing.
Palpate the cervical lymph glands.
Notes:
The only disease that move with protrusion of tongue is thyroglossal duct.
Cystic lesion with positive trans-lamination test is Branchial cyst.
Diffuse physiological thyroid enlargement: in growth, puberty, pregnancy need of
thyroxin increase so TSH level increase.
Previously doctors said that there is congenital ectopic thyroid tissue, but now they say
that this condition is not present, and there is acquired metastatic papillary carcinoma
instead of it.
Pretibial myxedema in grave's disease.
Proximal myopathy in hyperthyroidism.
Myxedema coma loss of consciousness due to hypoglycemia in the end stage of
hypothyroidism.
Berry's sign: In goiter, the carotid artery may be pushed posteriorly by the enlarged
thyroid and this is called displacement. When the infiltration of the carotid by the
tumor, the carotid pulse will be absent on that side. This is absent carotid pulse is
called Berry's sign. (examine it by palpation).
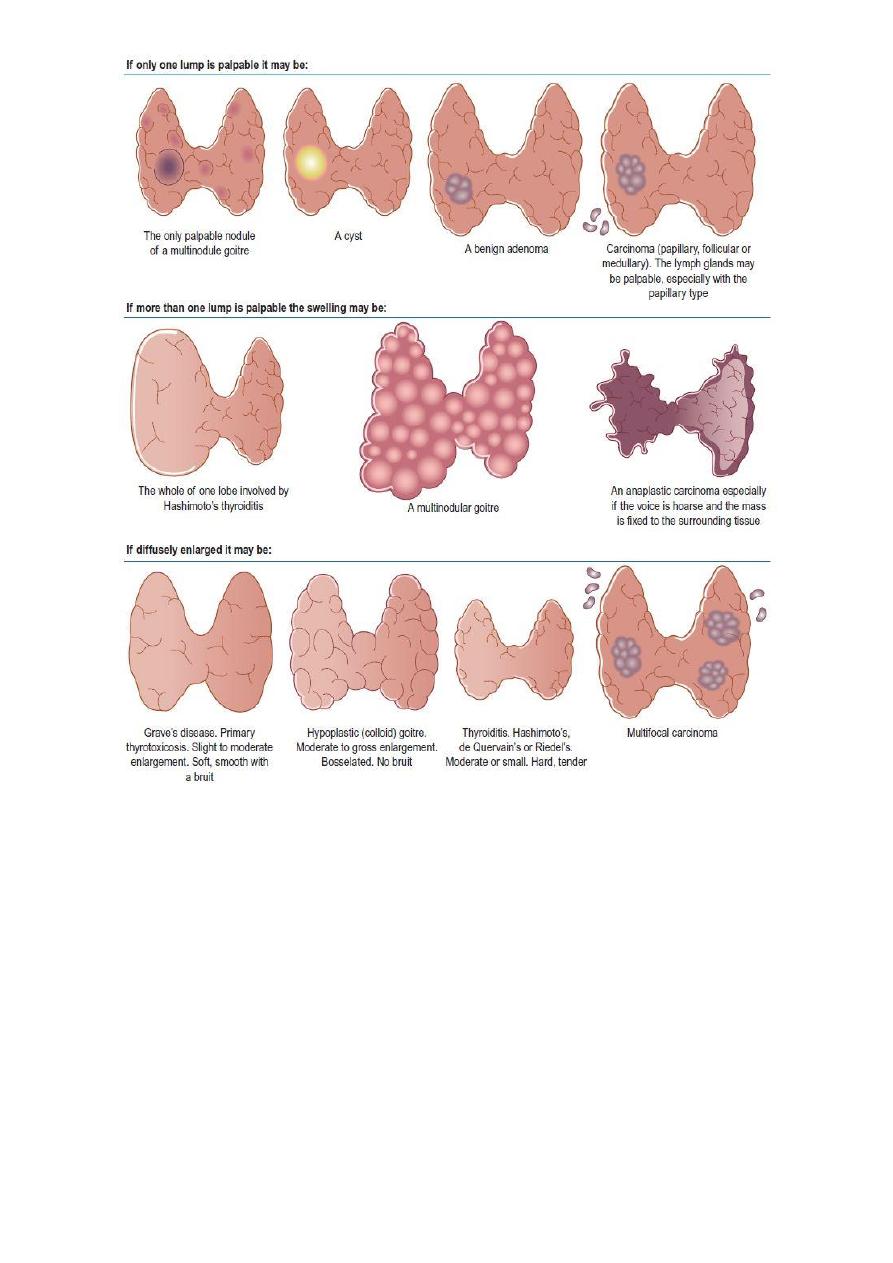
71
#Investigations in thyroid gland diseases:
Ultrasound of the neck: state of thyroid gland, calcifications, nodularity, L.N.
Radio-active iodine: diagnostic and therapeutic, detect hyperactive nodules.
