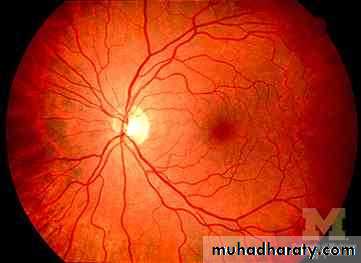
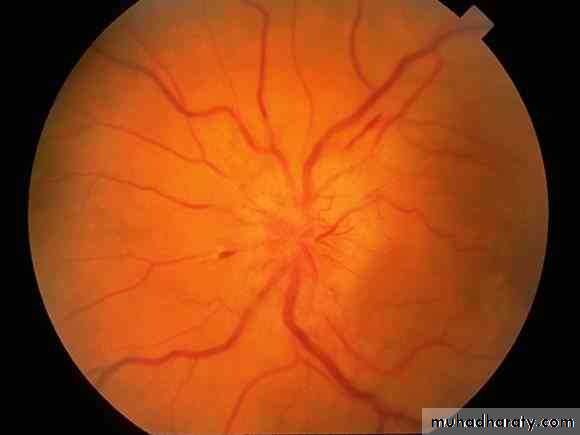
papilloedema with symptomatic raised ICP more than 20cm with normal imaging study of the brain ( absent intracranial mass or infection)
Idiopathic intracranial hypertension (pseudotumor cerebri)
Hot points
more common in obese women of childbearing ageusually self limiting, recurrence is common
a preventable cause of blindness from optic atrophy
perimetry is the best test to detect and follow visual loss
Clinical feature
symptoms and signs of raised ICP i.e. headache with papilloedema and no focal neurological deficit apart from abducent palsy (false localizing sign) leading to diplopiaenlarged blind spot due to papilloedema with conspicuous absence of altered level of consciousness in spite of raised ICP
diagnosis
Clinical features
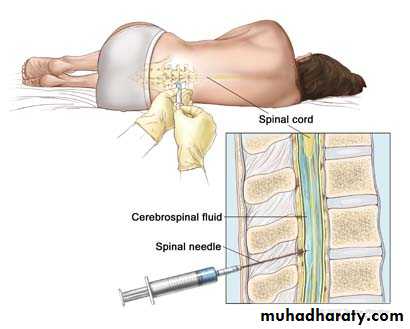
CSF pressure, more than 20cm H2O
CSF normal cytology and biochemistry some time low protein
Normal imaging study of the brain except for slit ventricles
MRV to exclude dural venous sinus thrombosis
Associated conditions
ObesityDrugs tetracyclines, nalidixic acid, ciprofluxacine, danazol, lithium, amiodarone, phenytoin, nitrofurantoin, nitroglycerine and steroids
Steroid withdrawal
Hypervitaminosis A
Hypoparathyroidism and hyperthyroidism
Addison disease and cushing disease
Uremia
Iron deficiency anemia
Menstrual irregularity
Oral contraceptive
Differential diagnosis
Brain mass, may be nonvisible on non enhanced CT scanDural sinus thrombosis
Meningeal carcinomatosis
Pseudopapilloedema: anomalous elevation of optic nerve head associated with hyperopia and drusen, but here there is positive retinal venous pulsation
Malignant hypertention
treatment
Spontaneous resolution is common between 1 month – 1 year
Recurrence rate 10 %
There is no reliable predictor of visual loss, i.e visual loss is unrelated to severity of headache, papilloedema, duration of symptoms.
Repeated ophthalmplogical examination by perimetry
treatment
Treat offending factorWeight loss
Medical treatment
• Diuretics
Carbonic anhydrase inhibitors
acetazolamide start by 250 mg PO q 8-12 hr increasing the dose till symptomatic relief or side effects or 2 gm is reached. Contraindicated in renal calculi and allergy to sulpha
topiramate(topomax) anticonvulsant with carbonic anhydrase inhibition 200 mg PO BID
frusemide( Lasix )start 160 mg up to 320 mg
surgical
serial LP till remission.. 25% remit by 1st LP, aspirate 30cc daily till opening pressure be bellow 20cm then aspirate weekly with follow up
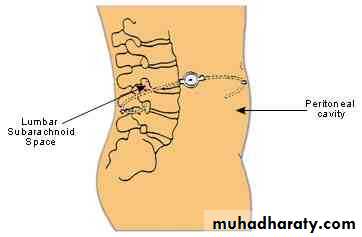
lumboperitoneal shunt
optic nerve sheath fenestration
subtemporal and suboccipital decompression