Chest Radiology
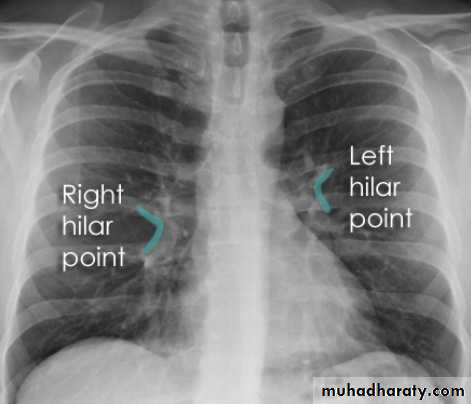
Hilar structuresThe hila (lung roots) are complicated structures mainly consisting of the major bronchi and the pulmonary veins and arteries. These structures pass through the narrow hila on each side and then branch as they widen out into the lungs. The hila are not symmetrical but contain the same basic structures on each side.
Key points
Each hilum contains major bronchi and pulmonary vessels
There are also lymph nodes on each side(not visible unless abnormal)
The left hilum is often higher than the right
Both hila should be of similar size and density. If either hilum is bigger and more dense, this is a good indication that there is an abnormality.
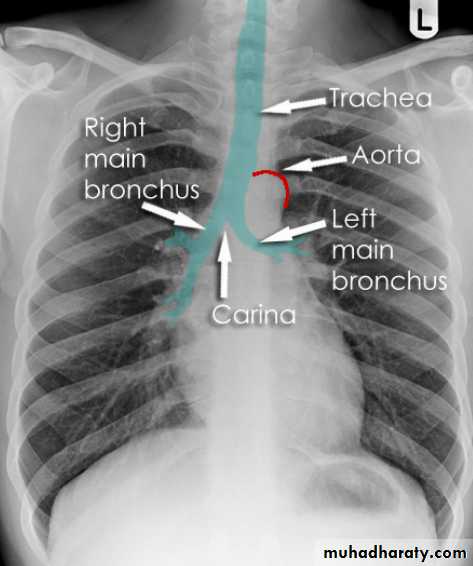
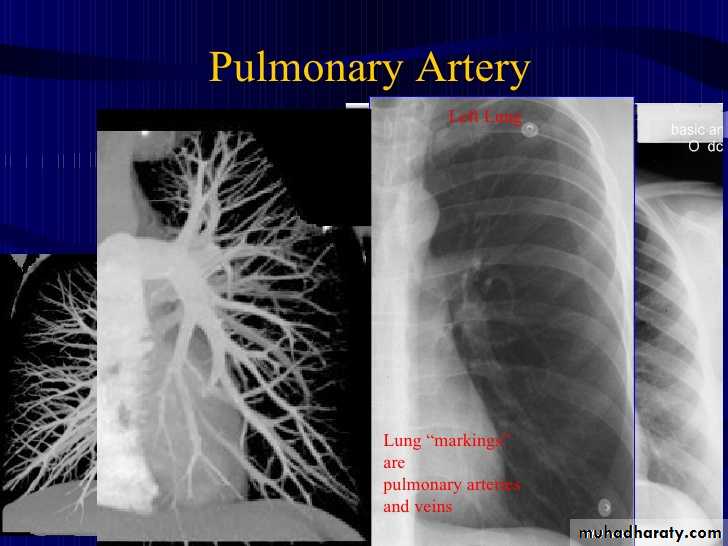
Lung markings reflects pulmonary vasculature
Soft tissues
The soft tissues are often overlooked when viewing a chest x-ray, however, abnormalities of the soft tissue may give important clues to a diagnosis. Whenever you look at a chest x-ray, have a look at the soft tissues, especially around the neck, the thoracic wall, and the breasts.Soft tissue fat
This close-up demonstrates a normal fat plane between layers of muscle. Fat is less dense than muscle and so appears blacker.
Note that the edge of fat is smooth. Irregular areas of black within the soft tissues may represent air tracking in the subcutaneous layers. This is known as surgical emphesyma.
Lung
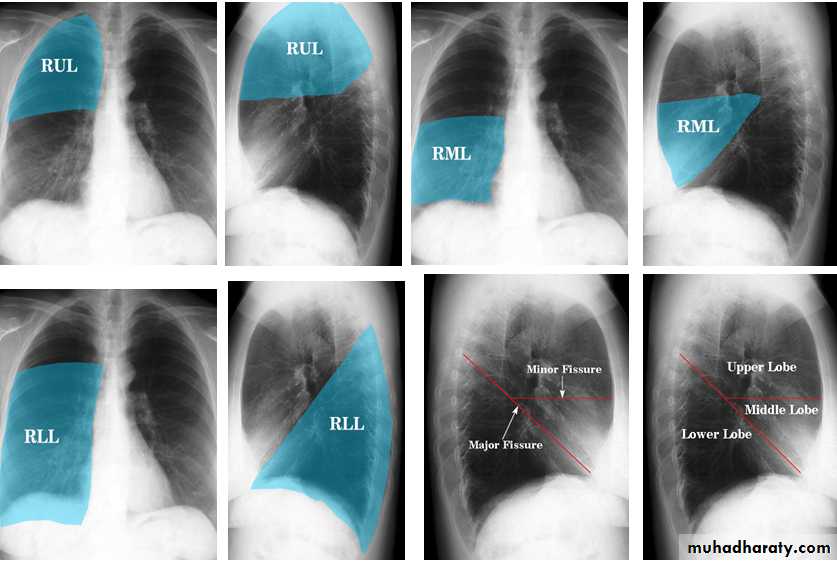
The left lung has two lobes and the right has three
Each lobe has its own pleural covering
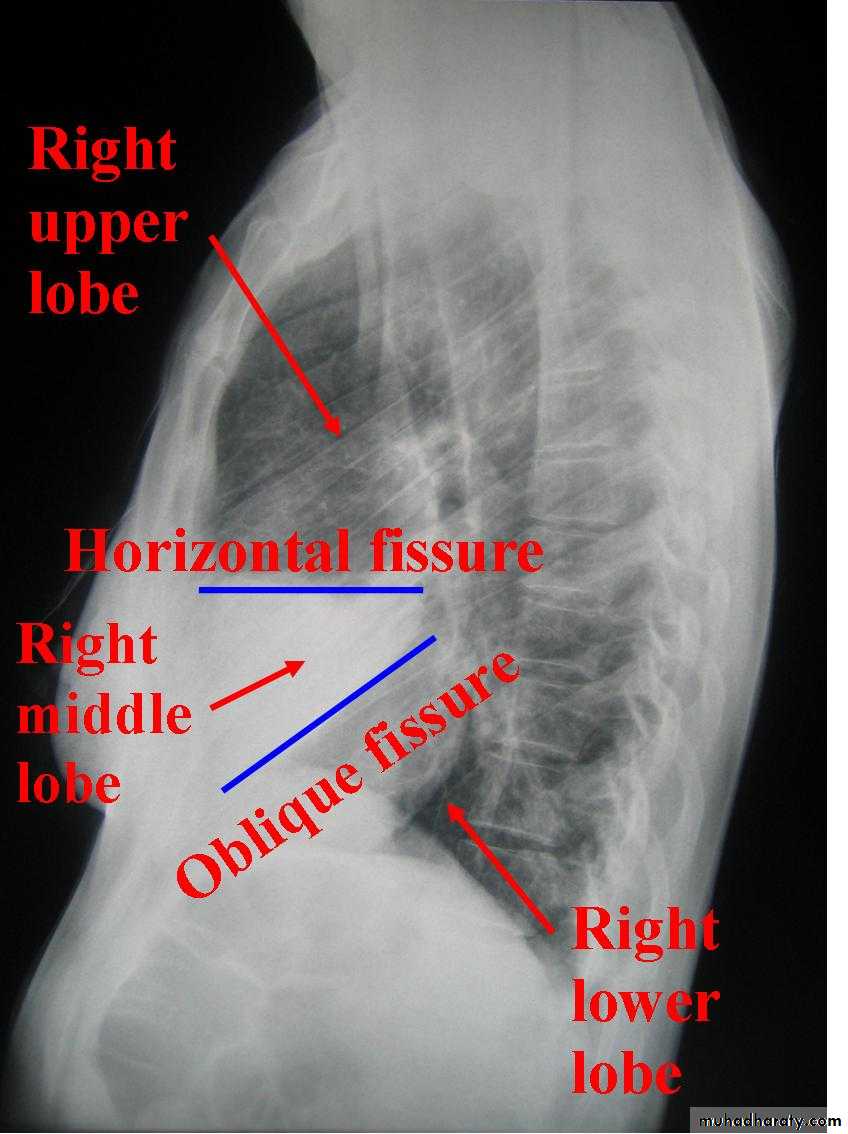
The horizontal fissure (right) is often seen on a normal frontal view
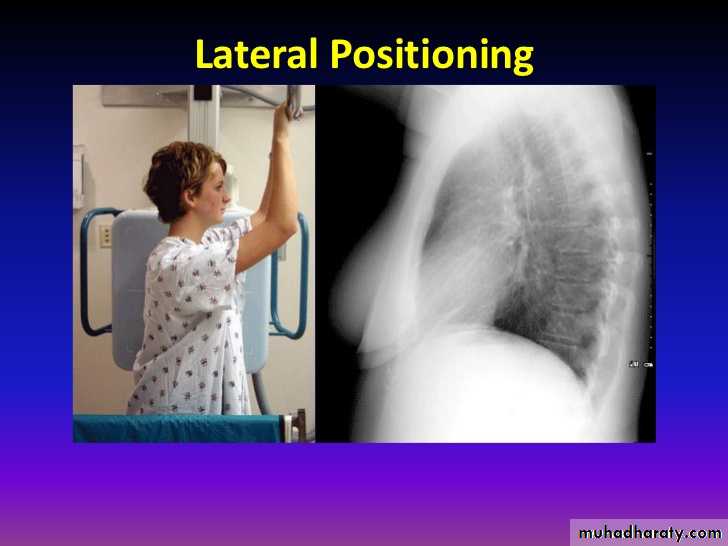
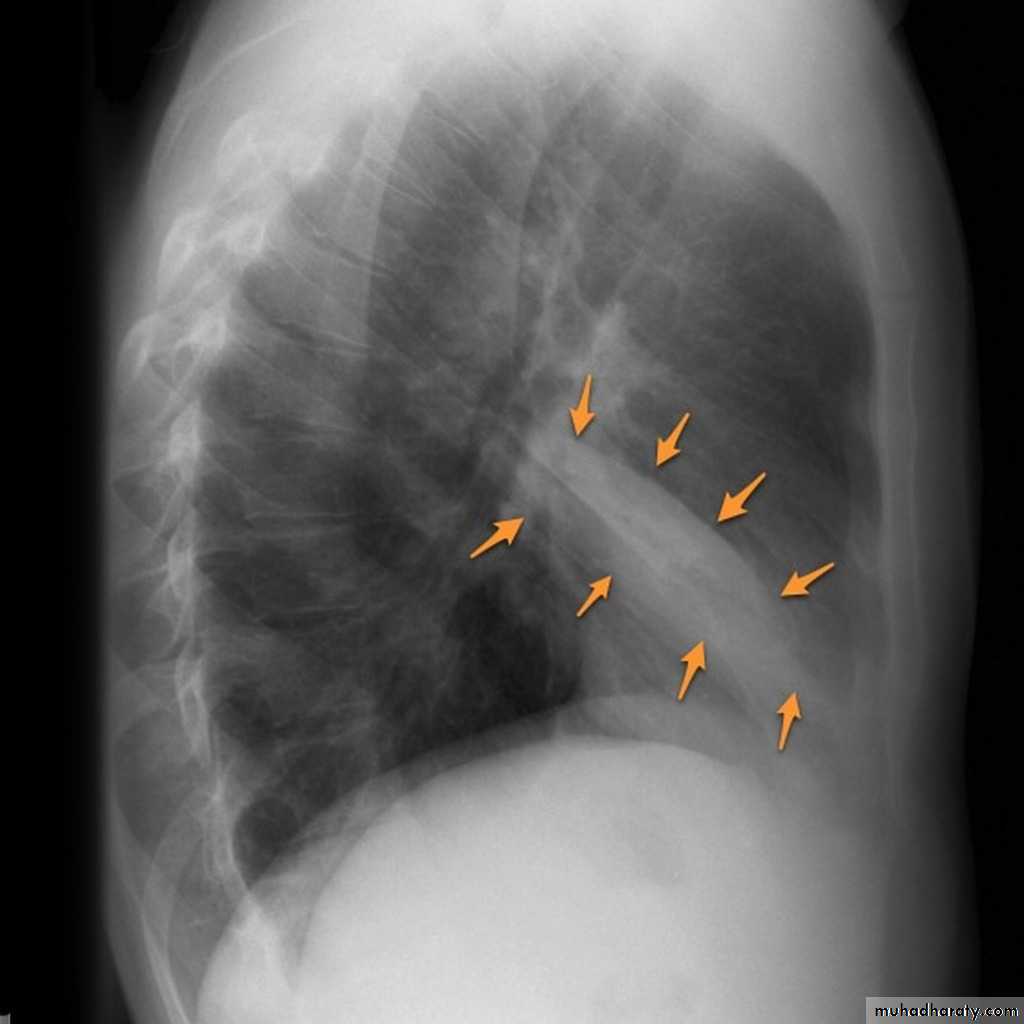
The oblique fissures are often seen on a normal lateral view .
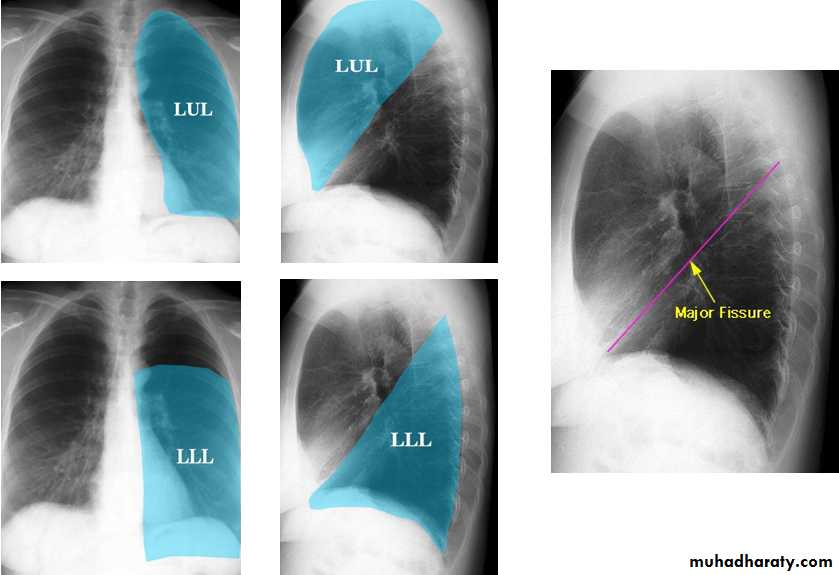
Lobes and fissures
This cut-out of a lateral chest x-ray shows the positions of the lobes of the right lung
On the left the oblique fissure is in a similar position but there is usually no horizontal fissure, and so there are only two lobes on the left.
Lung lesions
Lung lesionPatch >>>>>>>>>>>> a. consolidation (pneumonia & TB)
• b. collapse
Cavity >>>>>>>>>>>> a. TB
• b. abscess
c. ruptured hydatid cyst .
Mass >>>>>>>>>>>>> a. malignant mass (br.ca)
• b. metastases
• c. benign ( hydatid cyst)
Radiologic anatomy of the RT lung lobes
Radiologic anatomy of the LT lung lobes
Consolidation is a radiological sign that refers to non-specific air-space opacification on a chest radiograph or chest CT. Many things can fill the alveolar spaces, including fluid (heart failure), pus (pneumonia), blood (pulmonary haemorrhage) and cells (lung cancer)
Radiographic features
Consolidated areas are radio opaque on chest radiograph and chest CT compared to normally air filled lung tissue.
Lobar consolidation
Where increased density/opacity is seen in individual lung lobes. Sharp delineation can be seen when consolidation reaches a fissure, since it does not cross. Air bronchograms can also be seen due to bronchi becoming visible against the dense diseased tissue. Volume loss is usually not seen..
Multi-focal consolidation
Multiple areas of opacity seen throughout the lung most often is due to bronchopneumonia, starting from bronchi and spreading outwards. Usually ill defined with peripheral distribution. Neoplasms such as a primary malignancy or metastasis can also cause this picture.
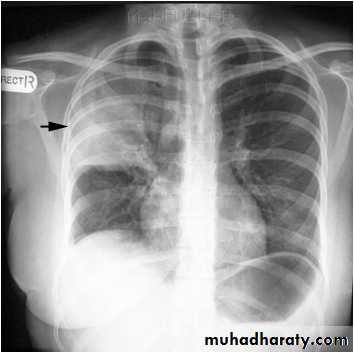
Right upper lobe consolidation
RUL consolidation will be seen as an increased opacity within the right upper lobe. Opacity may be sharply bordered by the horizontal fissureSome loss of outline of the upper right heart border may be apparent
Radiological sign in chest radiograph
Dense opacity seen above the horizontal fissure.
Air-bronchogram line
The lower border of the consolidation is sharply delinated by the horizontal fissure suggesting it lies in the anterior segment of the RUL
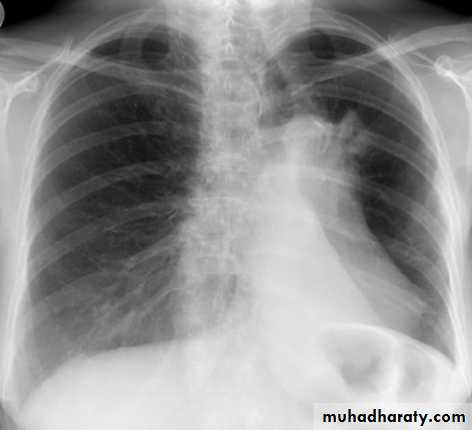
Right middle lobe consolidation
The right middle lobe is bordered superiorly by the horizontal fissure, and medially by the right heart border. Any abnormality, which increases density of this lobe, may therefore obscure the right heart border, or be limited superiorly by the horizontal fissure.
Radiographic features
Features of right middle lobe (RML) consolidation on CXR include:
opacification of the RML abutting the horizontal fissure
indistinct right heart border
loss of the medial aspect of the right hemidiaphragm
air bronchograms
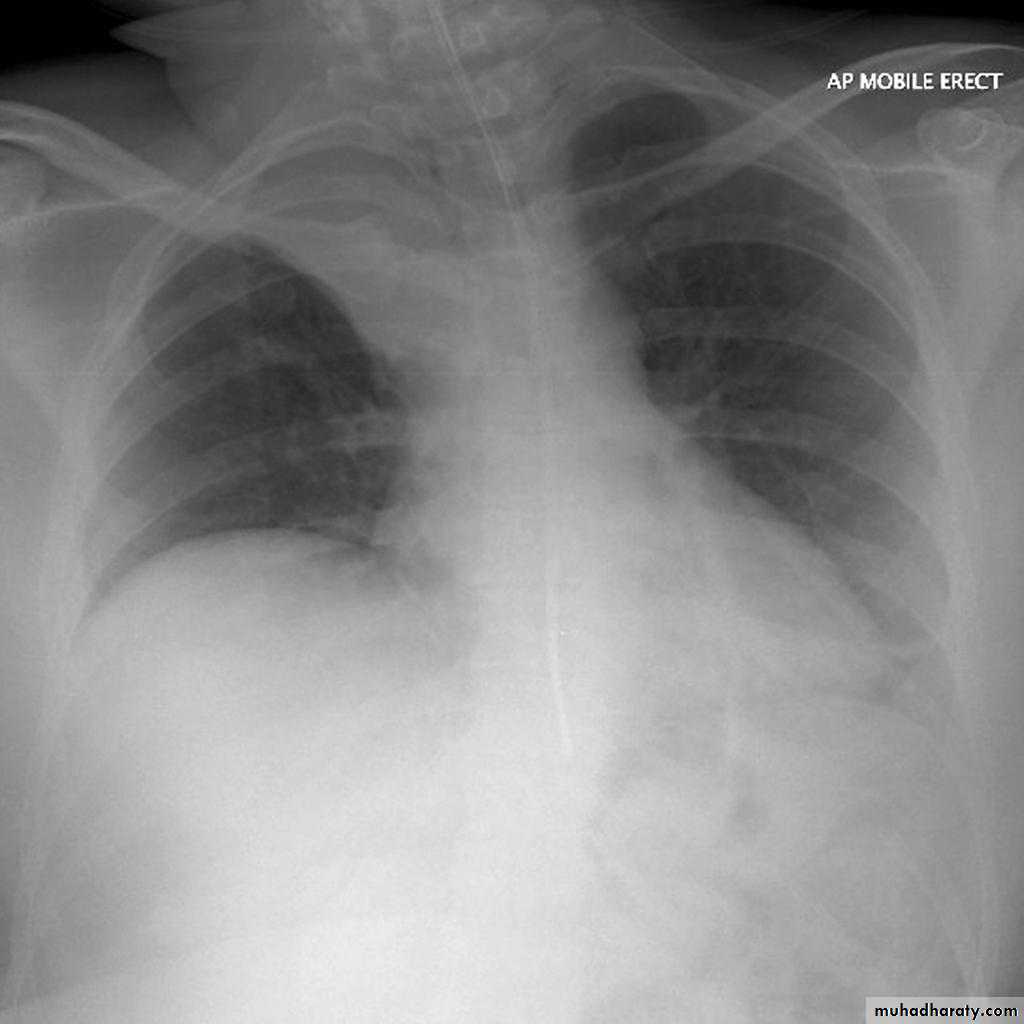
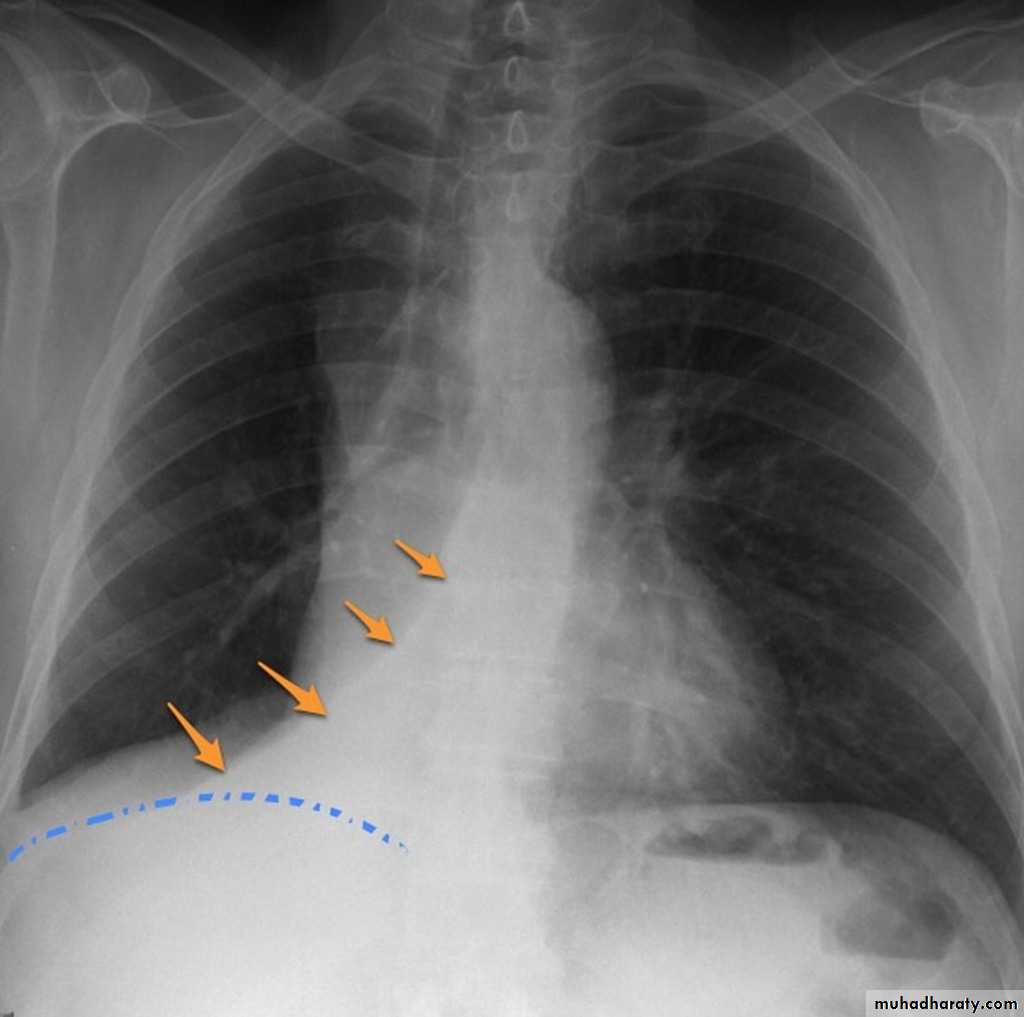
Right lower lobe consolidation
manifests as airspace shadowing that abuts the right hemidiaphragm,
obliterating the crisp margin of the hemidiaphragm and normal aerated lung.
bulging fissure sign refers to lobar consolidation where the affected portion of the lung is expanded. It is now rarely seen due to the widespread use of antibiotics.
The most common infective causative agents are :
Klebsiella pneumoniae
RT UL Consolidation



