
1
Lecture ( 2) pharynx Dr. Sa'ad Y. Sulaiman
Anatomy of the oral cavity
The oral cavity extends from the vermilion border of the lips (i.e. the
junction between the skin which is keratinizing and the mucus membrane
which is non- keratinizing and pink) to the oropharyngeal isthmus, i.e. up to
the anterior pillar of tonsils.
Common disorders of oral cavity
Ulcers of oral cavity
Causes
1. Infections
i.
Viral: e.g. Herpangina (Coxsackie virus) and herpes simplex;
multiple small vesicles which rupture to form small ulcers.
ii.
Bacterial: Vincent’s infection **, TB, syphilis.
iii.
Fungal: Candidiasis. **
2. Immune disorders:
Aphthus ulcer **
Behcet’s syndrome **
3. Trauma
i. Physical: cheek bite, ill-fitting denture.
ii. Chemical: silver nitrate, phenol, aspirin burn.
iii. Thermal: hot food or fluid
4. Neoplasms: squamous cell CA, minor salivary glands’ CA
5. Skin disorders: Erythema multiforme, lichen planus, bullous
pemphigoid, lupus erythematosus.
6. Blood disorders: Leukaemia, agranulocytosis.
7. Drug allergy: Systemic administration of drugs like penicillin,
tetracycline, sulpha …etc., or contact stomatitis due to local reaction to
mouth washes, tooth paste, prosthetic dental materials …etc.
8. Vitamin deficiencies.
9. Miscellaneous: radiation mucositis, cancer chemotherapy, diabetes
mellitus, uraemia.

2
Miscellaneous lesions of the tongue
Median rhomboid tongue:
developmental anomaly seen as red
rhomboid area, devoid of papillae on the dorsum of the tongue.
Geographical tongue
:
Erythematous areas, devoid of papillae
,
surrounded by an irregular keratotic white outline
Hairy tongue:
This is characterized by a hairy black- brown or yellow
aspect of the dorsal surface of the tongue due to chromogenic bacteria.
Smoking seems to be a promoting factor. Treatment is by scraping the lesion
with tongue cleaner, application of half-strength hydrogen peroxide,
improving the general nutritional status by vitamins and removal of
causative factors if known.
Fissured tongue:
It may be congenital or seen in cases of syphilis,
deficiency of vitamin B complex or anemia.
Ankyloglossia (Tongue tie):
congenital anomaly characterized by the
presence of elongated lingual frenulum tethering the entire oral tongue to the
floor of the mouth and alters the mobility of the tongue. Early surgical
treatment is required to avoid delay in speech and trouble with eating.
Fordyce’s spots:
They are aberrant sebaceous glands present under the
buccal or labial mucosa and shine through it as small yellowish-brown
granules.
Tumours of Oral Cavity
I. Benign tumours
(a) Solid tumours: papilloma, fibroma, haemangioma, pyogenic
granuoloma, pregnancy granuloma and minor salivary gland
neoplasm.
(b) Cystic lesion
s:
Mucoele: retention cyst of minor salivary glands.
Ranula: It is a cystic translucent lesion seen in the floor of mouth on
one side of the frenulum and pushing the tongue up. It arises from the
sublingual salivary gland due to obstruction of its duct. Some ranulae
extend into the neck (plunging type).
3
Treatment is complete surgical excision if small, or marsupialisation, if
large.
II.
Premalignant lesions
Leucoplakia: this is diagnosed clinically. White patches on the oral
mucosa are abnormal. Aetiology is unknown. Treatment is by
excision and this is best performed using the KTP laser.
Erythroplakia: is a red patch on the mucosal surface and has a high
malignant potential. It should always be widely removed and a split-
thickness graft applied.
Melanosis and mucosal hyperpigmentation: Benign pigmented
lesions of oral mucosa may transform into malignant melanomas.
III.
Malignant lesions
Carcinoma of oral cavity
Non-squamous malignant lesions
Minor salivary gland tumours
Melanomas
Lymphomas
Stomatitis
Is a general term used to describe an inflammation of the whole lining of
the mouth. The following are the most common types:
Aphthus ulcer (recurrent aphthus ulcer RAU,
recurrent aphthus stomatitis RAS, recurrent
oral ulcer ROU):
Definition: Benign, recurrent ulceration of the oral mucosa, which appear
as painful white or yellow ulcer surrounded by bright red area.
Incidence: common form of mouth ulcer, affecting women more than men.
They may occur at any age, but usually first appear between the age of 10
and 40.
Aetiology: The cause is unknown and currently there no preventive
measure. The following factors may be suggested:
4
1. Autoimmune process (attack of mucous membrane by the own body’s
immune system).
