
EXAMINATION
OF THE SPINEبسم الله الرحمن الرحيم
1
SYMPTOMS
PainSciatica
Stiffness
Deformity
Numbness or paraesthesia
Urinary symptoms
Other
2
How to Start
• IPEEP• INTRODUCE.
• PERMISSION.
• EXPLANTION.
• EXPOSURE.
• POSITION.
3
The Apley System
All joint examinations follow this system:Look
Feel
Move : Active then Passive
Special Tests
Radiograpgy.
4
Patient in standing
5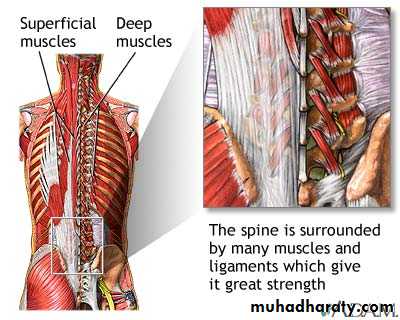
6
7
INSPECTION
BONE CONTURES.SOFT TISSUE CONTOURES.
COLOUR AND TEXTURE OF THE SKIN.SCARS OR SINUSES.
8
9
10

11
12
13
14
PALPATION
SKIN TEMPERATURE.BONE CONTOURS.
SOFT TISSUES CONTOURS:Palpate swellings
LOCAL TENDERNESS.
15
16
MOVEMENTS
Spinal joints :FLEXION .
EXTENSION.
LATERAL FLEXION.
ROTATION.
PAIN ON MOVEMENT.
MUSCLE SPASM.
17
Costo-vertebral joints
Ranged indicated by chest expansion.Sacroiliac joints
Pain on movement imparted by lateral compression of pelvis.MOVEMENTS
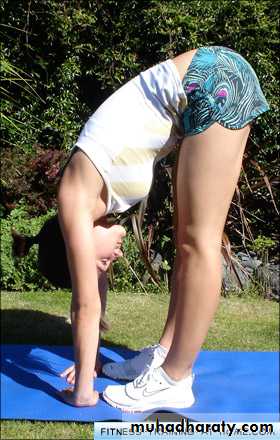
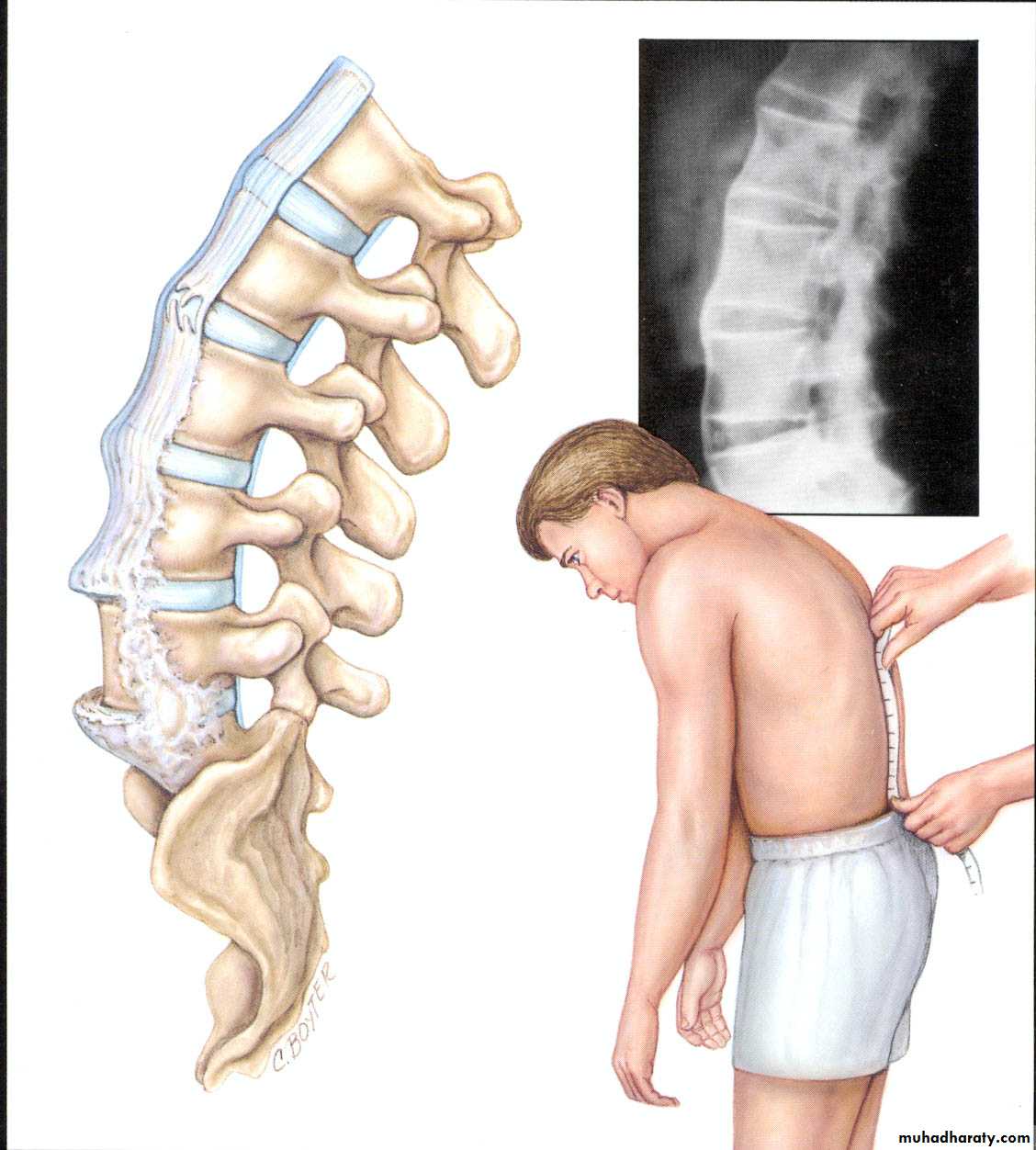
18FLEXION .
