Dr.Hadeel M.Al-Hialy
M.B.Ch.B. F.I.C.M.S
small bowel
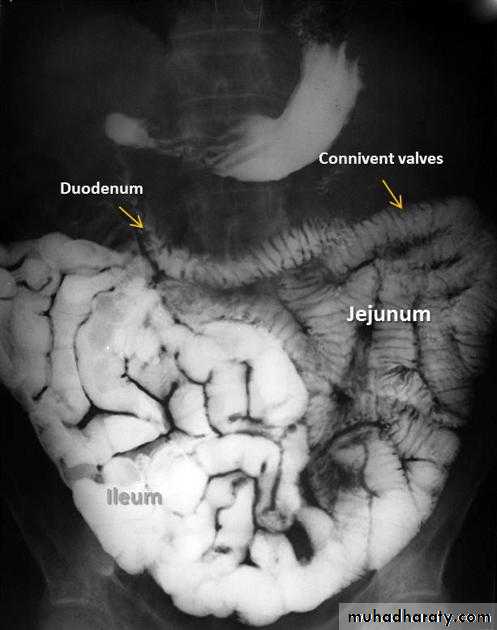
Barium follow-throughBarium follow-through
A barium follow-through procedure is a type of medical imaging technique. It is used to evaluate the presence of disease in a person's small intestine.Examination
Barium follow through x-rayThe patient drinks a contrast medium containing barium sulfate. This contrast medium appears white on x-rays, and shows the outline of the internal lining of the bowel. X-ray images are taken as the contrast moves through the intestine, commonly at 0 minutes, 20 minutes, 40 minutes and 90 minutes. This enables the radiologist to assess the bowel as it becomes visible. The test is completed when the Barium is visualised in the terminal ileum and Caecum, which marks the beginning of the large bowel. This is one of the most common places for pathology of the bowel to be found, therefore imaging of this structure is crucial. The test length varies from patient to patient as bowel motility is highly variable.
The barium is non-toxic and passed out normally as a stool, although the appearance may be paler than usual.
Pathology
The Barium follow-through test is used to diagnose conditions of the small bowel, most commonly
Crohn's disease
Ulcerative colitis
Bowel cancer

Malabsorption

MalabsorptionMalabsorption is difficulty absorbing nutrients from food substances
causes of malabsorption include:Celiac disease
some medications used to treat obesity
Certain types of cancer (lymphoma, pancreatic cancer, gastrinomas)
Certain types of surgery (gastrectomy with gastrojejunostomy,
surgical treatments for obesity, partial or complete removal of the ileum)
Chronic liver disease
Crohn's disease
Damage from radiation treatments
Parasite infection, including Giardia lamblia
Soy milk protein intolerance
Whipple's disease
Vitamin B12 malabsorption may be due to:
Pernicious anemia
Bowel resection
Radiological appearance of Mal absorption syndrome
* Loss of normal feathery appearance of the small bowel
* Flocculation & segmentation of the Ba
* Widening of the spaces between bowel loops due to mucosal edema
*+/_ spiky appearance of the small bowel loops


Inflammatory bowel disease
Due to the overlap in clinical presentation of Crohn's disease (CD) and ulcerative colitis (UC), imaging often has a role to play in distinguishing the two. Distinguishing features include:bowel involved
CD : small bowel 70 - 80%, only 15 - 20% have only colonic involvement
UC : rectal involvement 95%, with terminal ileum only involved in pancolitis (backwash ileitis)
distribution
CD : skip lesions typical
UC : continuous disease from rectum up
gender
CD : no gender preference
UC : male predilection

Crohn's disease
is an idiopathic, chronic inflammatory process of the gastrointestinal tract that can affect any part of the tract from the mouth to the anus. Individuals with this condition often experience periods of symptomatic relapse and remission.ages of 15 and 25 years of age, with no gender predilection . There is a familial component and incidence also varies with geographical location..
Radiographic features
The characteristic of Crohn's disease is the presence of skip lesions. The frequency with which various parts of the gastrointestinal tract are affected varies widely :small bowel : 70 - 80 % + regional ileitis
small and large bowel : 50 % + regional ileitis
large bowel only : 15 - 20 %
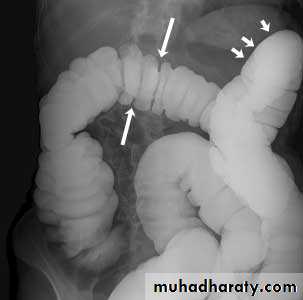
X-Ray Manifestations
• Squaring of the folds-early manifestation from obstructive lymphedema• Apthous ulcers-small nodular filling defects (mound of edema) with central ulceration
• Skip lesions-discontinuous involvement of the bowel with intervening normal areas
• Cobblestoning-irregular, blanket-like appearance to bowel wall caused by criss-crossing longitudinal and transverse ulcers separated by areas of edema
• Pseudopolyps-islands of hyperplastic mucosa between denuded areas of mucosa
• Filiform post-inflammatory polyps
• Pseudodiverticula-from bulging area of normal wall opposite side of scarring from disease, usually on anti-mesenteric side
• String-sign-marked narrowing of terminal ileum (usually) from a combination of edema, spasm and (sometimes, but not always) fibrosis; frequently associated with proximal dilatation

Ulcerative colitis (UC)is an inflammatory bowel disease which predominantly affects the colon, but also has extra intestinal manifestations.

