Fifth stage
radiologyLec-1
د.هديل
6/3/2017
G.I.TRadiological investigations:
1- Contrast examination Barium study Ba. Swallow, Ba. Meal, Ba. Follow through & Ba enema 2-Endoscopic Ultrasound .3- CT & MRI.4-Nuclear medicine (FDG-PET): flurodeoxyglucose positron emission tomography.

THE OESOPHAGUS
Barium Swallow:1. Conventional2. Double contrast (DC)3. Flouroscopy + spot films
Technique:
1.Patient will need to be NPO after midnight before the exam2.The patient will have to swallow a contrast agent: Barium or Gastrograffin
May also swallow sodium bicarbonate for double contrast barium swallow
3.X-ray tech will have the patient perform various maneuvers so that the barium can coat the GI tract
Indications:
Odynaphagia
Dysphagia
Hematemesis
Abdominal pain
Unexplained weight loss
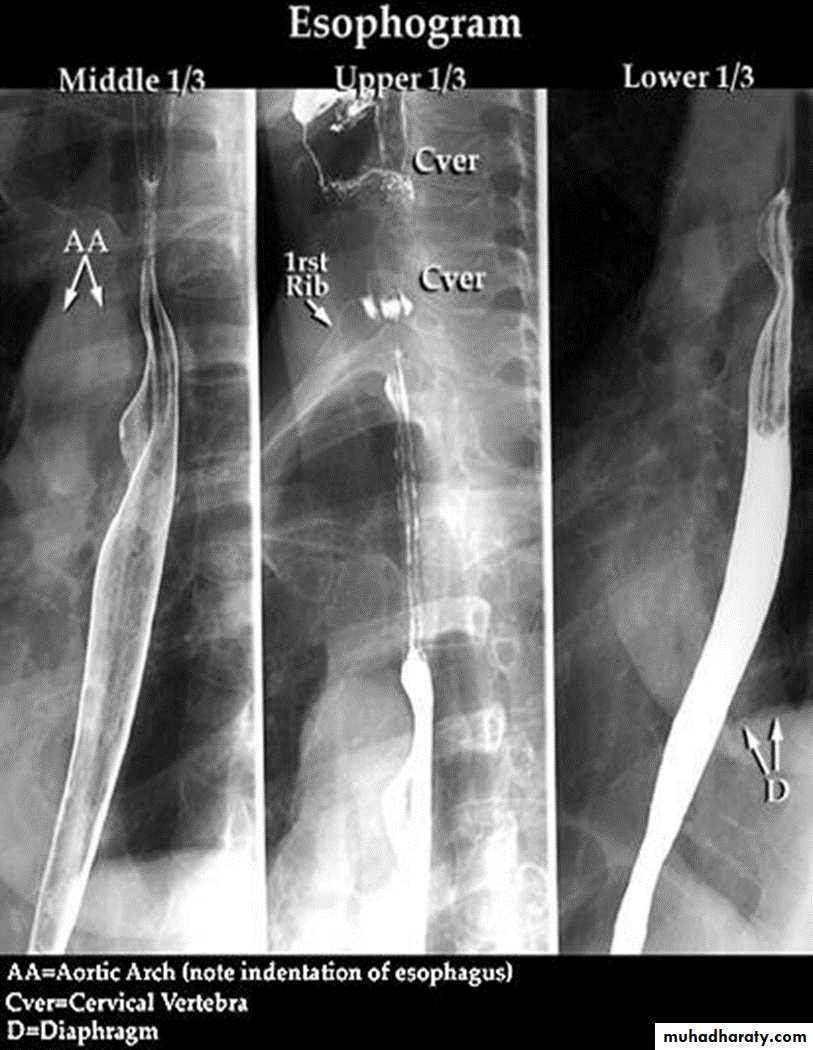
The Normal Anatomy: *Long tubular structure * Length 25-30 cm* Start at level of C5 ( Crico-pharengeal)* End – Cardiac sphincter* Three portions Cervical Thoracic Abdominal* Normal Mucosal pattern (DC) thin regular longitudinal Parallel Numbers of lines ( 4-5 )
Areas of normal Narrowings:- body of the cervical vertebra - AA- LT atrium- diaphragmatic hiatus

On the Hypo pharyngeal part Common structures that we can visualize are:
EpiglottisPost cricoid impression
Crico pharyngeal muscle impression
lateral pharyngeal pouches

LEFT: Lateral view: Epiglottis (red arrow).
