
1
Fifth stage
Surgery
Lec-1
Dr.Bassam
Alabbasi
26/2/2017
Rerespiratory distress in neonate
Differrential diagnosis
surgical aspect
A. Air way obstruction
1. Nose Bilateral coanal Atresia
2. Pharynx a. Nasopharyngeal mass
b.pierre Robin syndrome
c. Base of tongue mass
3. Larynx a. Laryngomalacia
b. webs , Atresia
c.Neoplasm
4. Tracheobronchial tree
a. Tracheomalacia
b. Esophageal Atresia & TEF
c. Forgut cyst
d. Pulmonary sequestration
B- Compression of lung tissue by air , fluid and blood .
C- Anatomic Defect in the Diaphragm .
-congenital diaphragmatic hernia.
D. Intrinsic pulmonary Lesions.
* Congenital lung cysts
* Congenital lobar emphysema
* pulmonary Sequestration
* Agenesis , or lung hypoplasia
* cystic Adenomatoid malformation of the lung
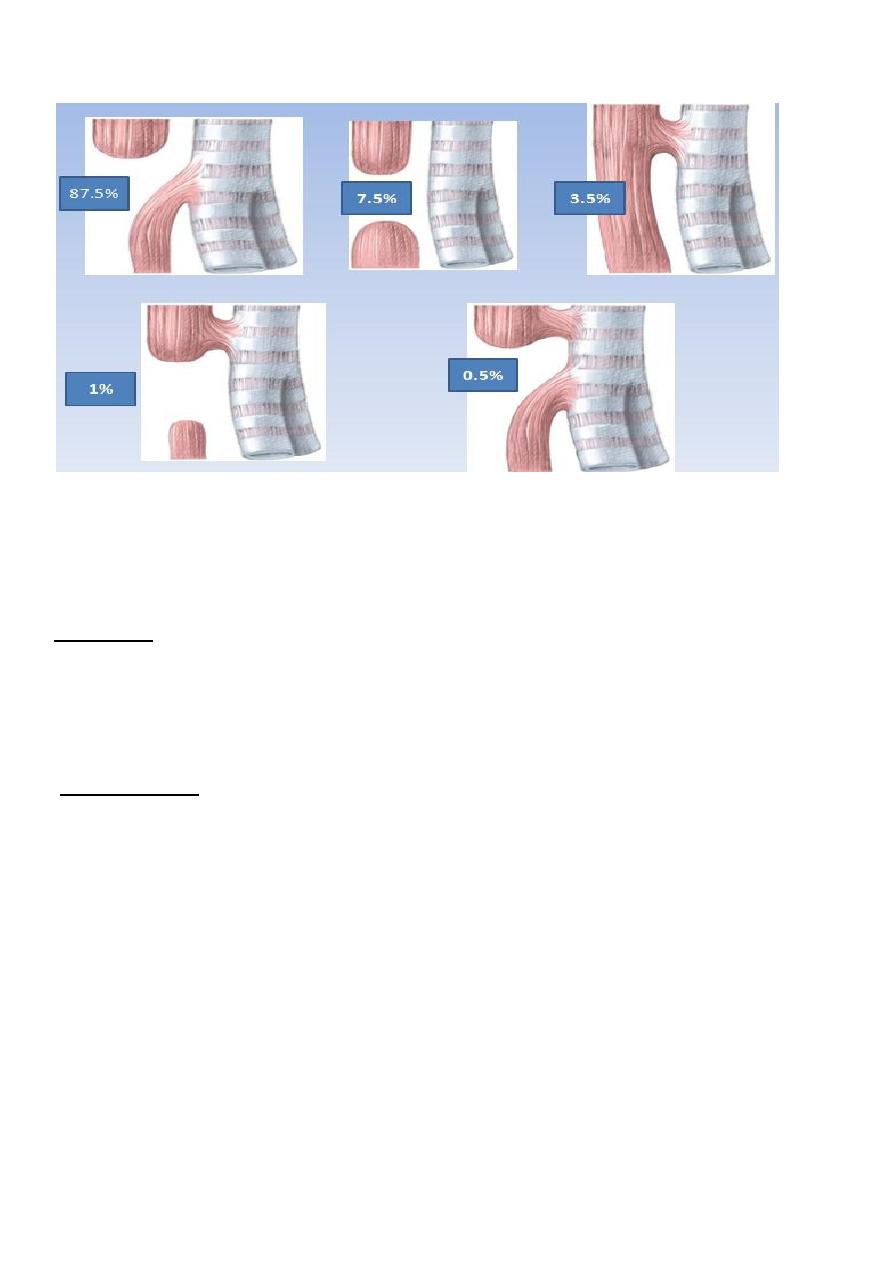
Esophageal atresia and tracheoesophageal fistula
-complet interruption of the esophagus
-blind upper esophageal pouch &lower sigment that usually communicates with trachea
2
Classification
Pathophysiology
-saliva (or milk) accumulate in the blind pouch &spill over the trachea choking and cyanosis.