RT UL Consolidation

Klebsiella (Friedlander's) pneumonia: the bulging fissure sign.

RT middle lobe consolidation

RML consolidation
RT lower lobe consolidation
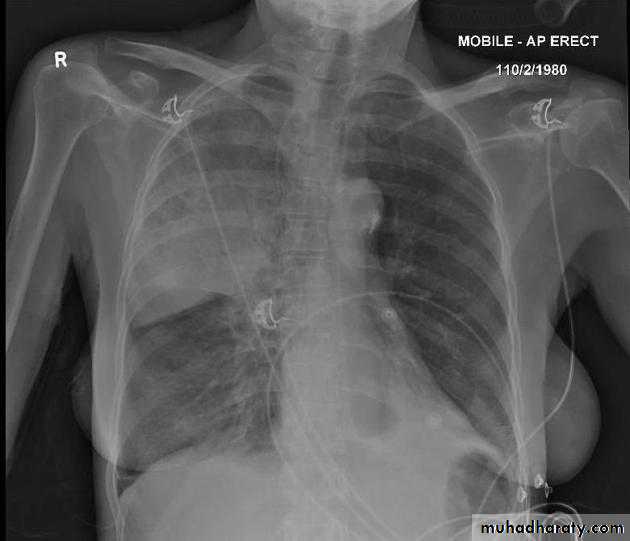
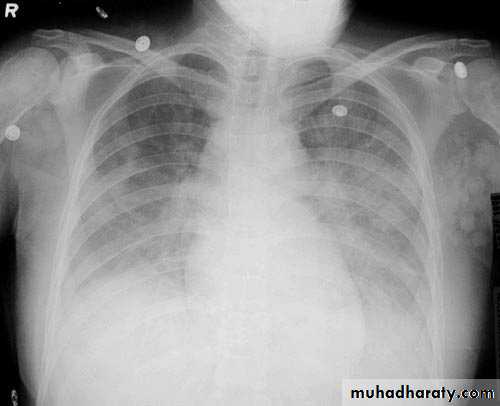
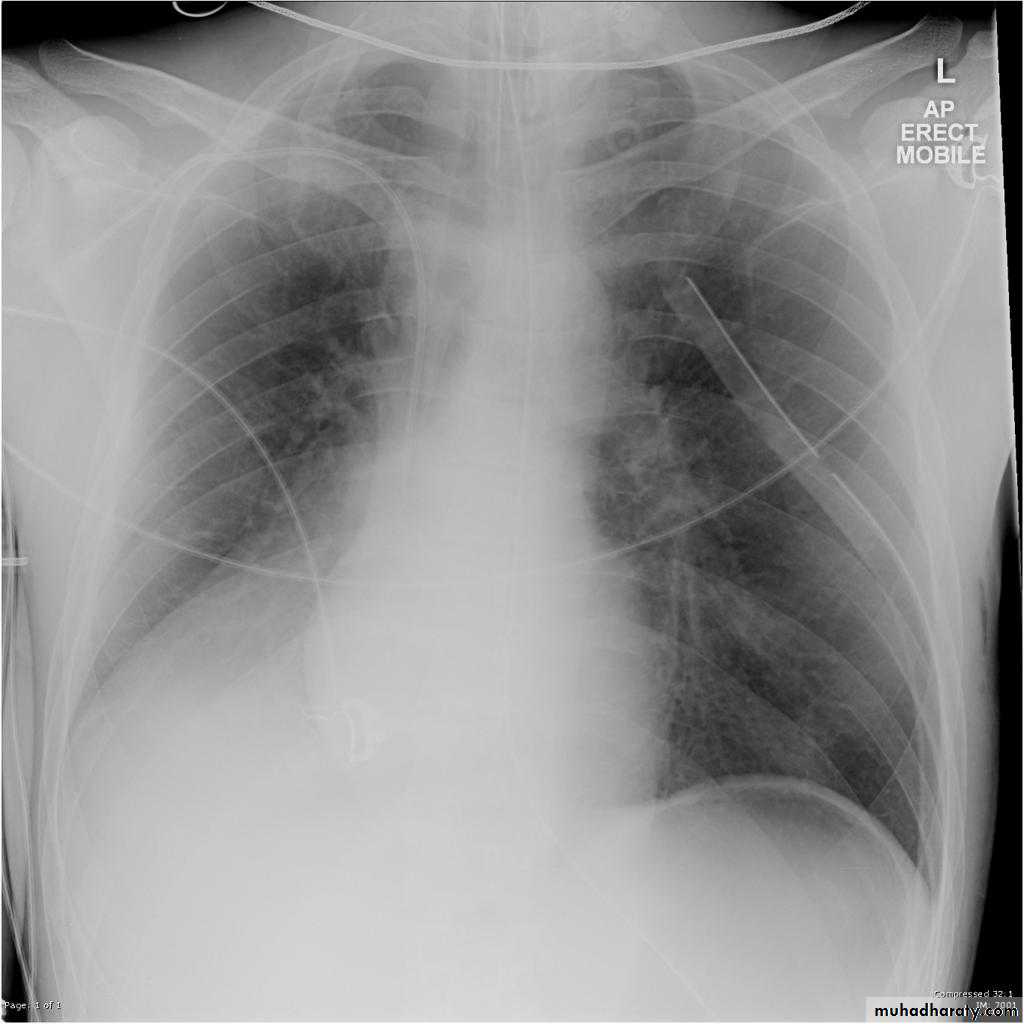
TOTAL LUNG CONSOLIDATION
Bronchopneumonia
Bronchopneumonia (also sometimes known as lobular pneumonia 1) is a radiological pattern associated with suppurative peribronchiolar inflammation and subsequent patchy consolidation of one or more secondary lobules of a lung in response to a bacterial pneumonia.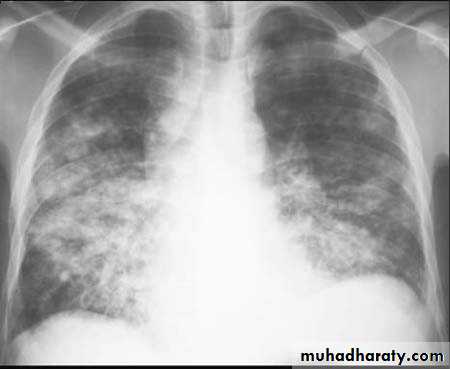
Lobar lung collapse
Lobar collapse refers to the collapse of an entire lobe of the lung. As such it is a subtype of atelectasis (although collapse is not entirely synonymous is atelectasis), which is a more generic term for 'incomplete expansion'. Individual lobes of the lung may collapse due to obstruction of the supplying bronchus.Causes include:
luminal
aspirated foreign material
mucous plugging
mural
bronchogenic carcinoma
extrinsic
compression by adjacent mass
Radiographic features
RadiographThe appearance on chest x-ray varies according to the lobe involved and are discussed separately:
>right upper lobe collapse
>right middle lobe collapse
>right lower lobe collapse
>left upper lobe collapse
>left lower lobe collapse
>lingular collapse
Some features, however, are generic markers of volume loss and are helpful in directing ones attention to the collapse, as well as enabling distinction from opacification of the lobe without collapse (e.g. lobar pneumonia). These features include 5:
elevation of the ipsilateral hemidiaphragm
crowding of the ipsilateral ribs
shift of the mediastinum towards the side of atelectasis
crowding of pulmonary vessels or air bronchograms
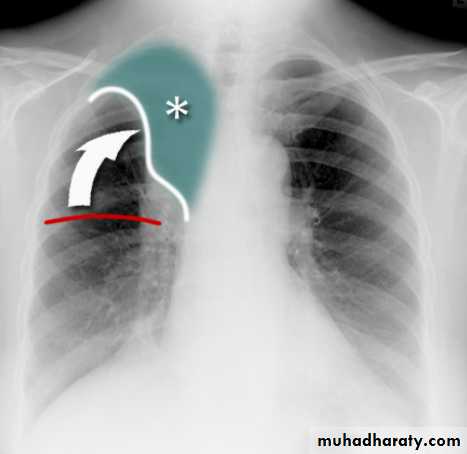
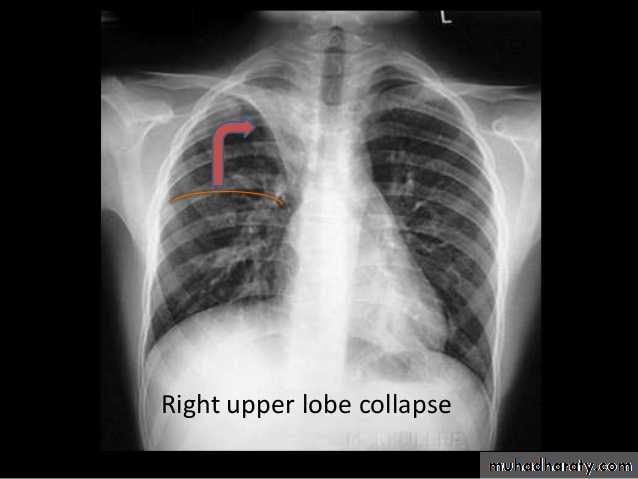
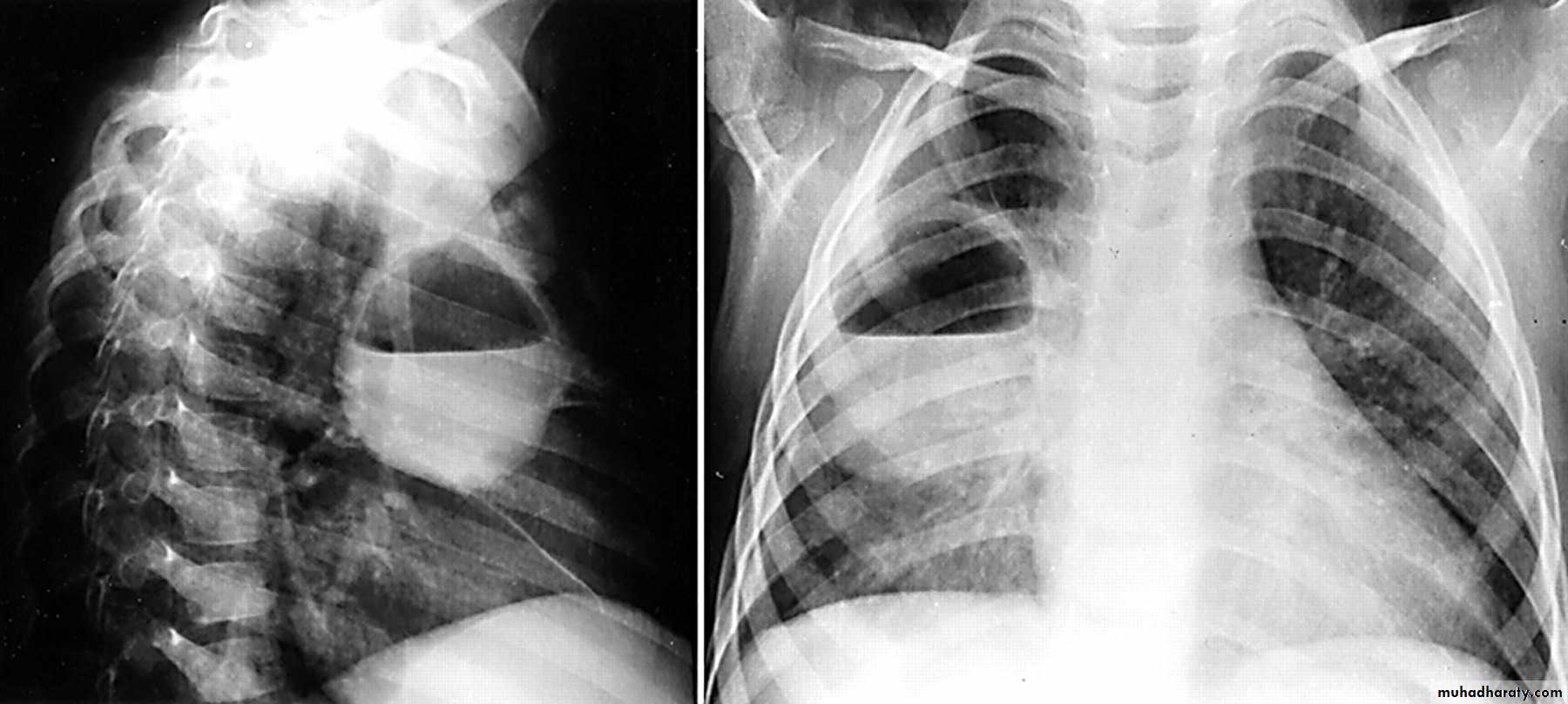
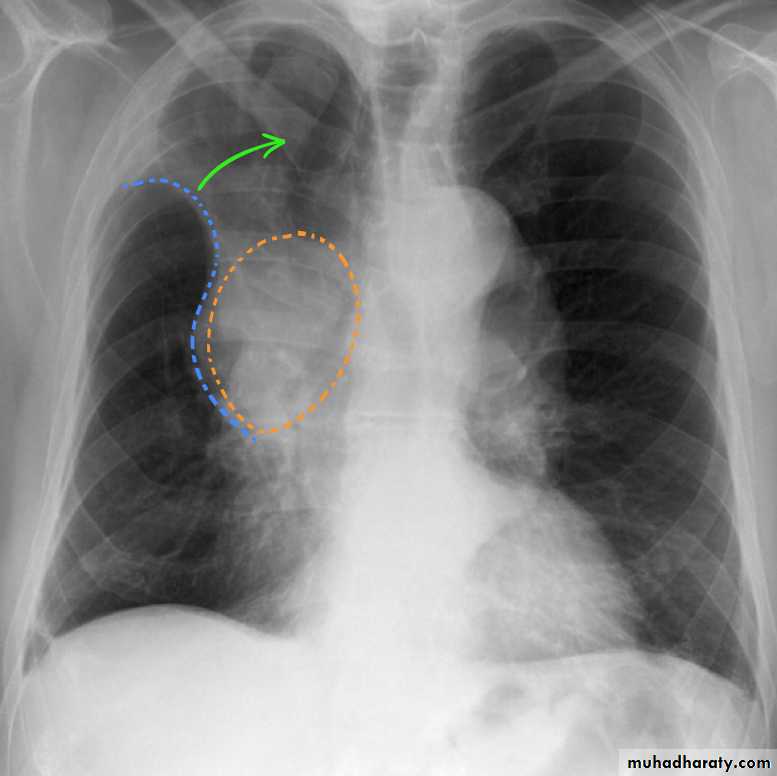
Right upper lobe collapse has distinctive features, and is usually easily identified on frontal chest radiographs .
Radiographic features
Chest radiograph
Collapse of the right upper lobe is usually relatively easy to identify on frontal radiographs. Features consist of :
increased density in the upper medial aspect of the right hemithorax
elevation of the horizontal fissure
loss of the normal right medial cardiomediastinal contour
elevation of the right hilum
hyperinflation of the right middle and lower lobe result in increased translucency of the mid and lower parts of the right lung
right juxtaphrenic peak
A common cause of lobar collapse is a hilar mass. When a right hilar mass is combined with collapse of the right upper lobe, the result is an S shape to elevated horizontal fissure. This is known as Golden S sign .
Non-specific signs indicating right sided atelectasis are also usually present including:
elevation of the hemidiaphragm
crowding of the right sided ribs
shift of the mediastinum and trachea to the right
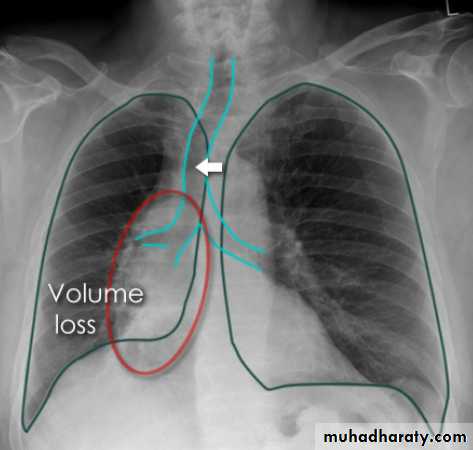
Right middle lobe collapse has distinctive features, and is usually relatively easily identified.
Radiographic features
Chest radiograph
Frontal chest XR showing opasity cause obscuration of the RT cardiac border
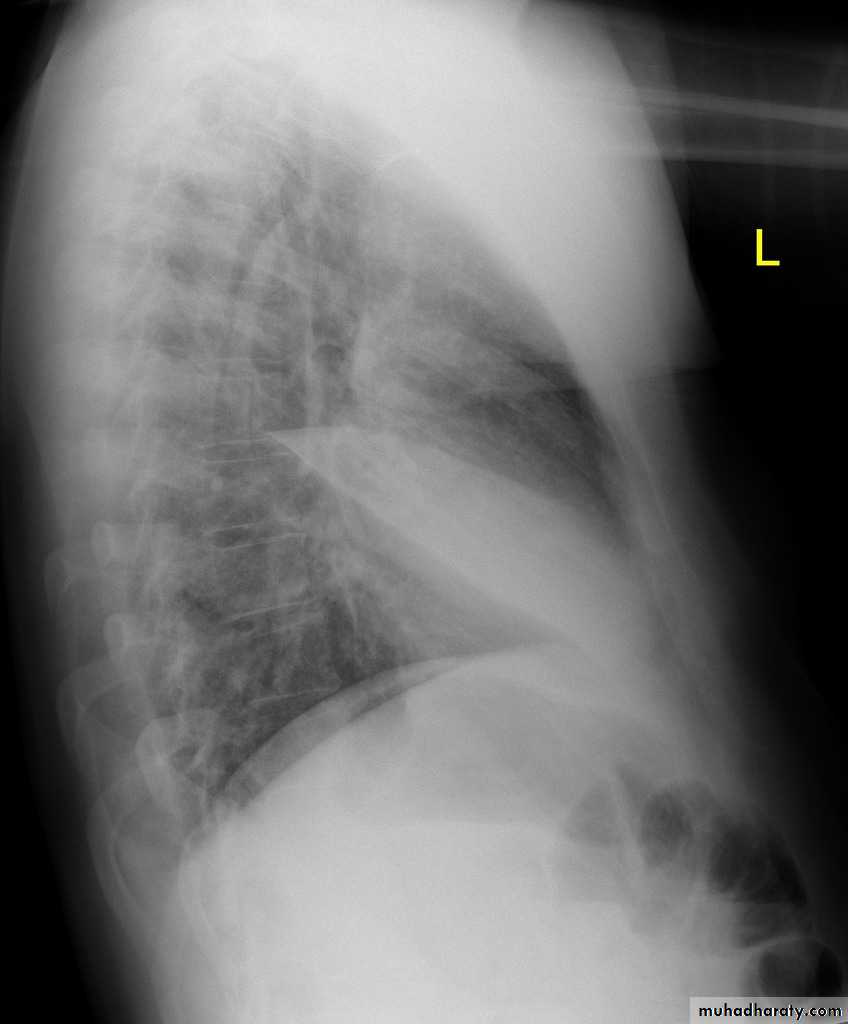
Lateral chest XR film the opacity is tongue like shape
versus (triangular in shape) in RT middle lobe consolidation seen in lateral chest XR film
RT lower lobe collapse
usually the medial aspect of the dome of right hemidiaphragm is lost.
the right hilum is depressed
It is important to note that the right heart border, which is contacted by the right middle lobe remains well seen.
Non-specific signs indicating right sided atelectasis may also be present (although due to the small size of the right middle lobe they may well be subtle). They include:
elevation of the hemidiaphragm
crowding of the right sided ribs
shift of the mediastinum to the right
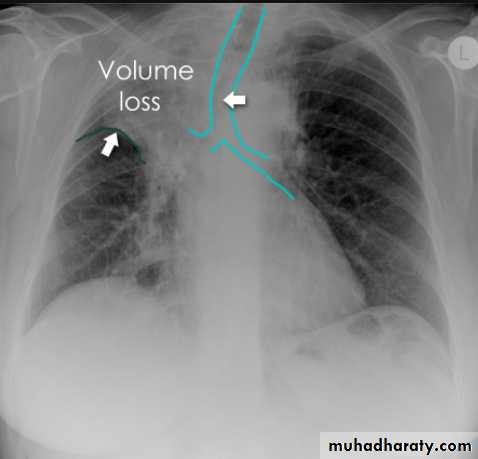
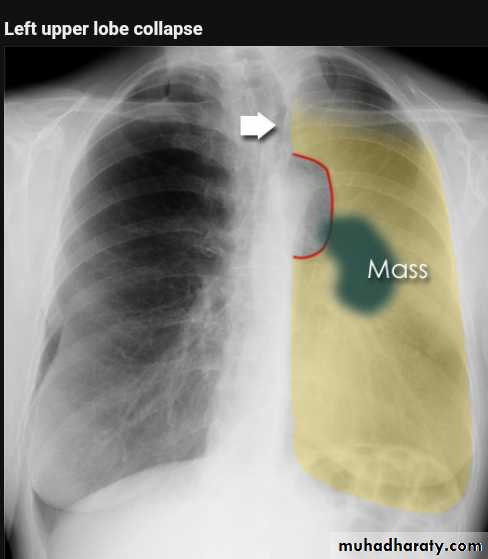
Left upper lobe collapse has distinctive features but can be challenging to identify on chest radiographs by the uninitiated.
Radiographic features
The left upper lobe collapses anteriorly becoming a thin sheet of tissue apposed to the anterior chest wall, and appears as a hazy or veiling opacity extending out from the hilum and fading out inferiorly . It thus reverses the normal slight increase in radiographic density seen as you move down the lung (due to increased thickness of the chest soft tissues).
Parts of the normal cardiomediastinal contour may also be obliterated where the left upper lobe, particularly the lingula abut the left heart border. The anterior parts of the aortic arch are also often obliterated from view.
In some cases the hyperexpanded superior segment of the left lower lobe insinuates itself between the left upper lobe and the superior mediastinum, sharply silhouetting the aortic arch and resulting in a lucency medially. This is known as the luftsichel sign.
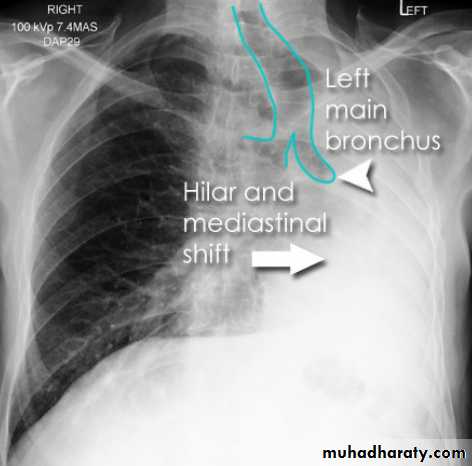
The left hilum is also drawn upwards, resulting in an almost horizontal course of the left main bronchus and vertical course of the left lower lobe bronchus.
Non-specific signs indicating left sided atelectasis will also be present, including:
elevation of the hemidiaphragm
'peaked' or 'tented' hemidiaphragm: juxtaphrenic peak sign
crowding of the left sided ribs
shift of the mediastinum to the left
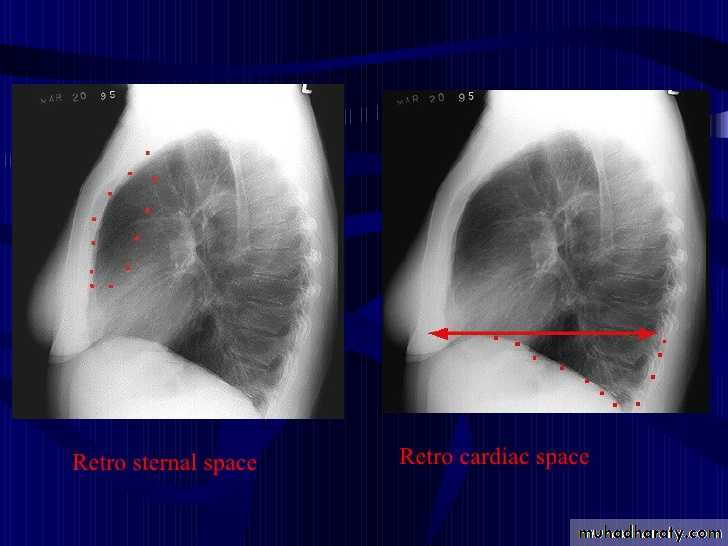
On lateral projections the left lower lobe is hyperexpanded and the oblique fissure displaced anteriorly. There is associated increase in the retrosternal opacity.
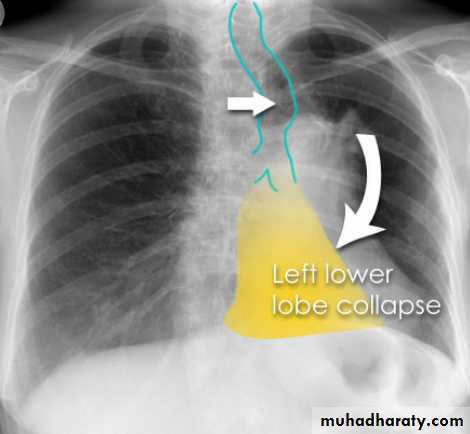
Left lower lobe collapse has distinctive features, and can be readily identified on frontal chest radiographs, provided attention is paid to the normal cardiomediastinal contours. The shadow cast by the heart does however make it harder to see than the right lower lobe collapse
Radiographic features
Left lower lobe collapseis readily identified in a well penetrated film of a patient with normal sized heart, but can be challenging in the typical patient with collapse, namely unwell patients, with portable (AP) often under-penetrated films, often with concomitant cardiomegaly. Features to be observed include :
triangular opacity in the posteromedial aspect of the left lung
edge of collapsed lung may create a 'double cardiac contour'
left hilum will be depressed
loss of the normal left hemidaphgragmatic outline
loss of the outline of the descending aorta
Non-specific signs indicating left sided atelectasis are usually also be present including:
elevation of the hemidiaphragm
crowding of the left sided ribs
shift of the mediastinum to the left
On lateral projection the left hemidiaphragmatic outline is lost posteriorly and the lower thoracic vertebrae appear denser than normal (they are usually more radiolucent than the upper vertebrae) .

