Pediatric surgeryClinical practice
DR. Bassam Al-Abbasiالصور من الدكتورالشرح من كتابة الطلاب
Head and Neck


Cleft lip and palate
Problems:• Aspiration during feeding
• Nasal speech
• Cosmetic problems
• Affect the hearing (glue ear)
• Lead to recurrent chest infection
Surgery:
• In 6 months to 1 year for cleft palate
• In 3 months for cleft lip
Feeding:
• Use special bottle tit
• In setting position


Cleft lip repair (cheiloplasty)
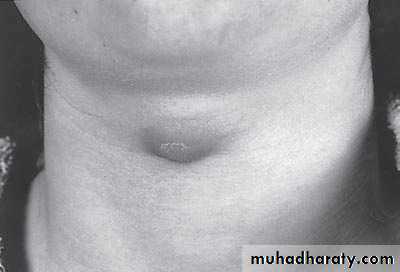

First photo:
Diagnosis: thyroglossal cystProblems:
• Lead to infection
• Lead to fistula
• Could convert to malignancy
Need surgery remove the fistula tract + remove the hyoid bone to
prevent recurrence
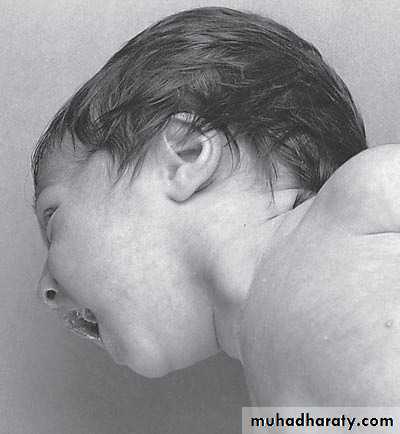
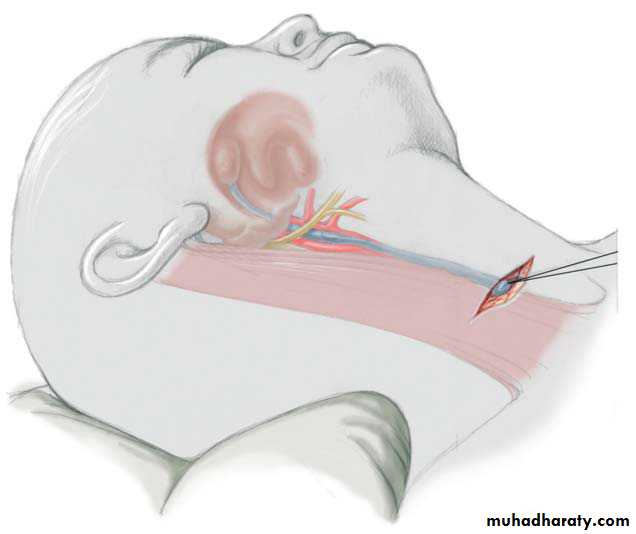
Second photo:
Diagnosis: cystic hygromaNotes:
• It is due to lymphatic obstruction
• Common at the sites of communication between the trunk and the extremities
like cervical region, axilla, groin.
Treatment:
• By surgery: it depends on presence of complications like compression, infection
bleeding (rapid increase in size and become pale and shock)
• During surgery be careful to some nerves like hypoglossal never, spinal
accessory nerve, mandibular branch of facial nerve


Diagnosis:
sternocleidomastoid torticollis (first photo)sternocleidomastoid mass (second photo)
Notes:
• Ask about breech presentation and obstructed labor• If not treat the mass it could be converted to torticollis
• Treatment of mass is by physiotherapy by twisting the chin and movement of
ear and massage 90% will disappear if not treated do surgery by
cutting the mass and muscle.
• Treatment of torticollis is by surgery.
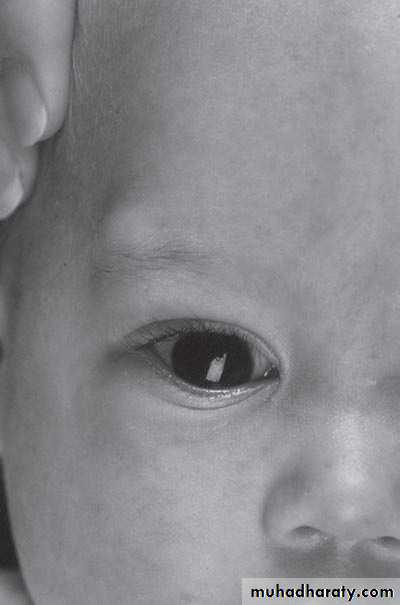
First photo:
Diagnosis: External angular dermoid
Notes:
• Treated by surgery excision and complete remove• Problems infection, trauma, cosmetic
Second photo:
Diagnosis: remnant of second branchial arch branchial cyst or fistula
Site: anterior border of sternocleidomastoid muscle between tonsil
and lower two third of sternocleidomastoid muscleProblems: infection – malignancy
Treatment: surgery (excision)The Umbilicus

