
Orthopedic
For
5
th
stage
http://goo.gl/rjRf4F
I
LOKA
©
http://www.muhadharaty.com/orthopedic
I

Content
Topics:
Page:
Orthopedic History
3
Physical examination
6
Examination of specific joints
11
Orthopedic investigations
21
Acute compartment syndrome
23
Notes
25

Part1
: Orthopedic History
Identifying data:
NASOMRA Name, age, sex, occupation, marital status, residence, address.
Date of admission.
Date of examination.
Chief compliant:
Pain.
Swelling.
Stiffness.
Deformity.
Weakness.
Instability.
Change in sensation.
Loss of function.
History of present illness:
1- Pain:
Analysis by SOCRATES.
The most common symptom.
Ask the patient to point where it hurts.
Refereed pain is due to inability of the cerebral cortex to distinguish between sensory
messages from embryologically related sites.
Pain in or near the skin is localized, but in deep structures is more diffuse as hip disease
manifest with pain in the knee.
Autonomic pain affect the autonomic nerves is more vague, more widespread, and
associate with vasomotor and tropic changes.
Pain is sharp, sudden onset, exaggerated by movement, relieved by rest and
immobilization, usually not referred.
2- Stiffness:
Stiffness may be generalized (typically in rheumatoid arthritis and ankylosing
spondylitis) or localized to a particular joint.
Patients often have difficulty distinguishing stiffness from painful movement.
Ask when it occurs rheumatoid arthritis (regular early morning stiffness of many
joints), osteoarthritis (transient stiffness of one or two joints after periods of inactivity).
‘Locking’ is a term used to describe the sudden inability to complete a certain
movement; it suggests a mechanical block due to a loose body or a torn meniscus
becoming trapped between the articular surfaces.
3- Swelling:
Swelling may be in the soft tissues, the joint or the bone.
Is the swelling followed an injury?
Onset: it appeared rapidly (probably a hematoma or a haemarthrosis) or slowly (soft
tissue inflammation or a joint effusion).
Painless or painful? (painful in acute inflammation, infection, tumor).
Constant or comes and goes?
Increasing in size?
4- Deformity:
Examples: round shoulders, spinal curvature, knock-knees, bow-legs, pigeon-toes and
flat-feet.
If the deformity is progressive, or if it appears on only one side of the body, it may be
serious.
Some deformities are only variations of the normal (short stature or wide hips).
Some deformities disappear spontaneously with growth (flat feet or bandy legs in an
infant).
5- Weakness:
Generalized weakness is a feature of all chronic illness.
Any prolonged joint dysfunction will inevitably lead to weakness of the associated
muscles.
Weakness affecting a single group of muscles suggests a more specific neurological
disorder.
6- Instability:
The patient complains that the joint ‘gives way’ or ‘jumps out’.
If this happens repeatedly it suggests ligamentous deficiency, recurrent subluxation
or some internal derangement such as a loose body.
7- Change in sensibility:
Tingling or numbness signifies interference with nerve function:
o Pressure from a neighboring structure (a prolapsed intervertebral disc).
o Local ischemia (nerve entrapment in a fibro-osseous tunnel).
o Peripheral neuropathy.
8- Loss of function:
Functional disability is more than the sum of individual symptoms and its expression
depends upon the needs of the patient.
What to one patient is merely inconvenient may to another be incapacitating.
Each symptom is need more detail:
1. when it begin.
2. suddenly or gradually.
3. spontaneously or after some specific events.
4. how it progressed.
5. what make it better or what it make it worse.
Systemic review:
Past history:
Ask about previous accidents, illnesses, operations and drug therapy.
Family history:
Information about musculoskeletal disorders in the patient’s family.
Social history:
Details about work, travel, recreation, home circumstances and the level of support
from family and friends.
----------------------------------------------------------------------------------------------------------
See this paper
www.muhadharaty.com/lecture/3483
Part2
: Physical examination
Clinical examination may be considered under three headings:
1. Examination of the part complained of.
2. Investigation of possible sources of referred symptoms.
3. General examination of the body as a whole.
1. Examination of the Part Complained of:
Exposure for examination:
It is essential that the part to be examined should be adequately exposed and in a
good light.
Inspection
The bones Observe the general alignment and position of the parts to detect any
deformity, shortening, or unusual posture.
The soft tissues Observe the soft-tissue contours, comparing the two sides. Note any
visible evidence of general or local swelling, or of muscle wasting.
Color and texture of the skin Look for redness, cyanosis, pigmentation, shininess, loss
of hair, adventitious tufts of hair or other changes.
Scars or sinuses If a scar is present, determine from its appearance whether it was
caused by operation (linear scar with suture marks), injury (irregular scar), or
suppuration (broad, adherent, puckered scar).
