
1
Fifth stage
Pediatric
Lec. 4
.د
رياض
1/3/2017
Poliomyelitis
It is one of the causes of acute flaccid paralysis syndrome causing paralysis of the muscles
of the limbs caused by; either wild strain PV , or by oral vaccine induced virus. It is
transmitted from person to person via feco-oral route.
Poliovirus is RNA enterovirus.
Patterns of polio infection
• Basically three forms of infection
• A. minor illness (abortive) not affecting muscle power, presents as flu like fever, sore
throat ,vomiting.95%
• B. aseptic meningitis as headache, neck stiffness,fever. 2-3% of cases, no paralysis
• C. paralytic form 1% cause acute flaccid paralysis of the limbs , even bulbar or
bulbospinal paralysis.
Diagnosis and differential diagnosis
• Acute flaccid paralysis syndrome defined as Any acute limping less than 15 days
onset with weakness and absent reflexes should consider acute flaccid paralysis AFP
syndrom (polio,GB,TM) so send stool sample to the preventive medical center for
polio virus detection by; culture ,and by PCR to detect type of polio virus.
• Guillain-Barre syndrome GB is another cause for AFP ,so it should be excluded . In GB
syndrome is acute ascending bilateral symmetrical paralysis,while in polio it is
unilateral paralysis.
• Transverse myelitis TM also should be excluded causing paraplegia.
2
EPSTEIN-BARR VIRUS
INFECTION
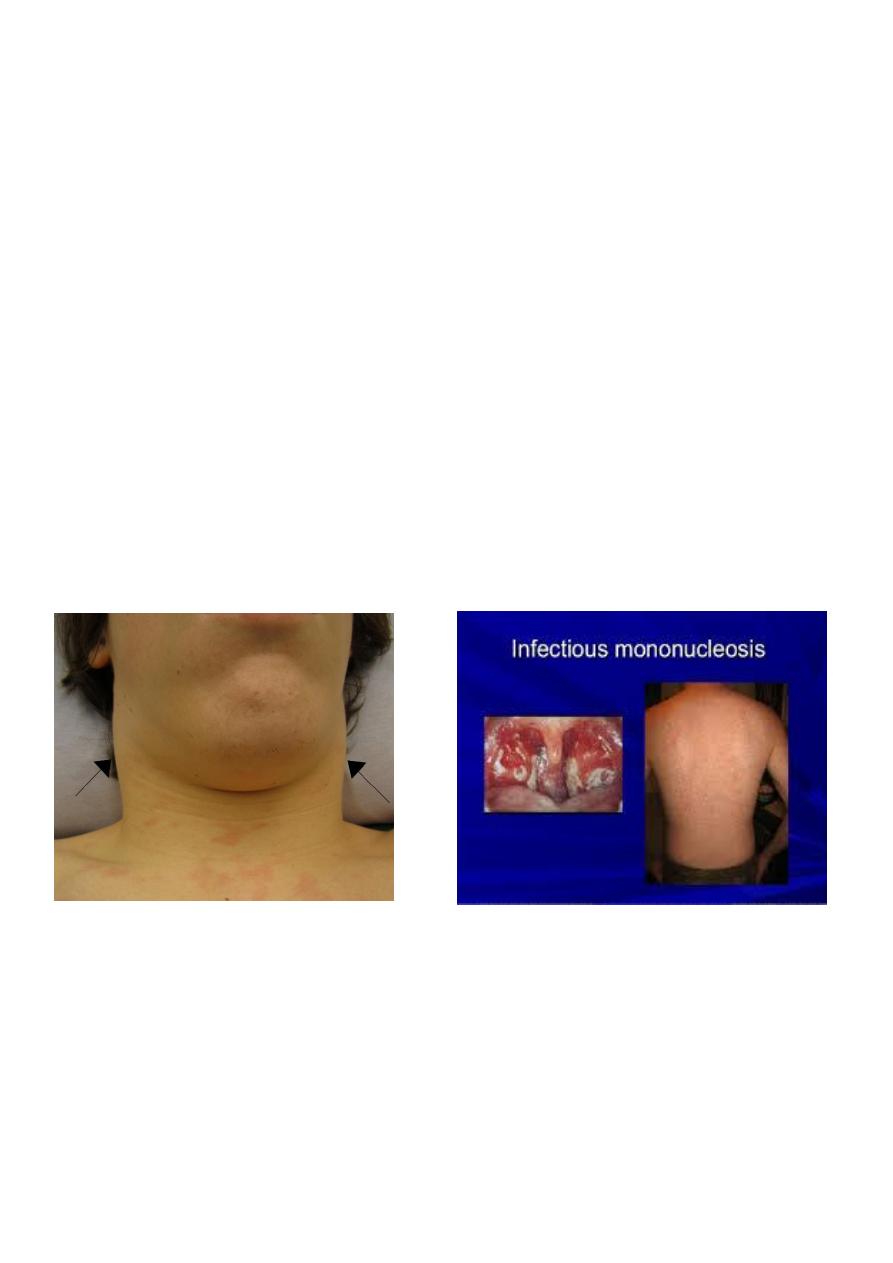
• INFECTIOUS MONONUCLEOSIS is the best known clinical syndrome caused mostly by
Epstein-Barr virus (EBV).it also called glandular fever. The virus is related to herpes
group; DNA virus. It causes 90% of infectious mononucleosis syndrome.
• Other 10% caused by CMV and Toxoplasmosis, even adenovirus.