Instruct the patient to stretch his fingers towards hIs toes, keepIng the knees straight.It is important to Judge what proportion of the movement occurs at the spine and how much IS contrIbuted by hIp flexion Some patients can almost reach their toes, despite a stiff back,
simply by flexing unusually far at the hips. (Normally the hamstrings limit hip flexion to about 90 degrees when the knees are straight.)
The range may be expressed as a percentage of the normal,. or
as the distance by which the fingers fall to reach the floor.
19
due entirely to movement at the hips,
the hamstrings being unusually lax. In estimatingtrunk flexion it is important to judge how much of the movement occurs at the
spinal joints and how much at the hips.
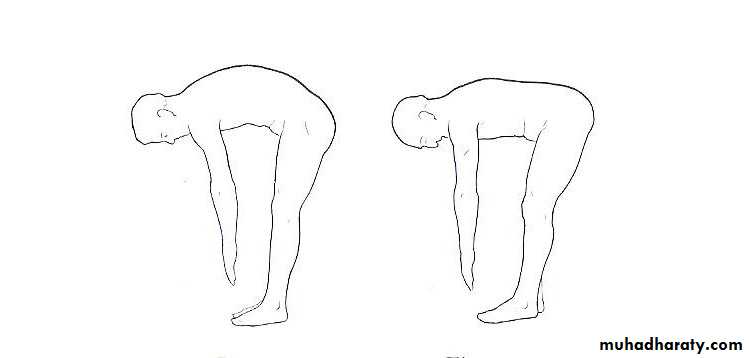
Normal flexion of lumbar spine
Apparent or false flexionApparent or false flexion
20

21
22
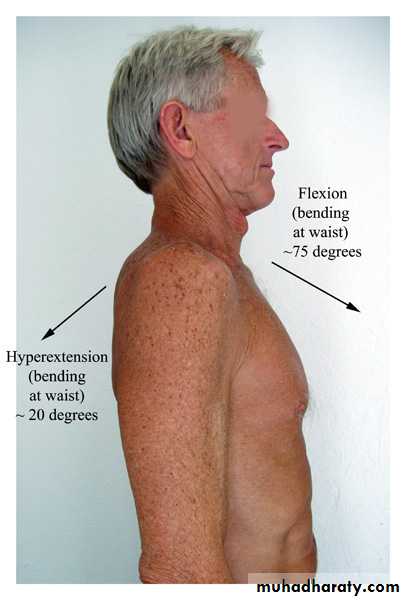
EXTENSION
Instruct the patient to arch the spine backwards, lookIng up at the ceiling.Judge the range and express approximately as a percentage of
the normal.