Palpation
The skin Is it warm or cold; moist or dry; and is sensation normal?
Skin temperature By careful comparison of the two sides. Causes of increase of local
temperature
increased vascularity, inflammatory reaction, rapidly growing tumor
(lead to hyperaemia with increase in skin warmth).
The bones Feel general shape, outline of the bones, feel in particular for thickening,
abnormal prominence, or disturbed relationship of the normal landmarks.
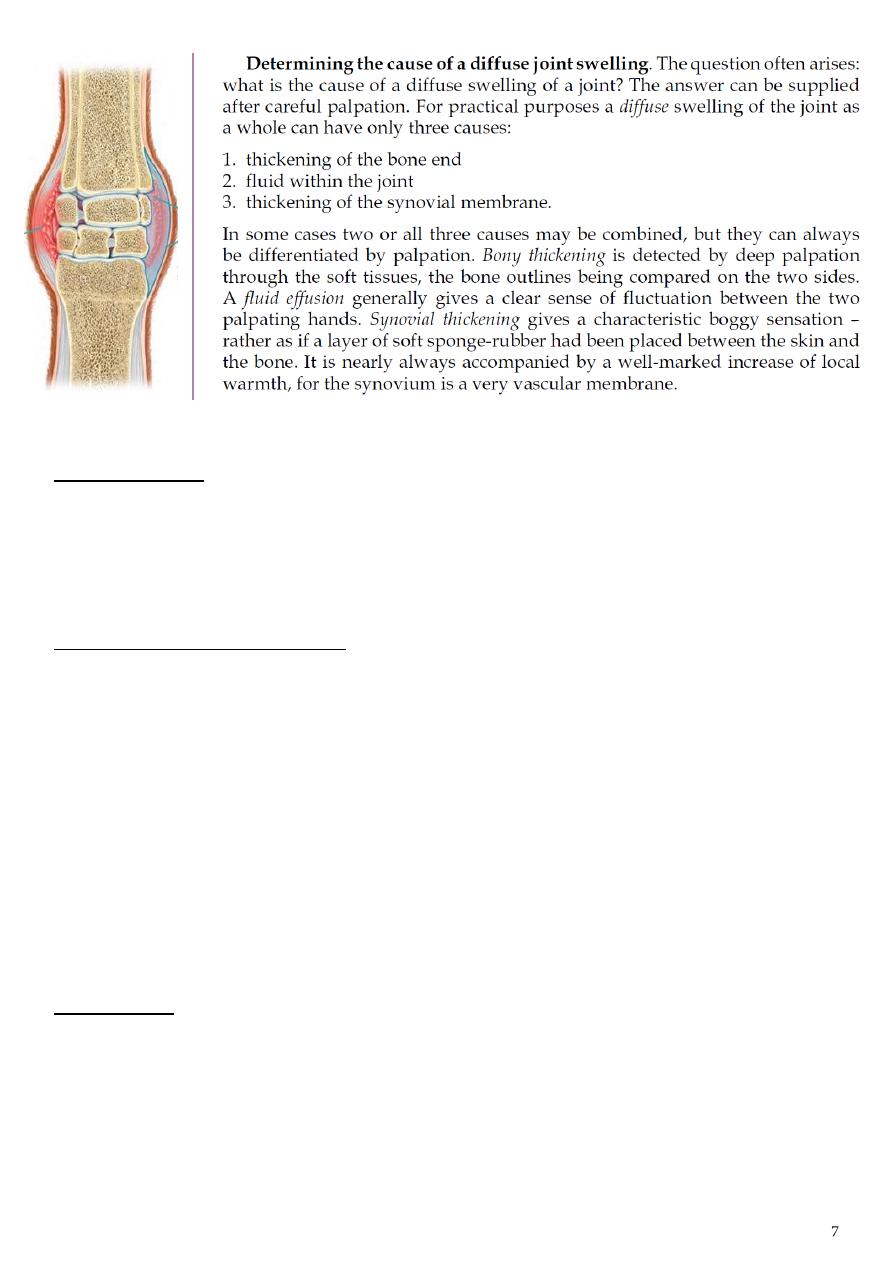
The soft tissues The muscles (are they in spasm, or wasted?), the joint tissues (is the
synovial membrane thickened, or the joint distended with fluid?), the detection of any
local swelling (cyst or tumor) or general swelling of the part, Are the pulses normal?
Local tenderness The exact site of any local tenderness should be mapped out and an
attempt made to relate it to a particular anatomical structure.
Measurements
Measurement of limb length is often necessary, especially in the lower limbs,
where discrepancy between the two sides is important.
Measurement of the circumference of a limb show any asymmetry, provides an
index of muscle wasting, soft-tissue swelling or bony thickening.
