Psychotropic drugs
Prof elham aljammasSept 2015
objectives
Identify general pharmacologic strategiesDiscuss antidepressants including indications for use and side effects
Describe mood stabilizers including indications for use and side effects
Review antipsychotics including how to choose an antipsychotic and side effects
Identify anxiolytic classes and indications for use
Management strategies
-Adjust dosage for optimum benefit, safety and compliance.-Use adjunctive and combination therapies if needed however always strive for the simplest regimen.
-Keep your therapeutic endpoint in mind.
Psychotropic drugs
Treat mood, cognition, and behavioral disturbances associated with psychological disordersMost are not used recreationally or abused
Benzodiazepines are the exception
General classes of disorders
Mood
Anxiety
Psychotic
Other Disorders
Attention Deficit Disorder
Depression
Depression is a serious disorder that afflicts approximately 14 million adults in the United States each year. The lifetime prevalence rate of depression in the United States has been estimated to include 16 percent of adults (21 percent of women, 13 percent of men), or more than 32 million peopleAntidepressants
Indications:Unipolar and bipolar depression,
organic mood disorders,
schizoaffective disorder,
anxiety disorders including OCD, panic, social phobia, PTSD,
premenstrual dysphoric disorder
and impulsivity associated with personality disorders.
General guidelines
Antidepressant efficacy is similar so selection is based on past history of a response, side effect profile and coexisting medical conditions.There is a delay typically of 3-6 weeks after a therapeutic dose is achieved before symptoms improve.
If no improvement is seen after a trial of adequate length (at least 2 months) and adequate dose, either switch to another antidepressant or augment with another agent.
Mood disorders/Antidepressants
MAO Inhibitors
TricyclicsSelective Serotonin Reuptake Inhibitors
Dual Action Antidepressants
Selective Norepinephrine Reuptake Inhibitors
Atypical antidepressant
Mood Stabilizers (Antimanic Agents)
LithiumCarbonateValproic Acid
Carbamazepine
Lamotragine
Topirimate
MAOI
Use in late 1950s & ended in early 1960suse ended due to side effect (death)
MAO breaks down many chemicals including tyramine
Tyramine is present in cheeses, red wines, alcohol, smoked fish
MAO in liver breaks down tyramine
Causes a hypertensive crisis "cheese syndrome"
increased blood pressure ➔ stroke ➔ death
increased heart rate ➔ heart attack ➔ death
MAOI
Bind irreversibly to monoamine oxidase thereby preventing inactivation of biogenic amines such as norepinephrine, dopamine and serotonin leading to increased synaptic levels.
Are very effective for depression
Side effects include orthostatic hypotension, weight gain, dry mouth, sedation, sexual dysfunction and sleep disturbance
Hypertensive crisis can develop when MAOI’s are taken with tyramine-rich foods or sympathomimetics.
MAOI
Serotonin Syndrome can develop if take MAOI with meds that increase serotonin or have sympathomimetic actions. Serotonin syndrome sx include abdominal pain, diarrhea, sweats, tachycardia, HTN, myoclonus, irritability, delirium. Can lead to hyperpyrexia, cardiovascular shock and death.To avoid need to wait 2 weeks before switching from an SSRI to an MAOI. The exception of fluoxetine where need to wait 5 weeks because of long half-life.
SSRIs
Tricyclic antidepressants
Act as agonists to catecholaminesNo "cheese syndrome"
Side effects are the major problem
Cardiotoxic
Sedative action
Block acetylcholine system, especially muscarinic receptors
blurred vision, dry mouth, urinary retention, constipation, mental confusion
Block histamine receptors - sedation
prescaution
Very effective but potentially unacceptable side effect profile i.e. antihistaminic, anticholinergic, antiadrenergic
Lethal in overdose (even a one week supply can be lethal!)
