Amenorrhea
objectivesTo know what is amenorrhea
To understand aetiology and management
To make students able to solve the patient’s problem with amenorrhea
Definition
Amenorrhoea is defined as the absence of menstruation.It may be classified as either physiological and pathological
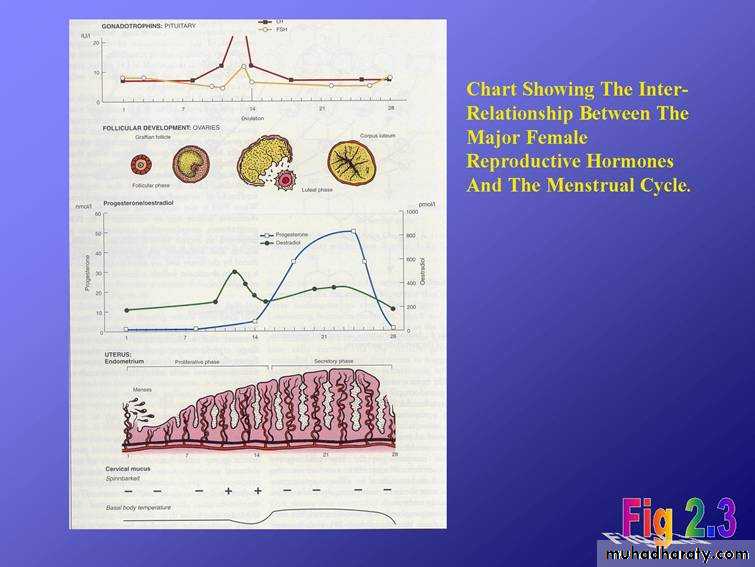
physiological amenorrhea
In pregnancy, lactation ,prior to the onset of puberty and after menopause
Pathological
Primary amenorrhoea describes the condition in which girls fail to develop secondary sexual characteristics by 14 years of age or fail to menstruate by 16 years of age. Secondary amenorrhoea describes the cessation of menstruation for more than 6 months in a normal female of reproductive age that is not due to pregnancyOligomenorrhea is defined as menses
occurring at intervals longer than 35 days
Classification
• Reproductive outflow tract disorders.• Ovarian disorders.
• Pituitary disorders.
• Hypothalamic disorders.
Causes of amenorrhoea
Reproductive outflow tract disorders• Asherman's syndrome
• Mullerian agenesis
• Transverse vaginal septum
• Imperforate hymen
• Testicular feminization syndrome
Ovarian disorders
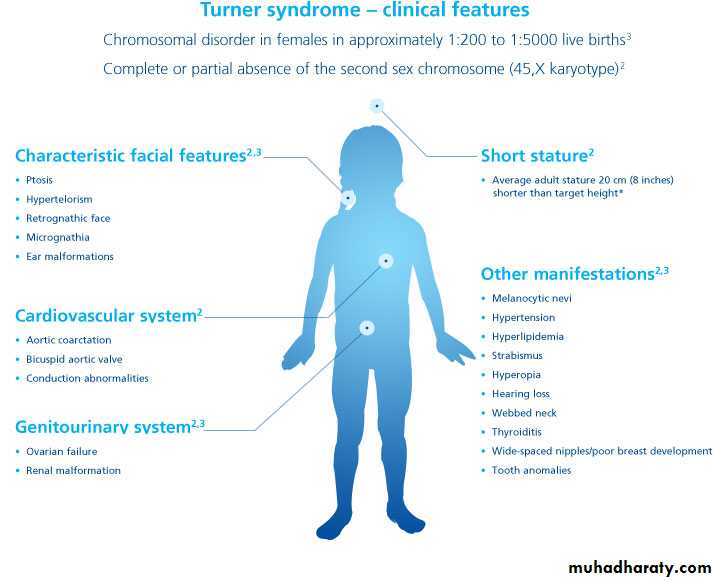
• Anovulation , e.g . polycystic ovarian syndrome• Gonadal dysgenesis, e.g. Turner's syndrome
• Premature ovarian failure
• Resistant ovary syndrome
Pituitary disorders
• Adenomas such as prolactinoma• Pituitary necrosis, e.g. Sheehan's syndrome
Hypothalamic malfunctions
• Resulting from excessive exercise• Resulting from weight loss/anorexia nervosa • Resulting from stress
• Craniopharyngioma
• Kallman's syndrom
Reproductive outflow tract abnormalities
• These may result from abnormal sexual development,• Mullerian agenesis is a congenital malformation where the Mullerian ducts fail to develop resulting in an absent uterus and variable malformations of the vagina..