Estimation of fixed deformity
Fixed deformity exists when a joint cannot be placed in the neutral (anatomical)
position.
The degree of fixed deformity at a joint is determined by bringing the joint as near as
it will come to the neutral position and then measuring the angle by which it falls
short.
Valgus deformity the distal part of a member is deviated laterally (outwards) in
relation to the proximal part (example: in hallux valgus the toe is deviated outwards in
relation to the foot, in genu valgum the lower leg is deviated outwards in relation to
the thigh).
Varus deformity is the opposite: the distal part of a member is deviated medially
(inwards) in relation to the proximal part (examples: cubitus varus and genu varum).
Movements
What is the range of active movement? use goniometer.
Is passive movement greater than active movement?
Is movement painful?
Is movement accompanied by crepitation?
Is there any spasticity (stiff resistance to free movement)?
Notes:
o The range of movement should be expressed in degrees, starting from zero which
is the neutral or anatomical position of the joint.
o Restriction of movement in all directions suggests some form of arthritis, whereas
selective limitation of movement in some directions, with free movement in
others, is more suggestive of a mechanical derangement.
o Passive movement will usually be found equal to the active range.
o The passive range will exceed the active only in the following circumstances:
o 1. when the muscles responsible for the movement are paralysed.
o 2. when the muscles or their tendons are torn, severed, or unduly slack.
o Joint Stiffness Arthrodesis: surgical fusion, Ankylosis: pathological fusion.
o Causes of joint deformity contracture of overlying soft tissues, muscle
imbalance, dislocation, joint destruction.
o Joint Laxity Persistent generalized joint hypermobility (Autosomal dominant).
Summary 1- Active movement, 2- Passive movement, 3- Record Degree of
movement, 4- Feel for crepitus, 5- Unstable movement, 6- Provocative / apprehension
tests, 7- Joint Stiffness 8- Deformity (Varus, Valgus) 9- Bony Lumps (size, shape, site,
margin, consistency, tenderness, multiplicity).
Stability
The stability of a joint depends partly upon the integrity of its articulating surfaces,
intact ligaments, healthy muscles.
When a joint is unstable there is abnormal mobility when testing for abnormal
mobility, to ensure that the muscles controlling the joint are relaxed, for a muscle in
strong contraction can often conceal ligamentous instability.
Power
The power of the muscles responsible for each movement of a joint is determined by
instructing the patient to move the joint against the resistance of the examiner.
With careful comparison of the two sides it is possible to detect gross impairment of
power.
The strength of a muscle is recorded according to the Medical Research Council
grading, as follows:
0 = no contraction.
1 = a flicker of contraction.
2 = slight power, sufficient to move the joint only with gravity eliminated.
3 = power sufficient to move the joint against gravity.
4 = power to move the joint against gravity plus added resistance.
5 = normal power.
Sensation
It is important to test sensibility both to light touch and to pin prick throughout the
whole of the affected area (numbness or tingling).
In unilateral affections the opposite side should be similarly tested for comparison.
The precise area of any blunting or loss of sensibility should be carefully mapped out.
Knowledge of the sensory dermatomes and the cutaneous distribution of the
peripheral nerves help in identification of the particular nerve or nerves affected.
Superficial sensations Hyperasthesia (increased), Dysaesthesia (unpleasant),
Hypoasthesia (diminished), Anaesthesia (loss).
Deep sensations vibration test, position sense, sense of joint posture, sterognosis
the ability to recognize shape and texture by feel alone.
Reflexes
The appropriate deep and superficial reflexes must be tested.
Superficial reflexes:
o The superficial reflexes are elicited by stroking the skin at various sites to produce
a specific muscle contraction.
o The best known are the abdominal (T7–T12), cremasteric (L1, 2) and anal (S4, 5)
reflexes.
o These are corticospinal (upper motor neuron) reflexes.
o Absence of the reflex indicates an upper motor neuron lesion (usually in the spinal
cord) above that level.
Deep reflexes:
o A deep tendon reflex is elicited by rapidly stretching the tendon near its insertion.
A sharp tap with the tendon hammer does this well.
o Comparing the two sides in this way, we can pick up fine differences showing that
a reflex is ‘diminished’ rather than ‘absent’.
o In the upper limb we test biceps, triceps and brachioradialis, and in the lower limb
the patellar ligament and Achilles tendon.
o The tendon reflexes are monosynaptic segmental reflexes.
o It is a reliable pointer to the segmental level of dysfunction.
o An unusually brisk reflex, on the other hand, is characteristic of an upper motor
neuron disorder (e.g. cerebral palsy, a stroke or injury to the spinal cord).
o The lower motor neuron is released from the normal central inhibition and there
is an exaggerated response to tendon stimulation.