23
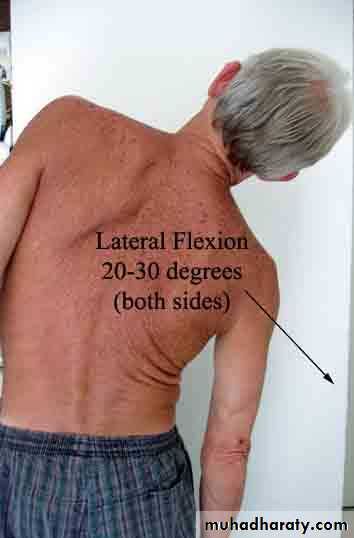
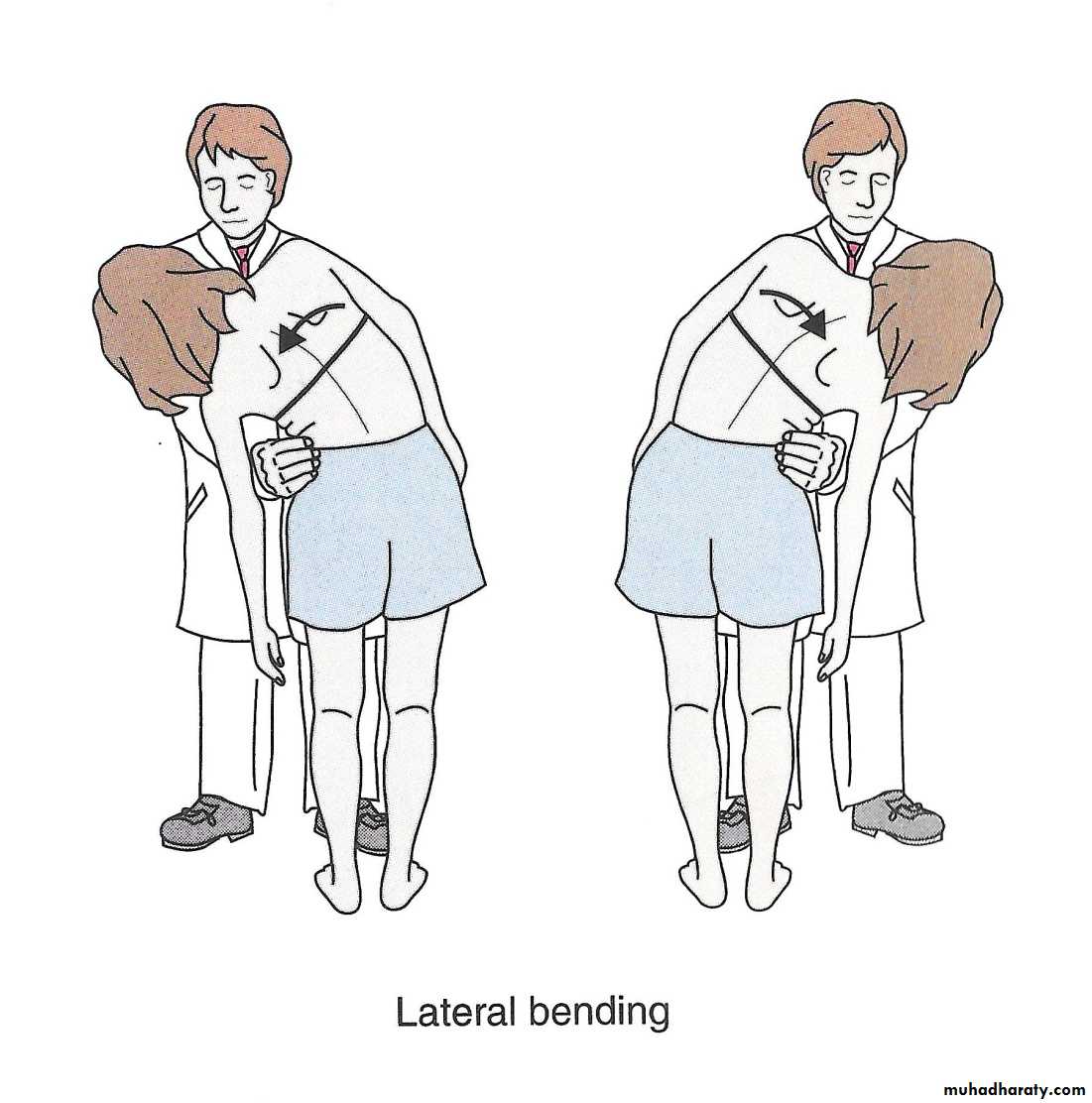
Lateral flexion
Instruct the patient to side each hand Inturn down the lateral side of the corresponding thigh. Observe the
range.