First photo:
Diagnosis: umbilical herniaTreatment: could resolve spontaneously or by surgery
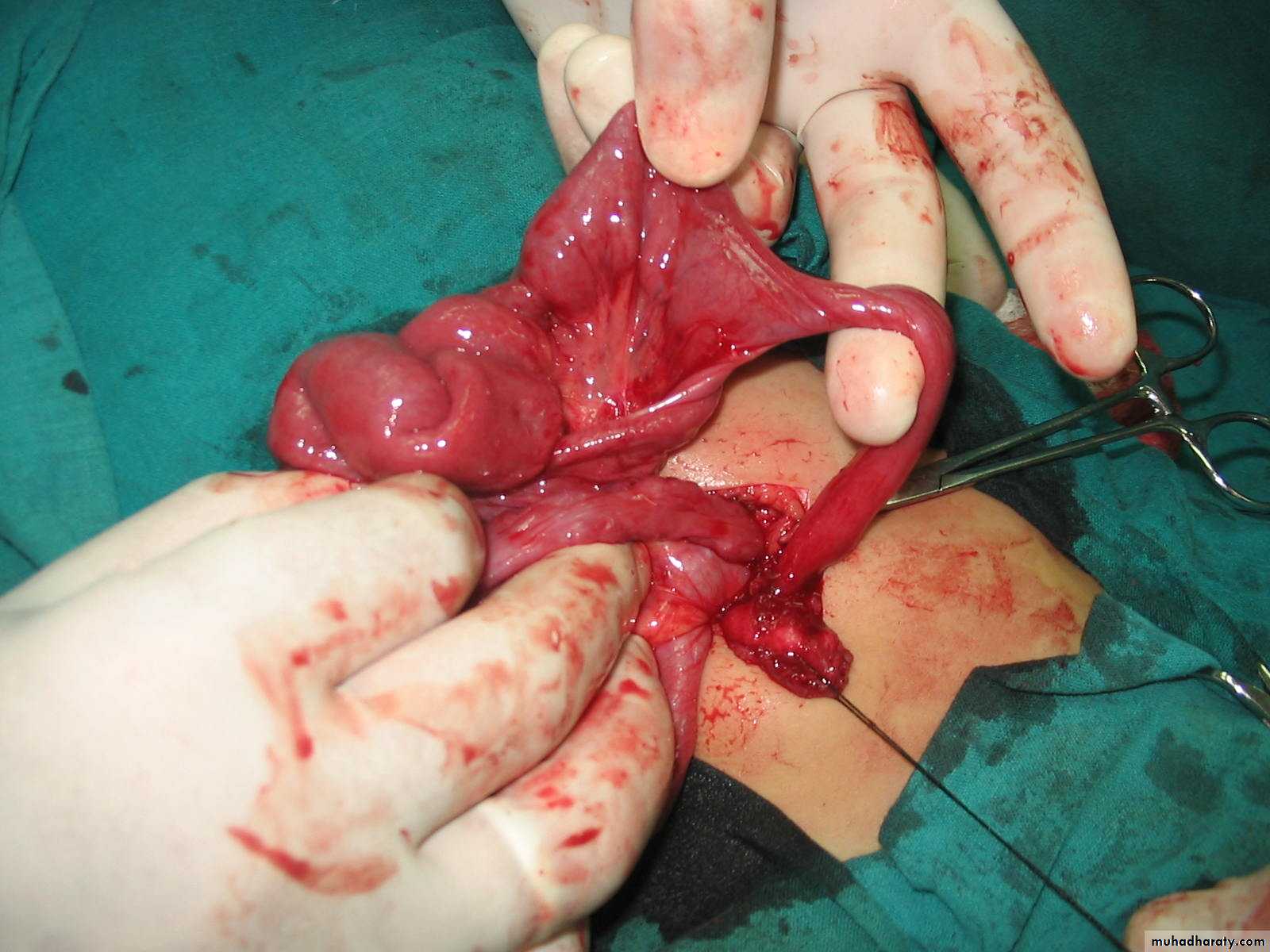
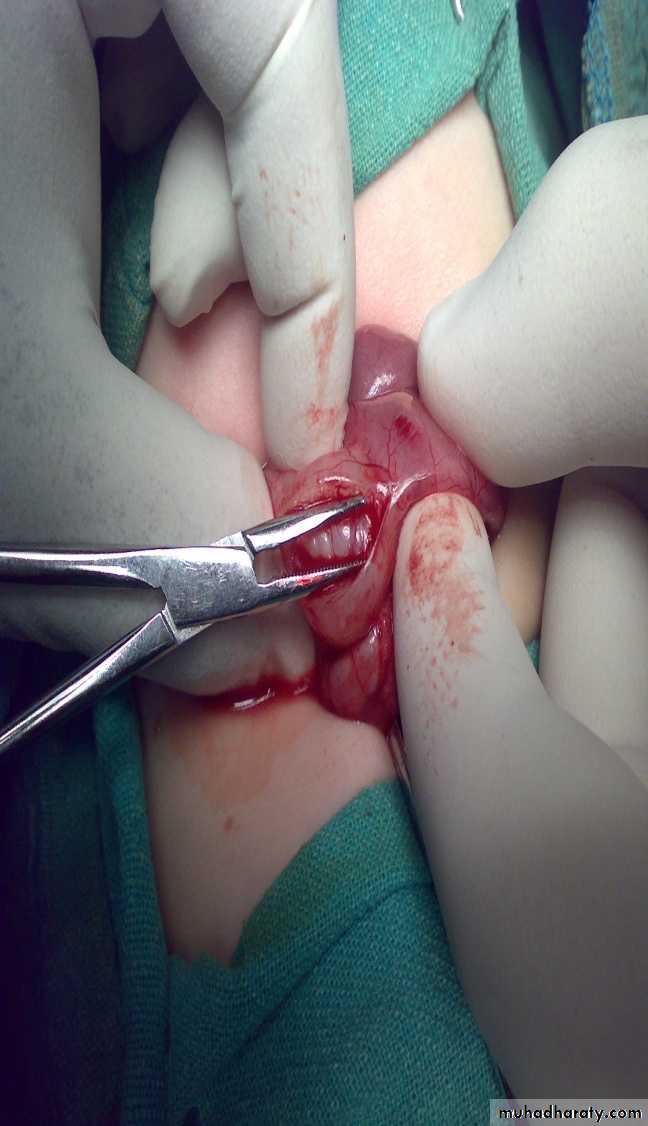
Second photo:Omphalo-mesenteric duct connection between umbilicus and bowel

