
1
Fifth stage
Gynecology
Lec. 1
.د
سراب
2/1/2017
Dysmenorrhoea
Is defined as painful menstruation and it is very common complaint.
Dysmenorrhoea can be classified as:
1. primary Dysmenorrhoea (primary spasmodic) (is the commoner type).
2. Secondary Dysmenorrhoea (congestive, acquired).
Primary dysmenorrhea
Presence of painful menstruation where there is no underlying pathology.
The prevalence of dysmenorrhoea is high. 72% of women reported dysmenorrhoea in their
life.
Aetiology
There are a number of factors that may have an aetiological role.
1. Endocrine:
Ovulatory cycle are necessary for development of primary dysmenorrhoea.
2. Abnormal uterine activity
Primary dysmenorrhoea is associated with uterine hypercontractility and a high resting
tone between contractions which may be mediated by increased
Prostaglandin levels or vasopressin.
3. Psychological:
It is unlikely but it may influence individual perception to painful stimuli.
Diagnosis
Diagnosis is usually based on history and normal findings on clinical examination.

2
History
It is usually occurs in girls or young women. It appears 6–12 months after the
menarche when ovulatory cycles begin to become established (The early cycles after
the menarche are usually anovular and tend to be painless).
The pain usually begins just prior to, or on the first day of the period. It lasts for several
hours or continuo throughout the first and second day.
It is usually described as a colicky (spasmodic, crampy) lower abdominal pain and
intense in suprapubic region associated with backache radiated to lower limb and
there may be associated gastrointestinal disturbances such as diarrhoea and vomiting
and other symptoms such as nausea, fatigue, and headache. Severe pain occur in small
number of women and leads to absence from work or education.
If symptoms are typical of primary dysmenorrhoea, a therapeutic trial may be
embarked on before considering any examination and investigation especially in
adolescents.
Examination
General examination : no abnormal finding.
Abdominal examination: no abnormal finding
pelvic examination in married patient : no abnormal finding.
Investigation
Investigation requested in these condition:
1. When clinical evaluation raises strong suspicion of underlying pathology.
2. When symptoms of primary dysmenorrhoea are not alleviated by combined oral
contraceptive pills and / or NSAID therapy.
Investigation by ultrasound examination or magnetic resonance imaging (MRI) or
laparoscopy or hysteroscopy according to history and differential diagnosis as no need
to do all investigation in most of cases.
Treatment
A. Reassurance and explanation.
B. Using heating pads or taking a warm bath may help to decrease pain.

3
C. Medical treatment:
1. Ant prostaglandins (NSAIDs): non-steroidal anti-inflammatory drugs
Acts via their suppression of menstrual fluid prostaglandins.
NSAIDs drugs such as ibuprofen (400mg every 6hours), mefenamic acid (500 mg every 8
hours), naproxen 250mg every 6 hours), and aspirin are all effective. Ibuprofen is the
preferred analgesic because of its favorable efficacy and safety profiles.
They are usually taken during the first few days of menstruation. The advantage of
starting treatment at the onset of menstruation is that it prevents the patient treating
herself when she is unknowingly pregnant which would only become apparent when a
period is missed.
2. THE COMBINED ORAL CONTRACEPTIVE PILL:
It is given especially when fertility control (contraception) is required.
They are thought to act by inhibiting ovulation and decreasing endometrial
production of prostaglandins and leukotrienes by inducing endometrial atrophy and
therefore reducing the amount of endometrial tissue available to produce these
mediators. Extended cycle use minimize the number of withdrawal bleeding
episodes.
Extended cycle oral contraceptive (Seasonale) is a 91-day oral contraceptive. Tablets
containing the active hormones are taken for 12 weeks (84 days), followed by 1 week
(7 days) of placebo tablets. it is particularly useful for women who experience
symptoms associated with the withdrawal bleed such as severe dysmenorrhoea.
3. Combination of both NSAIDs and Combined oral contraceptive pill.
4. Progestins:
a. Medicated intrauterine device (levonorgestrel intrauterine system (LNG-IUS)
(Mirena)): effective treatment for women who have a contraindication to either
NSAIDs or the combined oral contraceptive.
b. Medroxy progesterone acetate Depot (Depo-Provera) 150 mg Intra-Muscular (I.m.)
every 12 weeks.
Clinically they are effective since they render most women amenorrhoeic.
c. Desogestrel:
new progestogen only contraceptive pills. It effectively inhibit ovulation and relieve
symptoms of dysmenorrhoea.