The plantar reflex:
o Forceful stroking of the sole normally produces flexion of the toes (or no response
at all).
o An extensor response (the big toe extends while the others remain in flexion) is
characteristic of upper motor neuron disorders.
o This is the Babinski sign a type of withdrawal reflex which is present in young
infants and normally disappears after the age of 18 months.
Cortical and cerebellar function
A staggering gait may imply drunkenness, an unstable knee or a disorder of the
spinal cord or cerebellum.
If there is no musculoskeletal abnormality to account for the sign, a full examination
of the central nervous system will be necessary.
Peripheral circulation
Examination of the color and temperature of the skin.
The texture of the skin and nails.
The arterial pulses.
Special investigations as may be necessary.
This examination is particularly important in the case of the lower limb.
Tests of function
How much does the disorder affect the part in its fulfilment of everyday activities?
Methods of determining this vary according to the part affected.
The best test of function of lower limbs is to observe the patient standing, walking,
running and jumping, or climbing and descending stairs.
Special tests are required to investigate certain functions (example: Trendelenburg
test for abductor efficiency at the hip).
2. Investigation of Possible Sources of Referred Symptoms:
When the source of the symptoms is still in doubt after careful examination of the
part complained of, attention must be directed to possible extrinsic disorders with
referred symptoms.
This will entail examination of such other regions of the body as might be responsible.
Example1 in a case of pain in the shoulder it might be necessary to examine the
neck for evidence of a lesion interfering with the brachial plexus, and the thorax and
abdomen for evidence of diaphragmatic irritation.
Example2 in a case of pain in the thigh the examination will often have to include a
study of the spine, abdomen, pelvis, and genito-urinary system as well as a local
examination of the hip and thigh.
3. General Examination of the body as a whole:
It should be made a rule in every case.
Should examine the patient’s general physical condition and psychological outlook.
Part3
: Examination of specific joints
Shoulder joint examination
www.muhadharaty.com/lecture/3508/
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "both shoulders, arms, chest, back"
Look:
Look from anterior, posterior, and lateral side.
Symmetry, deformity at the same level? Scapular, outlines.
Swelling or redness, wasting, scar, sinus.
Push against the wall (for winging of scapula) lesion of the serratus anterior muscle
(C5,6,7).
Feel:
Ask him if he has any pain.
Temperature and tenderness (from sternoclavicular acrominoclavicular joint
acromion process supraspinatus tenderness, long head of biceps.. edge of scapula)
Move:
Active movement forward flexion (0-170°), extension (0-40°), abduction (0-160°
'painful arc?'), adduction, internal rotation (0-90°), external rotation (0-70°). Also
scapula movement.
Observe the range, symmetry, rhythm of the movement.
Passive movement here you have to feel the joint by the other hand to feel any
crepitus.
During the examination you have to observe the biceps function and painful arc.
Special tests:
Apley Scratch Test www.pthaven.com/page/show/161711-apley-scratch-test
Apprehension Test www.pthaven.com/page/show/157397-apprehension-test
The Painful Arc (Impingement syndrome)
1- Passively abduct the patient’s arm to its maximum point of abduction.
2- Ask the patient to lower their arm slowly back to a neutral position.
3- Impingement / supraspinatus tendonitis typically causes pain between 60-120° of
abduction.
Don't forget:
Neurovascular examination brachial a., axillary a., subclavian a., power, reflex
(biceps and triceps), sensation (axillary n.).
L.N examination axillary and supraclavicaular L.Ns.
Both suggest to examine the proximal and distal joints.
At the end:
cover the patient and thank him.
Elbow joint examination
www.muhadharaty.com/lecture/3509/
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure.
Look:
Look from anterior, posterior, and lateral side.
Symmetry, deformity at the same level? Carrying angle 5-10°.
Swelling or redness, wasting, scar, sinus.
Olecranon bursa.
Feel:
Ask him if he has any pain.
Temperature and tenderness (medial and lateral epicondyles + olecranon process).
Lateral epicondyle Tennis elbow "intensified by active extension of the wrist".
Medial epicondyle Golfer elbow.
Palpate and tap on the ulnar nerve.
Move:
Active movement full extention (0°), full flexion (140°), pronation (90°), supination
(90°), internal rotation (0-90°), external rotation (0-70°).
Passive movement here you have to feel the joint by the other hand to feel any
crepitus.

Special tests:
Tennis elbow, Golfer elbow www.muhadharaty.com/lecture/3485/
Don't forget:
Neurovascular examination brachial a., radial a., power, reflex, sensation.
L.N examination epitrochlear L.Ns.
Both suggest to examine the proximal and distal joints.
At the end:
cover the patient and thank him.
Wrist & hand examination
www.muhadharaty.com/lecture/3510/
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "when needed"
You can ask about hand dominance.