Diagnosis: Michaels diverticulum
Role of 2:• 2% of population.
• 2 type of mucosa(ectopic gastric mucosa).
• 2 feet from iliocecal valve.
• 2 inches in length.
Presentation:
• Bleeding per rectum (painless – bright red – profuse)
• Infection (lead to abdominal pain)
• Complication intestinal obstruction, volvulus, intussusception
• Incidental finding
Diagnosis:
• Use isotope (bind to gastric tissue (parietal cell) within the Michaels)• Laparoscope (diagnostic and therapeutic)
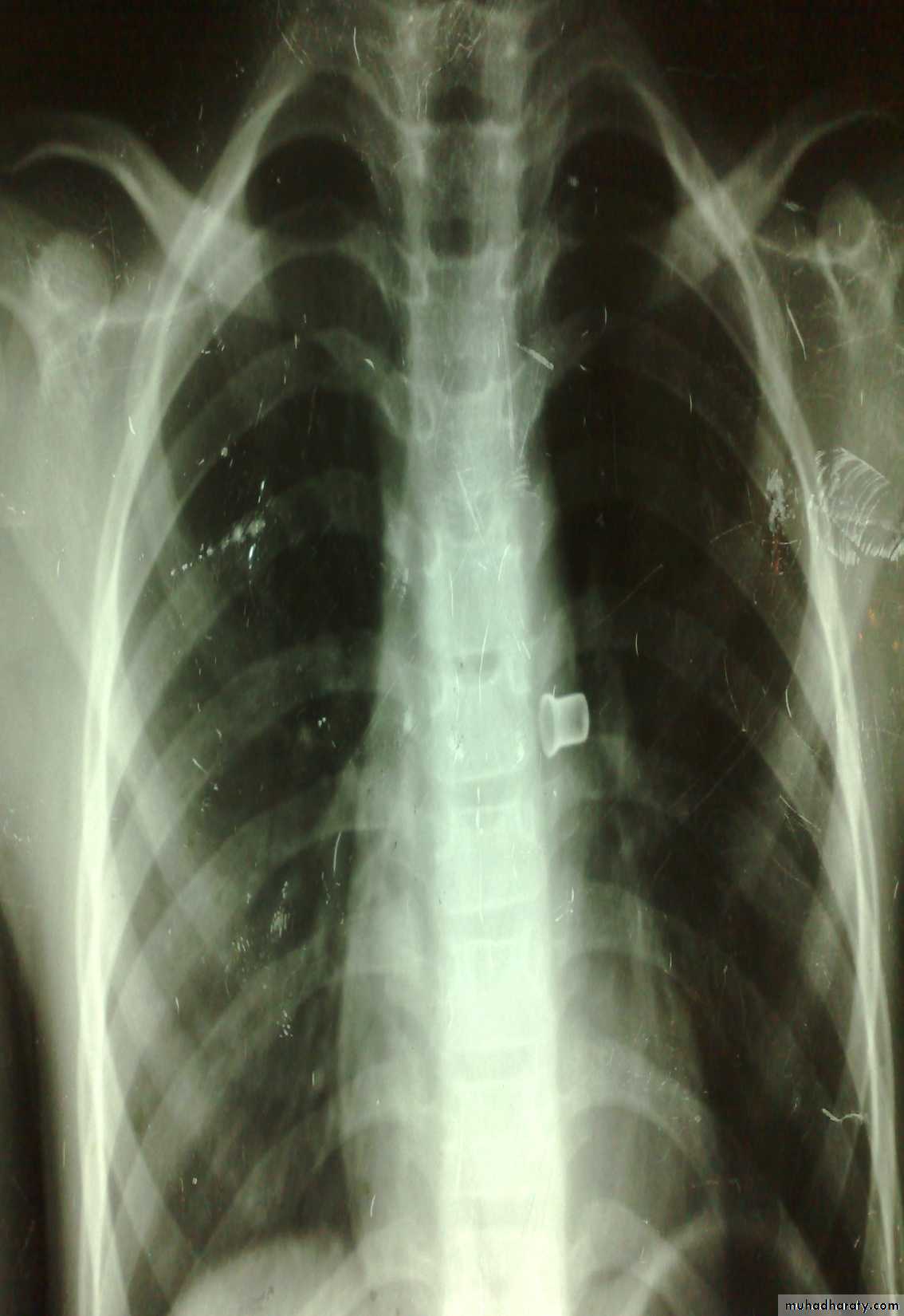
Vomiting in the First Months of Life


Diagnosis: pyloric stenosis
Presentation:• Projectile vomiting (not present in first two weeks)
• Olive mass in the abdomen
• Positive prestalsis
• FTT
Diagnosis:
• Clinically
• Ultrasound
• Ba-meal dilated stomach – failure to pass to intestine – string sign
Treatment: surgery pyloromyotomy (rami stick surgery)