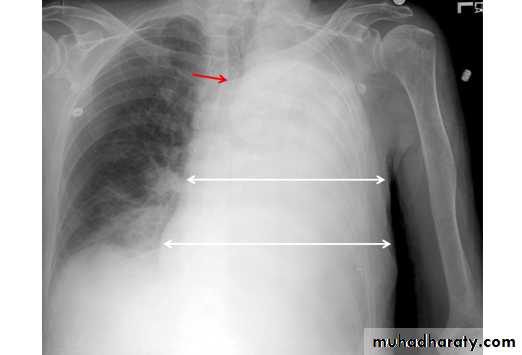
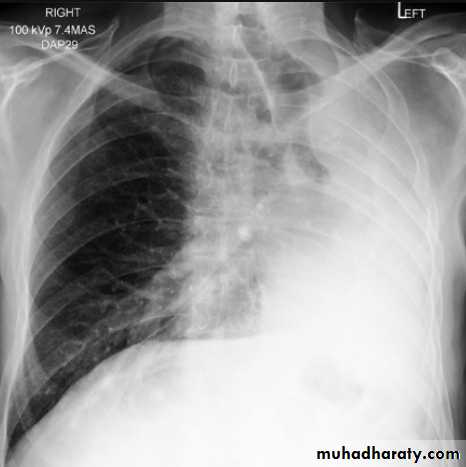
Total lung collapse
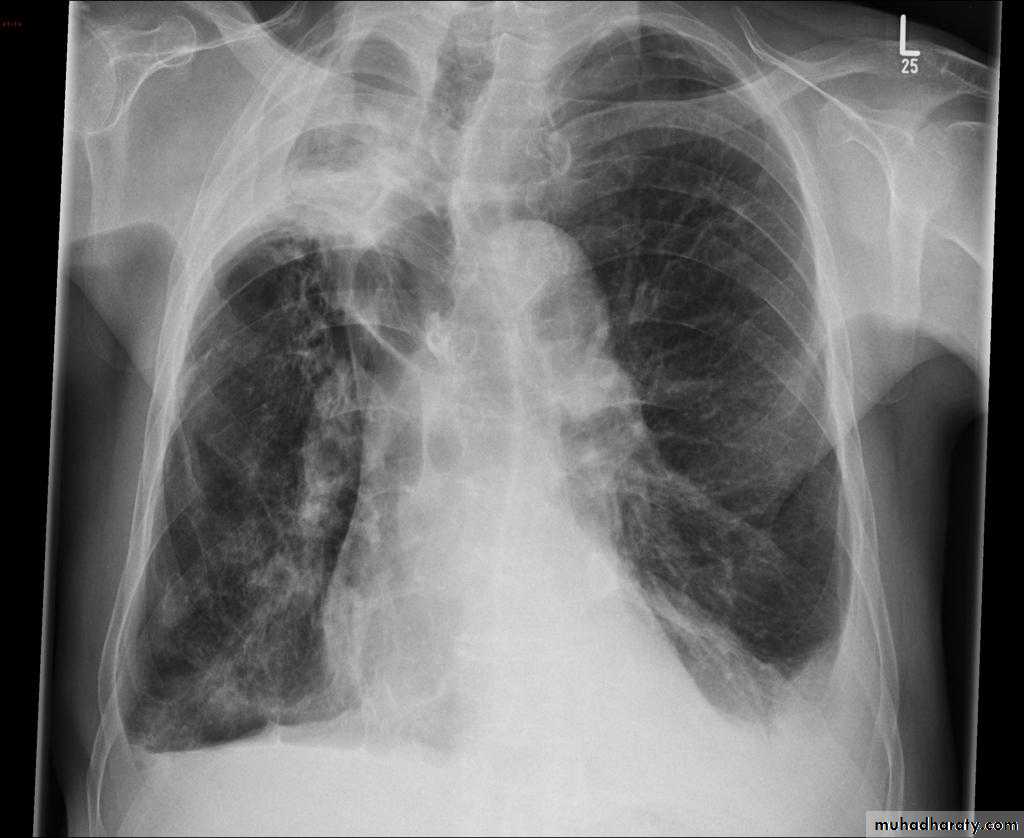
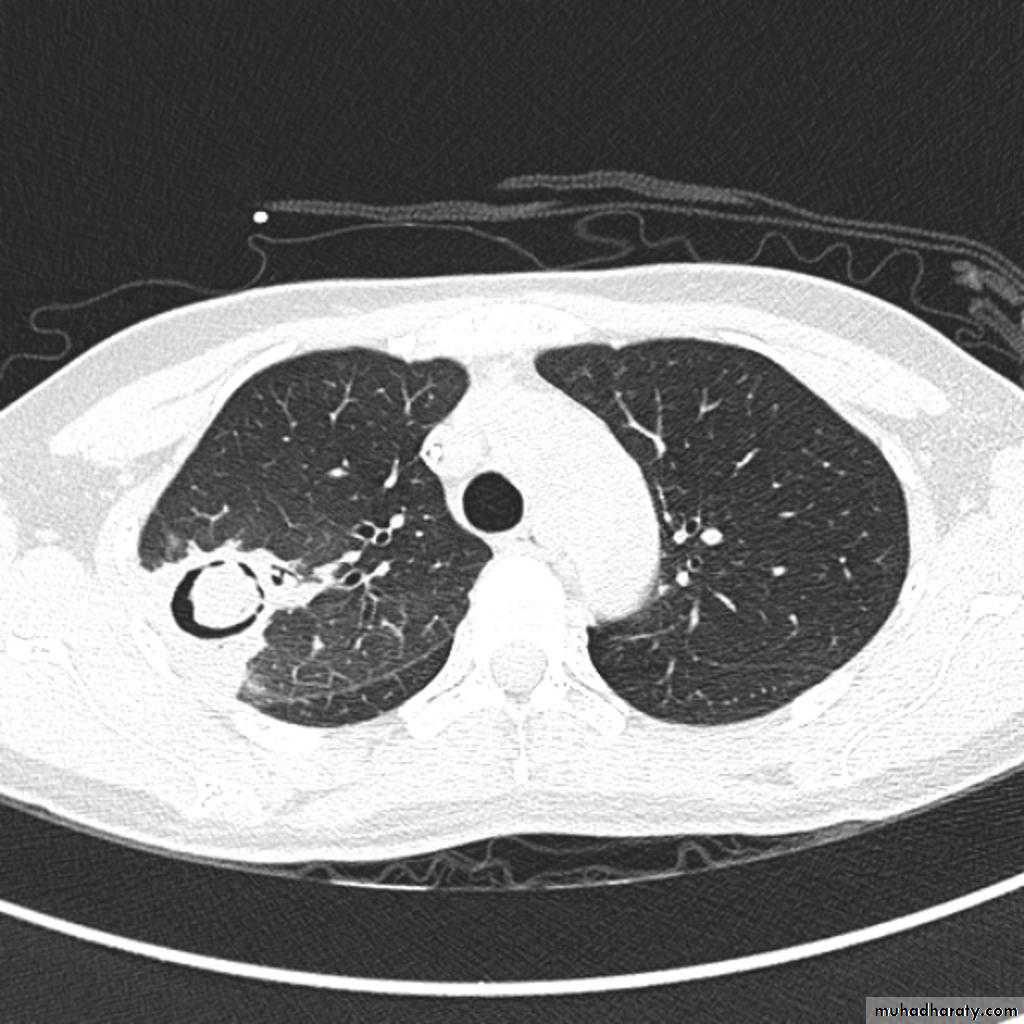
Lung abscess is a circumscribed collection of pus within the lung, is are potentially life threatening. They are often complicated to manage and difficult to treat
Lung abscesses are divided according to their duration into acute (< 6 weeks) and chronic (> 6 weeks) .
A primary abscess is one which develops as a result of primary infection of the lung. They most commonly arise from aspiration, necrotising pneumonia or chronic pneumonia, e.g. pulmonary tuberculosis
Some organisms are particularly prone to causes significant necrotising pneumonia resulting in cavitation and abscess formation. These include :
Staphylococcus aureus
Klebsiella sp: Klebsiella pneumonia
Pseudomonas sp
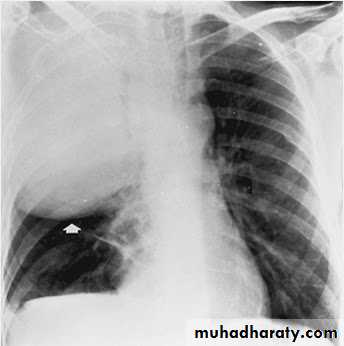
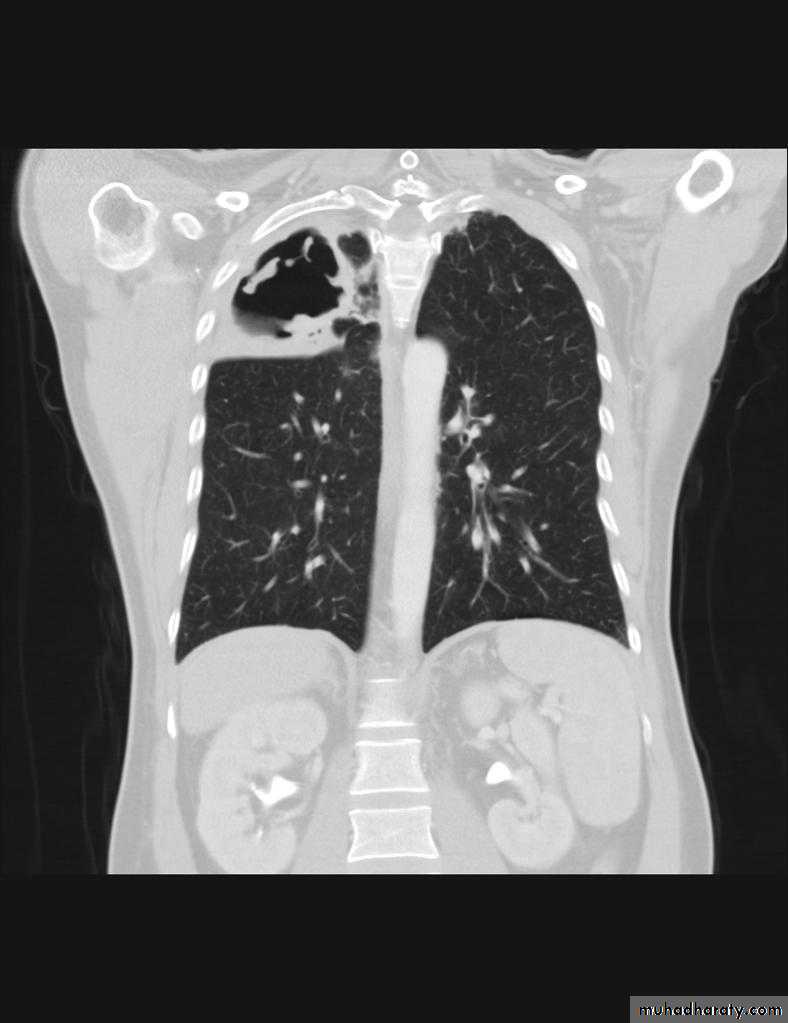
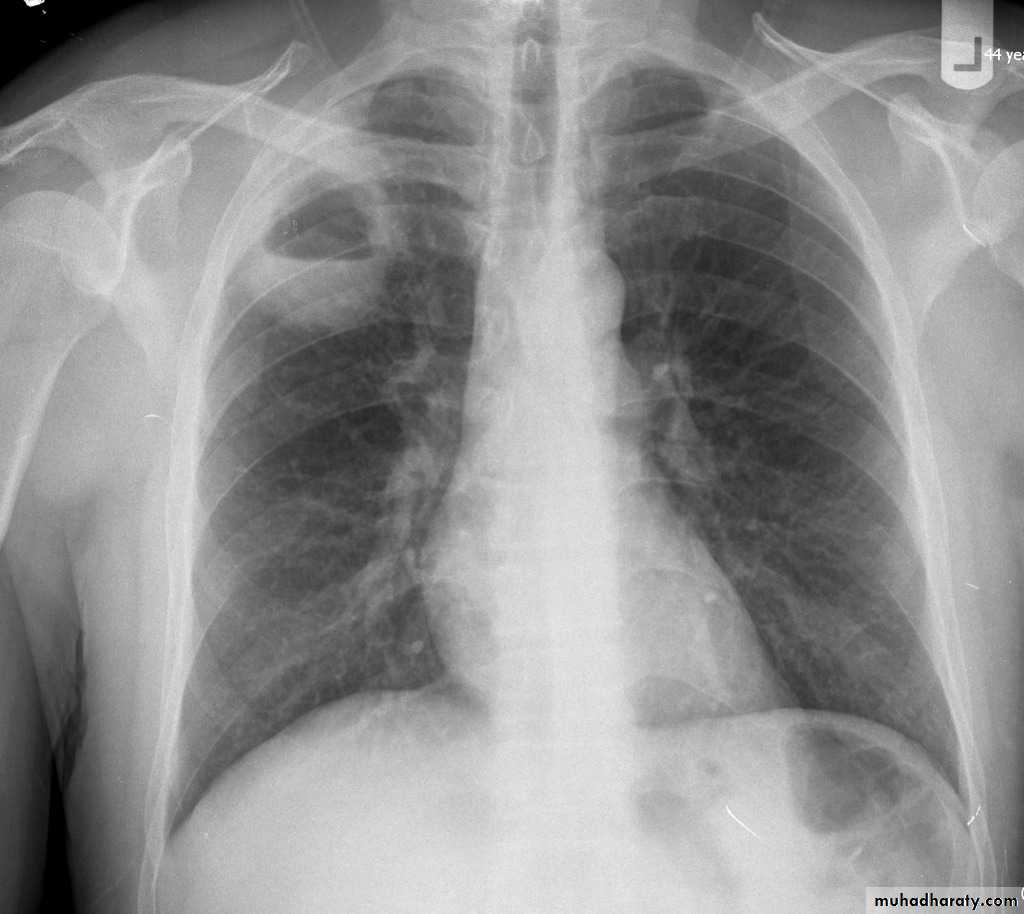
Plain film
The classical appearance of a pulmonary abscess is a cavity containing an air-fluid level. In general abscesses are round in shape, and appear similar in both frontal and lateral projections.
Very important
Empyema vs pulmonary abscess1.relationship to adjacent bronchi / vessels
abscesses will abruptly interrupt bronchovascular structures
empyema will usually distort and compress adjacent lung
2.split pleura sign thickening and separation of visceral and parietal pleura is a sign of empyema
3.abscesses have thick irregular walls
empyema are usually smoother
4.angle with pleura
abscesses usually have an acute angle (claw sign)
empyema have obtuse angles
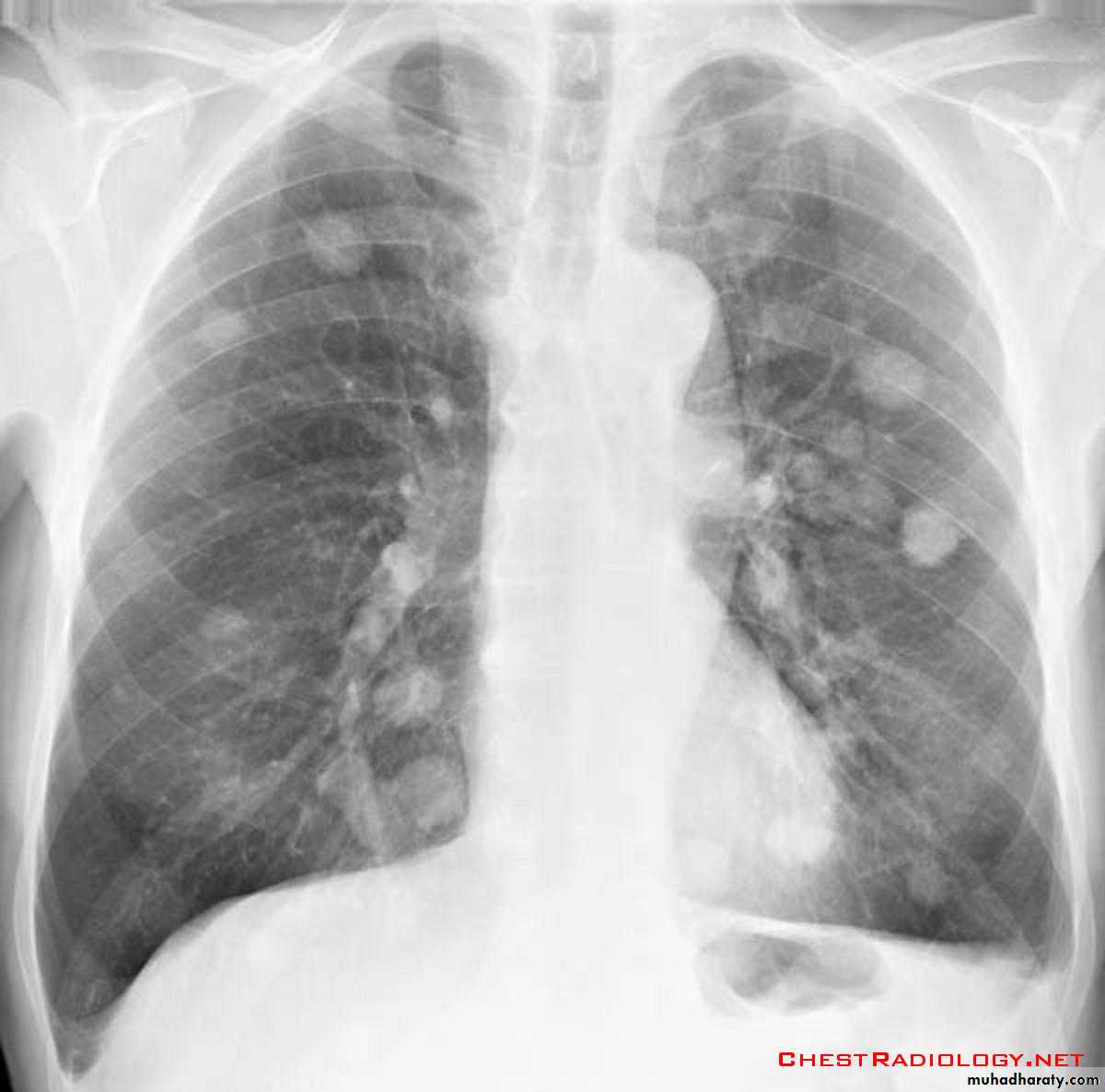
Hydatid cysts result from infection by the Echinococcus, and can result in cyst formation anywhere in the body. Humans are accidental host and the infection occurs by ingesting food contaminated with Echinococcus eggs ,Pulmonary hydatid infection is a common manifestation of hydatid disease.The lung is the second most common site of involvement with echinococcosis granulosus in adults after the liver (10-30% of cases), and the most common site in children. The coexistence of liver and lung disease is present in only 6% of patients .
Chest XR features include :
Non-complicated hydatid
multiple or solitary rounded opacity
diameter of 1-20 cm
unilateral or bilateral
predominantly found in the lower lobes
Complicated cysts may show:
meniscus sign or air crescent sign
cumbo sign or onion peel signThe onion peel sign (also called the cumbo sign) is a feature seen with complicated pulmonary hydatid cyst in which air lining between the endocyst and pericyst has the appearance of an onion
water-lily is seen in hydatid infections when there is detachment of the endocyst membrane which results in floating membranes within the pericyst that mimic the appearance of a water lily.
consolidation adjacent to the cyst (ruptured cyst)
Simple HC Ruptured HC

Lung tumor
Lung cancer, or frequently, if somewhat incorrectly, known as bronchogenic carcinoma, is the most common cause of cancer in men, and the 6th most frequent cancer in women worldwide. It is the leading cause of cancer mortality worldwide in both men and women and accounts for approximately 20% of all cancer deathssubtype has a different radiographic appearance, demographic, and prognosis:
squamous cell carcinoma of the lung
adenocarcinoma of the lung
large cell carcinoma of the lung
small cell carcinoma of the lung
Other malignant pulmonary neoplasms include lymphoma
Associations
Various paraneoplastic syndromes can arise in the setting of lung cancer
Sequamous cell CAmost common primary lung malignancy to cause paraneoplastic syndromes and SVC obstruction
Radiology of BGCA
The appearance depends on the location of the lesion.1.The more central lesions may merely appear as a bulky hilum, representing the tumor and local nodal involvement the lesion is irregular in outline have spiky or sun ray spiculation .
2.Lobar collapse may be seen due to obstruction of a bronchus. When the right upper lobe is collapsed and a hilar mass is present, this is known as the Golden S sign.
3.A more peripheral location may appear as a rounded or spiculated mass. Cavitation may be seen as an air-fluid level , more to be large cell CA .
4.Chest wall invasion is difficult to identify on plain films unless there is destruction of the adjacent rib or evidence of soft tissue growing into the soft tissues superficial to the ribs.
5.A pleural effusion may also be seen, and although it is associated with a poor prognosis, not all effusions are due to malignant involvement of the pleural space.

Pancosts tumor
A Pancoast tumour, otherwise known as superior sulcus tumour, refers to a relatively uncommon situation where a primary bronchogenic carcinoma arises in the lung apex and invades the surrounding soft tissues , adeno CA being the most frequent type ,Plain film
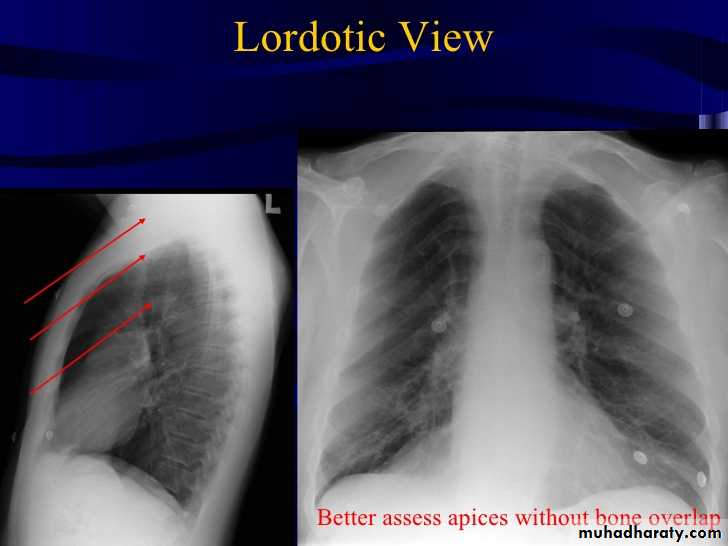
Plain films demonstrate a soft tissue opacity at the apex of the lung. Occasionally with rib involvement with extension into the supraclavicular fossa may be evident with surrounded bony destruction . Lordotic views may be helpful .
Must important complication is involvement of the sympathetic chain >>>>
* Ptosis
* Meiosis
* unhydrosis
Pancost tumor

Secondary lung tumor
Pulmonary metastases are common and the result of metastatic spread to the lungs from a variety of tumors and can spread via blood or lymphatics.1.Cannonball metastases refer to large well circumscribed, round multiple opacities like cannonballs
2.lymphangitis carcinomatosis , is the term given to tumor spread through the lymphatics of the lung , and is most commonly seen secondary to adenocarcinoma Unfortunately up to a quarter of patients with subsequently established lymphangitic carcinomatosis have normal chest x-rays . When abnormal the most common finding is of a reticulonodular pattern, with thickening of the interlobular septae which may resemble Kerley B lines + /- pleural effusion .
3.innumerable small metastases (miliary pattern).