Look:
Symmetry, deformity, swelling or redness, wasting, scar, sinus.
Skin (smooth, moist, dry & contracture), callosities (working man's hand).
Palmar creases (pallor), palmar erythema.
Nails pitting or other changes.
Examine the palmar, dorsal surface of the hand & even the extensor surface of the
forearm.
Feel:
Ask him if he has any pain.
Temperature, nodules.
Tenderness (styloid process in De Quervain's Tendinitis), (snuffbox in scaphoid injury),
(ulnar head in extensor carpi ulnaris tendinitis).
Palpate for dupuytren's contracture, flexor sheaths & crepitus with movement.
Don’t forget neurovascular examination (capillary refill, radial a., ulnar a., taping on the
ulnar n.).
Some schools say 'you can use finger squeeze'.
Move:
Active movement flexion (0-80°) "reverse prayer sign", extension (0-80°) "prayer
sign", ulnar deviation (0-40°), radial deviation (0-10°), pronation and supination (the
elbow joint must keep stable), thumb movement.
Observe the range, symmetry, rhythm of the movement.
Then passive movement.
Special tests:
Finkelstein test (for De Quervain's Tendinitis)www.muhadharaty.com/lecture/3496/.
Phalen (for flexion) www.muhadharaty.com/lecture/3497/.
Reverse phalen www.muhadharaty.com/lecture/3498/.
All done with palpation.
Don't forget:
Neurovascular examination Allen's test is included (
www.muhadharaty.com/lecture/3499/
).
L.N examination.
Function of hand assessment.
Suggest examine the proximal joints.
At the end:
cover the patient and thank him.
Hip joint examination
www.muhadharaty.com/lecture/3504/
Must be in 3 positions: supine, sitting & lying position.
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "when needed"
Then:
Trendelenburg's test
www.muhadharaty.com/lecture/3488.
Gait.
Iliopsoas function (in the sitting position)
Note: it is worth to start with special tests in hip examination.
Look:
Symmetry (both A.S.I.S. at the same level), deformity.
Swelling or redness, wasting, scar, sinus.
Leg length apparent length (from xiphisternum to medial malleolus), real length
(from A.S.I.S. to malleolus).
Feel:
Ask him if he has any pain.
Temperature and tenderness (ischial tuberosity, greater trochanter, tendon of the
adductor longus).
Move:
You have to support the pelvis by one hand to prevent its movement.
Active movement flexion (0-140°) THOMAS test, abduction (0-40°), adduction (0-
20°), internal rotation (0-50°), external rotation (0-30°).
Passive movement.
THOMAS test www.muhadharaty.com/lecture/3489/
Special tests:
Done in the previous steps.
Then:
Prone position (from the back) scar, swelling, sinus, wasting (gluteal and hamstring
muscles), tuft of hair, tenderness, extension (o-10°).
Don't forget:
Neurovascular examination.
L.N examination inguinal L.Ns.
Both suggest to examine the proximal and distal joints.
At the end:
cover the patient and thank him.
Knee joint examination
www.muhadharaty.com/lecture/3505/
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.

Make sure patient privacy.
Good exposure "when nedded"
Then:
gait.
Look:
Look from anterior, posterior, and lateral side.
Symmetry, deformity, swelling or redness, wasting, scar, sinus.
Shape, position & symmetry of patella.
Feel:
Ask him if he has any pain.
Temperature and tenderness (joint line, ligaments attachment, patella, patellar
ligmaent)
Asses joint effusion patellar taping and milking.
Posterior surface of patella.
Move:
Active movement flesxion, extension, rotation (the knee must be bent)
McMurray's test may feel clunck (www.muhadharaty.com/lecture/3493).
Then passive movement.
Special tests:
Valgus & varus stress tests www.muhadharaty.com/lecture/3491.
Drawer test www.muhadharaty.com/lecture/3492.
Crude test.
Patellar apprehension test www.muhadharaty.com/lecture/3494.
Sag sign www.muhadharaty.com/lecture/3494.
Then:
Prone position (from the back) scar, swelling, Baker's cyst, aneurysm.
Grinding & Destruction test.
Don't forget:
Neurovascular examination.
L.N examination popliteal L.Ns.
Both suggest to examine the proximal and distal joints.
At the end:
cover the patient and thank him.

Ankle joint & Foot examination
www.muhadharaty.com/lecture/3506/
Must be in 4 positions:
The patient facing you.
His back facing you.
Walking.
Tip toe waking.
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "when needed"
Then:
Gait.
Look:
Symmetry, deformity at the same level, swelling or redness, wasting, scar, sinus.
Observe the Achilles tendon, heel, medial longitudinal arch, sole & nails.
Feel:
Ask him if he has any pain.