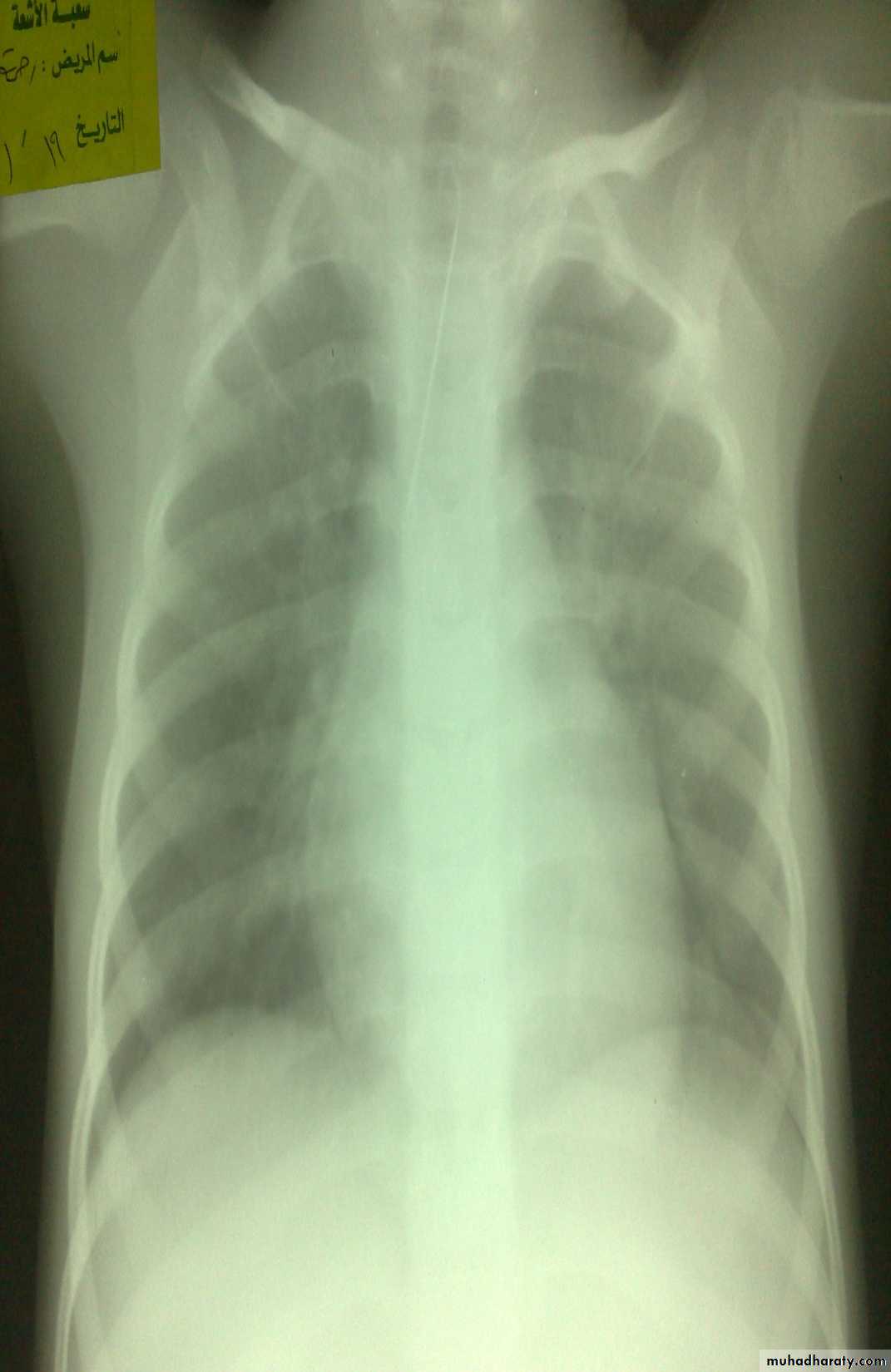
Diagnosis: achalasia cardia
Presentation:• Hailtosis
• Vomiting (not projectile)
• Wheezing