-gastric content aspirate through distal fistula Atelactasis and pneumonia(chemical pneumonitis)
-abdominal distention (gastric)splint diaphragm inadequit ventilation
Diagnosis
-Antinatally: ultrasonography show:
1-polyhydramnios.
2-small stomach.
3-abnormal esophageal contractions.
-Early diagnosis postnatally very important and confirmed by failure of orogastric tube to
pass to stomach.
-signs &symtoms:
1-excessive droling.
2-respiratory distress.
3-frothy white bubbles from nose an mouth(excessive salivation.
4-chocking at feeding causing aspiration pneumonitis.
Associated anomalies
1-Cardiac .
2- gasrointestinal(Anorectal).
3-Vertebral\skeletal(Limb).
4-Renal.
5-chromosomal (usualy trisomy 18 &21)
6-sometimes all are present together and called V A C T E R L

3
Investigations
1-x-ray of the cheast &abdomen provides informations about the followings:
a-coiling of NGT and level of obstruction.
b-prescence of air in the stomach which indicates fistula.
c- states of the lungs.
d-vertebral &ribs anomalies.
e- evidence of right aortic arche.
2-Echocardiography:to identify the type of associated congenital heart disease &aright
aortic arche
3- renal ultrasonography:to assess renal anomalies spcialy bilateral renal agenesis.
Treatment
-
pre operative:
1-frequent oral suction to keep the upper pouch empty and prevent aspiration
2-incubator to avoid heat loss.
3-intravenous fluid &antibiotics .
4- vitamin K .(1 mg I M).
5-Time of surgery : within 12 hrs of admission to hospital.
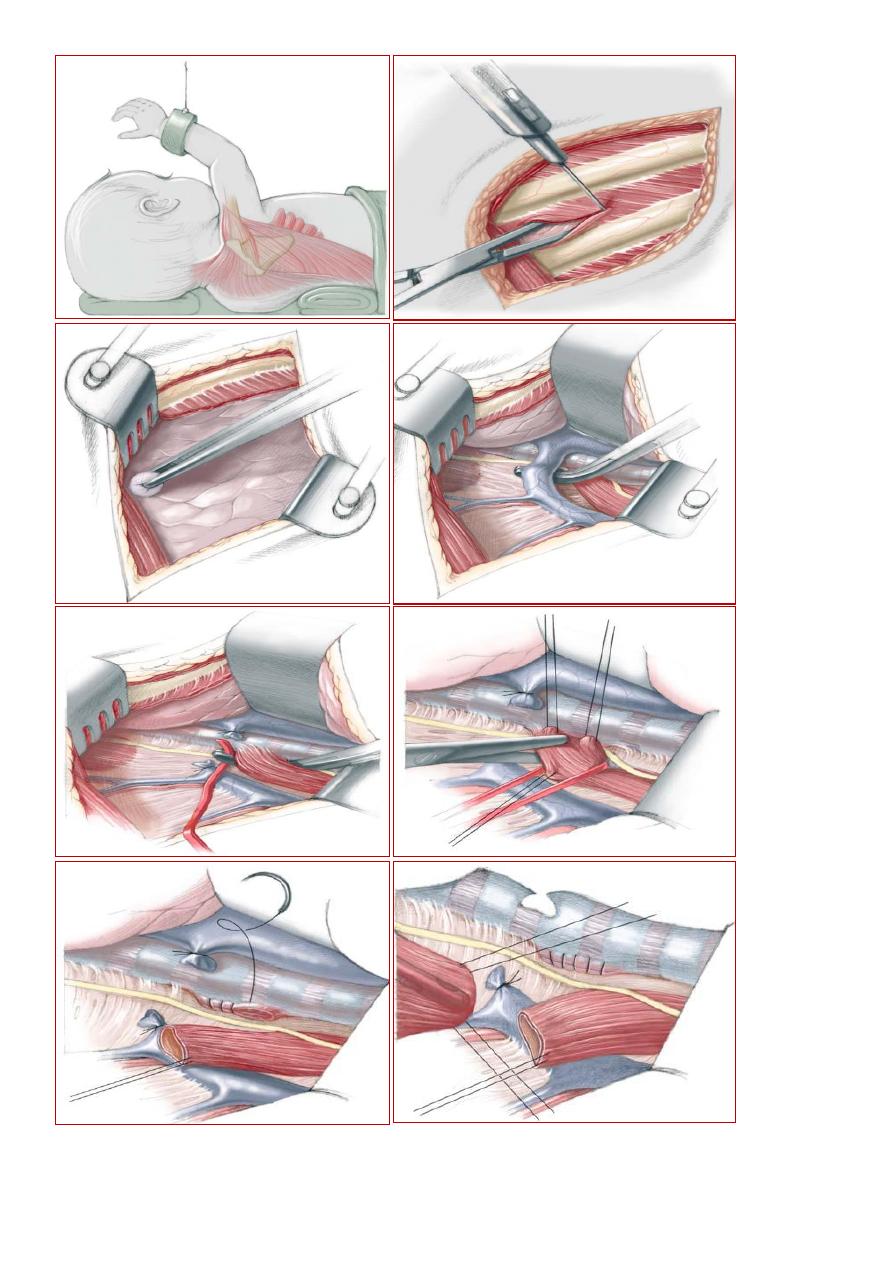
6- Surgery :
-right posterolateral extrapleural thoracotomy.
-azygous vein ligated.
-fistula identified and closed .
-upper blind pouch identified with end to end anastomosis
over a NGT and chest drain.
-sometimes ventilator is used specially in diseased lung.
-oral feeding can be commenced 3 to 4 days post operativly.
-sometimes thoracoscopic repair can be done.
4
5
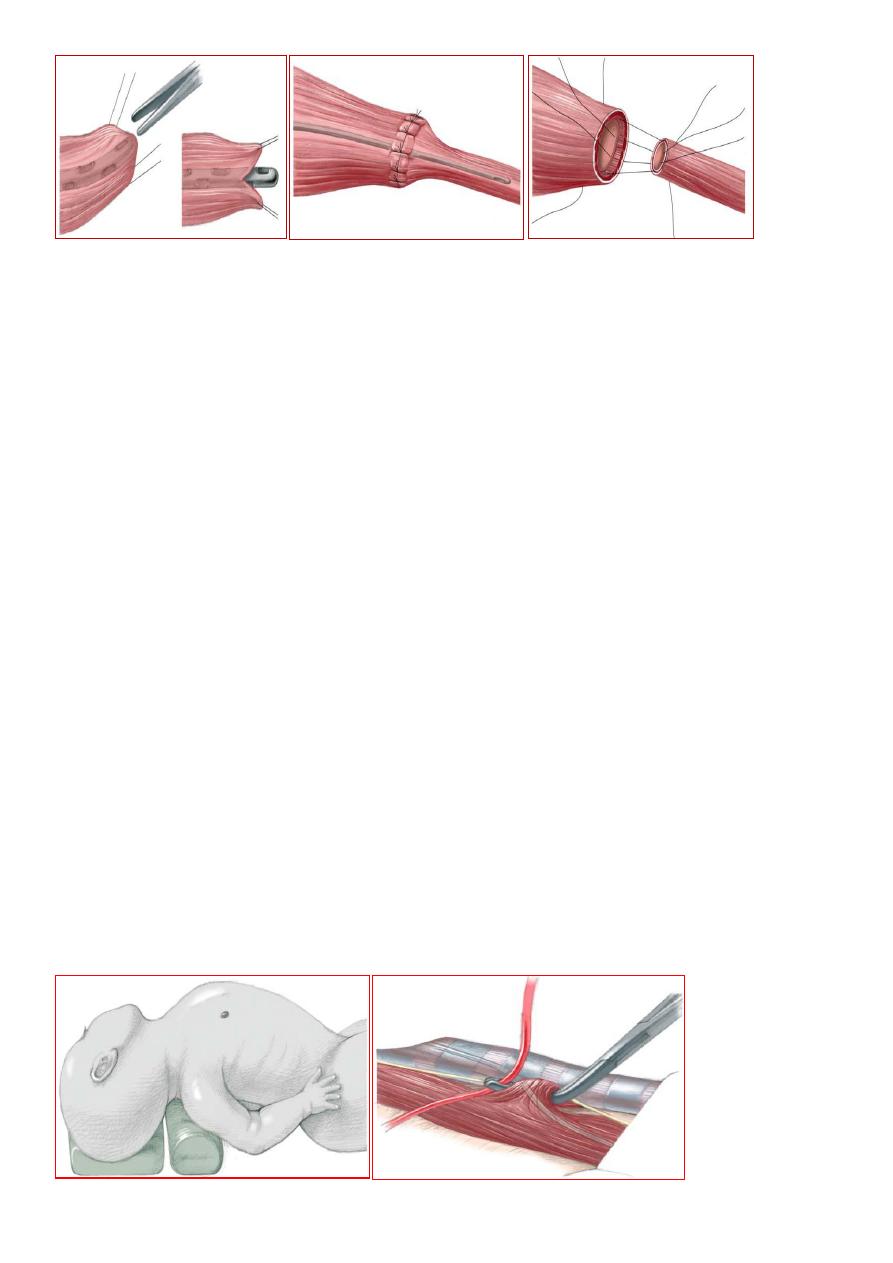
Esophageal Atresia without fistula