Pleural lesions
Pleural effusionPleural effusion tends to be used as a catch-all term denoting a collection of fluid within the pleural space. This can be further divided into exudates and transudates depending on the biochemical analysis of aspirated pleural fluid. Essentially it represents any pathological process which overwhelms the pleura's ability to reabsorb fluid.
Radiographic appearances
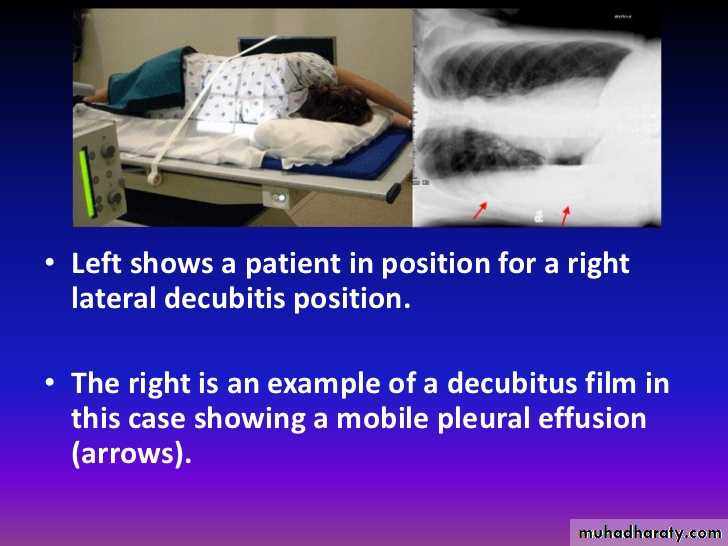
Plain radiographChest radiographs are the most commonly used examination to assess for presence of a pleural effusion, however it should be noted that on a routine erect chest x-ray as much as 250-600 ml of fluid is required before it becomes evident 6. A lateral decubitus film is most sensitive, able to identify even a small amount of fluid. At the other extreme, supine films can mask large quantities of fluid.
CXR (lateral decubitus)
A lateral decubitus film (obtained with the patient lying on their side, effusion side down, with a cross table shoot through technique) can visualise small amounts of fluid layering against the dependent parietal pleura.
CXR (erect)
Both PA and AP erect films are insensitive to small amounts of fluid. Features include:
blunting of the costophrenic angle
blunting of the cardiophrenic angle
fluid within the horizontal or oblique fissures
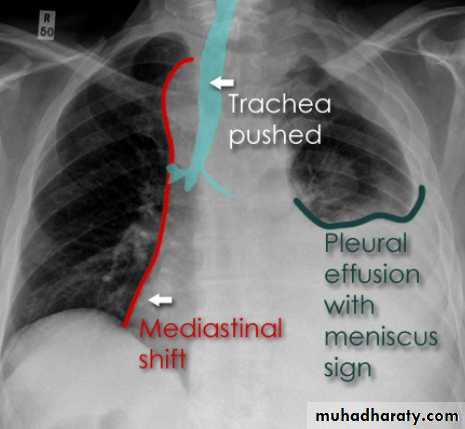
eventually a meniscus will be seen, on frontal films seen laterally and gently sloping medially (note:
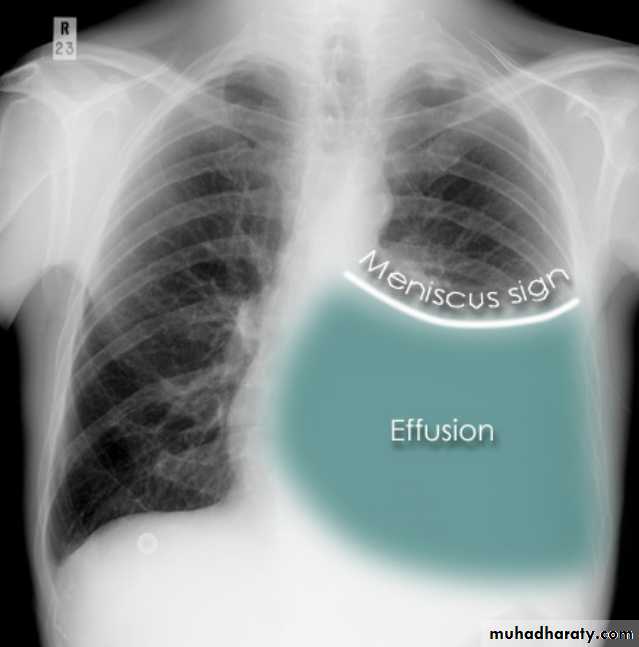

A subpulmonic effusion (infrapulmonary effusion) may be seen when there is previously established pulmonary disease, but can also be encountered in normal lungs , They are more common on the right, and usually unilateral
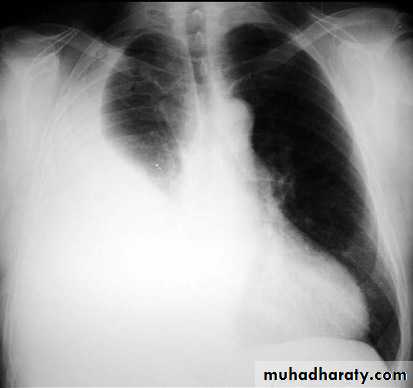
with large volume effusions, mediastinal shift occurs away from the effusion (note: if coexistent collapse dominates then mediastinal shift may occur towards the effusion)

An empyema can resemble a pleural effusion
and can mimic a peripheral pulmonary abscess, although a number of features usually enable distinction between the two Features that help distinguish a pleural effusion from an empyema include:Shape and location
Empyemas usually:
form an obtuse angle with the chest wall
unilateral or markedly asymmetric whereas pleural effusions are (if of any significant size) usually bilateral and similar in size .
lenticular in shape (bi-convex), whereas pleural effusions are crescentic in shape (i.e concave towards the lung)
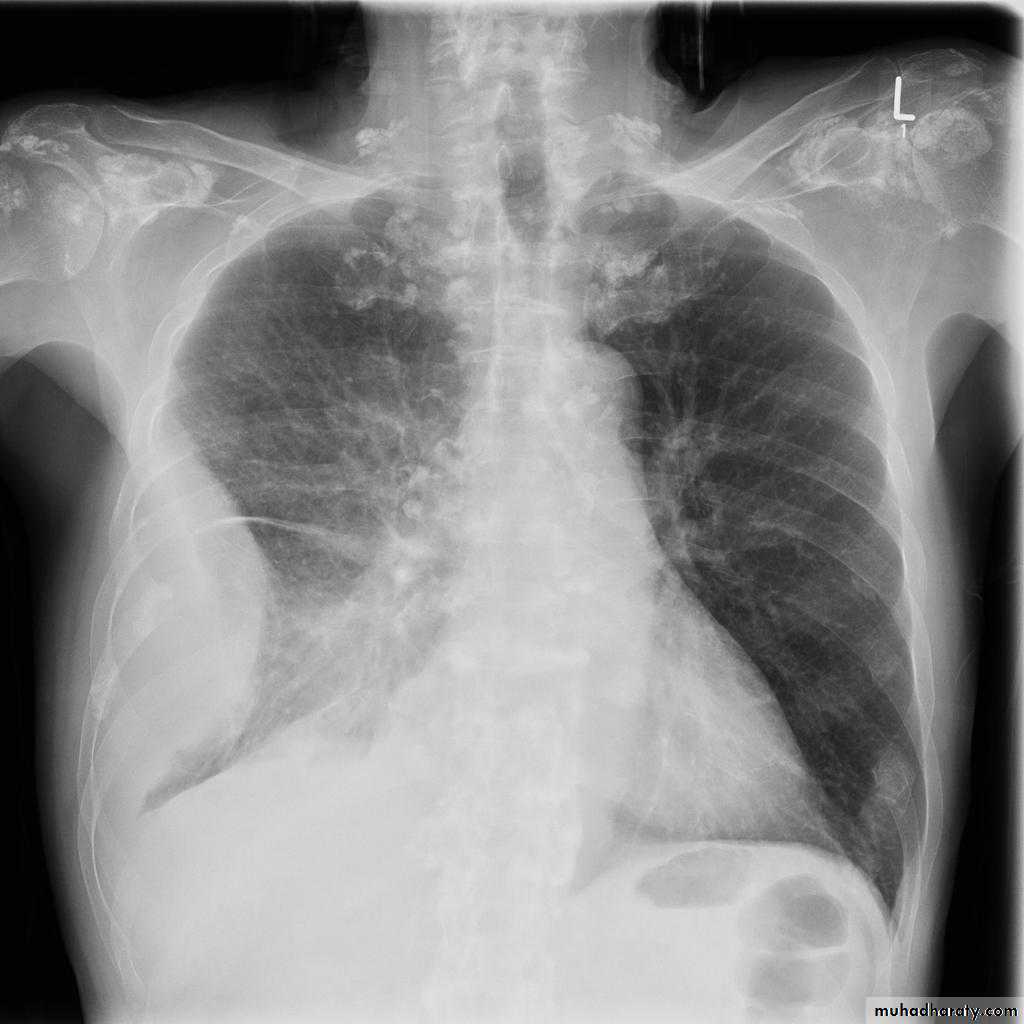
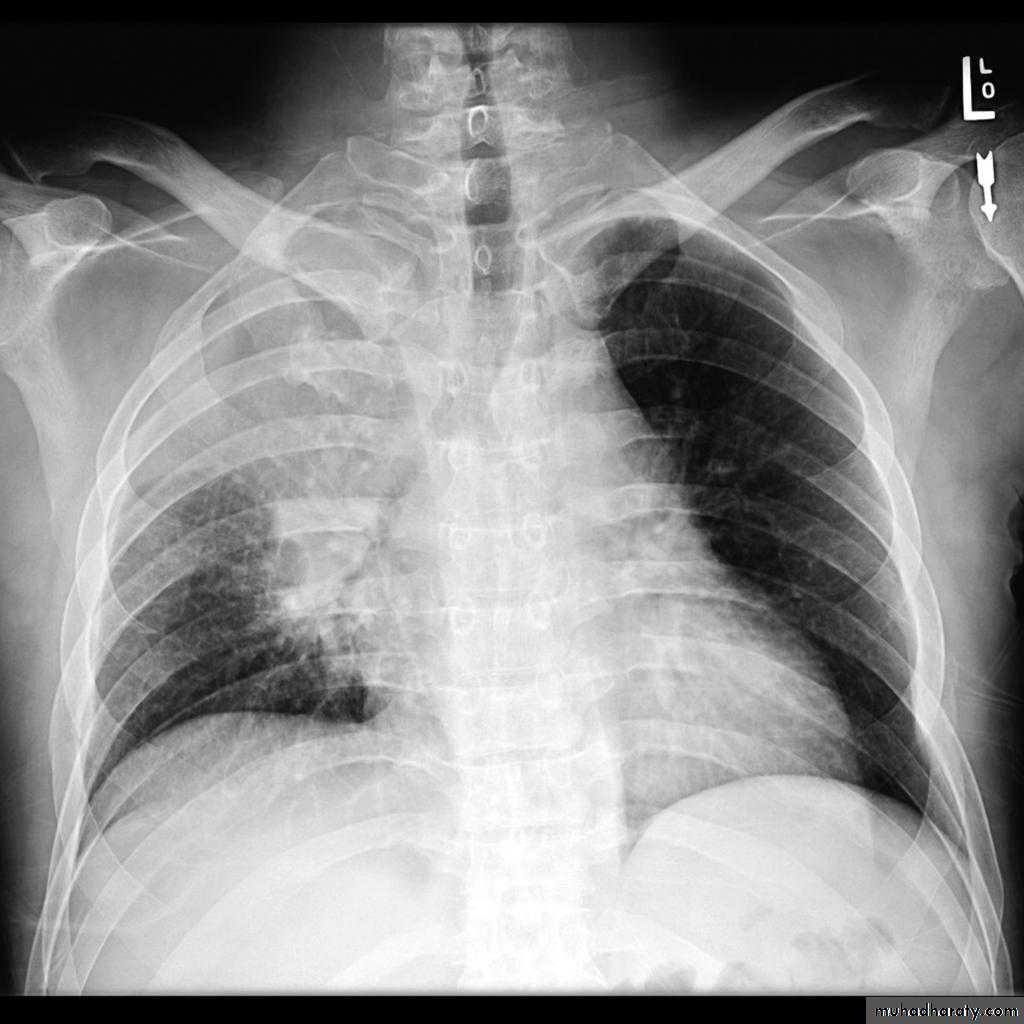
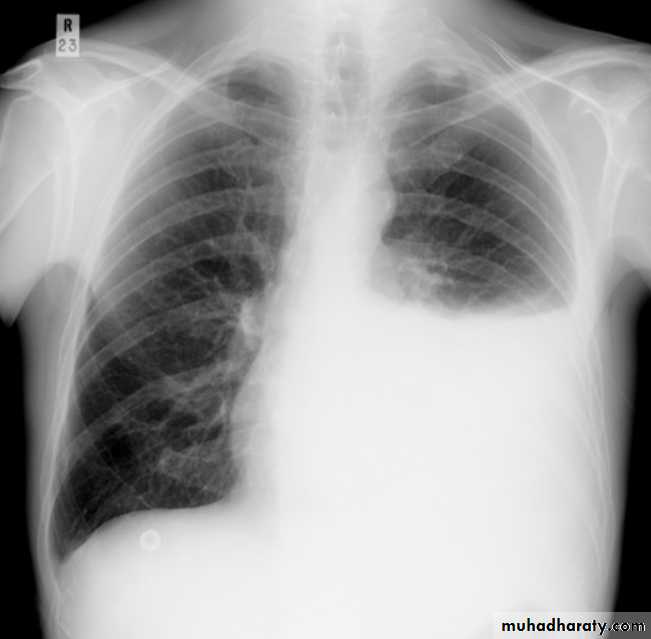
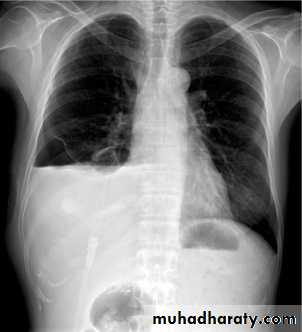
Pneumothorax
Pneumothorax refers to the presence of gas (air) in the pleural space. When this collection of gas is constantly enlarging with resulting compression of mediastinal structures it can be life-threatening and is known as a tension pneumothoraxIt is useful to divide pneumo thoraces into three categories :
primary spontaneous: no underlying lung disease marfan syndrum , Elher danus syndrome alpha-1 antitrypsin deficiency
secondary spontaneous: underlying lung disease is present
iatrogenic/traumatic
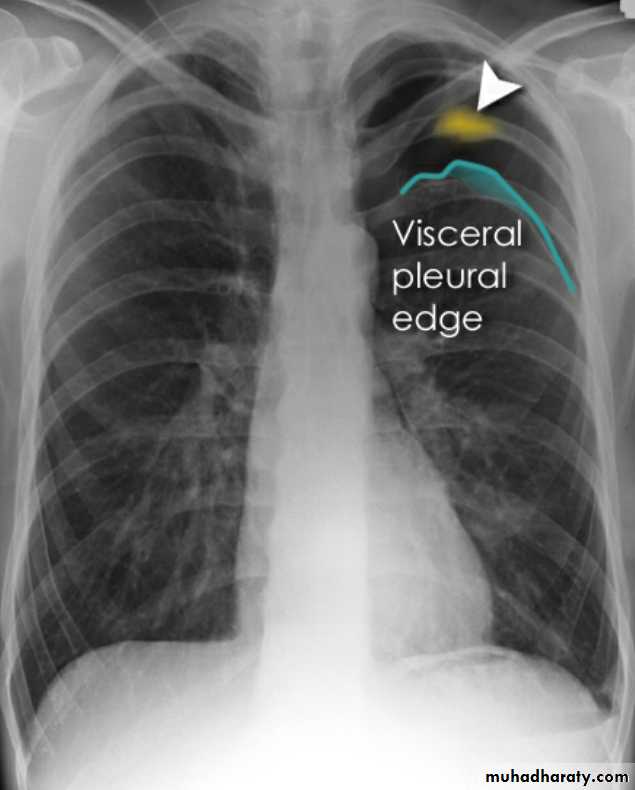
Radiographic features
Chest radiograph
A pneumothorax is, when looked for, usually relatively easily appreciated. Typically they demonstrate:
visible visceral pleural edge see as a very thin, sharp white line
no lung markings are seen peripheral to this line
the peripheral space is radiolucent compared to adjacent lung
the lung may completely collapse
the mediastinum should not shift away from the pneumothorax unless a tension pneumothorax is present