Can cause QT lengthening even at a therapeutic serum level
TCA
Have tertiary amine side chains
Side chains are prone to cross react with other types of receptors which leads to more side effects including antihistaminic (sedation and weight gain), anticholinergic (dry mouth, dry eyes, constipation, memory deficits and potentially delirium), antiadrenergic (orthostatic hypotension, sedation, sexual dysfunction)
Act predominantly on serotonin receptors
Examples:Imipramine, amitriptyline, doxepin, clomipramine
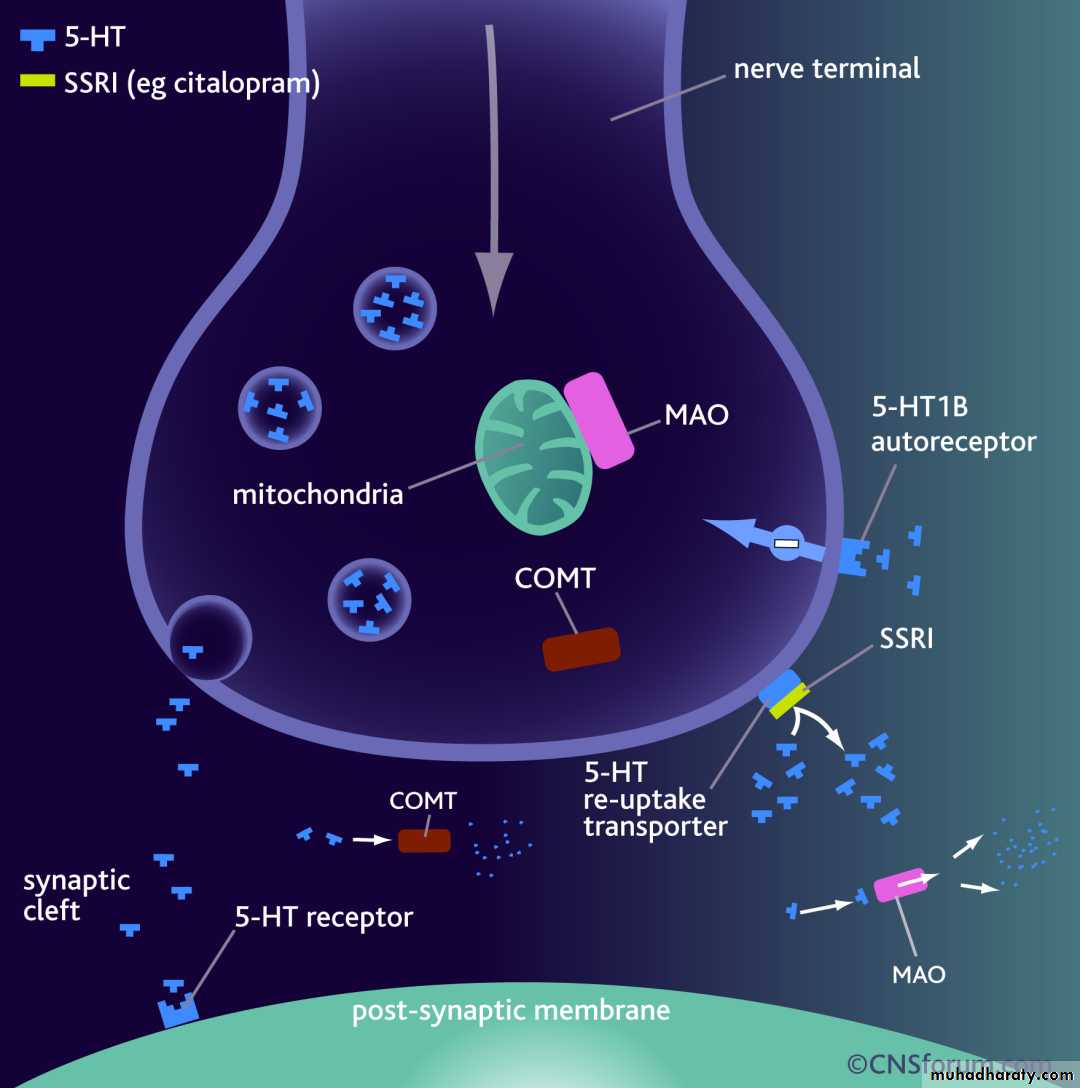
SSRI
Selectively block re-uptake of 5-HTWork on DA and NE as well but very little
Eliminate ACh and antihistamine effects
No more effective than MAOIs or tricyclics
Better because there are fewer side effects
On market since late 1980s & early 1990s
Fluoxetine – Prozac
Sertraline - Zoloft
Paroxetine - Paxil
Fluvoxamine - Luvo
Citalopram - Celexa
Escitalopram - Lexapro
SSRI
Selectively block re-uptake of 5-HT
Work on DA and NE as well but very little
Eliminate ACh and antihistamine effects
No more effective than MAOIs or tricyclics
Better because there are fewer side effects
On market since late 1980s & early 1990s
Fluoxetine – Prozac
Sertraline - Zoloft
Paroxetine - Paxil
Fluvoxamine - Luvo
Citalopram - Celexa
Escitalopram - Lexapro
Selective serotonin reuptake inhibitors
Block the presynaptic serotonin reuptakeTreat both anxiety and depressive
Most common side effects include GI upset, sexual dysfunction (30%+!), anxiety, restlessness, nervousness, insomnia, fatigue or sedation, dizziness
Very little risk of cardiotoxicity in overdose
Can develop a discontinuation syndrome with agitation, nausea, disequilibrium and dysphoria
SNRI
Selectively inhibits NE transporter.
Blocks re-uptake.
Atomoxetine (Strattera)
Reboxetine (Edronax, Vestra)
Dual action AD
Affinity for both 5-HT and NE.