-no connection to respiratory system.
-no gas below diaphragm on initial x-ray(also in prox. Fistula) .
-big gap primary anastomos is impossible.
- Gastrostomy to allow entral feeding.
-frequent suction of upper pouch.
-6 week later primary anastomosis done, if failed esophageal replacement is
required.(using either stomach,colon,or small bowel)
H-fistula
-the esophagus is intact .
-ther is abnormal fistulous communication at level of C7 or T1.
-clinically :
in first week of lifeepisod of coughing .
cyanosis during feeding.
pulmonary complications.
later on requrrent pulmonary infection .
abdominal distention mimmic bowel
obstruction.
Diagnosis:
1-barium swallow or mid esophageal contrast study .
2-bronchoscopy.
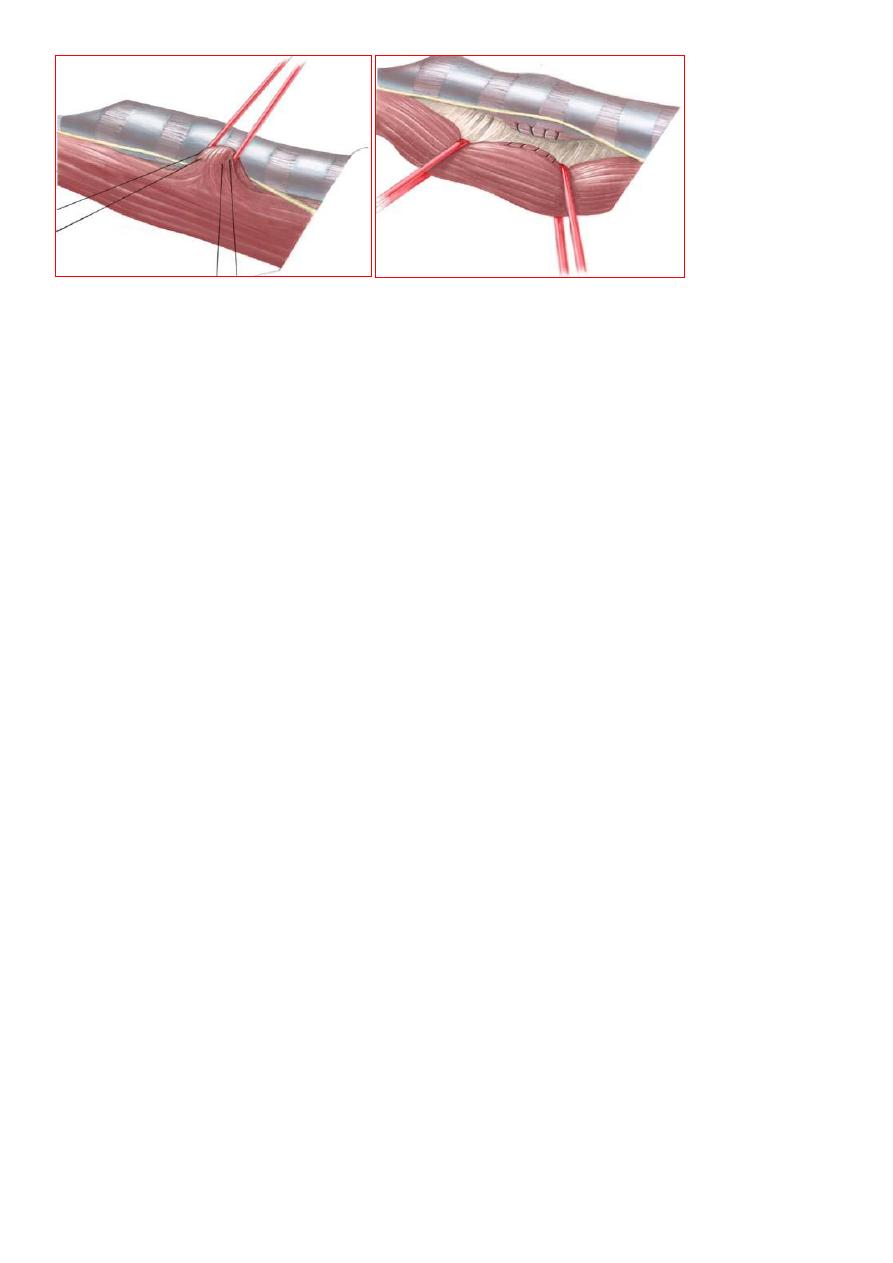
Treatment
-cervical approach.
-right cervical incision.
-identification of the fistula &division with tissue interposition to prevent recurrence.
6
Complication of surgery
1-anastomotic leak:2 types
a-minor common &treated conservativly.