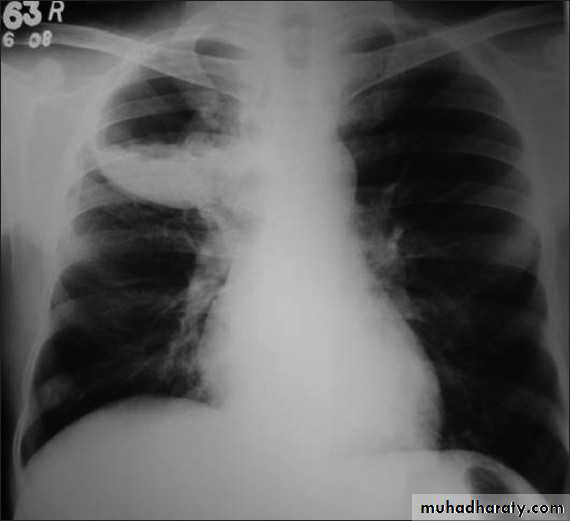
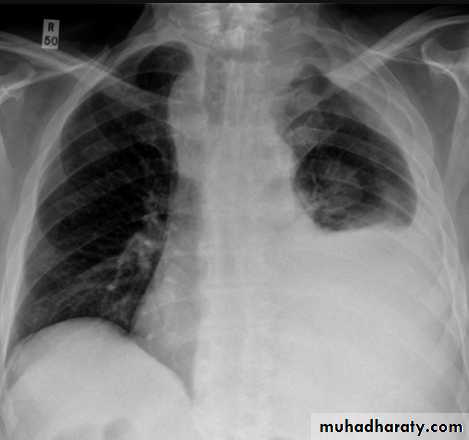
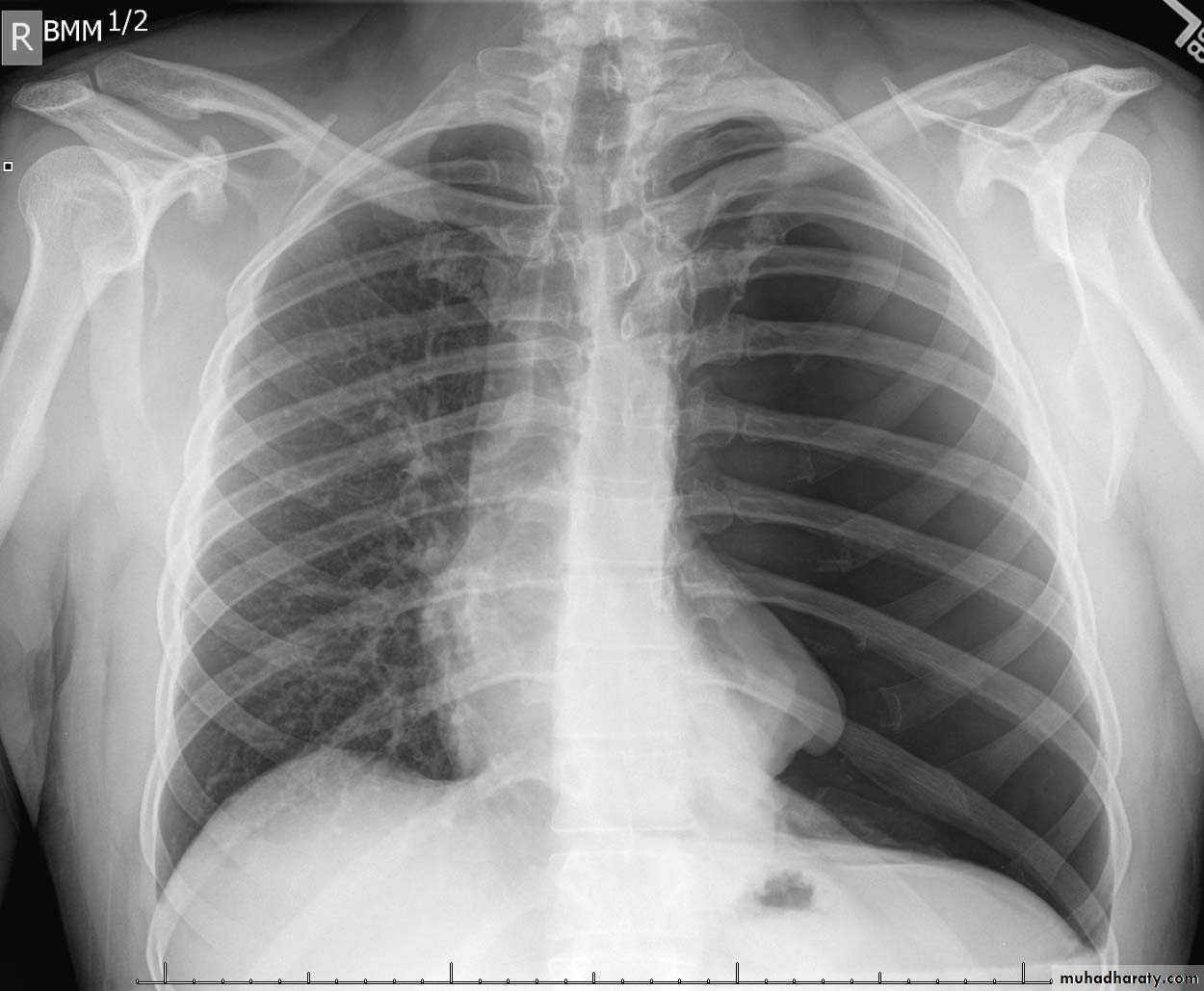
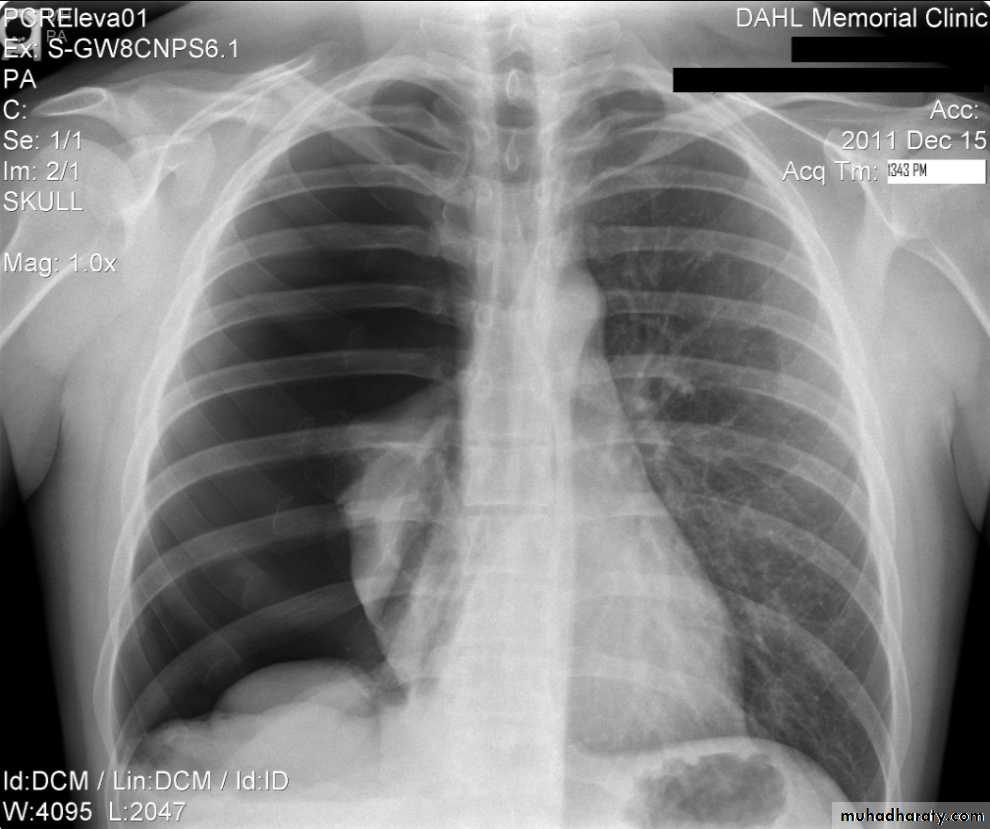
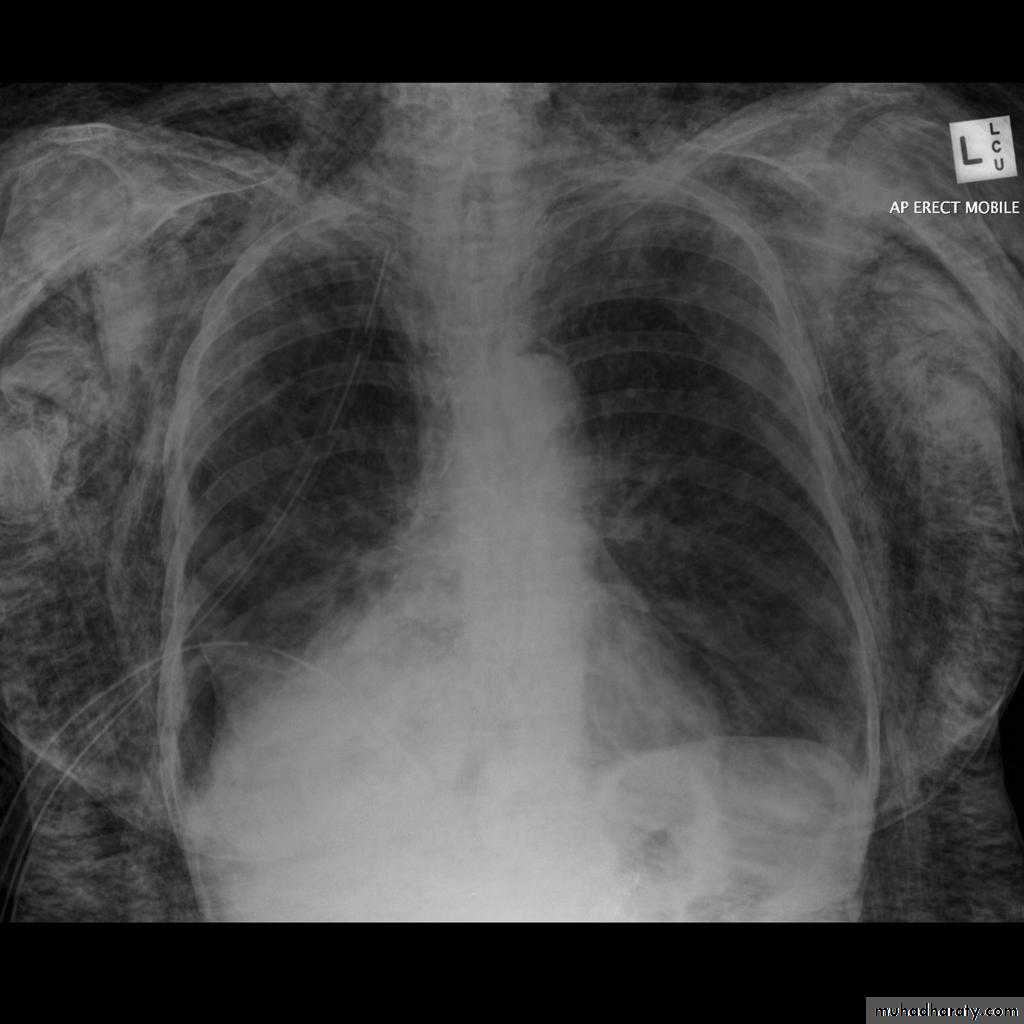
A tension pneumothorax
A tension pneumothorax occurs when intrapleural air accumulates progressively in such a way as to exert positive pressure on mediastinal and intrathoracic structures. It is a life threatening occurrence requiring rapid recognition and treatment is required if cardiorespiratory arrest is to be avoided.Radiographic features
A pneumothorax will have the same features as a run-of-the-mill pneumothorax with a number of additional features, helpful in identifying tension. These additional signs indicate over expansion of the hemithorax:
ipsilateral increased intercostal spaces
shift of the mediastinum to the contralateral side
depression of the hemidiaphragm
tension pneumothorax
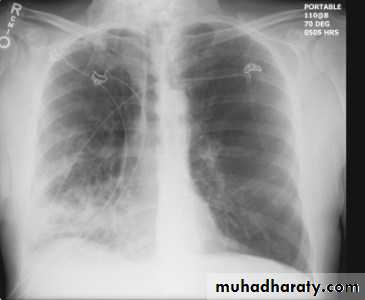
Hydro pnuemothorax
Hydropneumothorax is a term given to the concurrent presence of a pneumothorax as well as a hydrothorax (i.e. air and fluid) in the pleural space.Plain radiographs
On an erect chest radiograph, recognition of hydropneumothorax can be rather easy - and is clasically shown as an air-fluid level. On the supine radiograph, this may be more challenging where a sharp pleural line is bordered by increased opacity lateral to it within the pleural space may sometimes suggest towards the diagnosis 3,
Hydropnemothorax
Subcutaneous Emphysema
Subcutaneous emphysema, strictly speaking, refers to air in the subcutaneous tissues. But the term is generally used to describe any soft tissue emphysema of the body wall or limbs, since the air often dissects into the deeper soft tissue and musculature along fascial planes .Radiographic appearance
Plain film
If affecting the anterior chest wall, subcutaneous emphysema can outline the pectoralis major muscle, giving rise to the ginkgo leaf sign , dissecting air along tissue fat planes appears as multiple lines of lucency.
Subcutaneous Emphysema
Pneumomediastinum is the presence of extraluminal gas within the mediastinum. Gas may originate from the lungs, trachea, central bronchi, oesophagus, and track from the mediastinum to the neck or abdomen
Radiographic features
Small amounts of air appear as linear or curvilinear lucencies outlining mediastinal contours such as:
subcutaneous emphysema
air anterior to pericardium: pneumopericardium
air around pulmonary artery and main branches: ring around artery sign
air outlining major aortic branches: tubular artery sign
air outlining bronchial wall: double bronchial wall sign
continuous diaphragm sign: due to air trapped posterior to pericardium
air between parietal pleura and diaphragm: extrapleural sign