• Chest infection
Ba-swallow dilatation of esophagus with narrowing of lower part.
Treatment cardiomyotomy
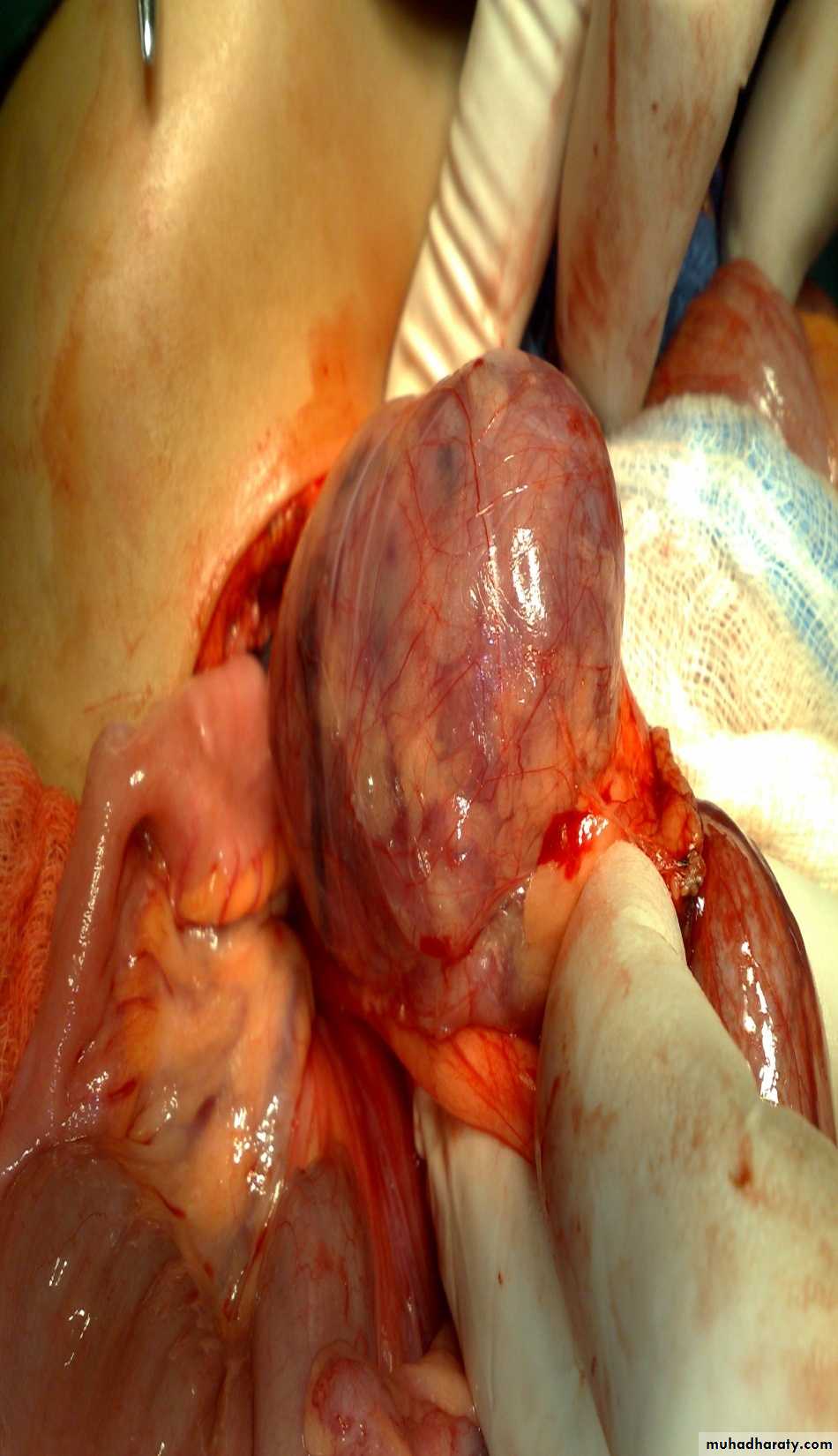
