Urticaria & Angioedema
LEC : 7Urticaria
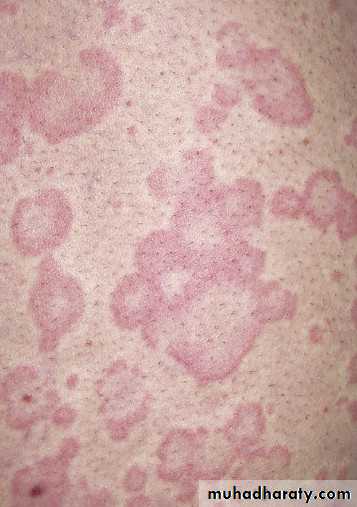
Urticaria, also referred to as hives or wheals, is a common and distinctive reaction pattern.Hives may occur at any age
20% of the population will have at least one episode.
Urticaria is classified as acute or chronic.
Angioedema frequently occurs with acute urticaria, which is more common in children and young adults.
Chronic urticaria is more common in middle-aged women and commonly accompanies angioedema.
The cause of acute urticaria is known in many cases.
The cause of chronic urticaria is determined in less than 5% to 20% of cases.
The evolution of urticaria is a dynamic process, new lesions evolve as old ones resolve.
Hives result from localized capillary vasodilation, followed by transudation of protein-rich fluid into the surrounding tissue; they resolve when the fluid is slowly reabsorbed.The edema in urticaria is found in the superficial dermis.
Lesions of angioedema are less well demarcated and the edema is found in the deep dermis subcutaneous/ submucosal locations.
Wheal






Clinical Classification of Urticaria/ Angioedema
1. Ordinary urticaria (recurrent or episodic urticaria not in the categories below)2. Physical urticaria (defined by the triggering stimulus):
Adrenergic urticaria
Aquagenic urticaria
Cholinergic urticaria
Cold urticaria
Delayed pressure urticaria
Dermographism
Exercise-induced anaphylaxis
Localized heat urticariaSolar urticaria
Vibratory angioedema
3. Contact urticaria (induced by biologic or chemical skin contact)
4. Urticarial vasculitis (defined by vasculitis as shown by skin biopsy specimen)
• 5. Angioedema (without wheals)
PATHOPHYSIOLOGY
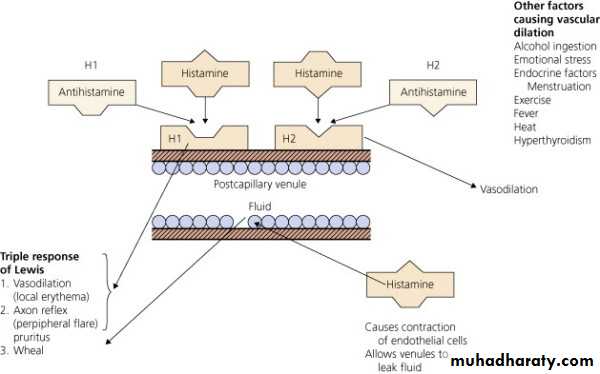
Histamine is the most important mediator of urticaria.
Histamine is produced and stored in mast cells.
A variety of immunologic, nonimmunologic, physical, and chemical stimuli cause histamine release.
Histamine causes localized capillary vasodilatation, which allows vascular fluid to leak between the cells through the vessel wall, contributing to tissue edema and wheal formation.
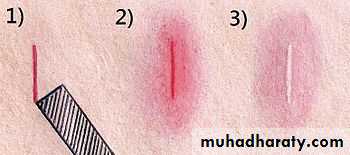
The “triple response” of Lewis???
Blood vessels contain two (and possibly more) receptors for histamine. The two most studied are H1 and H2.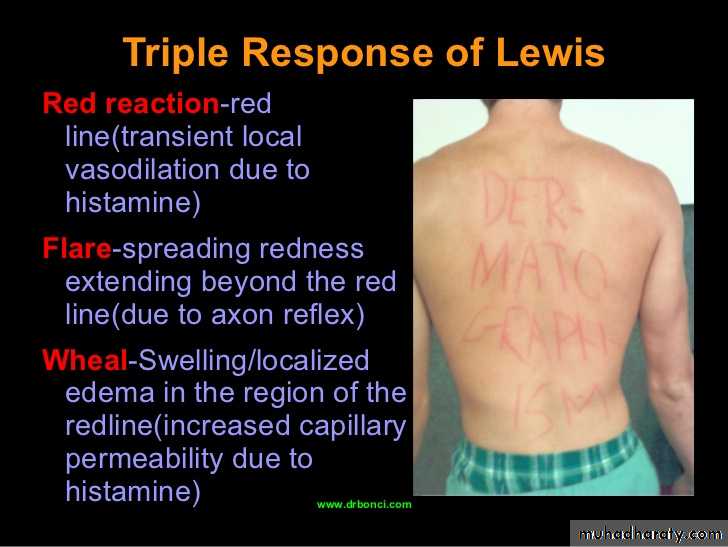
ACUTE URTICARIA
If the urticaria has been present for less than 6 weeks, it is considered acute.ETIOLOGY
1. IgE-MEDIATED REACTIONS
Circulating antigens such as foods, drugs, insect stings, natural rubber latex or inhalants interact with cell membrane–bound IgE to release histamine.
. 2. COMPLEMENT-MEDIATED, OR IMMUNE-COMPLEX-MEDIATED, ACUTE URTICARIA
Administration of whole blood, plasma, immunoglobulins, and drugs or by insect stings.
3. NONIMMUNOLOGIC RELEASE OF HISTAMINE
Acetylcholine, opiates, polymyxin B, and strawberries, aspirin/NSAIDs.CHRONIC URTICARIA
Patients who have a history of hives lasting for 6 weeks or more are classified as having chronic urticaria (CU).The etiology is often unclear.
The morphology is similar to that of acute urticaria but lesions are slightly deeper.
CU is more common in middle-aged women and is infrequent in children.
Individual lesions remain for less than 24 hours but the disease continues for weeks, months, or years
Angioedema occurs in 50% of cases and rarely affects the larynx.
About 70% of patients with CU have physical urticaria.
Aspirin/NSAIDs, penicillin, ACEIs, opiates, alcohol, fever, and stress exacerbate CU.
CU also results from the cutaneous mast cell release of histamine.
Over 30% of CU patients haveautoimmune phenomena:
a sthyroid autoimmunity.
.
There is a significant association between chronic urticaria and autoimmune thyroid disease.
Most patients are women.
Most patients are asymptomatic and have thyroid function that is normal or only slightly abnormal
Evaluation and management of acute & chronic urticaria
History and physical examinationGeneral : CBP , ESR, GSE, GUE, urine and blood sugar, liver and renal function tests
Skin test: commonly used in patient with chronic urticaria
We must exclude certain disease commonly associated with chronic urticaria As chronic infection especially sinus infection, UTI, connective tissue diseases, intestinal warms, internal malignancy, lymphoma, chronic exposure to external allergen
Rx
Avoid provoking factor
medications that exacerbate the hives (usually NSAIDs, aspirin, or beta blockers). These should be stopped until the urticaria resolves.
in acute sever urticaria we can start Treatment by IM antihistamine , I.V. steroid {hydrocortisone} and S.C. adrenaline
Topical Treatment usually CALAMIN lotion
H-1 antihistamine
Sedating (diphenhydramine ,hydroxyzine)
Mildly sedating (cetirizine)
Non-sedating (loratadine,desloratdin)
H-2 antihistamine (ranitidine, famotidine)
Leukotriene antagonist
resistant chronic urticaria – Cyclosporin,Methotrexate
PHYSICAL URTICARIAS
Physical urticarias are induced by physical and external stimuli.
They typically affect young adults.
More than one type of physical urticaria can occur in an individual.
Provocative testing confirms the diagnosis.
Most physical urticaria forms persist for about 3 to 5 years or longer.
Duration of individual lesions?
Dermographism
Most frequentStroking the skin, toweling, clothing.
Starts in minutes, lasting 2-3 hours.
Clinically: irregular pruritic wheals.
No systemic symptoms
Testing (Darier’s sign)
Rx


