Fifth stage
Surgery(ortho.)
Lec3p2
د.مثنى
18/10/2016
Bone Infection (Part 2)
Subacute haematogenous Osteomyelitis
-Osteomyelitis may present in mild form.
-Organism may be low virulent.
-The distal femur ,proximal ,distal tibia are the favorite site.
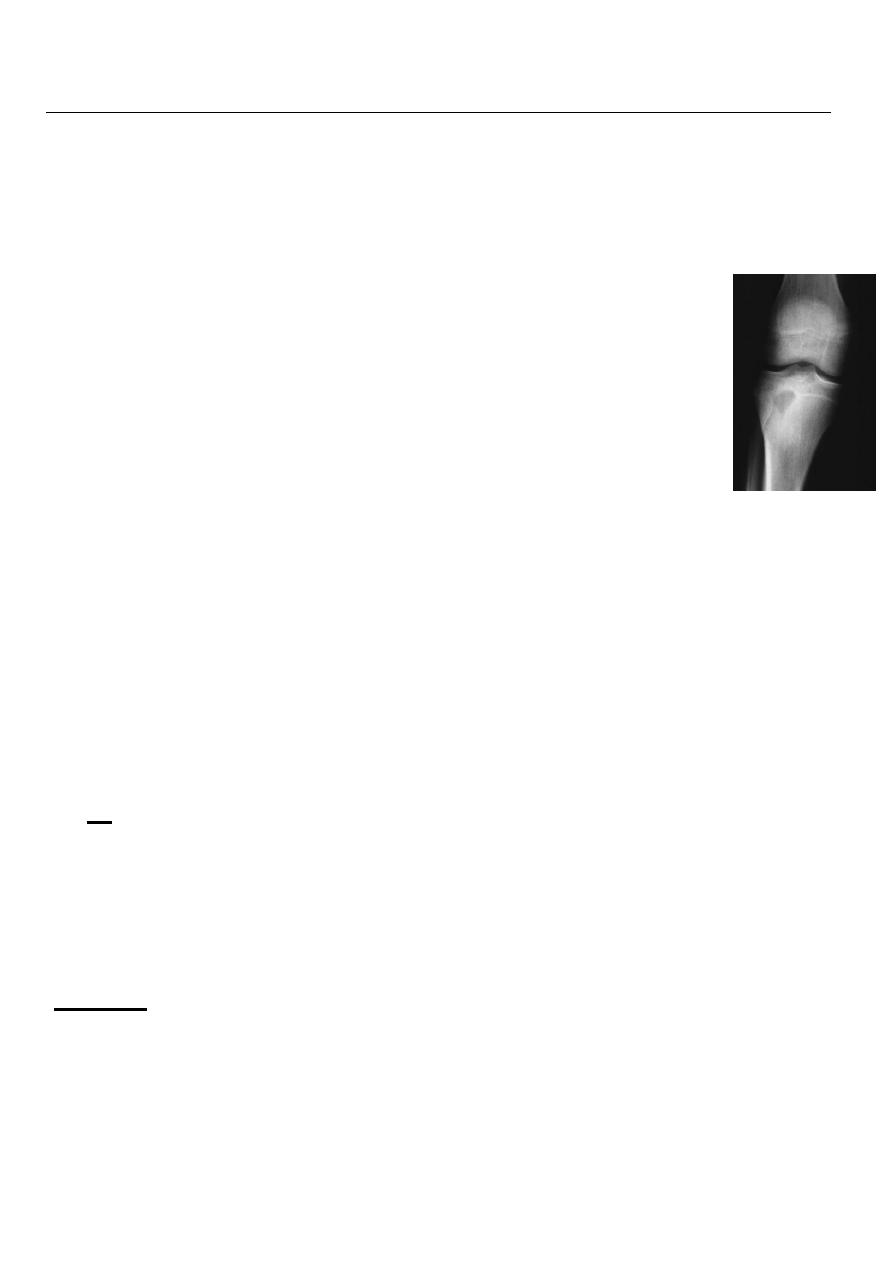
-The patient usually is child with pain near one of the large joint for weeks. -X
ray typical osteolytic lesion of small ,oval cavity surrounded with sclerosis.. -
Rx open with antibiotics
Chronic Osteomylitis
-If any of sequestrum, abscess cavity, sinus tract or cloacae is present. -Hematogenous
infection with an organism of low virulence may be present by chronic onset.