2-Asherman's syndrome
This refers to the presence of intrauterine adhesions, which prevent endometrial proliferation (and thus menstruation). The commonest cause of Asherman's syndrome in developed countries is over-vigorous uterine curettage (e.g. at uterine evacuation)..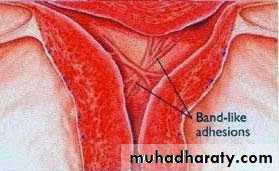
3-Tuberculosis of the uterus
has similar signs and symptoms with asherman syndrome, and should be considered in the differential diagnosis in areas where the infection is endemicOvarian disorders
• Ovarian failure• is the term used to describe the condition in which the stock of functional primordial follicles is exhausted and normal follicular development fails to occur despite the pituitary producing increasing amounts of gonadotrophins (luteinizing hormone [LH ] and follicle-stimulating hormone [FSH]).
Obviously in normal women ovarian failure occurs at the menopause (at a mean age of 51 years).
In some women, however, it may happen early (premature ovarian failure), possibly as a result of chemotherapy or radiotherapy, or in association with autoimmune disease.
2-resistant ovary syndrome
It has recently become clear that some women present with symptoms, signs and blood results identical to those of ovarian failure but that they do in fact have viable follicles in the ovary.These follicles are unresponsive to elevated gonadotrophin levels, giving rise to the term resistant ovary syndrome women with the resistant ovary syndrome may occasionally ovulate and conceive
3-p0lycystic ovary syndrome
The other common ovarian disorder leading to anovulation and amenorrhoea is PCOS

Pituitary disorders
1-prolactinomaThe commonest of these, the prolactinoma, which is microadenoma secretes prolactin. This causes the symptom of galactorrhoea and inhibits gonadotrophin activity, leading to oligomenorrhoea or amenorrhoea. Prolactinomas normally respond very well to treatment with bromocriptine or to newer drugs such as cabergoline
Women with significantly elevated prolactin levels (> 1000 pmol/L) should therefore be further investigated with computerized tomography (CT) scanning or magnetic resonance imaging (MRI) to visualize the pituitary.
Prolactin levels may alternatively be elevated as a side effect of some drug treatments (e.g. phenothiazines), and thus is it worth reviewing the drug history in any patient with hyperprolactinaemia
Hypothalamic disorders
Excessive weight loss (to 15-20 per cent below ideal body weight) and/or excessive exercise can lead to amenorrhoea by switching off hypothalamic stimulation of the pituitary (hypogondotrophic hypogonadism).Such women will have low (or normal) gonadotrophin levels
Clinical features of oligomenorrhoea/amenorrhoea
• A comprehensive history will include:• • developmental history,
• • age of onset of menarche,
• • presence or absence of cyclical symptoms.t-
• • history of chronic illness,
• • excessive weight loss/presence of an eating disorder,
• • excessive exercise
, • history or family history of anosmia,
• menstrual/contraceptive and reproductive history,
• past medical and surgical histories,
• presence of menopausal symptoms,
• current medications,
• family history of premature menopause
• development of any virilizing signs
or galactorrhoea (milk discharge from breasts),• psychological history,
• recent stressful events (past or present history of depression or an eating disorder).
Clinical examination
• Height:an abnormality in appropriate height for age may reflect an underlying chromosomal disorder (patients with Turner's syndrome are often short, whereas patients with androgen insensitivity are often tall). •
• Development of secondary sexual characteristics or any evidence of abnormal virilization
• Visual field disturbance or papilloedema may imply a pituitary lesion
Breast examination for presence of secodary sexual characters and galactorrhea.
Inspection of external genitalia may suspect imperforated hymen
Rectal examination in single ladies may detect abscent uterus
• Pelvic examination( in married ladies) may detect any pelvic organs anomalies
Also look for evidence of atrophic effects of hypo-oestrogenism within the lower genital tract
InvestigationsStep 1
Initial hormone tests
• Pregnancy test
• Prolactin
• Thyroid function
• LH and FSH
• Testosterone
Imaging studies
*Ultrasound:Determine the presence, state and size
of ovaries and any follicular activity.Determine the presence and size of
uterusChromosomal analysis:
chromosomal analysis and Karyotypeshould be done in primary amenorrhea if the diagnosis not clear with suspicion of chromosomal anomaly.
In Karyotype A buccal smear and examination of the polymorphnuclear leucocytes to determine if chromatin positive (XX) or chromatin negative
(XO or XY) and some time full chromosomal analysis may be need
Progesterone withdrawal test
This involves giving a progesterone (such as medroxyprogesterone acetate 10 mg) for 5 days, and then stopping.
If the outflow tract (uterus a d vagina) is normal, and there is sufficient endogenous oestrogen to induce endometrial proliferation, progesterone will decidualize the endometrium.
On withdrawing the progesterone, the decidualized endometrium will break down, and menstruation will ensue.
Step 2
If the patient does not bleed in response to progesterone, she should be given orally active oestrogen (e.g. oestradiol 2 mg) for 21 days, followed by progesterone as above.If the patient still fails to bleed in response to this treatment, the diagnosis is one of an outflow tract abnormality.