Location
o Begins in rectum with retrograde progressiono Rectosigmoid involved 95%; continuous involvement of left colon
oTerminal ileum in 5-10% with backwash ileitis
Ulcerative colitis (UC)
X-Ray ManifestationsAcute inflammatory stage
o Spasm and irritability
o Fine mucosal granularity earliest finding on air-contrast BE
o Spiculated, serrated bowel margins from tiny, multiple ulcerations
o Collar button ulcers
o Thumb printing from edema of wall
o Pseudopolyps
o Widening of the pre-sacral space
Subacute stage
o Coarser, more granular mucosa
o Inflammatory polyps= frond-like lesions of inflamed mucosa
Chronic stage
o Shortening of the colon-may be from spasm of longitudinal muscles or from irreversible fibrosis (lead-pipe colon)
o Loss of haustrations on left side of colon



Barium enema examination demonstrates loss of haustral folds in the entire descendingcolon with small ulcerations suggested. The colon has a "lead-pipe" appearance. The distribution and appearance are suggestive of ulcerative colitis.

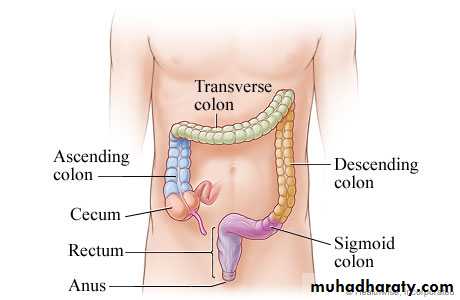
The large intestine (colon) extends from the cecum to the anus and includes the ascending colon, the transverse colon, the descending colon, the sigmoid colon, and the rectum.
Ba-enema
A barium enema, or lower gastrointestinal (GI) examination, is an X-ray examination of the large intestine (colon and rectum). The test is used to help diagnose diseases and other problems that affect the large intestine. To make the intestine visible on an X-ray picture, the colon is filled with a contrast material containing barium. This is done by pouring the contrast material through a tube inserted into the anus. The barium blocks X-rays, causing the barium-filled colon to show up clearly on the X-ray picture.There are two types of barium enemas.
single-contrast study , the colon is filled with barium, which outlines the intestine and reveals large abnormalities.
In a double-contrast or air-contrast study , the colon is first filled with barium and then the barium is drained out, leaving only a thin layer of barium on the wall of the colon. The colon is then filled with air. This provides a detailed view of the inner surface of the colon, making it easier to see narrowed areas (strictures),diverticula, or inflammation.

Colorectal carcinoma (CRC) is the most common cancer of the gastrointestinal tract and the second most frequently diagnosed malignancy in adults.
Clinical
o Peak age 50-70 years
o Weight loss
o Blood in stool
o Loss of appetite
o Change in bowel habits
Location
o Rectum (15%), sigmoid (20%), descending colon (10%), transverse colon (12%), ascending colon (8%), cecum (8%)
o More common in right colon with advancing years
o More common in left colon with chronic ulcerative colitis
Imaging findings
o 90-95% rate of detection by BEo Polypoid filling defect
o Annular constricting >>>>> apple-core lesion

Diverticular disease
Out-pouchings of bowel result in blind-ended diverticulae in communication with the lumen of the bowel. These most commonly occur within the sigmoid colon, although them may be present throughout the bowel.colonic diverticulosis : the presence of multiple diverticulae within the bowel
colonic diverticulitis : infection of the diverticulae, usually because the neck becomes blocked



Familial Polyposis Syndromes
Autosomal dominant with high penetrance (80%)• About 2/3 of affected people have a positive family hx of colonic polyps or ca and about 1/3 are sporadic cases
• Colonic polyps are numerous and of all different sizes
• They may be sessile or pedunculated
• Rectum and left colon are more commonly affected than right side of colon
• Often, however, the entire colon is carpeted with polyps
accounts for 1 percent of all cases of colorectal cancer



Sub-phrenic abscess : A pus-filled cavity in the subphrenic region which is the area below the diaphragm but above the colon and liver. The infection can occur as a complication of abdominal surgery, acute pancreatitis and trauma.
Dome shape luency below the diaphragm with straight air fluid level .