-The imprisoned sequestra provoke a chronic seropurulant discharge which
escapes through a sinus .
-Bacteria may remain dormant for years. -Giving
rise to recurrent flares of acute infection.
M. O.
Stap.aureus.
E coli.
Strep.pyogenes.
Proteus and pseudomonas.
Stap epidermis.
Causes:
1.
post acute infection.
2. post operative infection.
3. Compound fracture.
4. Chronic infection from the start as in T. B.
5.
osteomyelitis of garea.
1
Pathology
1.Bone is destroyed or devitalized.
2.Cavities containing pus and pieces of dead bone (sequestrum)
3.Sinuses .
4.Involucrum.
5.Pathological fracture.
Clinical features
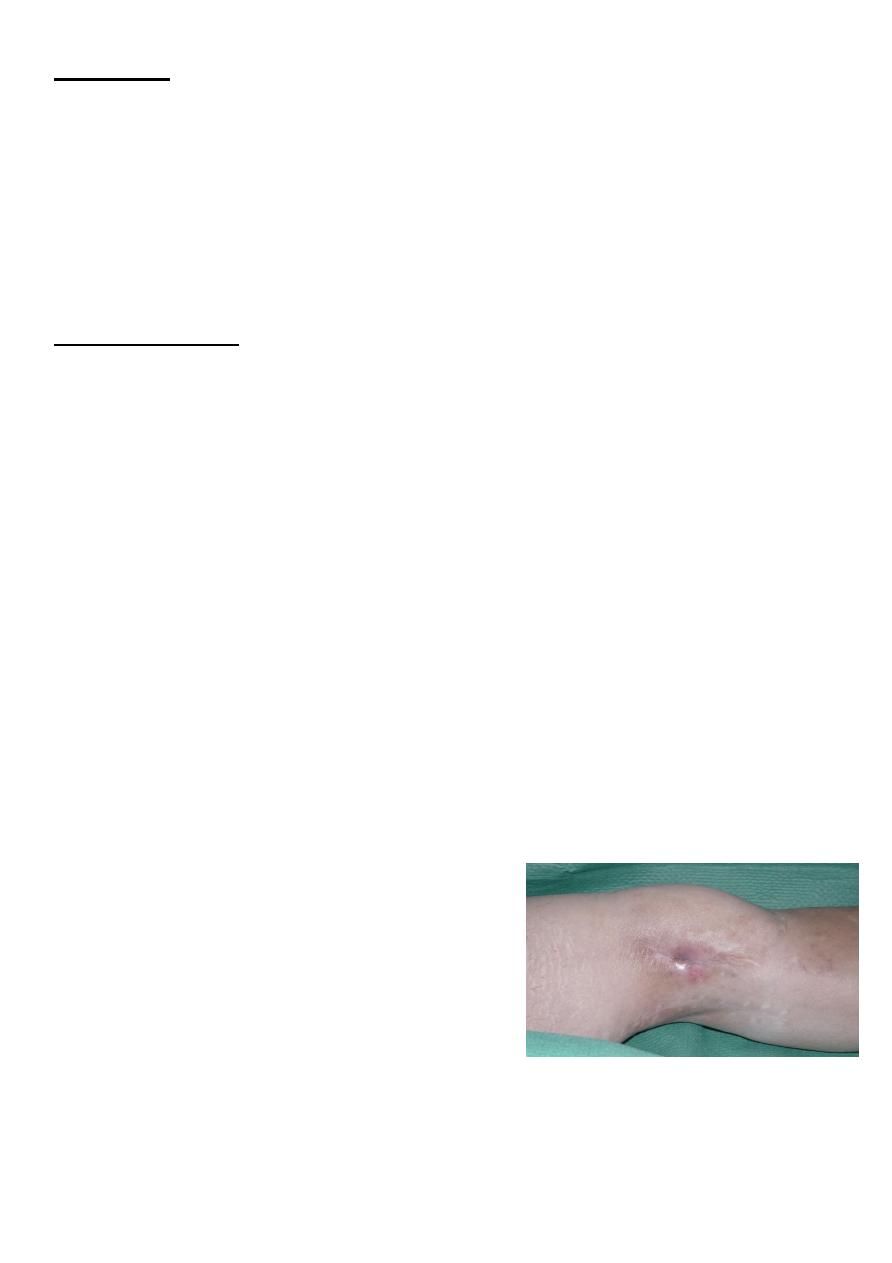
-During the period of inactivity, no symptoms are present.