Chronic obstructive pulmonary disease (COPD)
represents a spectrum of obstructive airway diseases. It includes two key components which are chronic bronchitis-small airways disease and emphysemaChronic bronchitis (CB)
Chronic bronchitis (CB) is often defined as the presence of productive cough for 3 months in two successive years in a patient in whom other causes of chronic cough, such as tuberculosis, lung cancer and heart failure, have been excluded . It can be an important pathological compotent of chronic obstructive pulmonary disease . (often considered as a distinct phenotype of COPD)
findings of chronic bronchitis on chest radiography
are nonspecific and include 1.increased bronchovascular markings and2.cardiomegaly other added radiological signs
* direct signs
3.thickened peripheral airways - may only be seen in the proximal portion
*indirect signs - many of these features may be non specific on their own
1.air trapping
2.subsegmental atelectasis
3.Dirty lung appearance
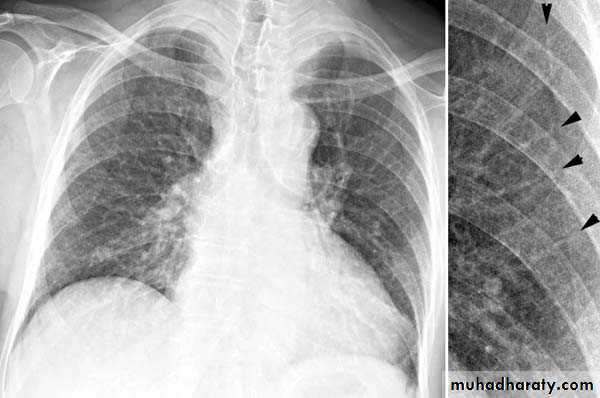
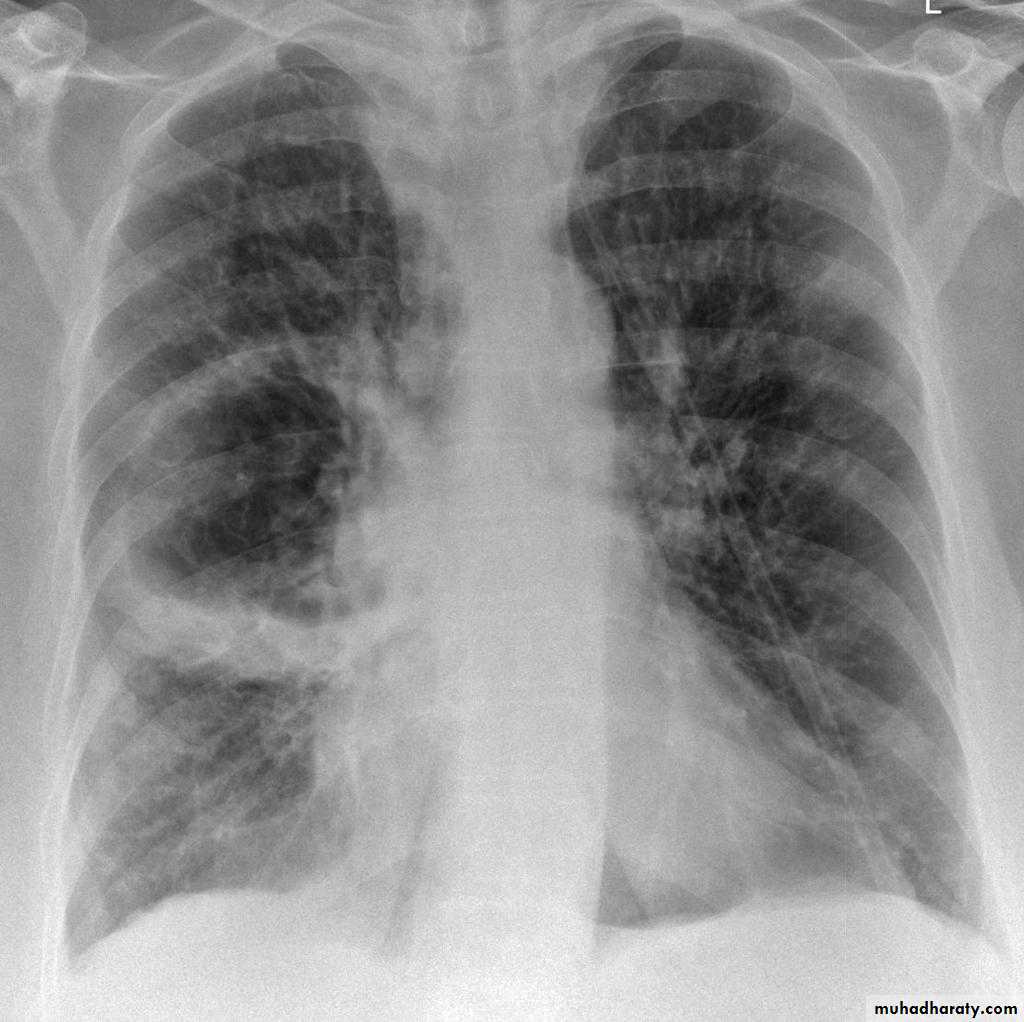
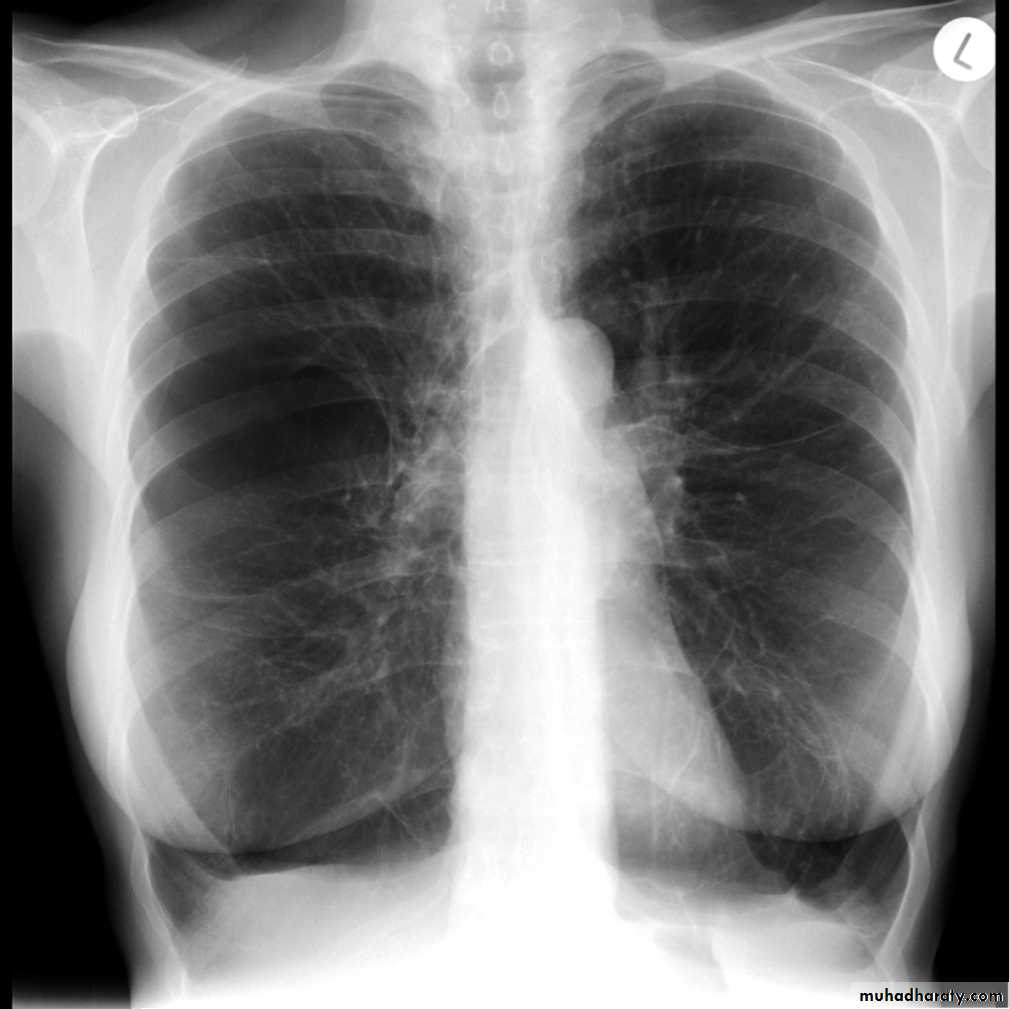
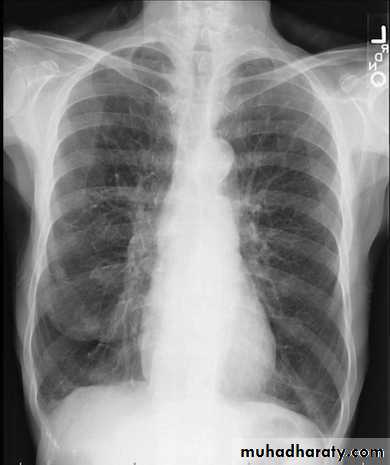
Pulmonary emphysema
Pulmonary emphysema is defined as the "abnormal permanent enlargement of the airspaces distal to the terminal bronchioles accompanied by destruction of the alveolar wall and without obvious fibrosis". Emphysema is one of the entities grouped together as chronic obstructive pulmonary diseaseRadiographic features
Plain film
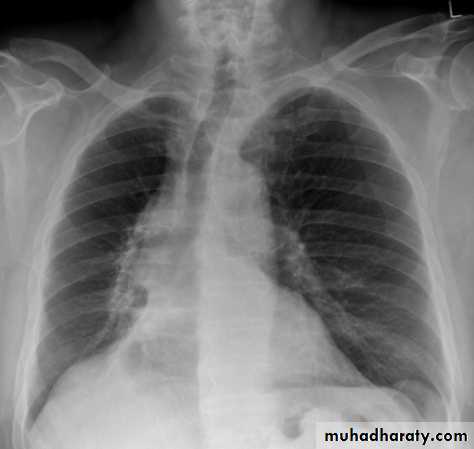
Except in the case of very advanced disease with bulla formation, chest radiography does not image emphysema directly, but rather infers the diagnosis due to associated features :
hyperinflation:
1.flattened hemidiaphragm(s): most reliable sign
2.ncreased and usually irregular radiolucency of the lungs
3.increased retrosternal airspace
4.increased antero-posterior diameter of chest
5.widely spaced ribs
6.sternal bowing
7.tenting of the diaphragm
8.saber-sheath trachea