Post cricoid impression (yellow arrows).Crico pharyngeous impression (white arrow).RIGHT: AP-view: Small lateral pharyngeal pouches (arrows)
The esophageal wall is composed of:
Mucosa
Musculature
Inner circular layer
Outer longitudinal layer:
Upper 1/3 striated muscle
Middle 1/3 striated and smooth muscle
Lower 1/3 smooth muscle
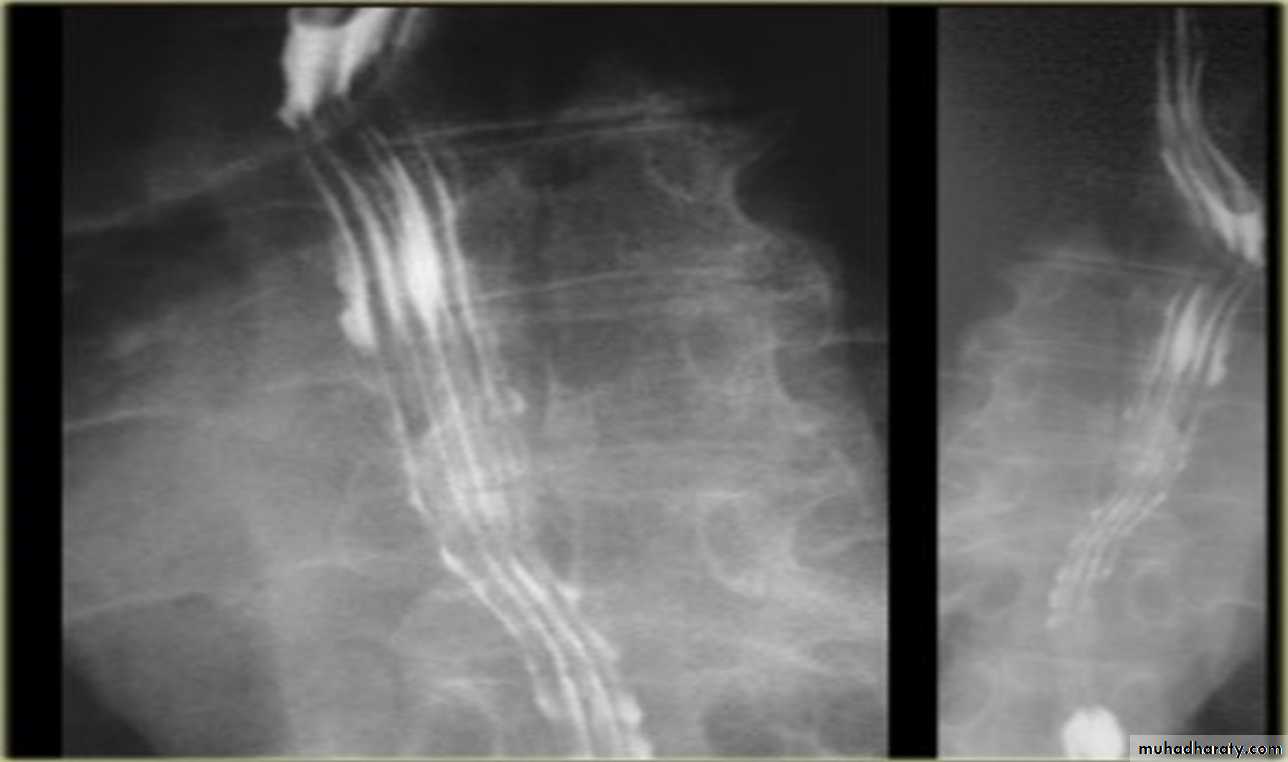
Esophagus mucosa: normal thin, parallel, uniform mucosal folds 3-4 in no.in double contrast examination