-Only Skin-thin, dark, scarred, poor nourished, past sinus, an ulceration that is not easily to
heal.
-Muscles-wasting contracture, atrophy
-Joint-stiffness
-Bone-thick, sclerotic.
-often contain abscess cavity
-At intervals, a flare-up occurs.
-The relapse is often the result of poor body condition and lower resistance
-A lighting up of infection is manifested by aching pain that is worse at night.
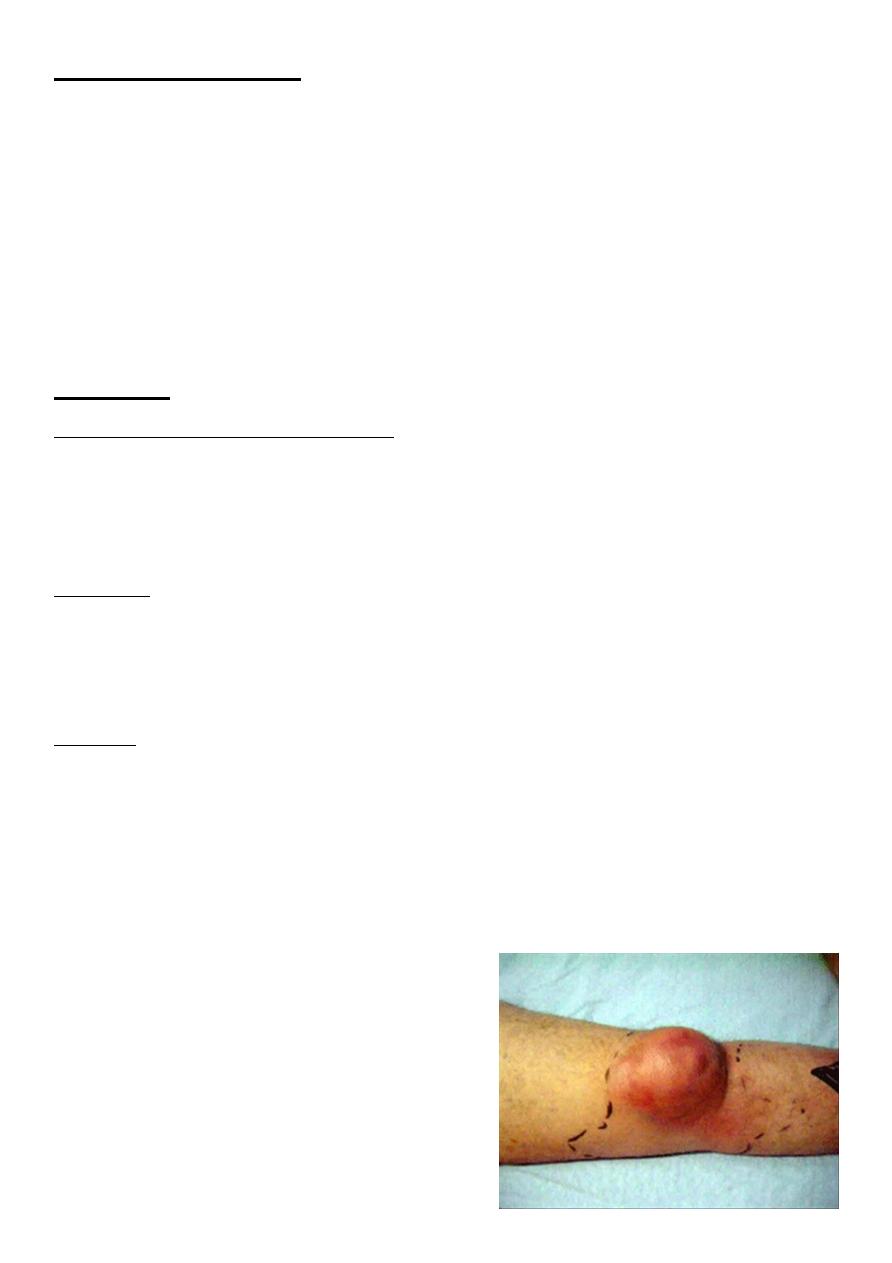
-Examination: Locally there will be :
some heat.