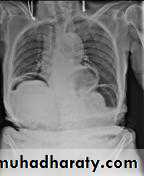
Pneumoperitoneum
Pneumoperitoneum describes gas within the peritoneal cavity, and is often the consequences of many a critical illness.Radiographic features
Plain film
Chest radiograph
An erect chest x-ray is probably the most sensitive plain radiograph for the detection of free intra peritoneal gas >>> crescent shape of lucency unilateral or bilateral
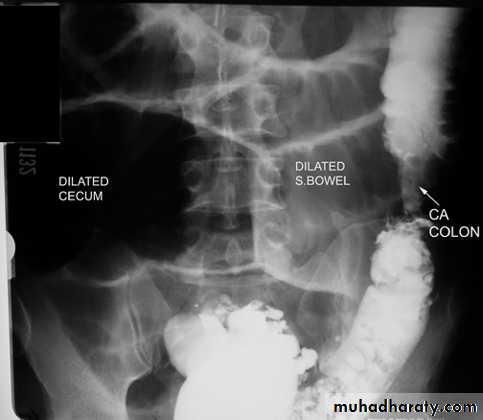
Bowel obstruction
Plain x ray SBOdilated loops with air fluid level in erect position
centrally placed
transverse lines (circular folds ) valvule convent's


Plain x ray LBO
dilated bowel with gasperipheral
haustra (not lines across bowel)
may have cut-off point

Sigmoid volvulus
Inverted U-shaped appearance of distended sigmoid loopLargest and most dilated loops of bowel are seen with volvulus
Loss of haustra
Coffee-bean sign à midline crease corresponding to mesenteric root in a greatly distended sigmoid
Sigmoid volvulus – bowel loop points to RUQ
Cecal volvulus – bowel loop points to LUQ
Bird’s-beak or bird-of-prey sign à seen on barium enema as it encounters the volvulated loop


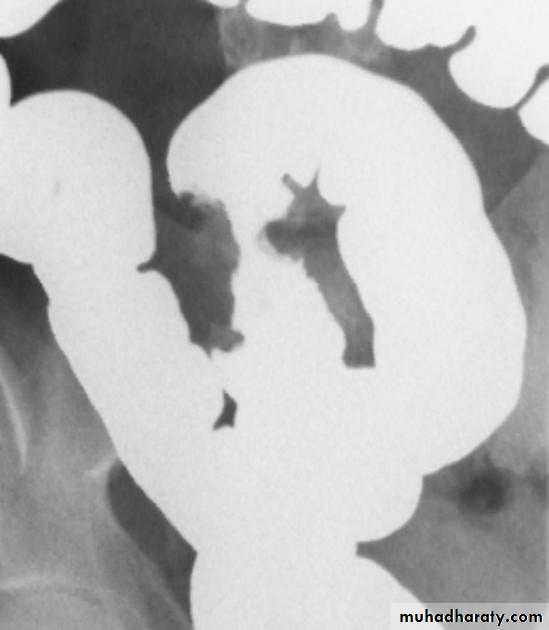
Intussusceptions'
Intussusceptions' occurs when one segment of bowel is pulled into itself (or a neighboring loop of bowel) by peristalsis.It is an important cause of an acute abdomen in children and merits timely ultrasound examination and reduction to preclude significant sequelae including bowel necrosis.
Intussusception may also occur in the adult population where it is usually caused by a focal lesion acting as a lead point.
Abdominal plain film
Abdominal x-rays may demonstrate an elongated soft tissue mass (typically in the right upper quadrant in children) with a bowel obstruction proximal to it.
Ultrasound
Ultrasound signs include
target sign (also known as the doughnut sign)
pseudo kidney sign
crescent in a doughnut sign
Fluoroscopy - contrast enema
A contrast enema remains the gold standard, demonstrating the intussusceptions as an occluding mass prolapsing into the lumen, giving the "coiled spring” appearance .





Ba enema examination
narrowing of recto-sigmoid segment of intestineproximal dilatation of the colon
depicted transition zone on the contrast enema is not accurate at determining the transition between absent and present ganglion cells.
The affected segment is of small calibre with proximal dilatation. Fasciculation / saw-tooth irregularity of the agangliotic segment is frequently seen



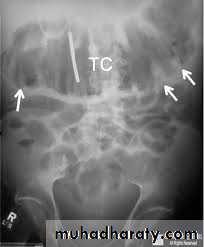
Toxic megacolon
Toxic megacolon (TM) is complication that can be seen in both types of inflammatory bowel disease, in infectious colitis, as well as in some other types of colitisRadiographic features
The colon (typically transverse colon) becomes dilated to at least 6cm (usually greater).There is additional loss of haustral markings, with pseudopolyps often extending into the lumen.
Thumbprinting from mucosal edema may be present.