24
25
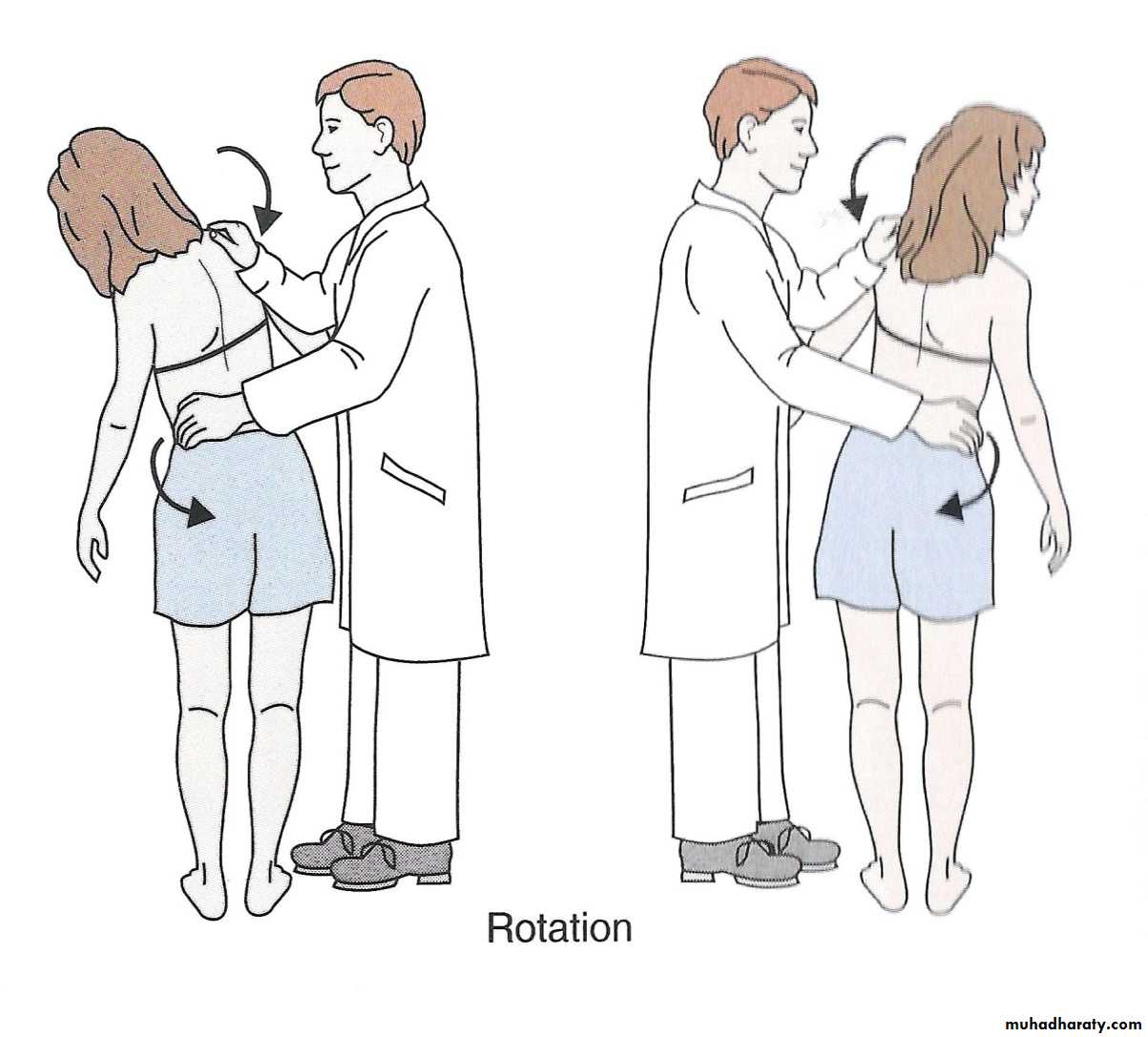
Rotation:
With the feet fixed, the patient rotates the shoulderstowards each side in turn. Note the range of spinal rotation as distinct
from that which occurs at the knees and hips.
