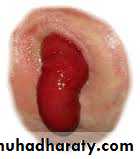
stoma
د.طارق العبيديAl-Madena copy
1
Colostomy: is an artificial opening made in to large bowel in order to divert feces and flatus to the exterior where they may be collected in an adhesive bag. It is classified in to temporary and permanent.
Al-Madena copy
2
Al-Madena copy
3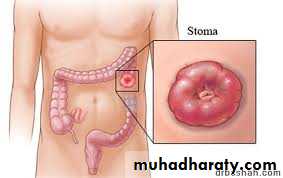
Al-Madena copy
4

Al-Madena copy
5Temporary colostomy: also called (defunctioning colostomy), this is most commonly established to relieve a distal obstruction of the sigmoid colon by carcinoma or diverticulitis. Other indications include vesico-colic fistula, protection of a low colorectal anastomosis after resection of the rectum,
Al-Madena copy
6

Al-Madena copy
7
Al-Madena copy
8

Al-Madena copy
9to prevent fecal peritonitis developing after traumatic injury to the colon or rectum, or top facilitate the operation of a high anal fistula.
Injury to colon should not be sutured immediately as small bowel , colostomy should be done for many reasons that the blood supply of large bowel is not abounding like small bowel,
Al-Madena copy
10
Heavy loaded with bacteria, containing solid material might threaten the suture line, but in special situation it can be sutured immediately in trauma to colon in following situations , if the injury to right side of colon, if the injury with in six hours,
Al-Madena copy
11
, if the peritoneum is not contaminated (not soiled ) with feces, if the patient is not present with shock, and if the injury is single not multiple (not associated with liver or spleen) and lastly if the injury is less than one cm in colon .
Al-Madena copy
12A temporary colostomy is made by bringing a loop of bowel to the surface of the skin called loop colostomy. When firm adhesion of colostomy to the abdominal wall has been taken after 7 days.
Al-Madena copy
13

Al-Madena copy
14A loop of colon can be most easily brought to the surface by using large bowel which has mesentery , most loop colostomy are made in the transverse colon and if the disease involve the left side of colon ,the right half of the transverse colon is preferred.
Al-Madena copy
15

Al-Madena copy
16
Al-Madena copy
17
Al-Madena copy
18
Al-Madena copy
19
Al-Madena copy
20
Al-Madena copy
21
Al-Madena copy
22Also the sigmoid colon is suitable for loop colostomy for the disease of the pelvic colon and rectum. After the distal obstruction is relieved ,colostomy is closed in 2 months.
Al-Madena copy
23
Double barreled colostomy: it designed to do absolute diversion of the content of colon to out side by making tow opening on the skin on called proximal colostomy and the other is called mucous fistula.
Al-Madena copy
24Al-Madena copy
25Hartmann colostomy: done by complete cut of the colon taking the proximal one to colostomy and the distal one is completely closed by suturing it and left in side the abdomen , this done in area of small mesentery to do loop colostomy.
Al-Madena copy
26
Al-Madena copy
27Permanent colostomy: this usually formed after excision of the rectum for carcinoma by abdomino-prineal resection. It is formed by bringing the distal end as end colostomy of the divided colon to the surface of the left iliac fossa where it is stitched in place immediately by sutures placed between the colonic margin and the surrounding skin.
Al-Madena copy
28
The point at which the colon is brought to the surface must be carefully selected to allow colostomy bag to be applied with out impinging on the bony prominence of the anterior superior iliac spine. The best site is usually 6cm above and medial to the bony prominence.
Al-Madena copy
29Colostomy bags and appliances: feces from colostomy are collected in disposable adhesive bags. A wide range of such bags is currently available. In large hospitals ,stomas therapists and stoma clinics Are being set up to offer advise to the patients on stoma care.
Al-Madena copy
30

Al-Madena copy
31
Al-Madena copy
32
Al-Madena copy
33
Al-Madena copy
34
Al-Madena copy
35
Al-Madena copy
36

Al-Madena copy
37Complications of colostomy(1)psychological trauma especially in the women and in the young age group due to bad smell and sounds of air which is uncontrolled so need a medical advise about the kinds of foods to prevent smell and sounds
Al-Madena copy
38
(2) prolapsed (3) retraction (4)necrosis of distal end. (5) stenosis of the orifice. (6) colostomy hernia. (7) bleeding from the margin. (8) colostomy diarrhea, this is infective enteritis respond to treatment. Colostomy with complication can be reformed by operation.
Al-Madena copy
39
Al-Madena copy
40
Al-Madena copy
41
Al-Madena copy
42
Al-Madena copy
43Caecostomy: in disparately ill patient with advanced large bowel obstruction, a caecostomy may be useful. In late cases of obstruction the cecum may become so distended ans ischemic that rupture of cecal wall may be distended.
Al-Madena copy
44
This can occur spontaneously, giving rise to fecal peritonitis, or at operation, when an incision in the abdominal wall reduces its supportive role and allows the cecum to expand.
Al-Madena copy
45
Direct suture to cecum is possible, resection of cecum by right hemicoloectomy in bad injury or performing of caecostomy, which is a temporary measure until the condition of the patient is improved then a definitive procedure then performed.
Al-Madena copy
46
Ileostomy: artificial opening in the ileum and can be temporary or more common permanent. The ileum should be brought through the lateral edge of rectus abndominis muscle.
Al-Madena copy
47
Al-Madena copy
48
Al-Madena copy
49
Care of ileostomy: during 1st few postoperative days the fluid electrolyte balance must be adjusted with great care. The fluid of ileostomy is irritant and contain pancreatic juice which cause severe skin inflammation.
Al-Madena copy
50
Al-Madena copy
51Indication: in case of total colectomy as in ulcerative colitis, rest of inflammatory process in ulcerative colitis and diverticulitis in fulminant phase as temporary ileostomy, in traumatic injury to the bowel.
Al-Madena copy
52Closure of colostomy: in temporary colostomy closure should be done in 2 moths of previous operation provided that there is no distal obstruction and distal anastomosis is healed.
Al-Madena copy
53
The patient should be admitted to the hospital 5 days before closure with encouraging fluid diet and use laxatives drug and antibiotics in form 3rd generation cephalosporin and metronidazole and this called chemical preparation and the use of frequent enemas to clean the distal bowel called mechanical preparation.
Al-Madena copy
54
Mannitol solution can be used with caution in fear of dehydration. Ba- enema should be done before operation to ensure there is no distal obstruction.
Al-Madena copy
55
In summary
May be colostomy or ileostomyMay be temporary or permanent
Temporary or defunctioning stomas as loop stoma
An ileostomy is spouted , a colostomy is flushed
Ileostomy effluent is usually liquid where colostomy is usually solid
An ileostomy patients more likely to develop electrolyte problems
Al-Madena copy
56An ileostomy is usually sited in right iliac fossa while a temporary colostomy may be transverse colostomy sited in right upper quadrant
End colostomy is usually sited in left iliac fossa
All patients should be counselled by a stomas care nurses before operation
Complications include skin irritation, prolapse, retraction, necrosis, parastomal hernia, bleeding and fistulation.
Al-Madena copy
57