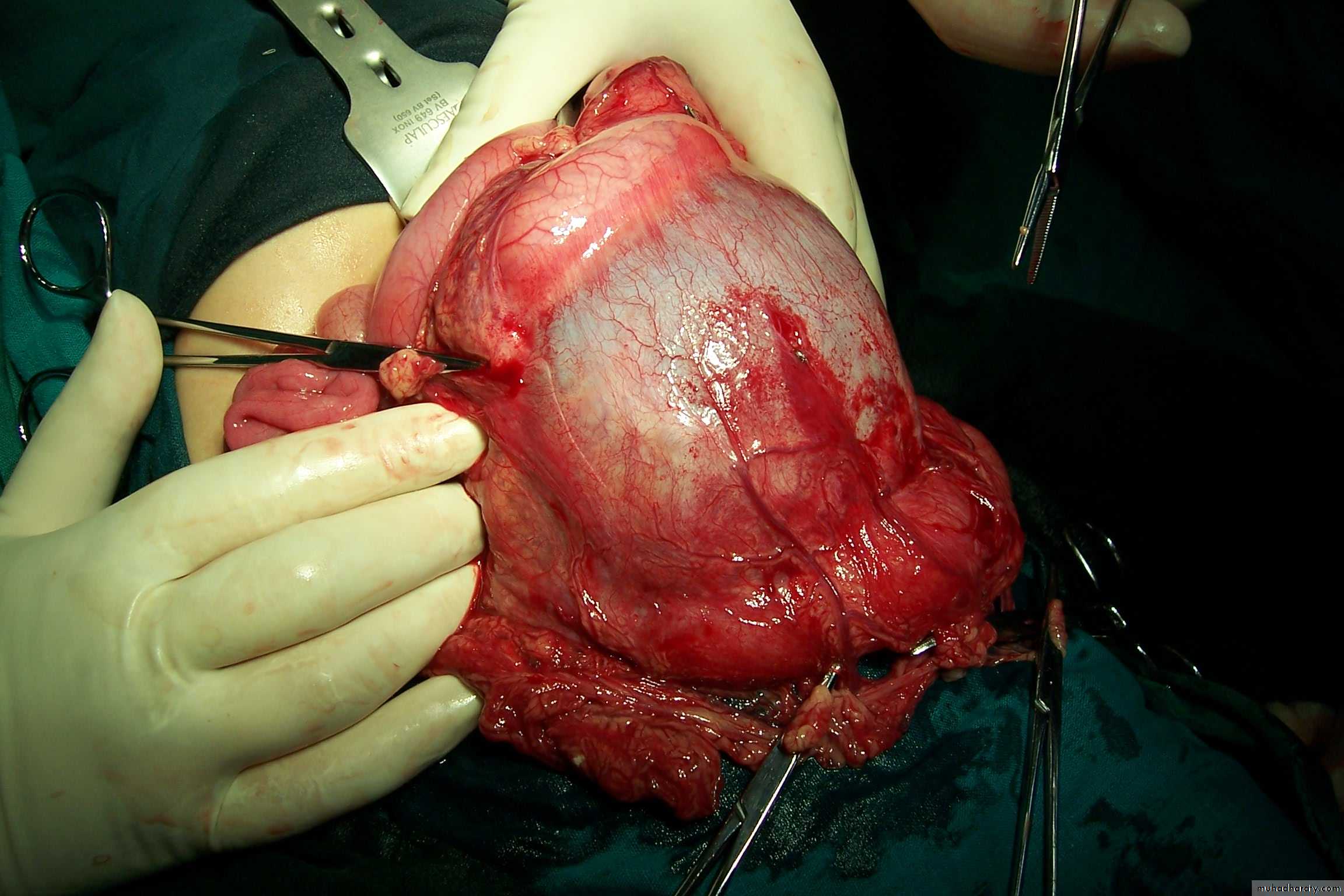
The Child with an Abdominal Mass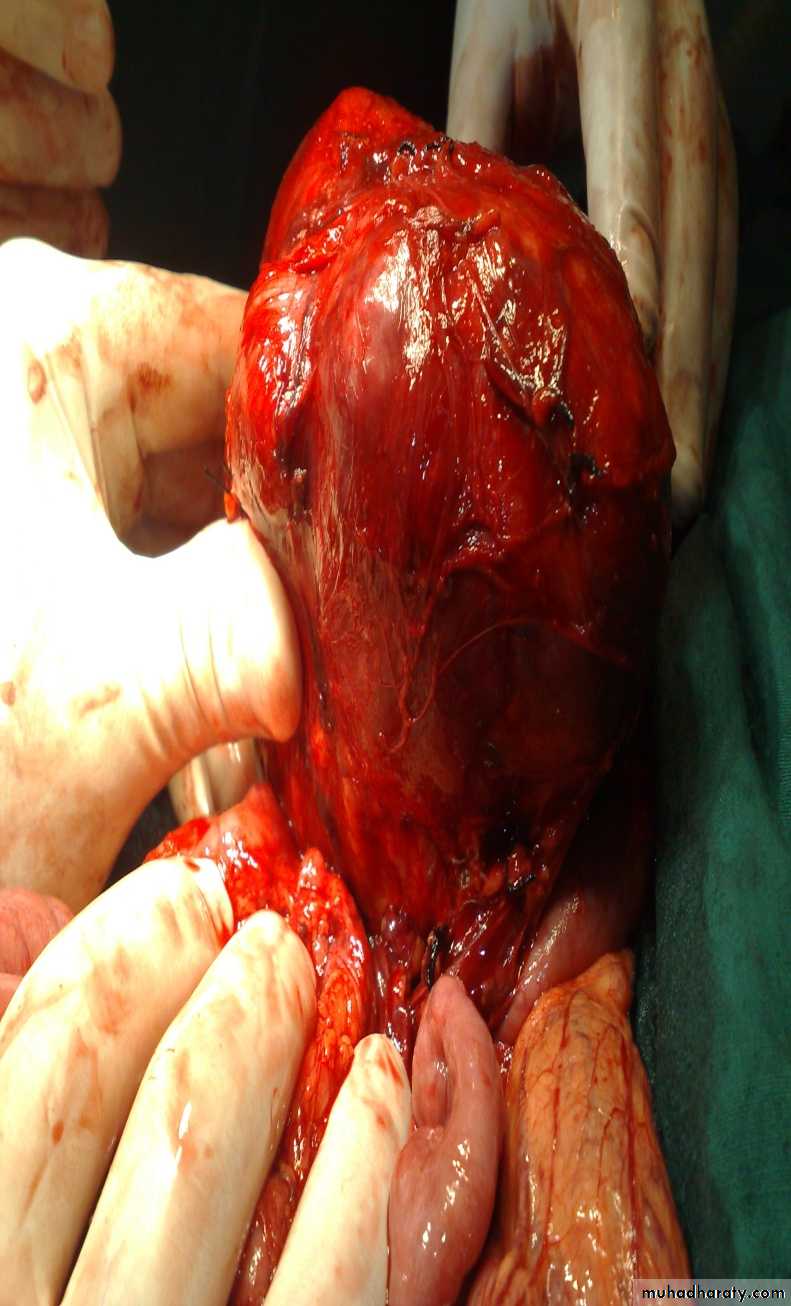

