
١
Fifth stage
Gynecology
Lec-
د
.
أ
ﺣ
ﻣ
د
ﺟ
ﺎ
ﺳ
م
19/12/2016
Premenstrual syndrome (PMS)
• the cyclical presence of somatic, psychological and emotional symptoms that worsen
as menses approaches and are ameliorated by the onset of menstrual flow.
• There is extreme in premenstrual syndrome. Premenstrual symptoms occur in most
women. 5–10% women have minimal or no symptoms while 5–10% have extreme
symptoms that there is a major impact on woman's life.
Aetiology
• There are many theories.
• *the hypothesis that ovarian steroids have a role in the pathophysiology of the
syndrome is obvious. As Women have no PMS before puberty, during pregnancy or
after the menopause and during suppression of the ovarian endocrine cycle with
danazol, GnRH analogues or by bilateral oophorectomy.
• *Relationship between variations in level of ovarian sex steroids and changes in
serotonin levels within the central nervous system.
• *Genetic, environmental, and psychological are important factors in mood disorders
as well as hormonal influence.
Symptoms
A wide range of symptoms has been described (more than 150-200 different
symptoms have been linked to PMS. but it is their timing and severity that are
most important, more so than the specific character.
The most common symptoms of PMS are:
Bloating.
Cyclic weight gain.
Mastalgia.
Abdominal cramps.
Fatigue.
Headache.
Depression.
Irritability.
٢
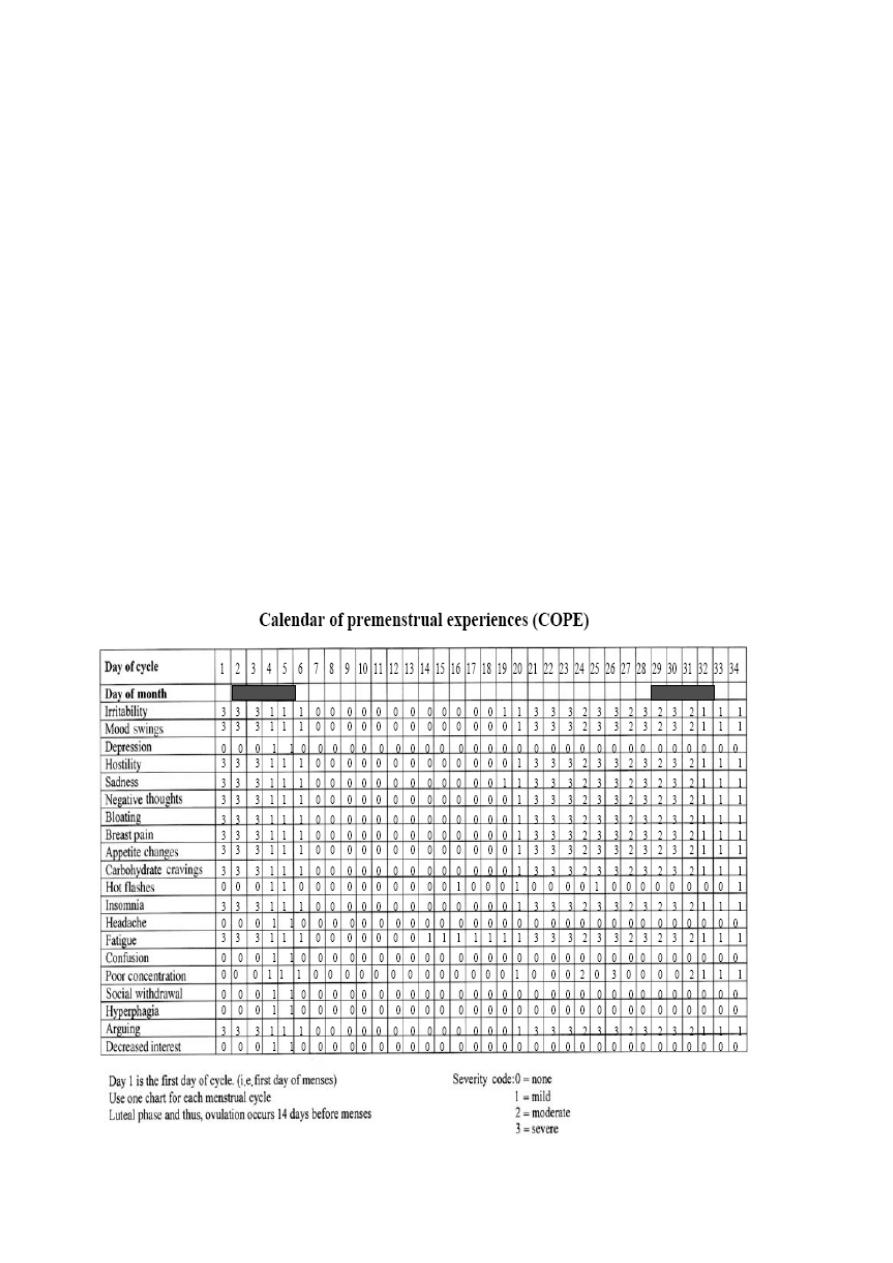
Diagnosis
• PMS is clinical diagnosis. In order to confirm the diagnosis there are a number of
criteria need to be met which are:
• 1. Symptoms are cyclic and occur during the luteal phase.
• 2. Symptoms increase in severity as the cycle progress.
• 3. Symptoms are relieved with the onset of menses and are absent by day
three (3) of flow.
• In order to confirm the diagnosis there are a number of criteria need to be
met which are :
• 4. There must be present for at least three consecutive cycles.
• 5. Symptoms should be of a severity to interfere with daily ac vi es.
• There are no objective tests (physical, biochemical or endocrine) to assist
in making the diagnosis.
• Prospectively completed specific symptom charts are required.

٣
GnRH analogue test
• The use of GnRH analogue test may be of benefit in clarifying the diagnosis
but it has never been proven scientifically as a true test. GnRH analogue
given for the purposes of removing the ovarian cycle to determine which
of a patient’s symptoms are clearly decreased.
Treatment
• A.Non–medical therapies
• Exercise and cognitive behavioural therapy may be of benifit. Other
treatment has not improved yet.
• B.Medical therapies
• a. Suppression of ovulation using:
• Combined oral contraceptive pills.
• Danazol.
• GnRH analogues.
• b. Selec ve serotonin reuptake inhibitors such as fluoxe ne 20 mg daily.
• C.Intrauterine progestagen (as levonorgestrel IUS):
• avoids re-stimulation of premenstrual syndrome at the same time that it
protects the endometrium; it reduces periods and provides contraception
Surgical treatment:
• hysterectomy with oopherectomy considered as the last option in those
woman who is refractory to pharmacological treatment.
• It is too invasive though is the only effective cure for premenstrual
syndrome.
• it can be followed by oestrogen replacement therapy without cyclical
progestagens.