26
Examination of the patientin recumbent
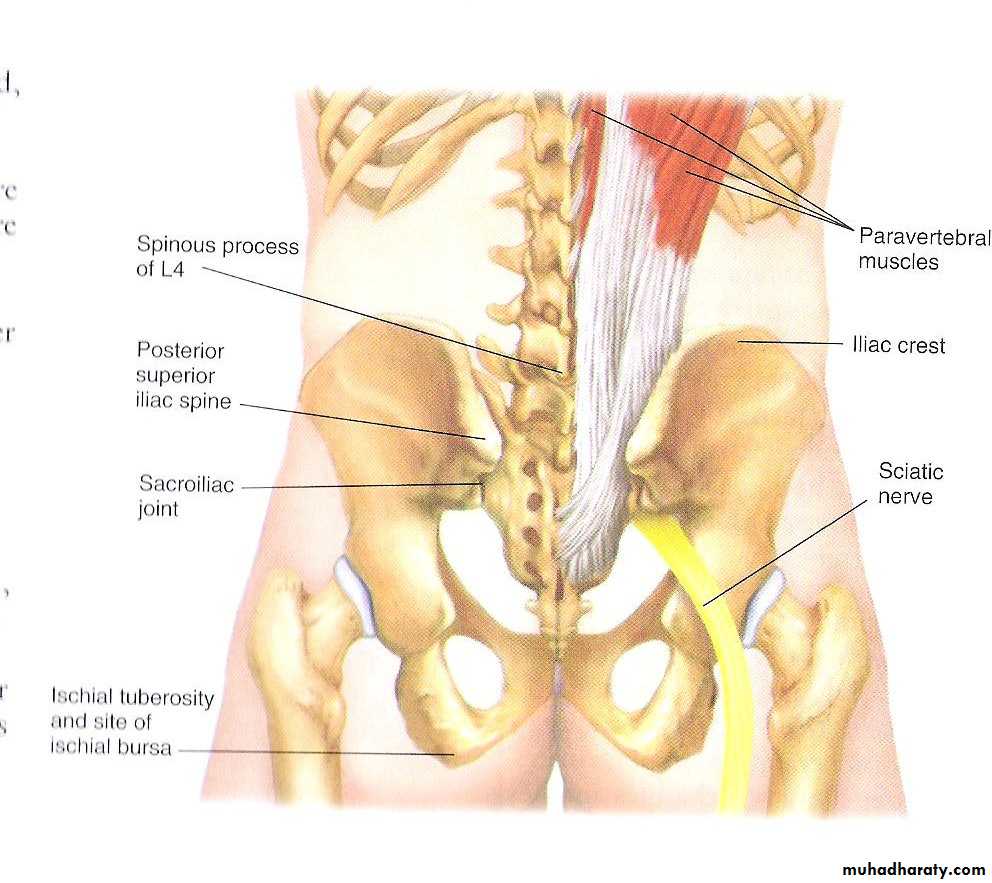
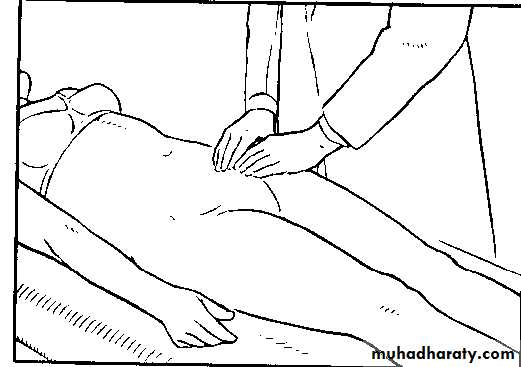
27Palpation of the iliac fossa.
Examine specifically for abcess.
28
Palpation of the iliac fossae and groins is an essential step in the
It should be rememberedthat a 'psoas' abscess originating from a tuberculous lesion of the
lumbar spine first becomes palpable deep in the iliac fossa. Such an
abscess is felt most easily by pressing the flat palmar surface of the hand
and fingers against the flat inner aspect of the iliac bone
29
Signs with patient lying face downwards
Bony outlinesTenderness
Sensations and Power
Femoral stretch test
30
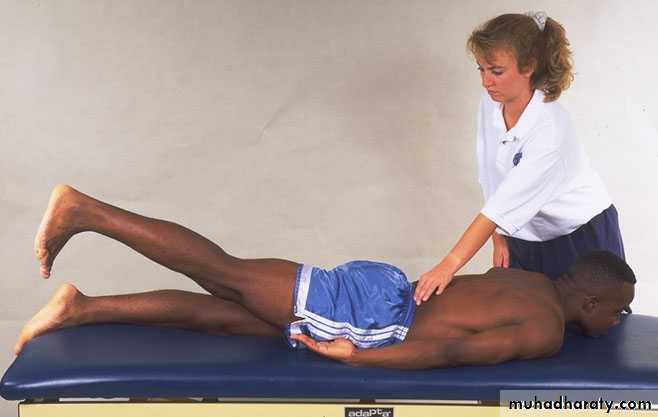
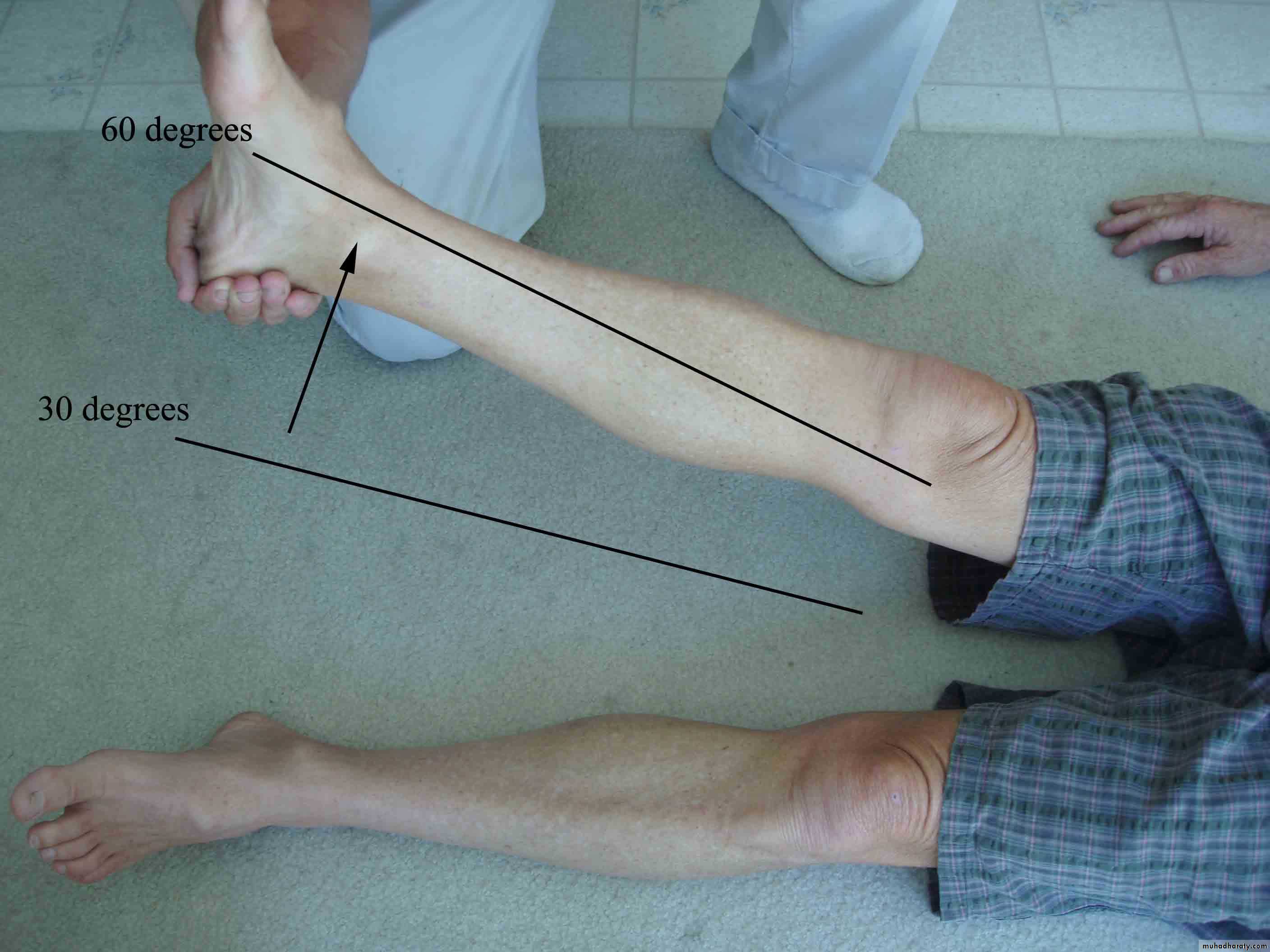
Femoral stretch test
Looking for femoral nerve root irritation L2-4Patient prone, ant thigh fixed to couch, flex each knee