4
5. Other drugs under evaluation or clinical trial studies used are:
a. vasopressin receptor antagonist:
b. Tocolytics agent: can reduce uterine contractility and thus are potentially effective.
These are:
a. Beta-adrenergic agonists
b. calcium channel blockers
c. Transdermal glyceryl trinitrate has also been evaluated
d. vitamin E
e. omega-3 polyunsaturated fatty acids beneficial in the management of
dysmenorrhoea in adolescents.
D. Other measures:
Psychotherapy.
Hypnotherapy.
Transcutanous nerve stimulation (acupuncture).
E. Surgery:
It may provide long term relief and used rarely in patients resistant to drug therapy.
ablation of uterine nerve.
presacral neurectomy.
Secondary dysmeonrrhoea
Presence of painful menstruation in the presence of an identifiable pathologic cause .
It is usually due to one of following:
1. Endometriosis.
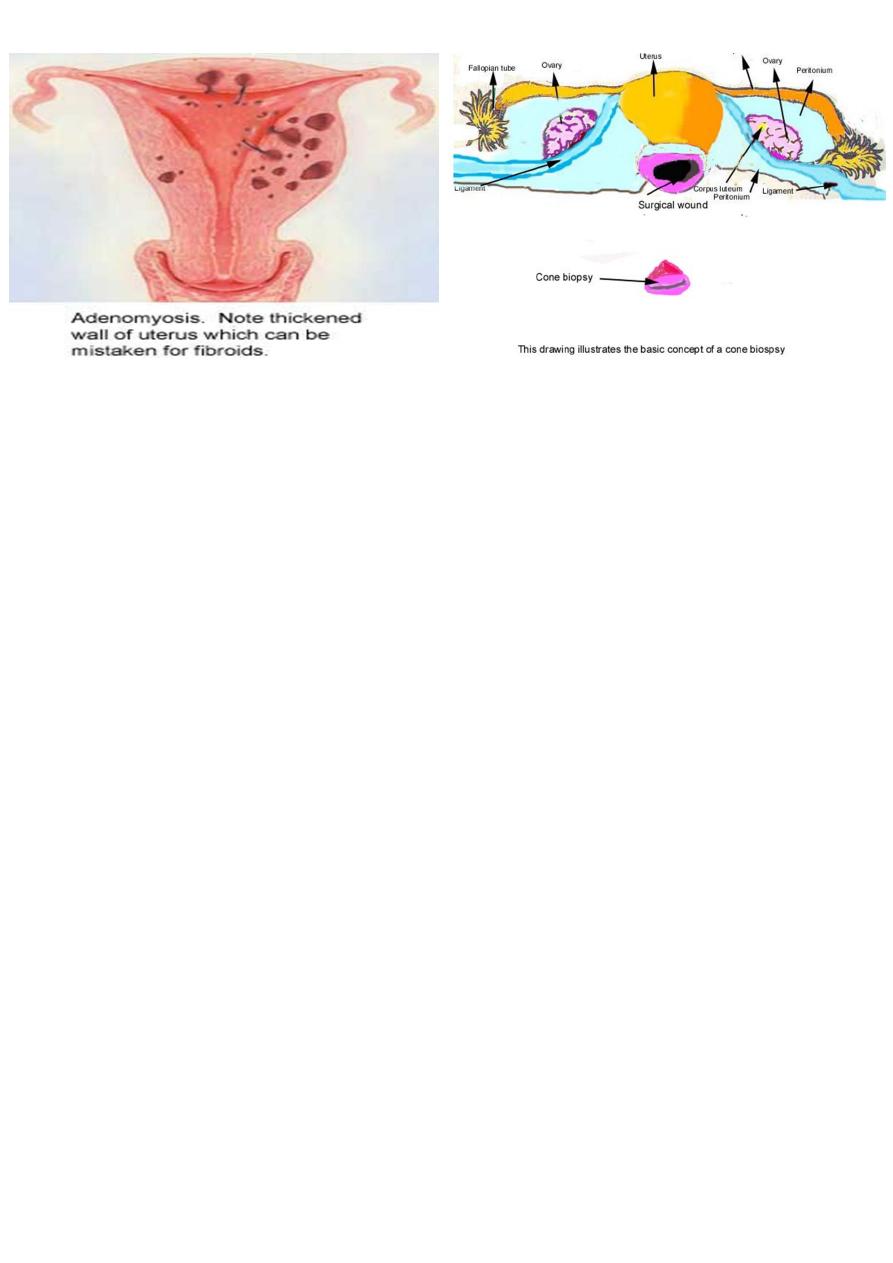
2. Adenomyosis.
3. Pelvic inflammatory disease (PID).
4. Asherman's syndrome (intrauterine adhesions).
5. Cervical stenosis (may result from conization).
6. Acquired fixed retroversion of uterus.
7. Uterine fibroids.
5
Management
It is easily diagnosed from history.
History
Secondary dysmenorrhoea is easily diagnosed from history.
It develops in older women (in their 30s or 40s). it may appear after some years of
painless menstruation.
The pain is often more severe prior to menstruation. The pain begins a few days prior
to menstruation and continuo throughout the period and even after the menses. It is
less related to the first day of flow. The pain is often a dull ache felt in lower
abdomen and back and sometimes extending to the thighs.
It is usually associated with dysparunia, infertility, abnormal uterine bleeding.
Clinical examination may not determine cause.
Investigations
May help to identify cause and choosing it according to case:
*Pelvic ultrasound show ovarian endometriosis and fixity of ovaries in PID.
*Hysterosalpingogram useful to identify intrauterine adhesion.
*Microbilogical cultures:
From endocervix, peritoneal fluid if PID is suspected.
*Laproscop

6
Treatment
Treatment of underlying cause (discussed in other lectures).
Treatment used of primary dysmenorrhoea are often helpful.
In patient with intractable dysmenorrhea, hysterectomy with bilateral
Oophorectomy may be needed.