Swelling.
Redness.
Tenderness.
Edema.
-Because pus may build up in cavity, then a sinus may
open and start to exudates purulent materials and
small sequestrum.
-The sinus closed and the infection subsided.
2
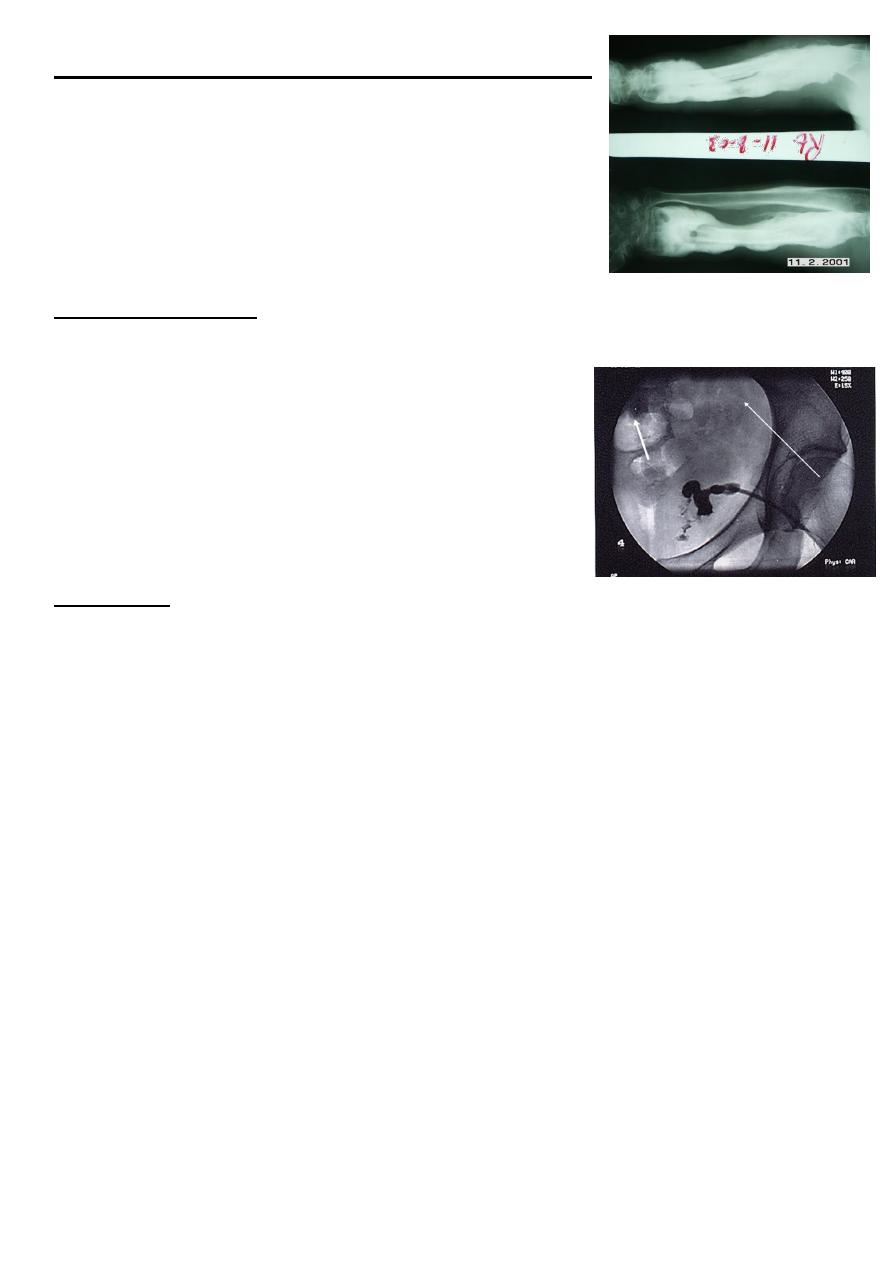
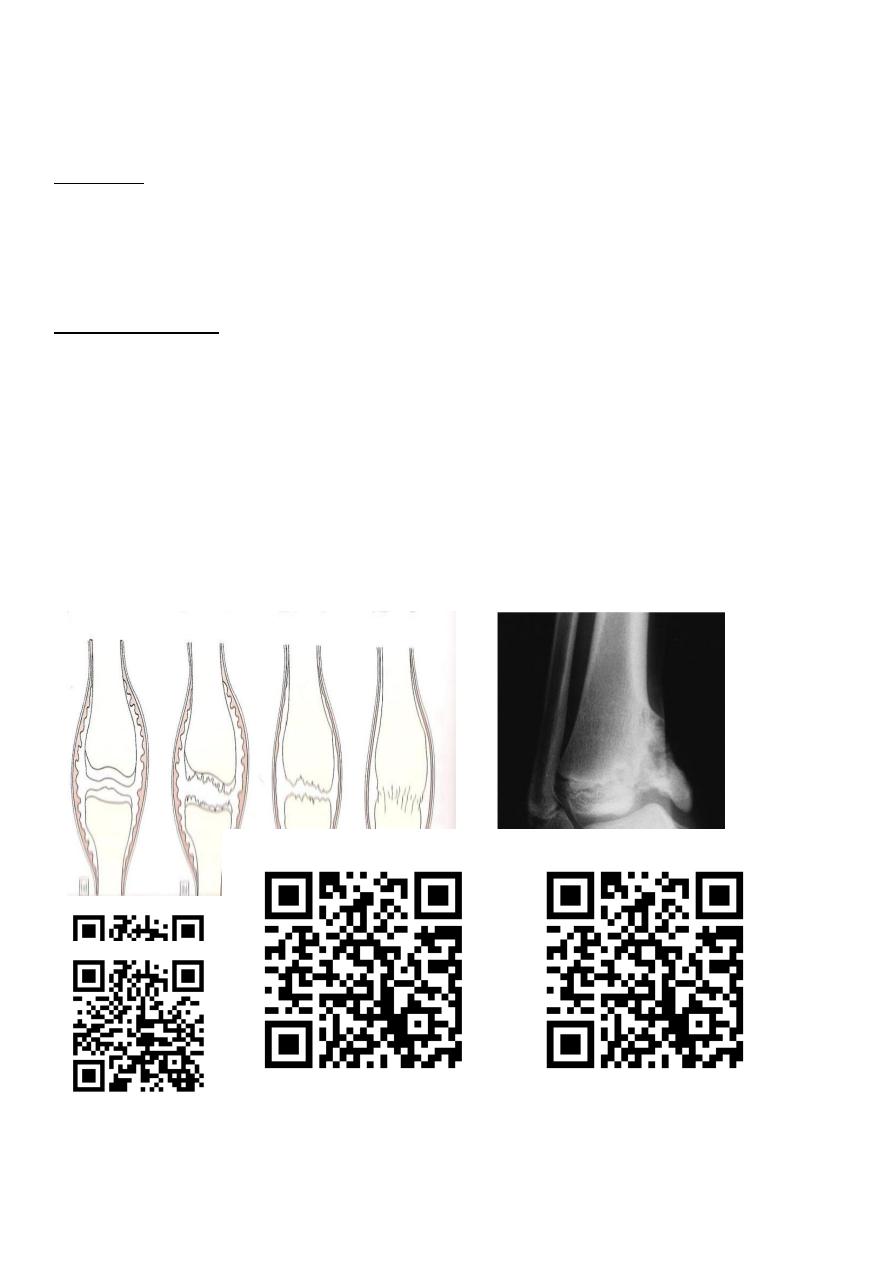
X-ray findings -------------------------------------------
-Bone resorption=cavitation.