Esophageal peristalsis
Normal:Primary contraction: Propels bolus through the esophagus
Secondary contraction: Follows primary contraction and propels any remaining bolus from thoracic esophagus
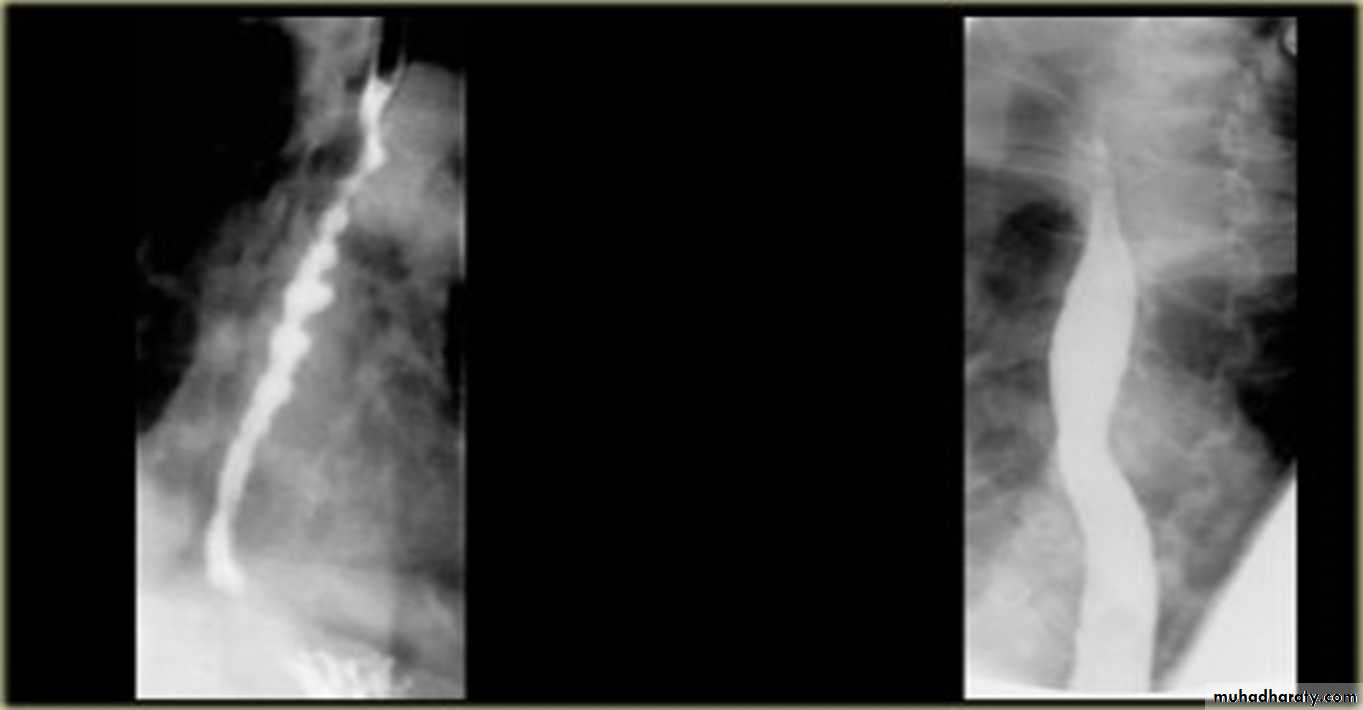
Abnormal contraction :
Tertiary contractionsDiffuse esophageal spasm
Nutcracker eosaphagus (crock screw)
Decreased peristalsis
resulting from achalasia, scleroderma, dermatomyositis, polymyositis, esophagitis, and secondary to many other diseases.