Delayed pressure urticaria
FrequentProlonged pressure (belt, bra, manual work, standing, sitting on a hard surface).
Starts within 3-12 hrs. lasting 4-36 hrs.
Clinically: diffuse tender swelling.
Flu-like symptoms
Rx (oral steroids)


Cholinergic urticaria
Very frequentGeneral overheating of body
Starts in 2-20 minutes, lasting ½ - 2 hour.
Clinically: tiny papular pruritic wheals.
Anaphylaxis and angioedema may occur.
Testing: exercising.
Rx


ANGIOEDEMA
AE (angioneurotic edema) is a hive-like swelling caused by increased vascular permeability in the subcutaneous tissue of the skin and mucosa and the submucosal layers of the respiratory and GI tracts.Hives and angioedema commonly occur simultaneously.
TYPES OF AngioedemaHAE (hereditary angioedema):
1. Type I: deficiency of C1 INH protein
2. Type II: dysfunctional C1 INH protein
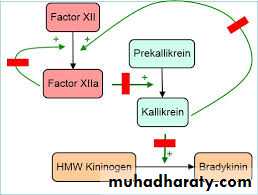
3. Type III: coagulation factor XII gene mutation
AAE (acquired angioedema):
1. Type I: associated with lymphoproliferative diseases
2. Type II: autoimmune (anti–C1 INH antibody) : Thyroid autoimmune disease–associated AE


Hereditary angioedema
Type 1 is the most common and results from a lack of functional C1 esterase inhibitor causing plasma kallikrein activation, which leads to the production of the vasoactive peptide bradykinin.Transmitted as an autosomal dominant trait.
The disease affects between 1 in 10,000 and 1 in 50,000 persons.
The disease begins in late childhood or early adolescence.
Many have ancestors and family members who died suddenly from asphyxia.
Mortality rate can reach up to 30%.Patients live in constant dread of life-threatening laryngeal obstruction which occurs in about 65% of cases.
Minor trauma, mental stress, and other unknown triggering factors lead to the release of vasoactive peptides that produce episodic swelling.
Histamine has no role in this type.



Clinical Presentation?
InvestigationsC1 INH (quantity and function) low
C4 low
C1q normal
24 hr urine histamine normal
tryptase normal.
Treatment:
Acute attacks (C1 INH conc., danazol, tranexamic acid, FFP)Prophylaxis (danazol, tranexamic acid)