-Sclerosis.
-Sequestrum.
-Pathological fracture may be present
.
INVESTIGATIONS
-E S R increased.
-WBC may be increased.
- culture from the sinus.
-A sinogram may help to localize a particular focus of
infection.
-Bone scans are useful in revealing hidden foci and
inflammatory activity.
Treatment
-It is very difficult to provide a permanent cure for chronic Osteomyelitis.
-most antibiotics fail to penetrate the barrier of fibrous tissue plus bone sclerosis.
-Chronic osteomyelitis presents quite different problem from the acute form.
- Its primary problem is surgical removal of all dead and poor vascularized tissues.
-The operation must be carefully planed as it often means significant removal of bone and
surrounding tissues.
-local muscle flap procedures.
3
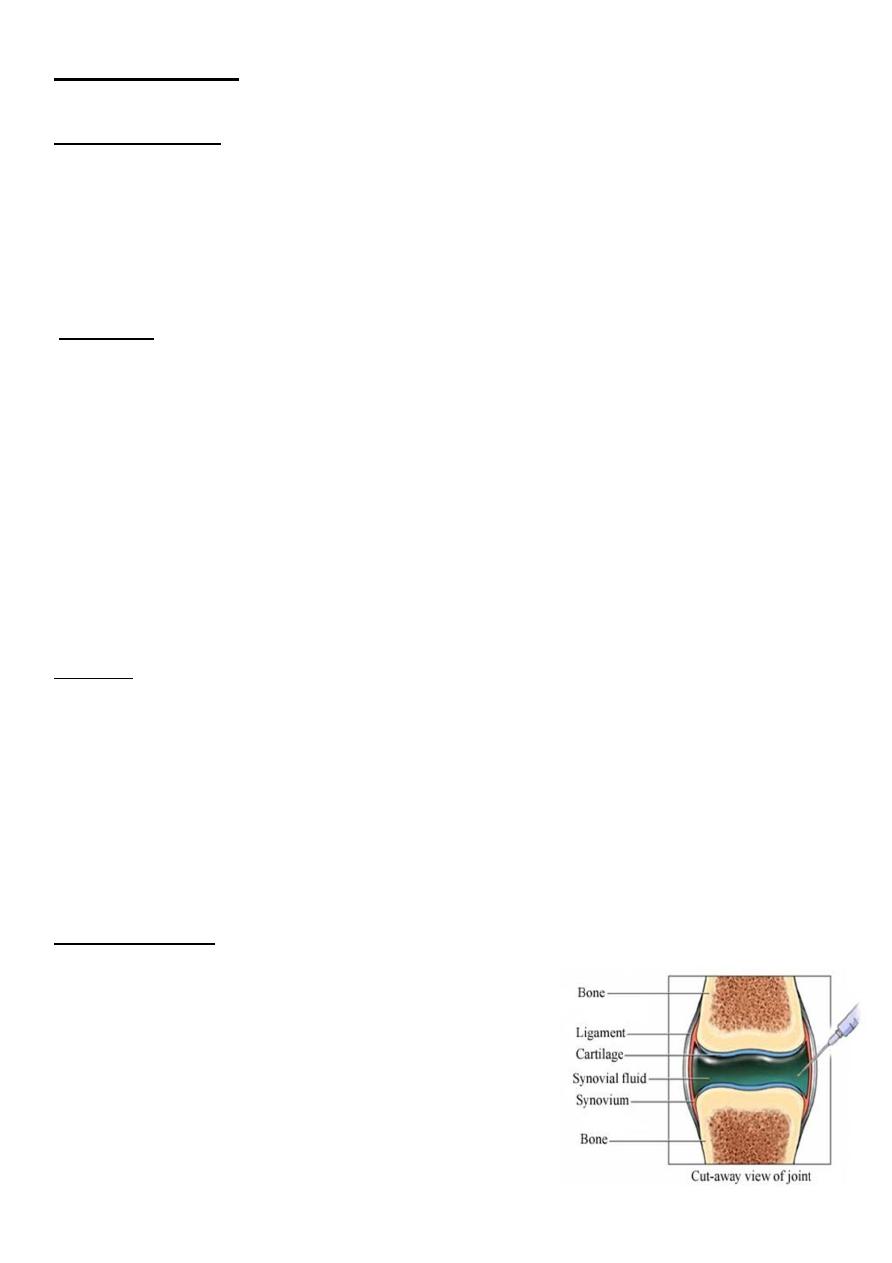
Acute suppurative arhtritis
-The most common - Staphylococcus aureus.
-The hips and knees are the most frequently affected sites.
Route of infection:
Hematogenous spread from an infective focus.
Spread from an adjacent focus (eruption of bone abscess.)
Direct introduction by the wound.
Intra articular injection.
Arthroscopy
.
Causative organism:
-Stap.
-Haemo.
Influ.
- Less commonly :
strep .
E-coli .
proteus
.
Pathology
1.serous arthritis.
Synovium is congested, edematous and infiltrated with WBC. Synovial fluid increased in
the amount with clear or slight opaque appearance and slight amount WBC
2.serofibrinous
arthritis-fibrin is excessive
3.Purulent arthritis:
-Local necrosis occur.
-Joint fluid full -WBC .
-Opaque, thick gray or yellowish in colour.
-The protolytic enzymes dissolve the articular
cartilage, even erode the bone-fibrous ankylosis
4
Clinical features
In newborn infants:
Baby is irritable.
Refuse to eat.
Rapid pulse.
Fever.
There may be an evidence of umbilical cord infection.
In children:
acute pain in single large joint like hip.
reluctance to use the limb.
ill.
rapid pulse.
swinging fever.
skin look red.
joint swelling.
local warmth.
marked tenderness.
all movement is limited
In adults:
-Often that the superficial joint is:
painful.
Swollen.
Inflamed.
Local warmth .
Tenderness.
- Movement is restricted.
Investigations
-X-ray in early cases is normal.
-Ultrasound shows joint effusion.
-In E-coli there may be an evidence of gas in the joint.
-WBC ,E S R is increased.
-Blood culture positive.
-Examination of the joint aspirate. with gram stain.
5
Differential Diagnosis
1. Acute osteomyelitis.
2. Trauma.
3. Irritable joint (the child not ill, no sign of infection).
4. Rheumatic fever.
5. Haemophilic bleed.
6. Gout and pseudogout.
7. Gauchers’ disease.
Treatment
Essential principles in the management:
1. The joint must be adequately drained.
2. Antibiotics must be given to diminish the systemic effects of sepsis.
3. The joint must be rested in a stable position.
Antibiotics.
The initial choice of antibiotics is based on the judgment of the most likely
pathogen's.
Then according the culture and sensitivity.