tertiary contractions

Diffuse esophageal spasm
Diffuse esophageal spasm produces intermittent contractions of the mid and distal esophageal smooth muscle, associated with chest symptomsCongenital Anomalies
1- Artesia with or with out tracheo-oesophageal fistula (TEF).2- Congenital Short oesophagus.
3- Congenital Duplication ( Neuro-enteric cyst )
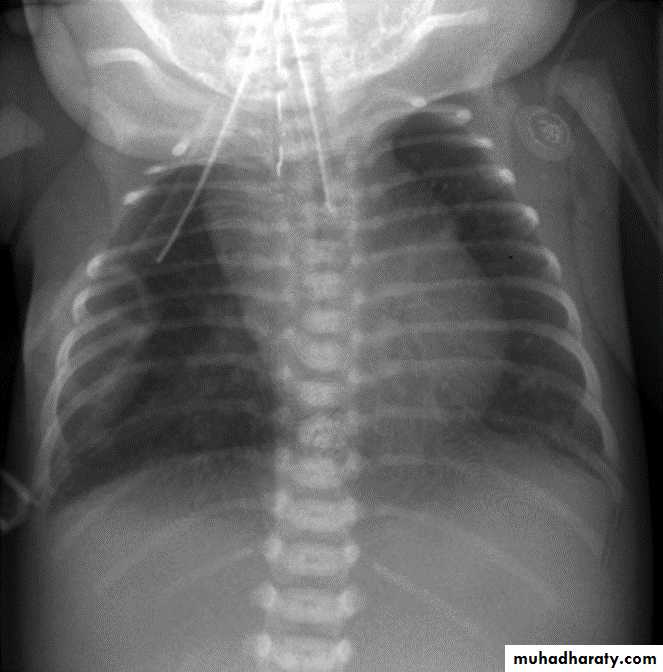
ATRESIA:
1-Complete blockage of the lumen .
2- The diagnosis is suggested after birth by inability of infant to feed or by choking during swallowing .
3- The blocked segment is mostly seen at level of thoracic inlet
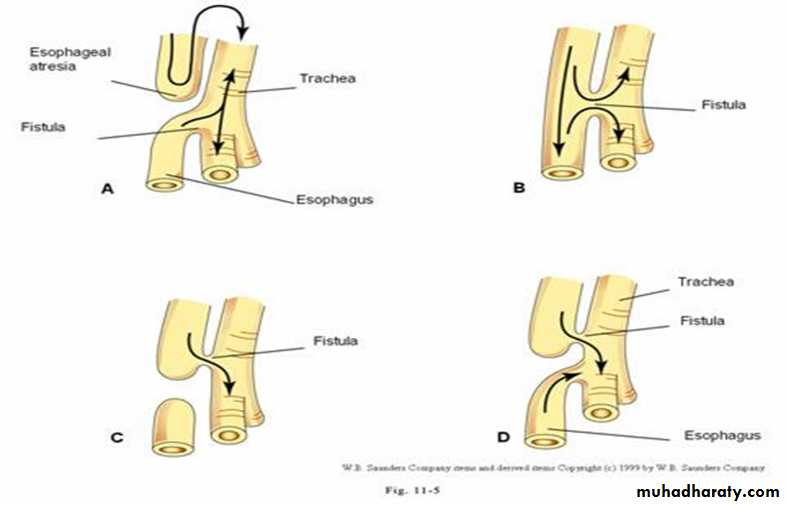
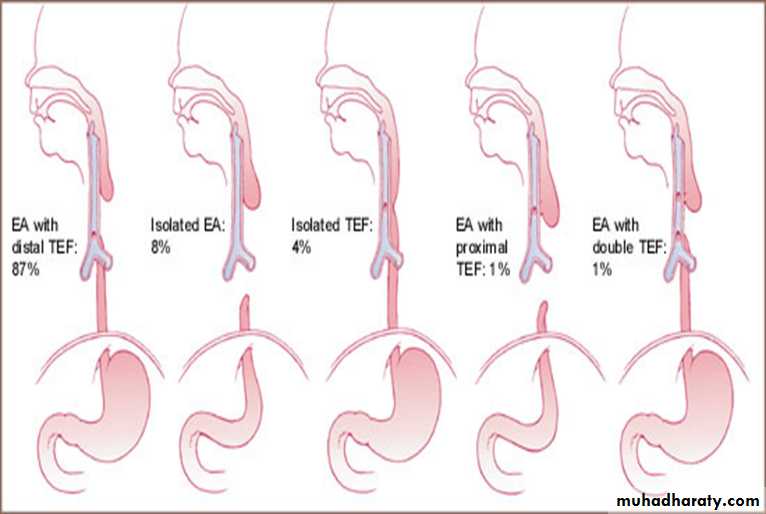
TYPES OF FISTULA



Acquired Lesions
DYSPHAGIA : CAUSES :1- Carcinoma ( Malignant stricture).