b-magor leak mediastinitis&empyema.
2-stricture anastamosis or secondary to GERD
3- recurrent TEF.
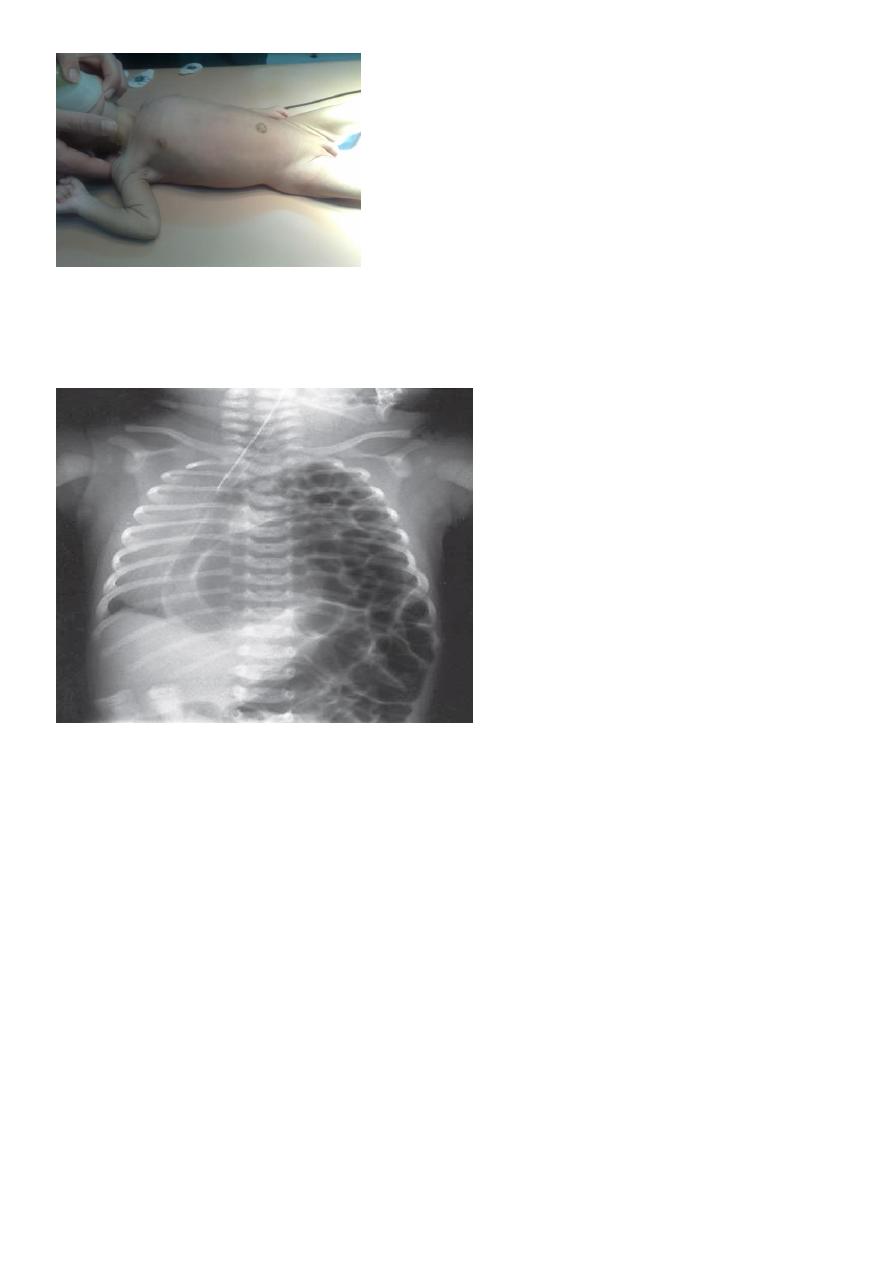
Congenital diaphragmatic hernia
The diaphragm develops largely from three structures:
1- the pleuroperitoneal membrane;
2- the septum transversum;
3- the marginal ingrowths from the muscles of the body
wall.
The Bochdalek type is the most common.
During intra-uterine development, the small bowel, stomach, spleen and left lobe of the
liver pass through the defect in the diaphragm into the chest, limiting the space available
for the developing lung. This causes lung hypoplasia.
Antenatal diagnosis;-
-ultrasonography.
Postnatal diagnosis:-
Clinically
1-cyanosed with severe respiratory distress
within minutes of birth(pulmonary hypoplasia is severe).
2-tachypnoea, increased respiratory effort.
3-hyperinfl ated chest and scaphoid abdomen.
4-heart sounds are on the right side.
5-The most common serious abnormalities are heart defects.
7
Investigation
1-chest x-ray.
2-Alternatively, a barium study will show bowel within the thoracic cavity when there is a
diaphragmatic hernia.
Treatment
1-intensive cardiorespiratory
support and insertion of a nasogastric tube to prevent bowel dilatation within the chest.
2-avoid hyperinflation and barotrauma of the small hypoplastic lungs.
3-Ventilation with a face mask (‘bagging’) should be avoided Vigorous endotracheal
ventilation should also be avoided because of the risk of causing barotrauma and a tension
pneumothorax
Sudden deterioration is usually caused by tension pneumothorax.
when the infant’s condition is stable.
This may be anywhere between 12 h and 7 or more days after birth.
In left-sided defects, a left transverse or subcostal abdominal incision is used.
The management of the infant with severe hypoplastic lungs is diffi cult and may involve
highfrequency oscillation or extracorporeal membrane oxygenation.The major cause of
death remains pulmonary hypoplasia and pulmonary hypertension.

8