Pain felt in anterior compartment of the thigh
Aggravated further by extension of hip
31
32
NEUROLOGICAL STATE OF LOWER LIMB
Straight leg rasing test.Muscular system.
Sensory sysytem.
Reflexes.
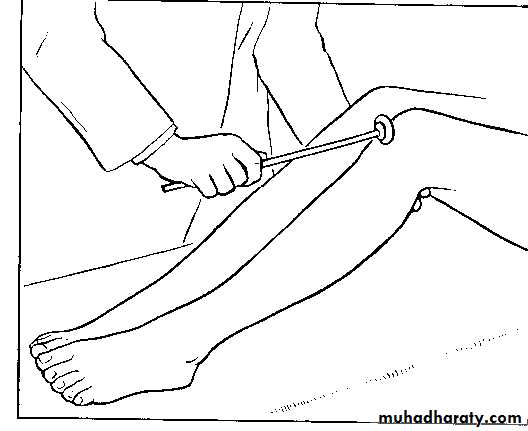
33
Signs with patient lying on his back
Straight leg raising test (sciatic stretch)34


35
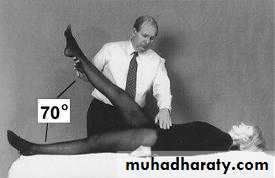
Straight leg raising test
Holding the knee straight, lift each lowerlimb in turn to determine the range of pain-free movement (normal
= 90 degrees; often more in women)
When associated with
clearly defined sciatica (and in the absence of gross disease of the hip),
marked Impairment of straight leg raising by pain suggests mechanical
Interference wIth one or more of the roots of the sciatic nerve.
The
pain is easily explained.