Clinical picture
• The virus transmitted by saliva. It is DNA herpes virus.
• Incubation period 1-2 months. Presentation as triad of fever for 1-2 weeks with
lymphadenopathy of the back of the neck, axilla, groin, and sore throat simulate
exactly follicular tonsillitis due to streptococcal infection. Hepatosplenomegaly may
be found They regress in 2-3 weeks. Fever resolve in 1week. Most of cases develops
body maculopapular rash when ampicillin or amoxicillin are given.
• Spontaneous improvement within 2-4 weeks without special treatment.
Rash of ampicillin in IMN
TONSILLITISLYMPHADENOPATHY in IMN
3
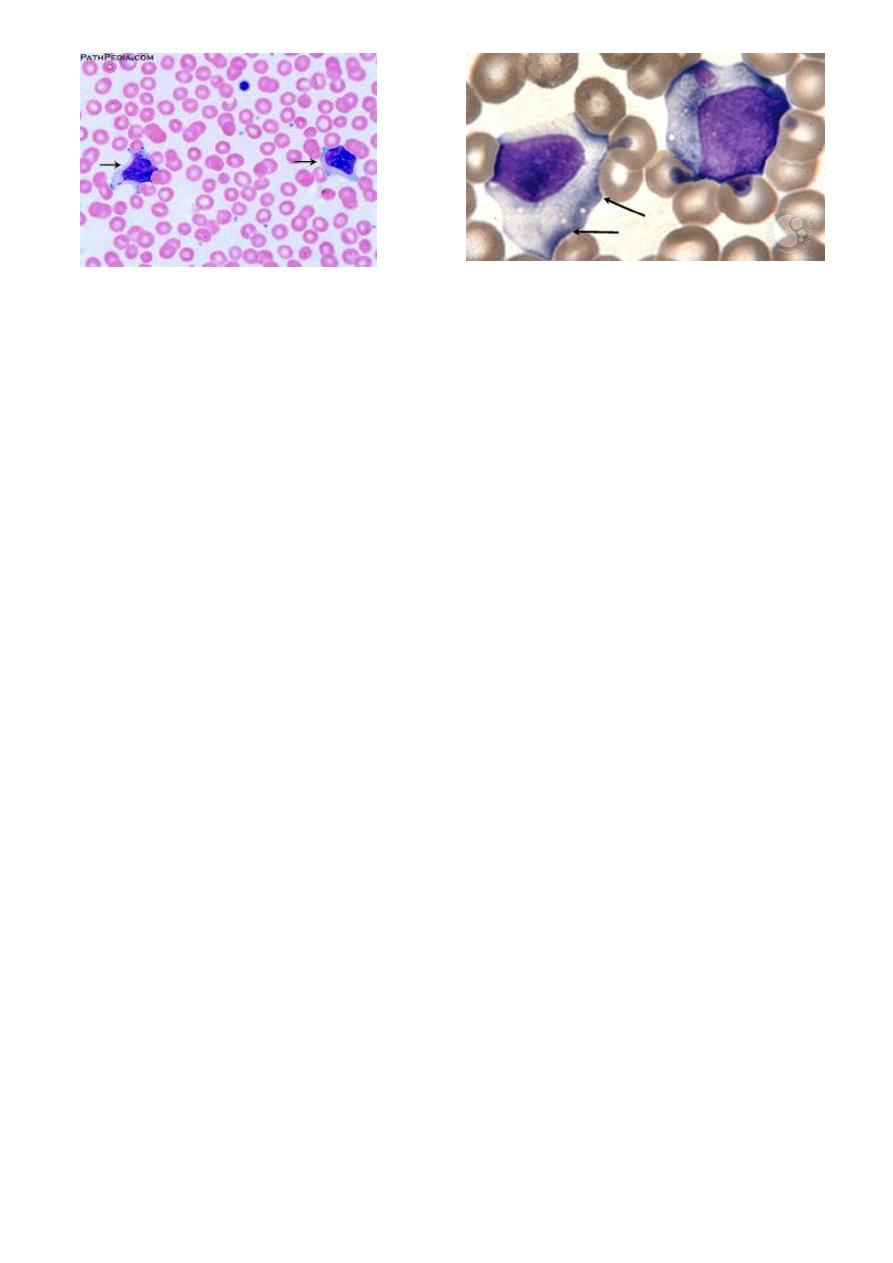
Atypical lymphocytes
Complications
• Splenic rupture if exposed to trauma, in 0.5%of cases.
• Upper airway obstruction due to pharyngeal oedema and swelling
• Other complications are rare includes; hepatitis and jaundice, encephalitis ,Guaillain-
barre syndrome, hemolytic anemia,, thrombocytopenia, carditis, Burkett lymphoma.
Diagnosis
• CBC shows high leukocytosis mainly due to lymphocytosis; with 20-40% of
lymphocyte count are atypical (reactive cells) seen in the blood film Throat swab
culture ; negative for strept.bact,
• Definite diagnosis for EBV infection is to detect EBV- IgM antibody in the serum by
the lab.
• Differential diagnosis of EBV infection are CMV, adenovirus,, and toxoplasmosis, all
these shows lymphocytosis, and even atypical lymphocytes, but negative EBV
serology tests.
Management
• Usually no need for specific treatment. It remits spontaneously within 1-2 weeks. Just
supportive like antipyretic, but in case of complications like upper respiratory
obstruction due to oropharyngeal or laryngeal edema corticosteroids may be used.
large cytoplasm,nucleoli in the nucleus,
indented by surrounding RBCs