If bleeding does occur in response to sequential oestrogen and progesterone, this indicates the problem is in the hypothalamo-pitl!itaryovarian axis
Step 3
Having excluded an outflow tract disorder, measurement of the LH and FSH levels should be repeated.Ideally, this should be done 6 weeks after the initial tests were performed, and 2 weeks after administration of either oestrogen or progesteroneI
. Elevated LH and FS H levels (> 40 lUlL and 30 lUlL, respectively) on two or more occasions at least 6 weeks apart and in the absence of menstruation suggest ovarian failure.
If LH and FSH levels are not elevated, and the above scheme of investigation has been followed, the disorder can be reliably localized to the hypothalamus.
This is commonly due to stress or weight loss (including weight loss due to anorexia nervosa), but may also be seen in severe systemic illness
Laproscopy
Laproscopy rarely used to assess
pelvic organ. It is useful in:* cases which there is doubt
about the nature of the gonads.*cases where ovarian biopsy is
needed to determine presence ofprimordial oocytes
Treatment
The treatment of amenorrhoea depends somewhat on the causeIn women in whom endogenous oestrogen levels are low (e.g. ovarian failure or hypogonadotrophic hypogonadism), oestrogen -and progesterone replacement (e.g. in the form of HRT)
In Cases of Turner's syndrome
Induce breast development by verygradually increasing oestrogen doses
then change to definitive treatment of
hormone replacement therapy (estrogen
and progestrone). They have no hope to
achieve pregnancy.
In hypogonadotrophic hypogonadism
who seek fertility will need therapy with
either human menopausal gonadotrophin injection or
gonadotrophin releasing hormone (GnRH)
androgen insensitivity
* Excision of gonads as this gonad is atestis and there is a malignant potential
in about 30% of cases
*Creation of neovagina to permit sexual
intercourse.*Treatment with oestrogen to augment
breast development and preventosteoporosis
Imperforate hymen
The imperforate hymen may at two agesIt may present in:
1-Early childhood
When the infant presents with a
bulging hymen behind which is a
mucocele, the vagina expanded by
vaginal secretions of mucus.
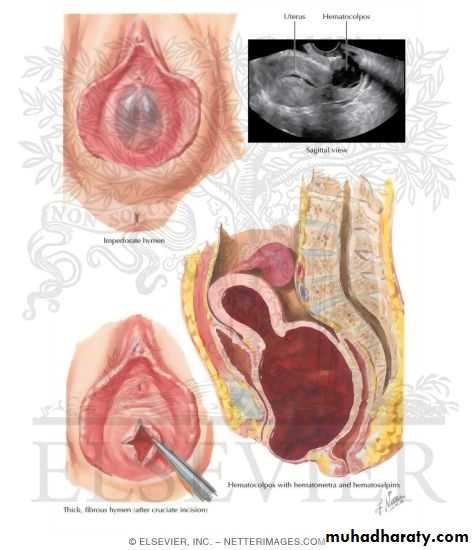
2-At puberty
The very distensible features of vagina allow quite large quantities of blood to collect insome cases. This situation is known as haematocolpos.
When some blood does accumulate within the uterine cavity it is known as a
haematometraClinical assessment
A pubertal girl complains of intermittent cyclical abdominal pain.The pain is due to dysmenorrhoea associated with
the accumulation of menstrual blood within the vagina. As the mass enlarges there may be associated difficulty with micturition and defaecation and even associated with retension of urine in some cases
Examination:
The patient has normal height & normal
secondary sexual characteristic.Occasionally there is abdominal mass
Pelvic examination by inspection of external genitalia showed a tense bulging bluish membrane (which is the hymen) closing the introitus
Ultrasound reveals blood collection in the vagina and uterus
treatment
After explanation of the condition and obtaining parents consent,a cruciate incision (+) in the hymen allows drainage of the retained menstrual blood with good antibiotic cover to prevent infection . From medico-legal point of view, the girl mustbe given a report confirm that the hymen was opened by surgical operation as treatment
Medical treatment
Anovulation:In patient desire pregnancy, ovulation
induction agents as clomiphene orgonadotrophins may be used.
In patient not desire pregnancy can use
combined oral contraceptive pills or cyclic
progestogens
Premature menopause is managed as
menopause use hormone replacementtherapy (HRT) to prevent osteoporosis
hyperprolactinemia
Use Dopamine agonists (Bromocriptine) 2.5mgdaily for three days then 2.5 mg twice a day for
six months.
It should be stopped if pregnancy
occurs. Cycle retain once Prolactin levels are
retain normal.
Surgical treatment should be performed for
patients with significant visual field defects orsymptoms that can not be relieved by medical
therapy
Surgical treatment
Some pituitary and hypothalamic tumors
may require surgery and, in some cases,
radiation.
Asherman's syndrome requires
hysteroscopic lysis of the intrauterineadhesions