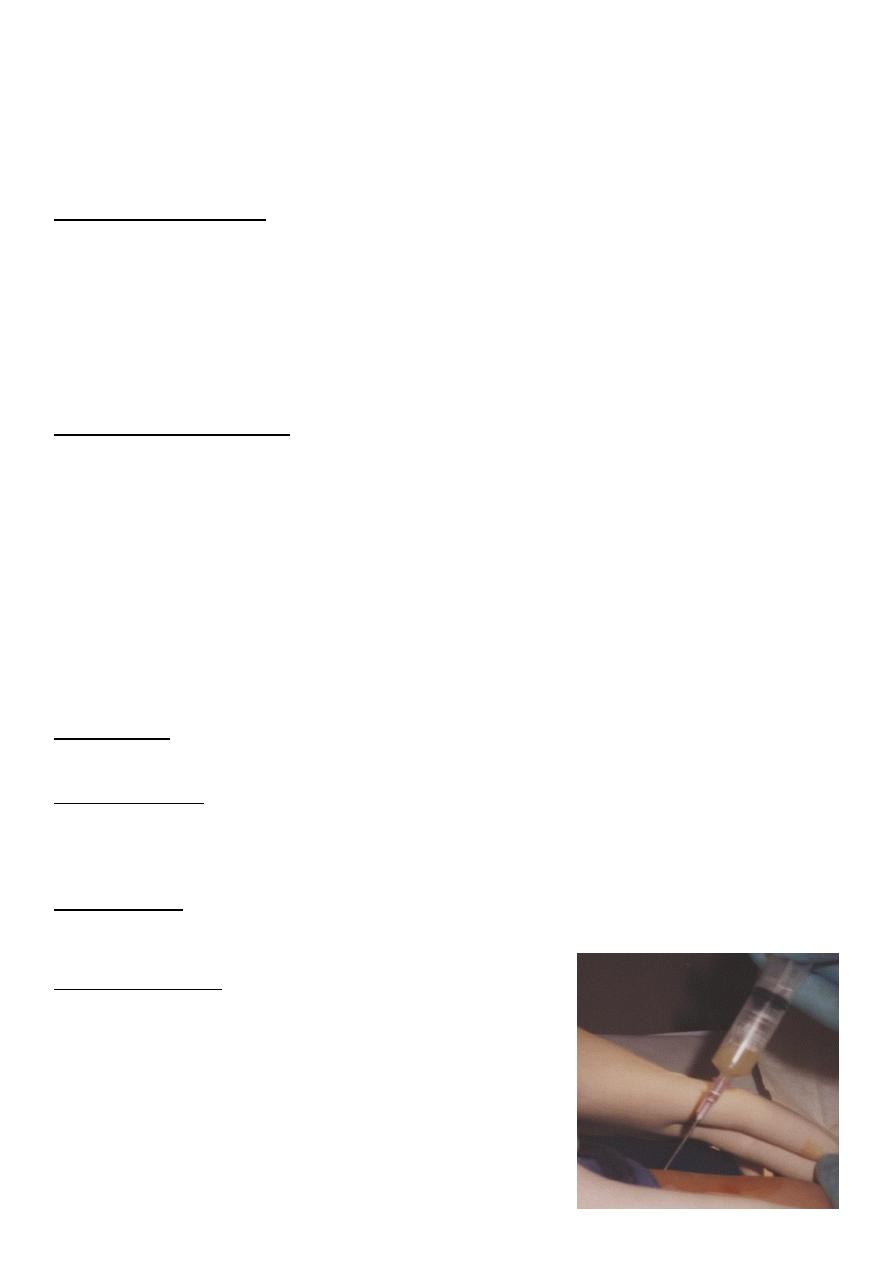
Drainage.
• If the diagnosis is made early and the involved joint is superficial, such as the
elbow or ankle.
• Aspiration should be performed .
• Repeated if necessary.
-The joint should be
splinted
in a position of function.
-Patient should be observed.
For a decrease in.
Pain.
Swelling.
Temperature.
And for improved joint mobility.
6
-Although some infections clear up within days, antibiotic regimens often should
be continued for 4 to 6 weeks, depending on the clinical course.
After care.
• If the articular cartilage is preserved so gently and gradually increasing movement.
• If the cartilage is destroyed. So the aim to keep the joint immobile while ankylosis is
awaited.
Complications
1. Epiphyseal destruction (in neglected infants).
2. Growth disturbance. ( shortening or deformity).
3. Ankylosis (due to cartilage damage).
https://www.muhadharaty.com/lecture/13442
7