2. Hereditary. The patient often has positive family history.
3. Nutritional deficiency (vitamin B 12, folic acid and iron).
4. Physical or emotional stress.
5. Viral or bacterial infection.
6. Food allergies.
7. Hormonal changes related to menstrual cycles.
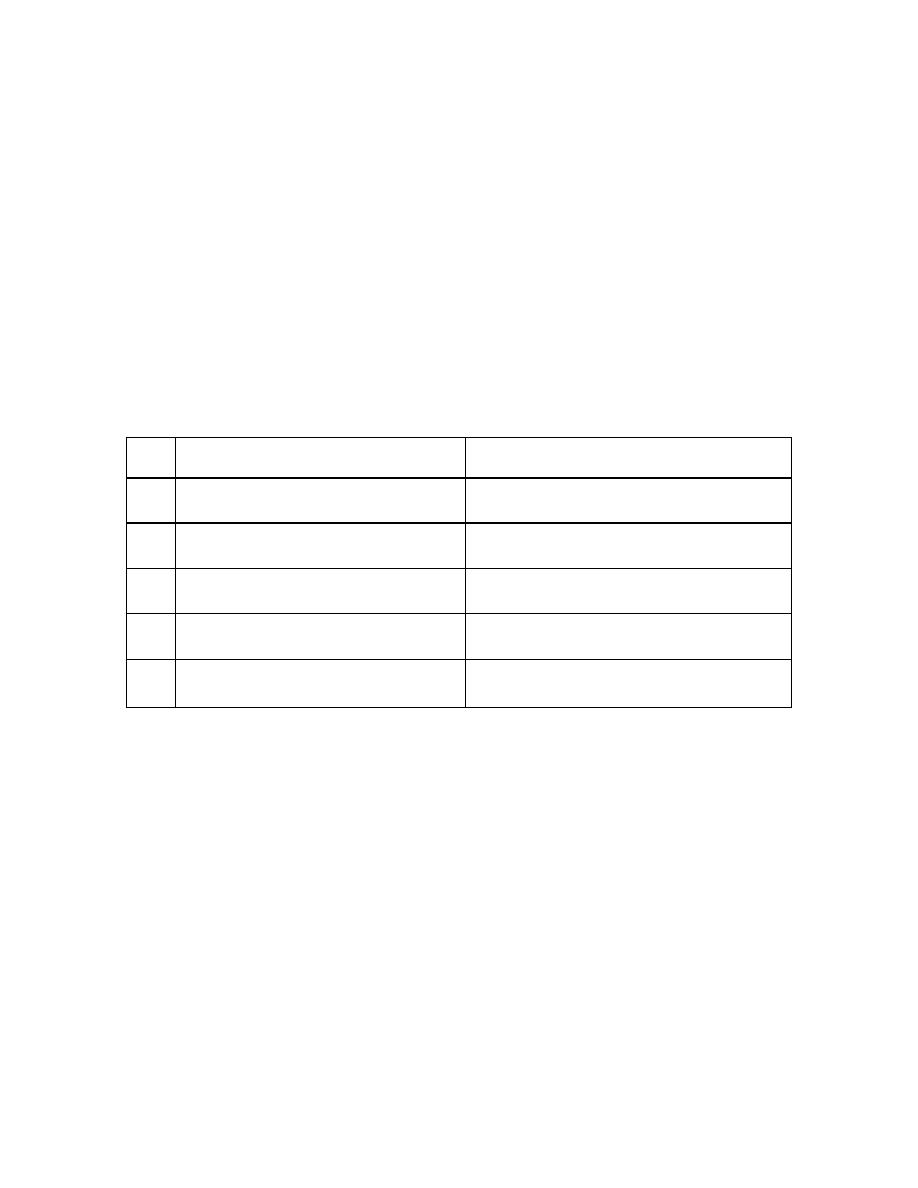
Classification: They are of two types
1. Minor aphthus ulceration.
2. Major aphthus ulceration.
Minor Aphthus ulcerations
Major Aphthus Ulceration
1
More common
Less common
2
2-10mm in size
2-4 cm in size
3
Multiple
Usually single
4
Painful
painful
5
They heal in about 7-10 days
without leaving a scar
They heal in about 3-6 weeks with a
scar
Treatment:
Minor ulcer: treatment is symptomatic as most ulcer s heal spontaneously.
1.
Patients should avoid oral trauma
, for
example, from hard foods and
acidic foods or drinks that may exacerbate pain or perhaps precipitate
ulcers.
2.
Topical analgesics (such as lidocaine).