Block re-uptake for both
In this sense, like TCAs
Duloxetine - Cymbalta
Atypical Antidepressants
The atypical antidepressants are a mixed group of agents that have actions at several different sites. This group includes bupropion, mirtazapine
,nefazodone], and
trazodone
atypical antidepressants
Bupropion (Wellbutrin)No effect on either 5-HT or NE
Effective at blocking DA reuptake
May be similar action to cocaine
Lowers seizure threshold
Venlafaxine (Effexor)
5-HT, DA and NE reuptake blocker
Drugs for bipolar
Treat the manic phases of Bipolar Disorder
Lithium
Valproic Acid
Carbamazepine/OxcarbazepineLamotragine
Topirimate
Symbyax – Combo of olanzepine and fluoxetine (Zyprexa & Prozac)
Mood StabilizersIndications: Bipolar, cyclothymia, schizoaffective, impulse control and intermittent explosive disorders.
Classes: Lithium, anticonvulsants, antipsychotics
Which you select depends on what you are treating and again the side effect profile.
lithium
Only medication to reduce suicide rate.Rate of completed suicide in BAD ~15%
Effective in long-term prophylaxis of both mania and depressive episodes in 70+% of BAD I pts
Factors predicting positive response to lithium
Prior long-term response or family member with good response
Classic pure mania
Mania is followed by depression
LITHIUM
Before starting :Get baseline creatinine, TSH and CBC. In women check a pregnancy test- during the first trimester is associated with Ebstein’s anomaly 1/1000 (20X greater risk than the general population)
Monitoring: Steady state achieved after 5 days- check 12 hours after last dose. Once stable check q 3 months and TSH and creatinine q 6 months.
Goal: blood level between 0.6-1.2mmol /lit
Lithium side effects
Most common are GI distress including reduced appetite, nausea/vomiting, diarrheaThyroid abnormalities
Non significant leukocytosis
Polyuria/polydypsia secondary to ADH antagonism. In a small number of patients can cause interstitial renal fibrosis.
Hair loss, acne
Reduces seizure threshold, cognitive slowing, intention tremor
Lithium toxicity
Mild- levels 1.5-2.0 see vomiting, diarrhea, ataxia, dizziness, slurred speech, nystagmus.Moderate-2.0-2.5 nausea, vomiting, anorexia, blurred vision, clonic limb movements, convulsions, delirium, syncope
Severe- >2.5 generalized convulsions, oliguria and renal failure
Study Questions
Choose the ONE best answer.12.1 A 55-year-old teacher began to experience changes in mood. He was losing interest in his work and lacked the desire to play his daily tennis match. He was preoccupied with feelings of guilt, worthlessness, and hopelessness. In addition to the psychiatric symptoms, the patient complained of muscle aches throughout his body. Physical and laboratory tests were unremarkable. After 6 weeks of therapy with fluoxetine, the patient's symptoms resolved. However, the patient complains of sexual dysfunction. Which of the following drugs might be useful in this patient?
A. Fluvoxamine.
B. Sertraline.
C. Citalopram.
D. Mirtazapine.
E. Lithium.
Correct answer = D. Sexual dysfunction commonly occurs with TCAs, SSRIs, and SNRIs. Mirtazapine is largely free from sexual side effects.
A 25-year-old woman has a long history of depressive symptoms accompanied by body aches. Physical and laboratory tests are unremarkable. Which of the following drugs might be useful in this patient?
A. Fluoxetine.
B. Sertraline.
C. Phenelzine.
D. Mirtazapine.
E. Duloxetine.
Correct answer = E. Duloxetine is an SNRI that can be used for depression accompanied by neuropathic pain. MAOs and SSRIs have little activity against neuropathic pain
A 51-year-old woman with symptoms of major depression also has narrow-angle glaucoma. Which of the following antidepressants should be avoided in this patient?
A. Amitriptyline.
B. Sertraline.
C. Bupropion.
D. Mirtazepine.
E. Fluvoxamine.
Correct answer = A. Because of its potent antimuscarinic activity, amitriptyline should not be given to patients with glaucoma because of the risk of acute increases in ocular pressure. The other antidepressants all lack antagonist activity at the muscarinic receptor.
A 36-year-old man presents with symptoms of compulsive behavior. If anything is out of order, he feels that “work will not be accomplished effectively or efficiently.†He realizes that his behavior is interfering with his ability to accomplish his daily tasks but cannot seem to stop himself. Which of the following drugs would be most helpful to this patient?
A. Imipramine.
B. Fluvoxamine.
C. Amitriptyline.
D. Tranylcypromine.
E. Lithium.
Correct answer = B. Selective serotonin reuptake inhibitors are particularly effective in treating obsessive-compulsive disorder; flu vox amine is approved for this condition. The other drugs are ineffective in the treatment of obsessive-compulsive disorder.