Temperature and tenderness (joints, joint line, under medial arch planter fasciitis,
on the sesamoid bones sesamoiditis, adjacent side of the 3
rd
& 4
th
toes Morton's
metatarsalgia).
Some schools say 'you can use finger squeeze'.
Move:
Active movement dorsiflexion (0-15°), plantarflexion (0-40°), inversion (0-30°),
eversion, toes movements (flexion & extension).
Then passive movement.
Then:
Prone position (from the back) calf and ankle examination.
Special tests:
Simmond Test for Achilles tendon rapture (www.muhadharaty.com/lecture/3500/).
Don't forget:
Neurovascular examination.
L.N examination.
Both suggest to examine the proximal and distal joints.
See the shoes may be medial one.
At the end:
cover the patient and thank him.
Cervical spine examination
www.muhadharaty.com/lecture/3507/
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "both upper limbs & the trunk"
Look:
Symmetry, deformity, swelling or redness, wasting, scar, sinus, ulcer, and skin lesion.
Feel:
Ask him if he has any pain.
Anterior from behind, posterior in prone position.
Temperature and spinous process for tenderness.
Finger breadth.
Move:
Active movement flexion (chin on chest 75°), extension (look up at the ceiling
60°), rotation (look over your shoulder 80°), lateral flexion (put your ear on the
shoulder 45°).
Special tests:
In the thoracic spine examination the chest expansion is the most important
difference & all other steps are the same.
Don't forget:
Neurovascular examination.
L.N examination.
Allen's test is included.
Suggest to examine the distal joints.
At the end:
cover the patient and thank him.
Lumbar spine examination
www.muhadharaty.com/lecture/3507/
Must be in 3 positions:
Upright.
Prone.
Supine position.
First:
Greet the patient, introduce yourself.
Take permission for examination.
Hand washing.
Make sure patient privacy.
Good exposure "both legs & the trunk"
Look:
Symmetry, deformity, swelling or redness, wasting, scar, sinus.
Skin lesions (Café au lait, herpes zoster, etc.)
From the back look again, hyperkyphosis, hyperlordosis, scoliosis or gibbus, pelbis
level.
Stand on his toes (S1,2), heels (L4,5), gaits.
Feel:
Ask him if he has any pain.
Temperature and spinous process for tenderness.
Finger breadth.
Move:
Active movement extension (lean forward), flexion, lumber excursion normally at
least increase 5 cm, lateral flexion (bend sideway) 30°, rotation (you have tostabilize
the pelvis) 40°.
Special tests:
Femoral stretch test (L2,3,4) www.muhadharaty.com/lecture/3501.
Sciatic stretch test (straight leg raising) + passive dorsiflexion + confirmatory test
www.muhadharaty.com/lecture/3502/.

FABER maneuver (for sacroiliac joint) www.muhadharaty.com/lecture/3503/.
Heel-hip-occiput test (for ankylosing spondylitis).
Don't forget:
Neurovascular examination hamstring power L4,5, gluteus maximus power, Knee
extension L3,4, big toe dorsiflexion L5, planter flexion S1, foot invesion L5 & eversion
S1.
L.N examination.
Abdomen for aortic aneurysm.
Suggest to examine the proximal and distal joints.
At the end:
cover the patient and thank him.
Part4
: Orthopedic investigations
Hematological tests
Full blood, Hb, differential count, Erythrocyte sedimentation rate
(ESR), Plasma viscosity, c-reactive protein (CRP), gama globulin.
Urinalysis
Protein, Blood.
Biochemical
Urea and creatinine, Uric acid, Calcium, Alkaline phosphatase,
Angiotensin-converting enzyme, Urinary albumin : creatinine ratio.
Serological
IgM rheumatoid factor, Anticyclic citrullinated peptides (ACPA),
Antinuclear factors, Anti-Ro, Anti-La, Anti-dsDNA, Anti-Sm, Anti-RNP, Antineutrophil
cytoplasmic antibodies.
Imaging
Plain radiography (X-rays), Ultrasonography, Isotope bone scan, MRI, CT
scanning, Radionuclide imaging, Dual-energy X-ray absorptiometry (DXA).
Joint aspiration
Polarised light microscopy, Bacteriology, Biopsy and histology.
Synovial fluid analysis
Arthrocentesis done after injures, suspected infection, acute
synovitis in adult, chronic synovitis.
Bone biopsy
open (surgery), closed (needle).
Arthroscopy
Diagnostic, Therapeutic.
Electro diagnosis
Motor nerve conduction, Sensory nerve conduction,
Electromyography.
How to report the orthopedics and fractures x-ray?
(example))
First:
This is a plain x-ray, A-P view.
Taking for Ahmed rami, 30 years old.
At the 20
th
of October 2014.
Right or left??