Even a normal sciatic nerve is tautened by
straight leg raising, though not to the point of causing pain by
dragging on the meningeal sheath that encloses the nerve root.
36
NORMALLY UP TO 90 DEGREE
37
38
39

40
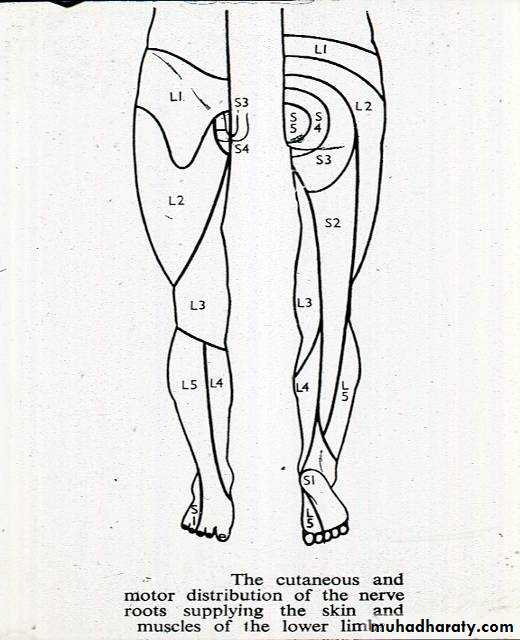
Cutaneous distribution of nerve roots
41
Circulation in the limbs
Femoral artery pulsationPopliteal artery pulsation
Dorsalis and posterior tibial artery pulsation
Rectal examination
42Muscular system
Examine the muscles for wasting, hypertrophy, and fasciculation. Note the tone.and test the power ,
comparing it with its counterpart in the opposite 11mb.
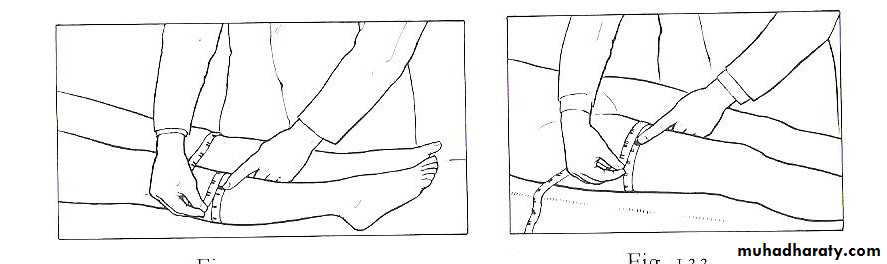
Circumiferential measurement is a reliable method of comparing
(calf muscles and thigh, the girth being measured at the widest part or equator
43
Muscle Power Testing MRC Scale
0 Total paralysis1 Barely detectable contracture
2 Not enough to act against gravity
3 Strong enough to act against gravity
4 Still stronger but less than normal
5 Full power
44

45
SENSORY SYSTEM
For touch ,pin prick.
Deep stimuli .
Joint position.
Vibration.
Heat and cold examination
46
SWEATING.
Feel the digit if it is moist , or dry.
Sweating depend upon intact sudomotor nerve fibers.
47
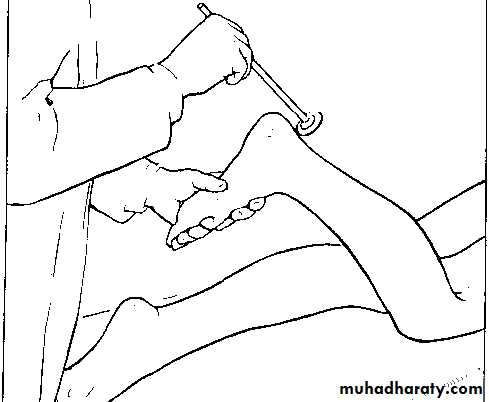
REFLEXES
.48
The patellar reflex is dependent mainly on L.4 nerve
49
Testing the calcaneal reflex (mainly S. I nerve),
50
Examination of potential extrinsic sources of neck symptoms.
Examination should include.Abdomen,
pelvis,
rectal examination,
lower limbs
Peripheral vascular system.
51
Sometimes there are no local symptoms to indicate that the spine is the seat of the disorder,
Pain referred entirely to the buttock or to the lower 11mb.
often complain only of pain 'in the hip' or 'in the leg' when true source of the trouble is the lumbar spine.
Conversely, the symptoms may suggest a spinal lesion when in fact they arise from abdomen, pelvis, or lower limb, or from occlusion of artery or a leaking aortic aneurysm.