3.
Topical steroids may be effective in aborting progression of ulcer e.g.
1% triamcinolone dental paste (Kenalog in Orabase) that will cover the
ulcer , enhance healing and not affected by saliva.
4.
Antimicrobial mouth washes to prevent secondary infection and improve
oral hygiene e.g. (mouthwashes containing chlorhexidine gluconate).

5
Major aphthus:
Treatment is more aggressive. Steroid and antibiotic mouthwashes are
useful and a short course of systemic steroid may be effective e.g.
one-week
course of 30 to 60 mg of oral prednisolone.
Any persistent ulcer should be biopsied to exclude malignancy.
Vincent’s
infection
(
acute
necrotizing
ulcerative gingivitis)
This is a highly infectious ulcerative lesions affecting the gingivae and
tonsils, caused by two gram negative organisms (fusiform bacillus and a
spirochaete ). It was common during the First World War due to lack of
hygiene in cleaning of eating and drinking utensils.
Diagnosis: swab from the affected area will show the causative organisms.
Treatment:
1. Systemic antibiotic: Penicillin or Erythromycin and metronidazole.
2. Frequent mouth washes (with sodium bicarbonate mouth solution).
3. Attention to dental hygiene.
Fungal ulcers ( moniliasis or thrush)
Occur in cases of prolonged antibiotic therapy, in poorly nourished children
and in patients suffering from debilitating illness. Presented as creamy-white
plaque on the tongue, buccal and pharyngeal mucosa which are easily
removed with slight bleeding.
Treatment: topical application of nystatin or clotrimazole or 1% of aqueous
solution of gentian violet after each feed.
Behcet’s Syndrome (occulo-oro-genital
syndrome)
It is characterized by triad of (1) aphthus-like ulcers in the oral cavity (2)
genital ulceration and (3) uveitis. There may also be vasculitis of the skin,
synovitis and meningoencephalitis. It is a relapsing condition of unknown
aetiology.

6
Symptoms of Pharyngeal Disease
1) Sore throat:
This is described by the patient as discomfort or raw sensation in the
throat. It is commonly due to inflammatory causes as pharyngitis and
tonsillitis, but may be due to tumor. Pain of tonsillitis is made worse by
swallowing and is typically referred to the ear. Persistent pain specially
when associated with trismus suggests either quinsy or cancer.
2) Dysphagia:
It is difficulty in swallowing and it must be differentiated from
odynophagia which is painful swallowing. True dysphagia is a real difficulty
in swallowing resulting in food coming back to mouth. It means the presence
of cancer of hypopharynx or esophagus until proved otherwise. It usually
starts as dysphagia to solid food then progress to fluid and even to the
patient's own saliva. Dysphagia due to neurological causes is more severe to
fluid than to solid food, e.g. in CVA
3) Difficulty in speech:
Muffled speech can occur due to pharyngeal tumors of big size. Paralysis
of the soft palate can lead to abnormal speech called rhinolalia aperta
(hypernasality). This is in contrary to rhinolalia clausa (hyponasality) when
there is nasal obstruction by anything like common cold or nasal polyp or
tumor.
4) Difficulty in breathing:
Some pharyngeal diseases are likely to impede the airway leading to
stridor e.g. retropharyngeal abscess and Ludwig's angina.
5) Cervical lymphadenopathy: may be infective or malignant.
Infections of The Pharynx
(PHARYNGITIS)
In the pharynx the most common site involved in an infection is the
oropharynx. Nasopharyngitis occurs in early stages of coryza, but is of
no significance, and infections of hypopharynx are unknown. In the
7
oropharynx the area involved are: The lateral wall (tonsillitis), the
posterior wall (Pharyngitis), the floor (Lingual tonsillitis). The roof
(The soft palate) is rarely infected.
Acute pharyngitis
This is the more frequent variety,
occurring primarily during the winter
months and less often in autumn and spring. It precedes the common
cold,
and
may
accompany
influenza,
measles,
infectious
mononucleosis, scarlet fever, typhoid fever or small pox.
Symptoms:
Sore throat which ushers in the coryza is accompanied by a feeling of
coldness, a slight pyrexia, headache, backache and joint pain. The
throat feels dry, raw, uncomfortable or painful especially on
swallowing. There may also be some hoarseness. These symptoms last
for a day or two.
Signs: on examining the throat there is an obvious redness, and
sometimes swelling, of the mucosa of the soft palate, tonsils and
posterior pharyngeal wall. The cervical lymph nodes are palpable and
tender. In children the mouth should be examined for Koplik’s spots in
case the pharyngitis is the precursors of measles.