Showing:
"Check for any abnormality in"
The lower third of the right thigh (femur), knee joint, upper part of tibia & fibula.
Good quality of skeletally mature (if epiphyseal plate is fused).
I don’t accept this x-ray because it doesn’t show the other view .. (rule of 2).
There is a back slap from above the knee to ….
Disrupted skin, sheels in subcutaneous, swelling & the muscle is normal.
Any fracture describe it … ((transverse, oblique or spiral, impacted, green stick,
compression)).
Any displacement describe it … ((shifted, angulated, overlapped, impacted,
twisted)).

Don’t forget the proximal and distal joints.
Soft tissue study:
Unless examined early, these are liable to be forgotten.
looks for:
muscular planes.
bulging around joints as in rheumatoid arthritis.
presence of calcification.
Bones:
Looks for deformity, irregularity.
Cortex for: Periosteal surface (periosteal reaction).
Endosteal surface.
Trabecular structure.
Density: increase in density (sclerosis)
Decrease as in osteoporosis.
The joint:
The radiographic joint consists of the articulating bones and the space between
them.
The space occupied with radiolucent cartilage.
Looks for narrowing of this space, flattening, erosion, sclerosis.
Rule of 2:
2 views A.P and lateral for example.
2 occasions after 10 days in scaphoid fracture for example.
2 limbs in children to compare with the other limb.
2 joints proximal and distal.
2 bones radius and ulna for example.
2 opinion two doctors.

Part5
: Acute compartment syndrome
What is it?
Compartment syndrome is defined as increased pressure within a compartment of the
body, commonly in the arm or leg. Acute compartment syndrome is caused by trauma.
Common causes:
Major trauma e.g. car crash
Lower leg or radial/ulnar fractures
Crush injuries
Plaster of Paris casts – causing restriction
Burns
Pathophysiology:
Muscular compartments are enclosed by fascia, which defines the borders of each
compartment. Fascia doesn’t stretch, therefore even small
amounts of bleeding and/or tissue edema within a given compartment can result in
significant increases in pressure. The increase in pressure reduces the incoming blood
supply of the compartment, which can result in tissues being deprived of oxygen.
In addition venous and lymphatic drainage from the compartment is also compromised,
adding to the problem by increasing compartment pressure even further, leading to a
vicious cycle of continually increasing pressure. As a result, if this is left untreated tissue
can become hypoxic and be permanently damaged, potentially resulting in loss of
function or loss of a limb completely.
If Compartment Syndrome is not treated quickly and effectively, skeletal muscle can begin
to rapidly break down, this is known as rhabdomyolysis. One of the breakdown products
is myoglobin, which can damage the kidneys leading to acute renal failure.
History and Examination:
Symptoms & signs of limb ischemia are best remembered by the 6 Ps!
Painful
Pale
Pulseless

Paraesthesia
Paralysis
Perishingly cold
Pain is often out of proportion to the clinical situation. An example may be a post-op
Orthopedic patient who despite large amounts of both IV & hourly oral morphine continues
to have severe pain in the associated limb.
Diagnosis:
Compartment Syndrome is primarily a clinical diagnosis but pressure gauges can be used if
the diagnosis is not clear.
Treatment:
The only treatment is fasciotomy, a surgical procedure which releases the pressure in the
affected compartment, in addition to releasing the pressure in all other surrounding
compartments. This may need to be done multiple times in some cases.
How to approach compartment syndrome as a junior doctor:
History and examination
Observations
Pain control (do not forget this!)
If affected limb is in a cast –> Split the cast!!!
Ensure patient is nil by mouth – in case they need an emergency fasciotomy
Make seniors aware and request urgent review – ensure you communicate your
concern
Part6
: Notes
Causes of bone deformity:
1. Congenital pseudarthrosis.
2. Bone softening, rickets.
3. Dysplasia, exostosis.
4. Plate injury.
5. Fracture malunion.
6. Pagets’ disease.
Causes of joint deformity:
1. Skin contracture (burn).
2. Fascial contracure (dupuytrens’).
3. Muscle contracture (volkmanns’)
4. Muscle imbalance.
5. Joint instability (torn ligament).
6. Joint destruction (arthritis).

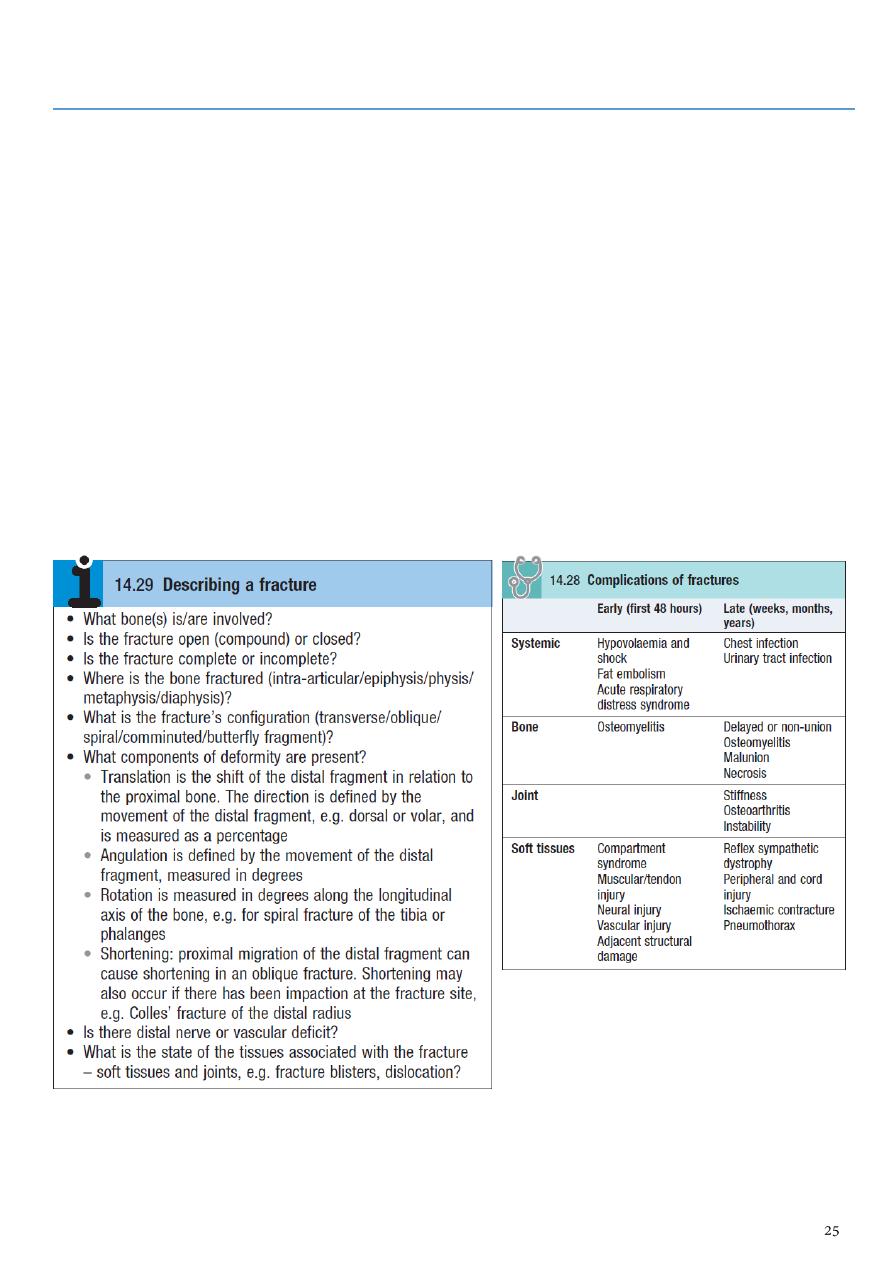
General treatment of fracture:
1- At the accident site:
Air way.
Protection cervical spine.
Breathing.
Bleeding stoppage by direct pressure OR by tourniquets (time).
Circulation (Fluid replacement).
Examination.
Analgesia.
Splintage to reduce pain, blood loss.
Transport by proper stretcher.
2- In the hospital:
Rapid survey.
Constant re-evaluation.
Definitive care.
Manipulation (Reduction) Conservative (closed), Operative (open).
Hold:
1.Continuous traction
2.Skin traction
3.Skeletal traction
4.Fixed traction
5.Balanced traction
6.Combined traction
Functional bracing.
Internal fixation:
o Screw.
o Plate.
o Wire.
o L-plate.
o Compression screw.
o K-nail.
External fixation.
3- Exercise (physiotherapy):
Prevention edema: by elevation.
Active exercise:So to pump edema fluid and stimulate circulation ,prevent soft tissue
adhesion &promotes fracture healing.

Internal fixation:
Indications:
1. Failure conservative.
2. Fracture two bones.
3. Intra articular fracture.
4. Pathological fracture.
5. In difficulty nursing patient.
Complications:
1. Infection.
2. Non-union.
3. Implant failure.
4. Re fracture.
External fixation:
Indications:
1. Fracture with severe soft tissue injuries.
2. Complicated fracture.
3. Infected non-union.
4. Fracture pelvis.
5. Multiple injuries.
6. Bone lengthening.
7. Plastic surgery (flap).
8. Fracture neck femur.
Complications:-
1. Over distraction Reduce load transmission.
2. Pin tract infection.