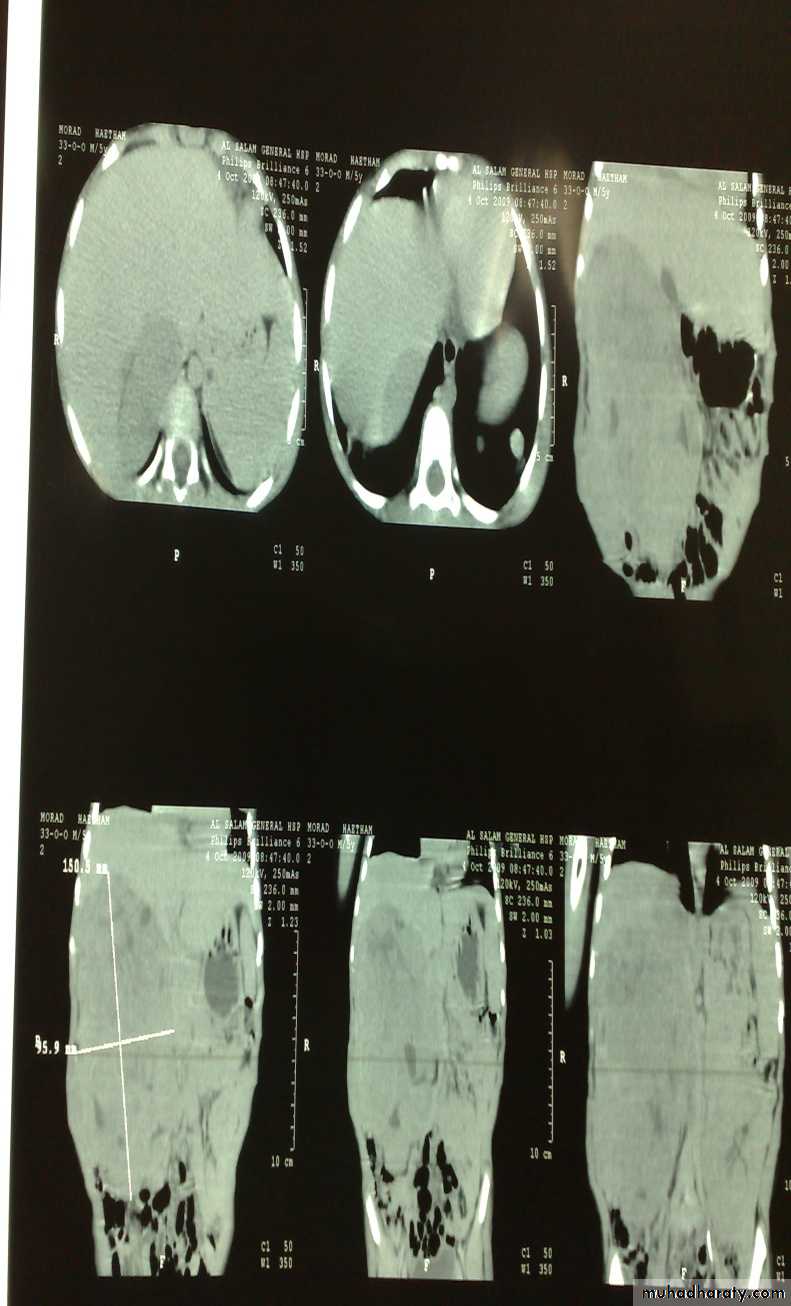
5 years child, presented with mass in the flank.
DDx of mass in the flank:1- Wilms tumor
2- Neuroblastoma
3- Neglected PUJ obstruction
Presentation:
1- Mass2- hematuria
3- hypertension
Treatment by surgery remove the kidney + chemotherapy
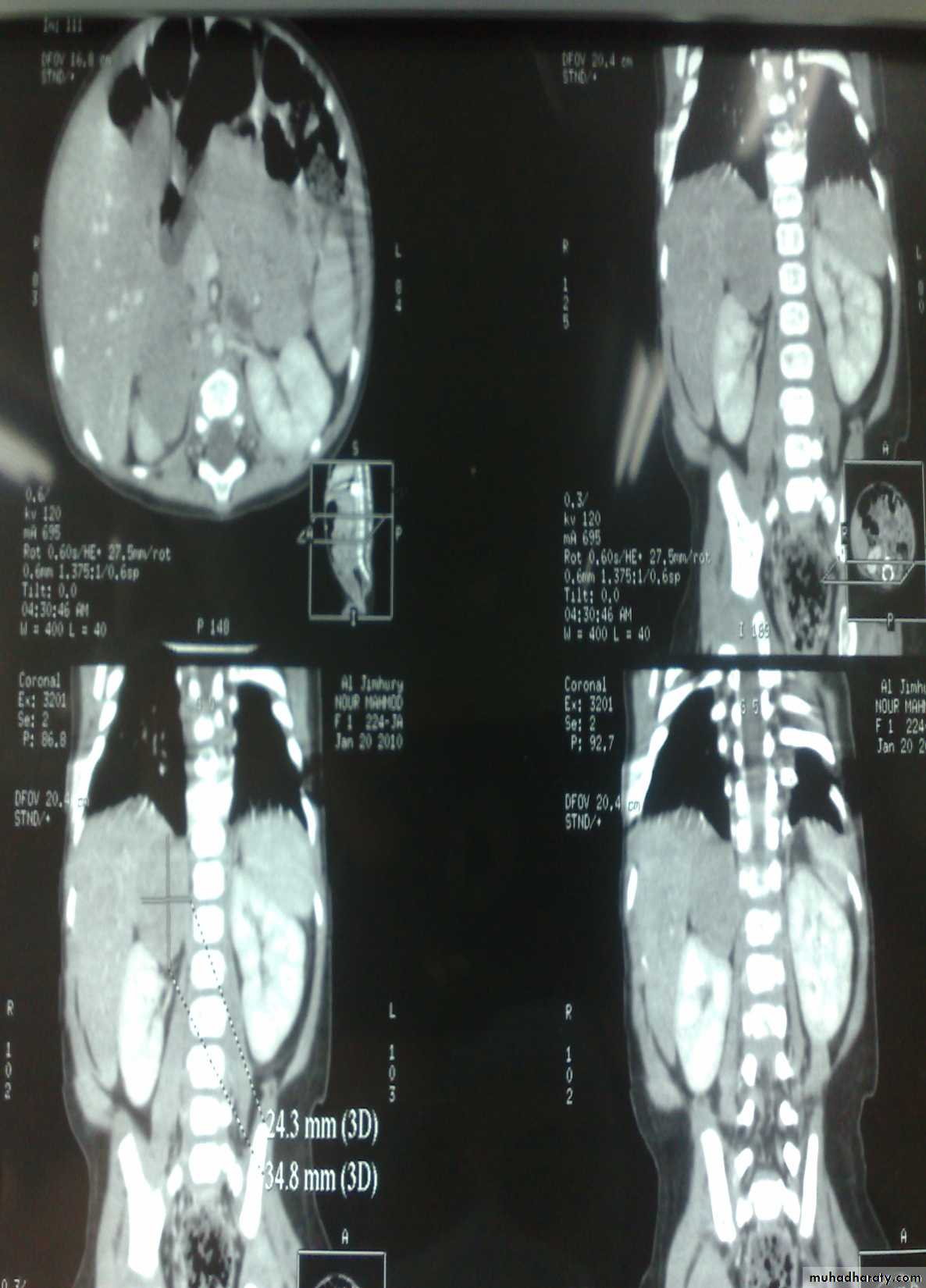
Neuroblastoma in the adrenal gland