9.vascular changes paucity of blood vessels ( absent pulmonary markings in outer 1/3 of the lung fields )
10 .pulmonary arterial hypertension
pruning of peripheral vessels
increased calibre of central arteries
right ventricular enlargement
Emphyzema
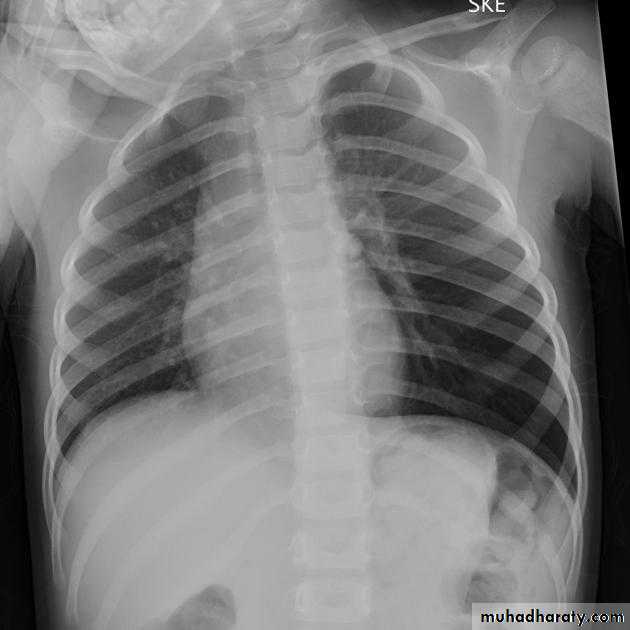
Unilateral obstructive emphysemaunilateral emphysema or atelectasis are the most common findings; only uncommonly will a radio-opaque foreign body be demonstrated ,Aspirated foreign bodies have a predominance for the right tracheo bronchial tree.

Pulmonary bullae are focal regions of emphysema with no discenible wall which measure more than 1cm in diameter
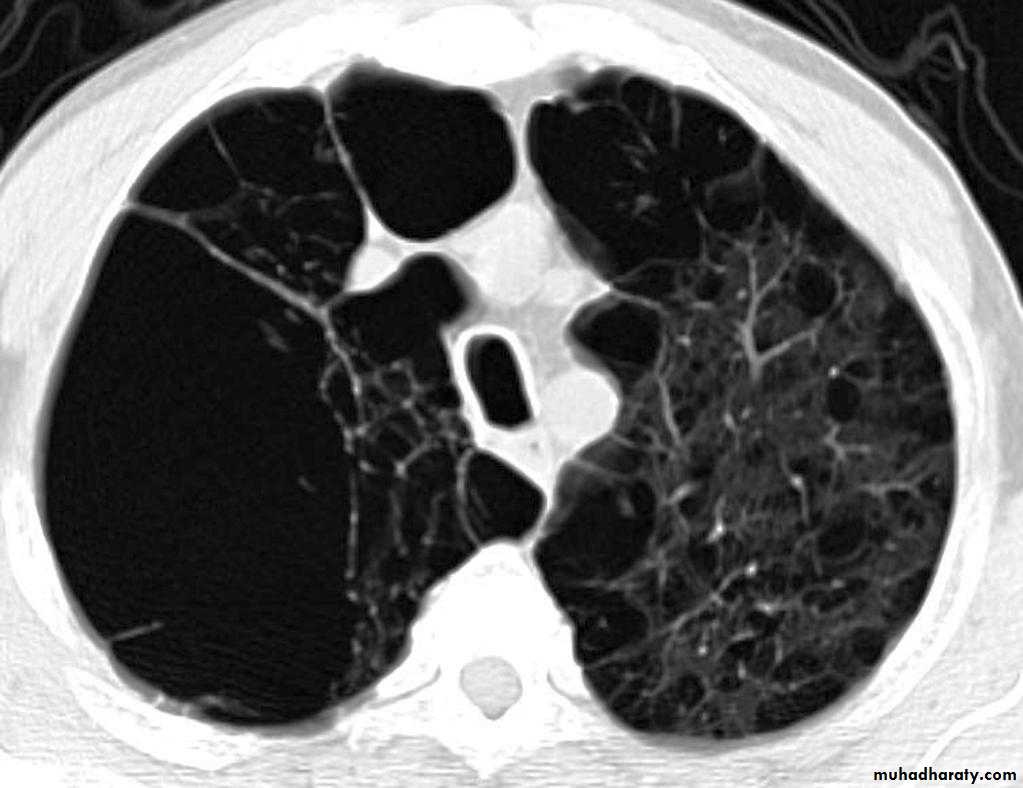
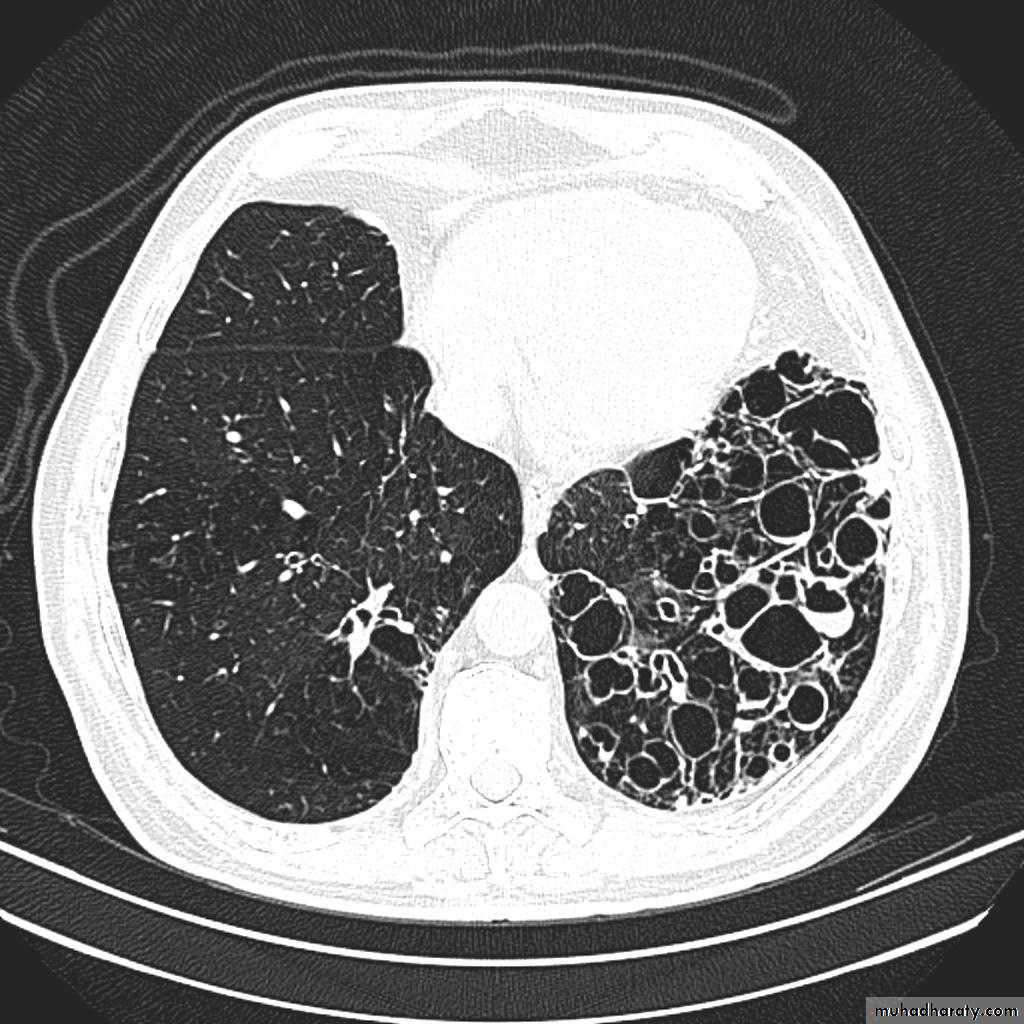
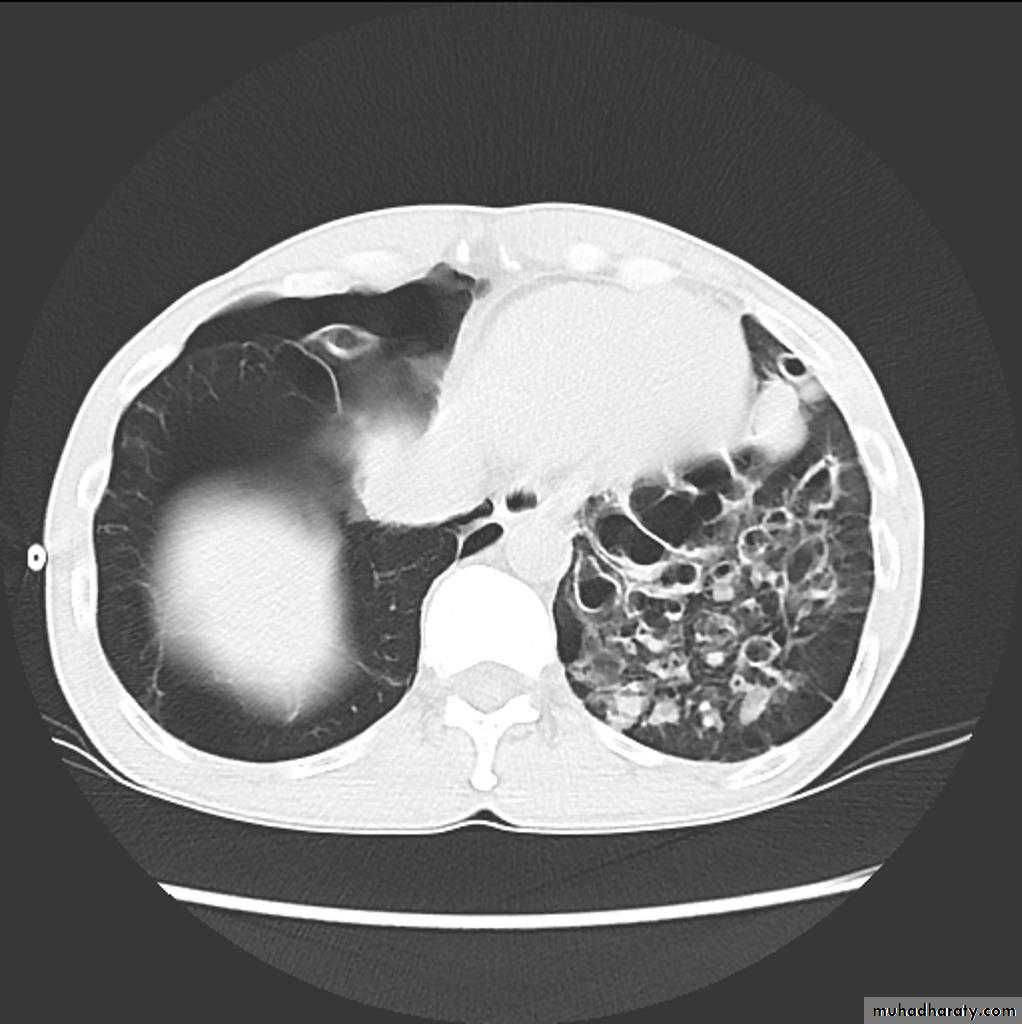
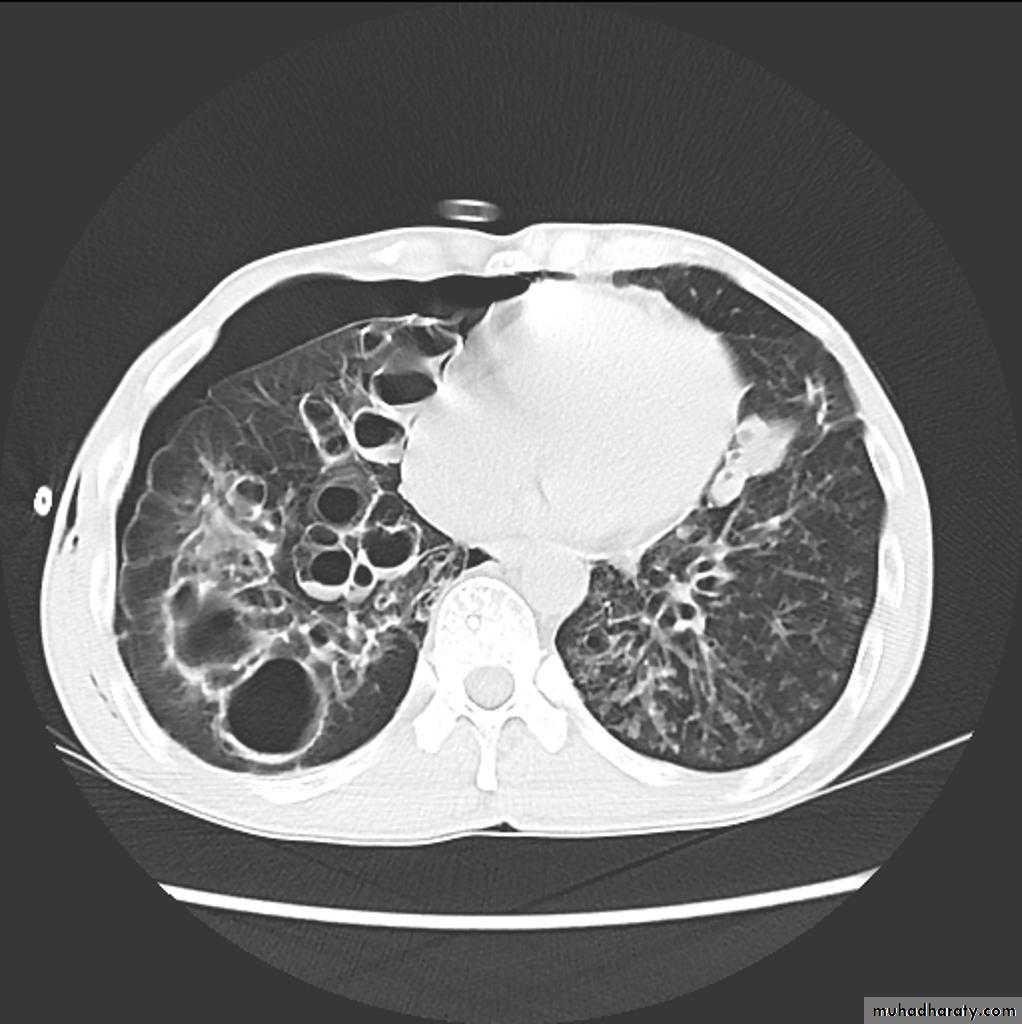
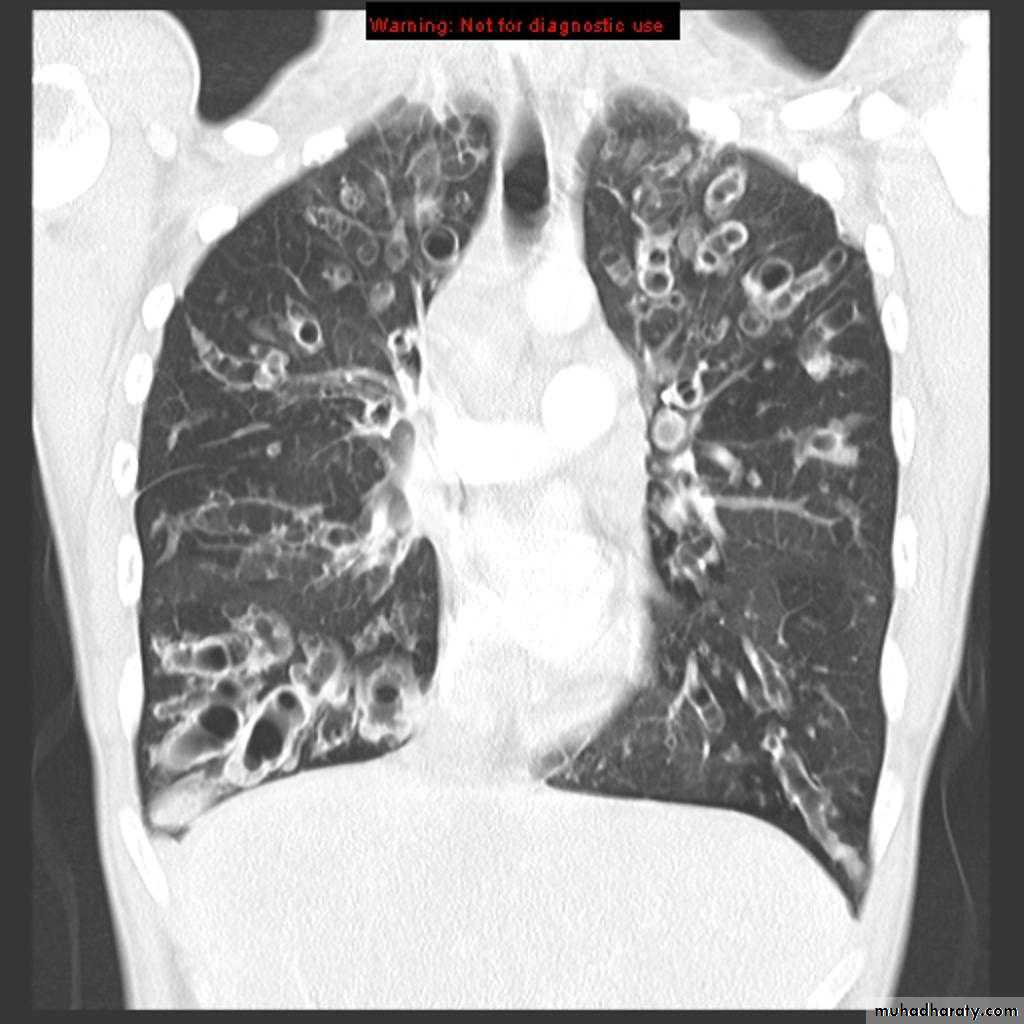
Bronchiactasis
Bronchiectasis refers to abnormal dilatation of the bronchial tree and is seen in a variety of clinical settings. CT is the most accurate modality for diagnosis. It is largely considered irreversibleCauses of bronchiactasias very important to consider
post-infective (most common)necrotising bacterial pneumonia, e.g Staph. aureus, Klebsiella, B. pertussis
granulomatous disease, e.g tuberculosis, MAIC, histoplasmosis
allergic bronchopulmonary aspergillosis (ABPA)
congenital
congenital cystic bronchiectasis
cystic fibrosis (CF)
ciliary dysfunction syndromes, e.g. Kartagener syndrome
bronchial obstruction
malignancy, e.g. bronchogenic carcinoma
inhaled foreign bodies
chronic aspiration lung changes
Plain radiograph
Chest x-rays are usually abnormal
1. Tram-track opacities are seen in cylindrical bronchiectasis, and
2. air-fluid levels may be seen in cystic bronchiectasis.
Honey comb shadow
3.Overall there appears to be an increase in bronchovascular markings, and bronchi seen end on may appear as ring shadows .
4.Pulmonary vasculature appears ill-defined, thought to represent peri bronchovascular fibrosis .