52
53
General examinations
ImagingPlain x-rays
AP and lateral views
Oblique views
PA view of S.I. Joint
Computed tomography (with mylography)
MR imaging
Radioisotope scanning
Discography and facet joint arthrography
54

55

56

57
58
CLASSIFICATION OF DISORDERS OF THE TRUNK AND SPINE
59
CONGENIT AL ABNORMALITIES
Lumbar and sacral variationsHemivertebra
Spina bifida
60
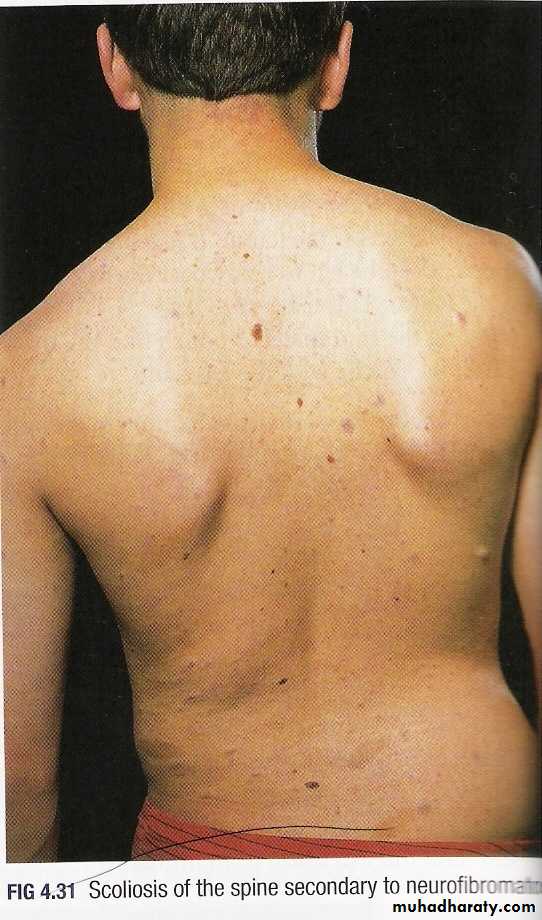
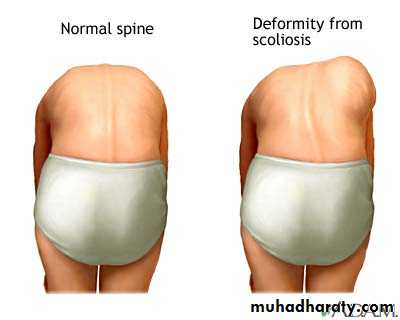
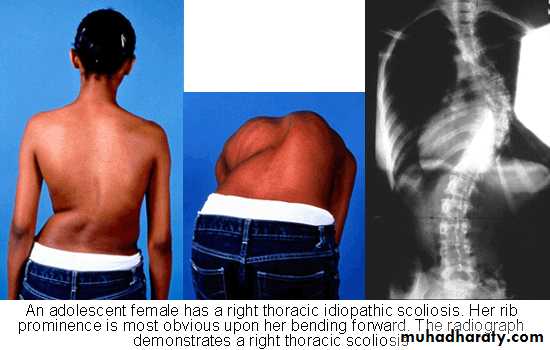
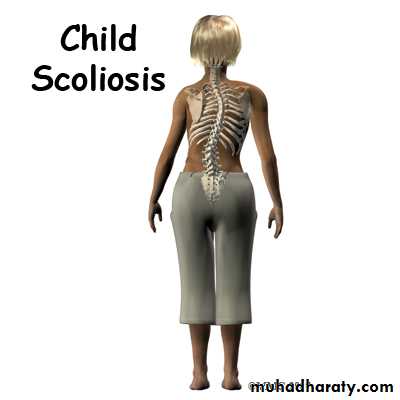
DEFORMITIES
ScoliosisKyphosis
Lordosis
61
INFECTIONS OF BONE
Tuberculosis of the thoracic or lumbar spinePyogenic infection of the thoracic or lumbar spine
62
ARTHRITIS OF THE SPINAL JOINTS
Rheumatoid arthritisOsteoarthritis
Ankylosing spondylitis
63
OSTEOCHONDRITIS
Scheuermann's vertebral osteochondritisCalve's vertebral osteochondritis
64
MECHANICAL DERANGEMENTS
Prolapsed lumbar intervertebral discAcute lumbago
Spondylolysis
Spondy lolisthesis
Spinal stenosis
65
TUMOURS
Tumours in relation to thecord, or nerve roots
Other tumours of the trunk
66
CHRONIC STRAINS
Chronic lower lumbar ligamentous strainCoccydynia
67
MISCELLANEOUS
FibrositisSenile osteoporosis
68
DISORDERS OF THE SACRO- ILIAC JOINTS
Tuberculosis of a sacro-iliac joint
Ankylosing spondylitis
Other forms of arthritis
Sacro-iliac ligamentous strain
69