Diagnosis: non-Hodgkin lymphoma
Presentation:1- Mass
2- Intussusception
Investigation: FNA
Treatment: surgery + chemotherapy (for one year)

Diagnosis: Sacro-coccygeal teratoma
Problems:1-obstructed labor
2- Malignancy (if neglected for 2-3 months)
Treatment: surgery + remove the coccyx to prevent recurrence
Spleen, Pancreas and Biliary Tract

غير مطلوب

غير مطلوب



First photo:
Diagnosis: rectal prolapseCauses:
• Constipation or diarrhea
• Weak pelvic muscles
• Worm (trichuris trichiura)
Grades:
• Grade1 يطلع ويرجع conservative treatment by taping
• Grade2 يطلع ويحتاج الى دفع للدخول surgery (Therach operation)
• Grade3 يطلع وما يرجع ابد surgery (Therach operation)
Second photo:
Diagnosis: Perianal fistula
Treatment: surgery (fistulectomy or fistulotomy)
Third photo:
Diagnosis: rectal polyp
Cause in infection
Red-bleed mass + bleeding per rectum
Treatment: excision (use sigmoidoscope)


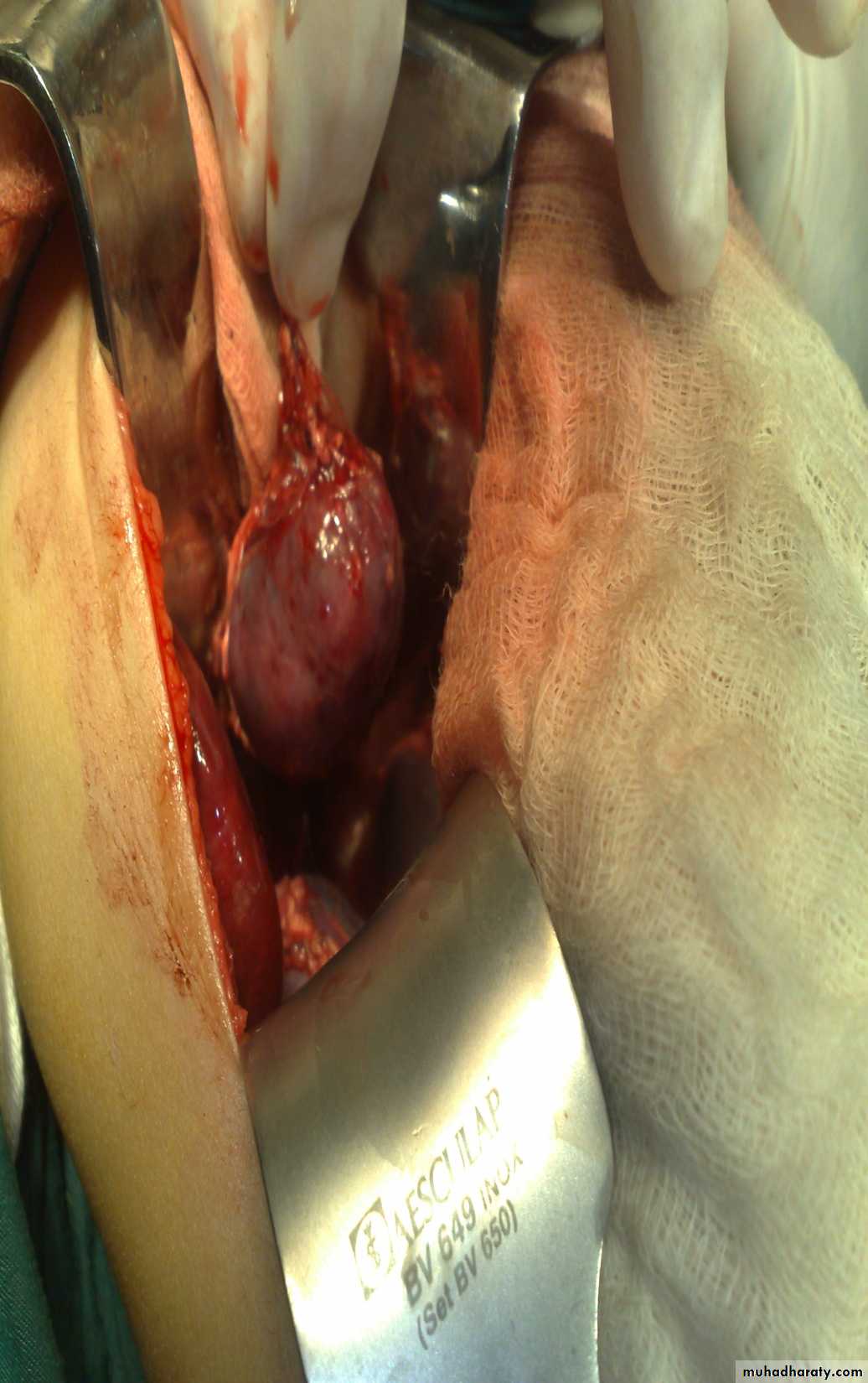
Hernia
Varicocele

Diagnosis: undescended testes
Problems:• Tumor
• Sterility
• Infection
• Orchitis (like appendicitis)
Treatment:
• If palpable do fixation
• If not palpable do laparoscopy
• If not present do nothing


غير مطلوب