Treatment: Simple acute pharyngitis is usually a self-limiting disease,
lasting for 3-4 days; so treatment is only symptomatic: bed rest,
analgesic (paracetamol) and warm fluids by mouth. If the attack is
prolonged or the constitutional symptoms are severe antibiotics are
prescribed: Penicillin or erythromycin.
Membranous Pharyngitis
Causes:
1. Viral: Infectious mononucleosis.
2. Bacterial: Diphtheria and scarlet fever.
8
3. Fungal: Candidiasis.
mentioned previously
4. Spirochaetes: Vencent’s angina.
5. Blood dyscrasia: agranulocytosis, and leukaemia.
Diphtheria
Is a specific infection of Corynebacterium diphtheria which is
disseminated by droplets and coughing. Children mostly affected with a
mortality of 10%.
Clinical picture
The disease has incubation period of 4 days. The patient is severely ill,
although the temperature seldom rises over 38C.
On examination The disease is characterized by:
The appearance of false membrane on the tonsils, soft palate and
posterior pharyngeal wall. The disease may spread to affect the nasal
cavity and nasopharynx. The membrane is usually grey in colour,
firmly attached to the mucosa and leaves bleeding surface when it is
removed.
Tender and enlarged cervical lymph nodes.
NOTE: Pharyngeal membranes are of two types:
1. TRUE MEMBRANE: Inflammatory reaction mucoid or purulent
exudate cover the pharyngeal mucosa and form a True Membrane. The
underlying mucosa is intact So removal does not leave bleeding surface
2. FALSE MEMBRANE: Certain Inflammatory reaction Necrosis of
surface epithelium The subepithelial tissue produce fibrinogen
change to fibrin form the false membrane (with the necrotic epithelium)
The membrane covers the submucosa because the epithelium is destroyed
removal leaves bleeding surface
9
Investigation
Swab for bacteriological examination including part of the
membrane.
Complication
o Laryngeal obstruction and stridor Tracheostomy.
o Myocarditis and neuritis.
Treatment
1. Antitoxin: Intravenous 20,000-100,000 units depending on the
severity of the infection.
2. Systemic I.V. Penicillin.
Agranulocytosis
A rare condition in which polymorph nuclear leukocytes are reduced in
number or disappear from the circulation.
Aetiology
Idiopathic
Hypersensitivity reactions to certain drugs like chloramphinicol and
sulphonamides.
Cytotoxic agents bone marrow depression.
Clinical picture
o Fever, headache with sore throat and halitosis.
o Diffuse grayish membrane with superficial ulceration.
o The cervical lymph nodes are not usually involved.
Investigation: CBC and blood film.
Treatment
Treat the cause and any causative drug is immediately withdrawn.

10
Steroid and systemic antibiotic.
Fresh blood transfusion is necessary.
Chronic pharyngitis
1. Specific: T.B. and syphilis
2. Nonspecific
Nonspecific
chronic pharyngitis
Chronic irreversible inflammation of the mucus membrane of the
pharynx with hyperplasia of its various elements. Not infrequently the
normal lymphoid tissue on the posterior pharyngeal wall undergoes
hypertrophy so called granular pharyngitis. A frequent finding is thick
vertical bands of lymphoid tissue on the posterolateral wall of the
pharynx behind the posterior pillar of the fauces- the so-called lateral
pharyngeal band.
Aetiology
Exact aetiology is unknown:
1. Recurrent attacks of acute pharyngitis (sore throat).
2. Chronic sinusitis with post-nasal drip
3. Irritants such as tobacco, alcohol and industrial fumes
4. Gastro-Esophageal reflux disease (GERD)
5. Mouth breathing.
Clinical Picture
1. Discomfort and pain in the throat without fever. There is none of the
malaise of tonsillitis and the condition persists for weeks or months.
2. Foreign body sensation in the throat and tendency to clear the throat,
which results from postnasal drip bathing the posterior pharyngeal
wall.
3. Tiring of voice( not hoarseness)
4. Fear of cancer may be dominant in patient's mind.
Examination
- Catarrhal (simple type): mild hyperaemia of the pharyngeal mucosa.
- Hypertrophic type: scattered nodules on the posterior pharyngeal
wall giving a granular appearance.
Treatment
Cessation of smoking is the most important step.

11
Appropriate treatment of postnasal drip –if present- (by
intranasal steroid), and acid reflux (by proton pump inhibitor like
omeprazole and lansoprazole).
Reassurance by the exclusion of malignancy.
Soothing gargles such as crushed soluble aspirin may relieve the
condition transiently.
…………………………………………………………………………...