X-ray: shifting of the trachea, widening of the mediastinum.
CT & MRI.
Thyroid function test: TSH, T3, T4, Thyroglobulin.
o Patient take thyroxin T4 high, T3 normal, TSH low.
o Hypothyroidism T4 low, T3 low, TSH high.
o Primary hyperthyroidism T4 high, T3 high, TSH low.
o Secondary hyperthyroidism T4 high, T3 high, TSH high.
Auto-antibody titers.
Blood test: serum calcium, blood count, ESR, CRP, CBC.
FNA, core biopsy, lobectomy (incisional or excisional biopsy).
Laryngoscope.
ECG: for atrial fibrillation.

71
(Salivary glands)
#Causes of swelling of a salivary gland:
Acute infection: Viral (e.g. mumps), Bacterial (e.g. Staphylococcus).
Duct obstruction
Sialectasis (chronic infection)
Tumour: Benign, Malignant.
Sarcoidosis (Mikulicz’s syndrome)
Sjogren’s syndrome
#Examination of Salivary gland swellings:
1- Approach
Sit/kneel to be at the same level as the patient's face
Examine as for any lump
2- Inspect
Swelling in the region of the parotid gland (lies wedged between the
sternocleidomastoid and the mandible) and the submandibular gland (at the angle of
the jaw, wedged between the mandible and mylohyoid)
Look for scars and the opening of a fistula (can follow parotidectomy or long-standing
parotid traumatic injury)
Stand back and look for facial asymmetry which occurs if the VIIth nerve is involved
with a parotid lesion.
3- Palpate from behind
Walk behind the patient and enquire about tenderness before palpating the swelling
Unilateral or bilateral?
Fixity? - ask patient to clench teeth
examine for other features as for any lump
check cervical lymphadenopathy
4- Other tests
Look inside mouth with pen torch at opening of parotid duct (Stensen's duct): opposite
upper 2nd molar and opening of submandibular duct (Wharton's duct)
Look for inflammation and pus, or the presence of a stone
Palpate the parotid duct and submandibular duct openings wearing a pair of gloves
Palpate the submandibular gland bimanually with a finger in the mouth and another
finger below the angle of the jaw
5- Completion
Perform a full ENT examination
#Parotid gland:
History:
72
Age: more common in the elderly and the debilitated.
Symptoms: pain, swelling, fever, rigor, others.
Systematic questions.
Previous history.
Examination:
Inspection: site, size, shape, surface, skin over, surrounding, scar.
Palpation: Tenderness, temperature, other features of swelling.
Mouth examination:
o Inspection: The orifice of Stensen's duct is opposite the second upper molar tooth
(color, pus, edematous).
o Palpation Feel the mouth of the duct (any thickening, swelling, tenderness).
Facial nerve examination:
o Facial deviation (as neurological exam).
o Corneal reflex.
o Special sensation to anterior 2/3 of the tongue.
Fixity: tension of masseter muscle, vertical and horizontal fixity, fixity to underlying
tissue.
Scar: searching for scar of previous surgery by elevating the ear.
Tonsillitis: open the mouth and see the tonsils.
Notes:
The parotid gland cannot be palpated bimanually because it lies behind the anterior
edge of the masseter muscle and the vertical ramus of the mandible.
Gentle pressure on the gland may produce a purulent discharge from the orifice of the
duct.
Why stones in submandibular gland is more than in parotid gland? The duct of
submandibular gland is more vertical and its secretion is mucous.
#Submandibular gland:
History:
Age: most common in young to middle-aged adults.
Sex: Males and females are equally afflicted.
Symptoms: pain and swelling beneath the jaw, caused by obstruction of Wharton’s
duct.
Development: The symptoms may recur and remit for periods of a few days or weeks if
the stone moves about in the duct, sometimes obstructing it, sometimes not.
Previous history.
Examination:
Inspection: site, size, shape, surface, skin over, surrounding, scar.
Palpation:
o Ballotable (finger below the tongue and finger from neck).
o Examine wharton's duct below the tongue.
Percussion.
Auscultation.

73
Nerves examination:
o Hypoglossal nerve: motor to the tongue examine tongue movement.
o Lingual nerve: sensation of posterior 1/3 of tongue.
o Marginal mandibular nerve.
Important structures of submandibular surgery: LDH Lingual nerve, Duct, Hypoglossal
nerve.
#Sublingual gland:
Ranula: caused by trauma or fibrosis that close the duct.
Ranula (unilateral), Ranging Ranula (bilateral).
Treatment: excision from mouth.
#Notes:
Stones: cause pain when see or eat food.
Fixity of mass:
o Contraction become more prominent (more movable) mass in the kin
o Contraction become more prominent (more fixed) mass in the fascia of
muscles.
o Contraction become less prominent mass deep to muscles.
Injury to hypoglossal nerve during surgery lead to atrophy of tongue in the
ipsilateral side.