TB of the lung
Tuberculosis encompasses an enormously wide disease spectrum affecting multiple organs and body systems predominantly caused by the organism Mycobacterium tuberculosisPulmonary manifestations of tuberculosis are varied and depend in part whether the infection is primary or post-primary. The lungs are the most common site of primary infection by tuberculosis and are a major source of spread of the disease .
Have 2 categories
Primary
Post primary TB
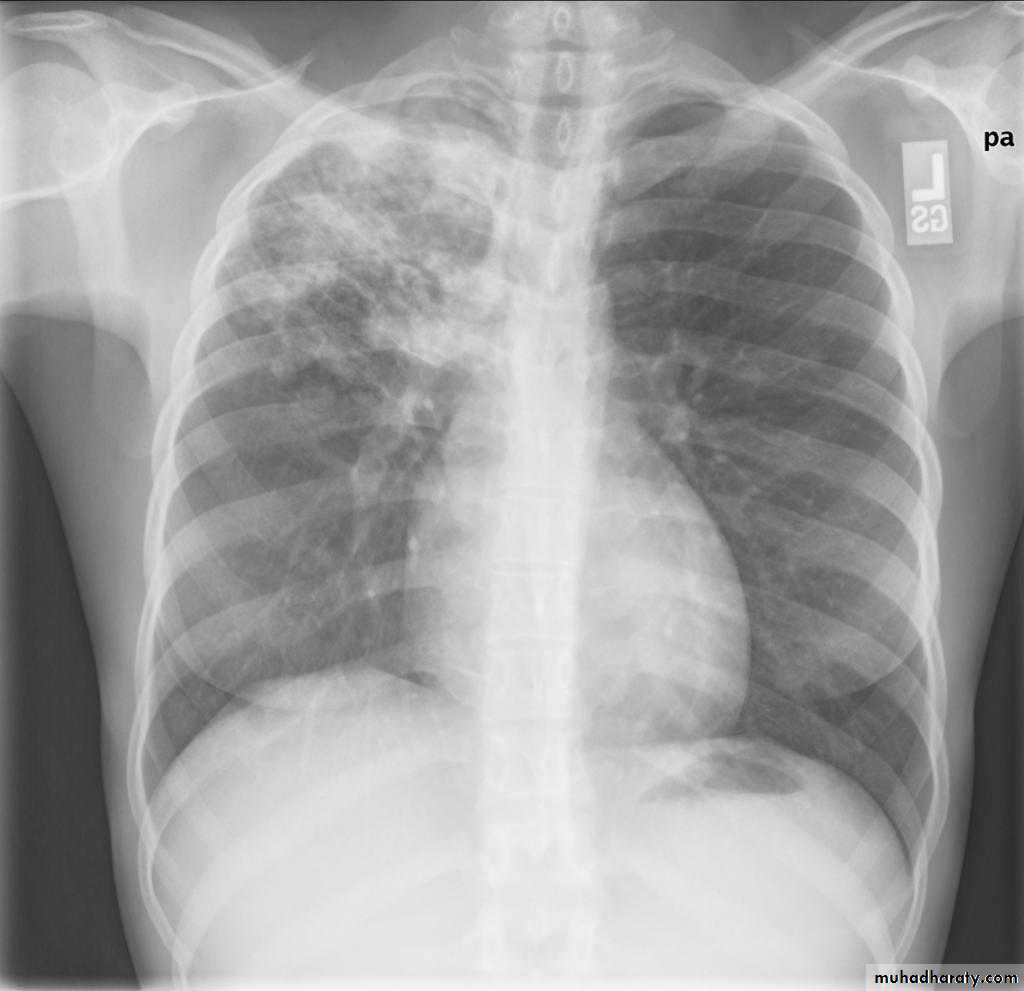
Primary pulmonary TB
Radiographic featuresprimary pulmonary tuberculosis
1.the initial focus of infection can be located anywhere within the lung and has non-specific appearances ranging from too small to be detectable, to patchy areas or consolidation or even lobar consolidation in RT upper or RT middle lobe . Radiographic evidence of parenchymal infection is seen in 70% of children and 90% of adults called Ghon lesion , +/- ipsilateral hilar or paratracheal Lymph adenopathy usually right sided
( Ghon focus + LAP ) called primary complex.
2.Later In most cases, the infection becomes localized and a caseating granuloma resolve eventually calcifies with or without calcification of the regional LN , Calcification of nodes is seen in 35% of cases . When a calcified node and a calcified Ghon lesion are present, the combination is known as a Ranke complex.
3. Pleural effusions are more frequent in adults .
Post primary TB radiographic appearance
Post-primary pulmonary tuberculosis, also known as reactivation tuberculosis or secondary tuberculosis occurs years later, frequently in the setting of a decreased immune status. In the majority of cases, post-primary TB within the lungs develops in either :
* posterior segments of the upper lobes
*superior segments of the lower lobes
Typical appearance of post-primary TB
1.patchy consolidation or poorly defined linear and nodular opacities in both apices , upper zone in one lung , & lower zone in other lung ( ulternating lesion ) .2. Post-primary infections are far more likely to cavitate with multiple abscess formation & air fluid level more develop in the posterior segments of the upper lobes.
3. Tuberculomas seen in post-primary TB and appear as a well defined rounded mass typically located in the upper lobes .
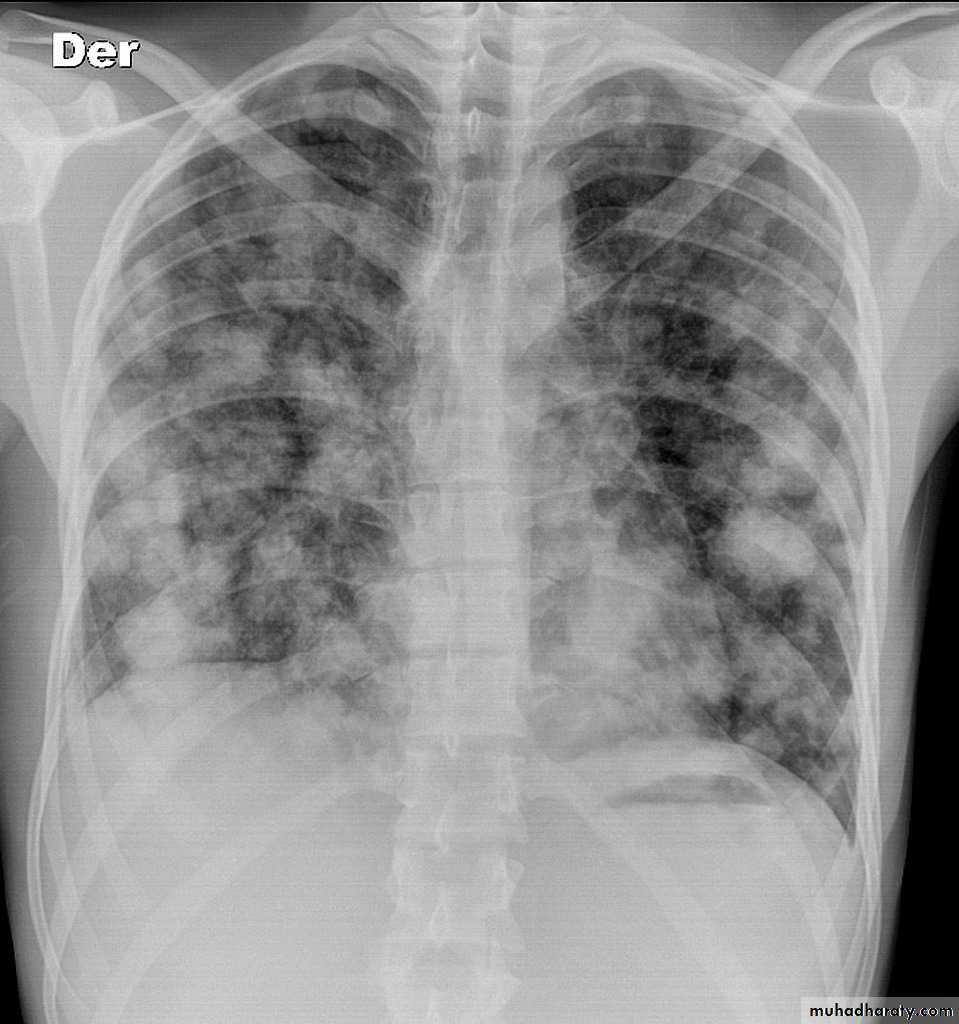
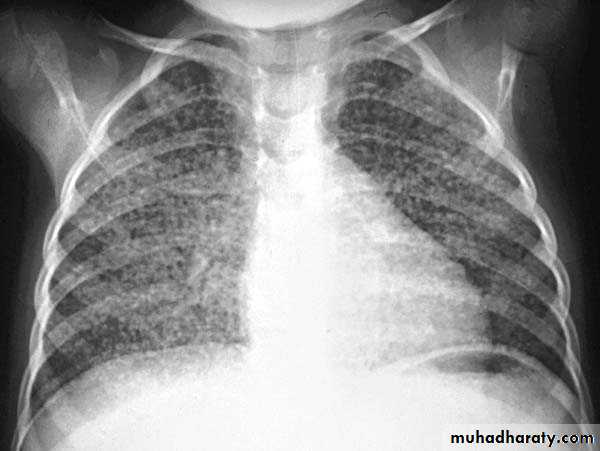
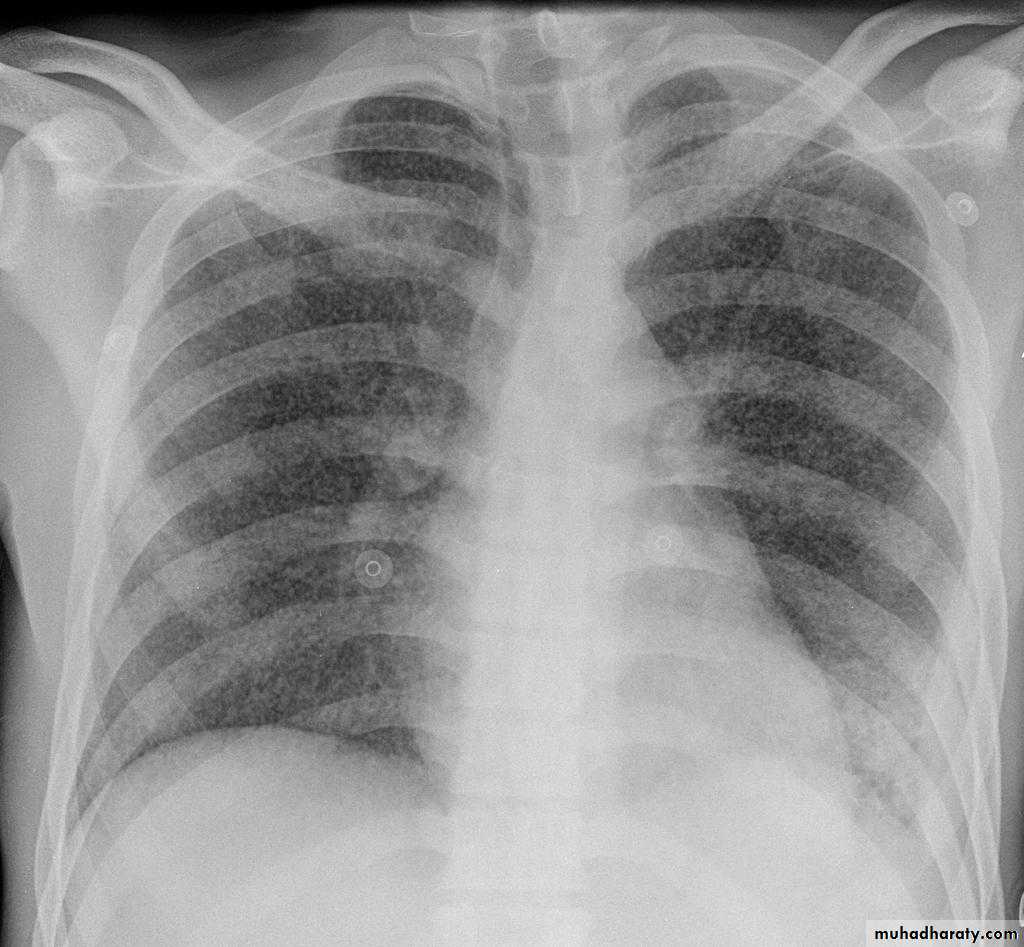
4. Miliary tuberculosis is uncommon but carries a poor prognosis. It represents haematogenous dissemination of an uncontrolled tuberculous infection. It is seen both in primary and post-primary tuberculosis. Although implants are seen throughout the body, the lungs are usually the easiest location to the image. Miliary deposits appear as 1-3 mm diameter nodules . are uniform in size and uniformly distributed

TB abscess
Complications
Recognized complications include:1.colonisation of cavities by fungus, e.g. aspergilloma
2.bronchiectasis
3.arterial pseudoaneurysms
bronchial artery pseudo aneurysm
pulmonary artery pseudo aneurysm / Rasmussen aneurysm
4.empyema
5.fibrothorax
6.bronchopleural fistula
Aspergiloma