2-Benign Stricture (Corrosive ).
3-Achalasia Cardia.
4-forgien body
5-osophagitis .
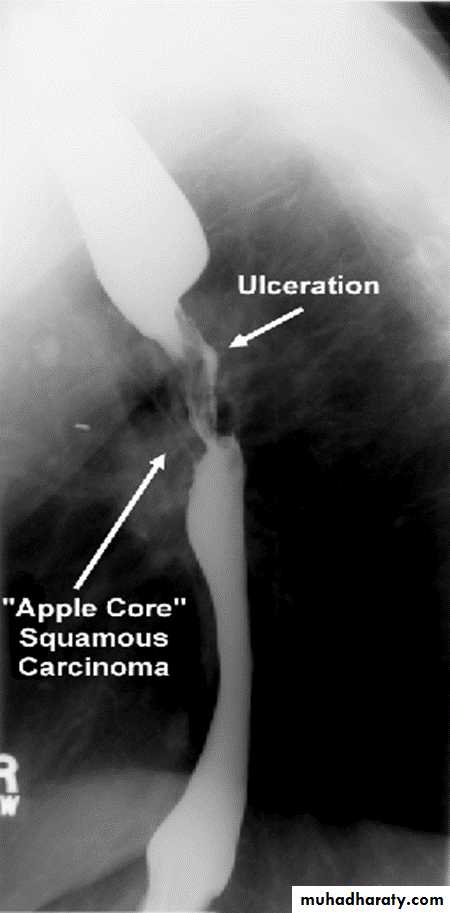
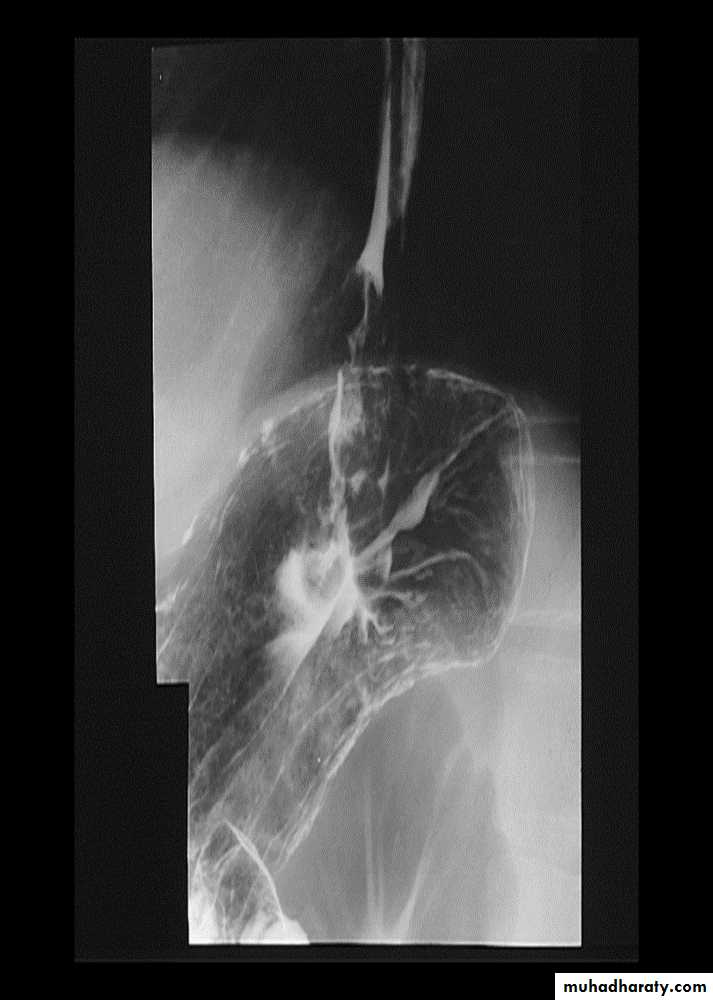
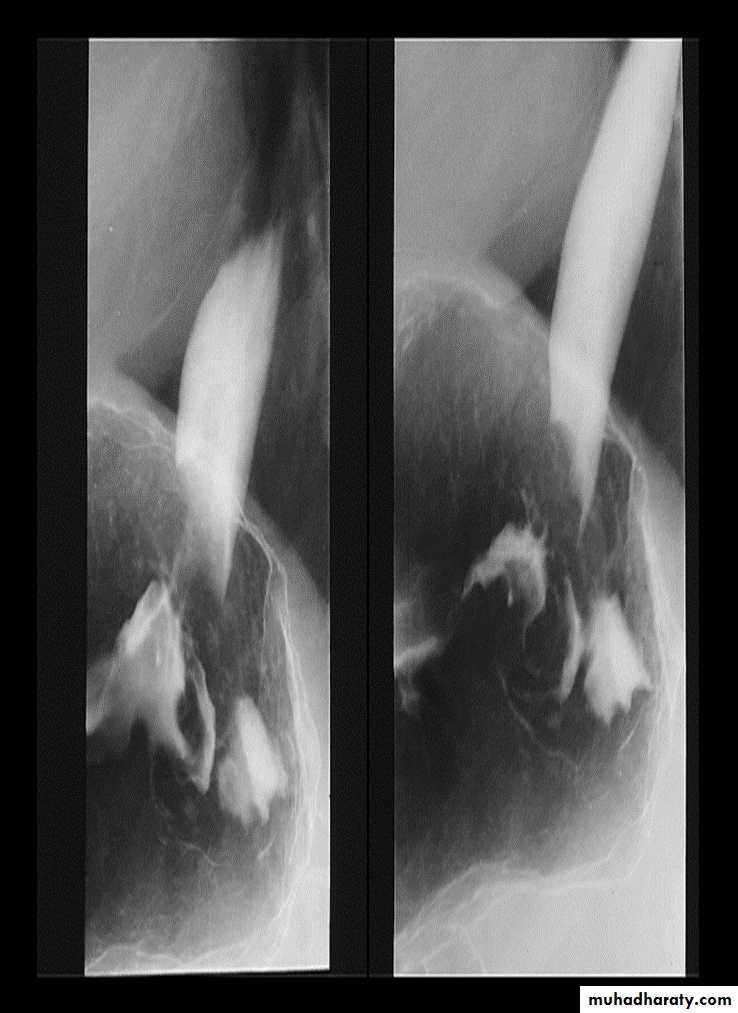
Malignant stricture
CA esophagus is the cause for the malignant stricture
The most common types of esophageal carcinoma are squamous cell carcinoma and adenocarcinoma .
esophagography is unique among esophageal studies for assessing both morphology and motility. Barium esophagography remains the study of choice for characterization of esophageal strictures. Esophageal carcinoma may demonstrate a variety of appearances on barium esophagrams.
Annular Carcinoma
Narrowing :
1-Constant.
2-Irrigular .
3-Variable length.
4- Shouldering sign.
5-Fistula (double tract).
6-Soft tissue shadow of the mass


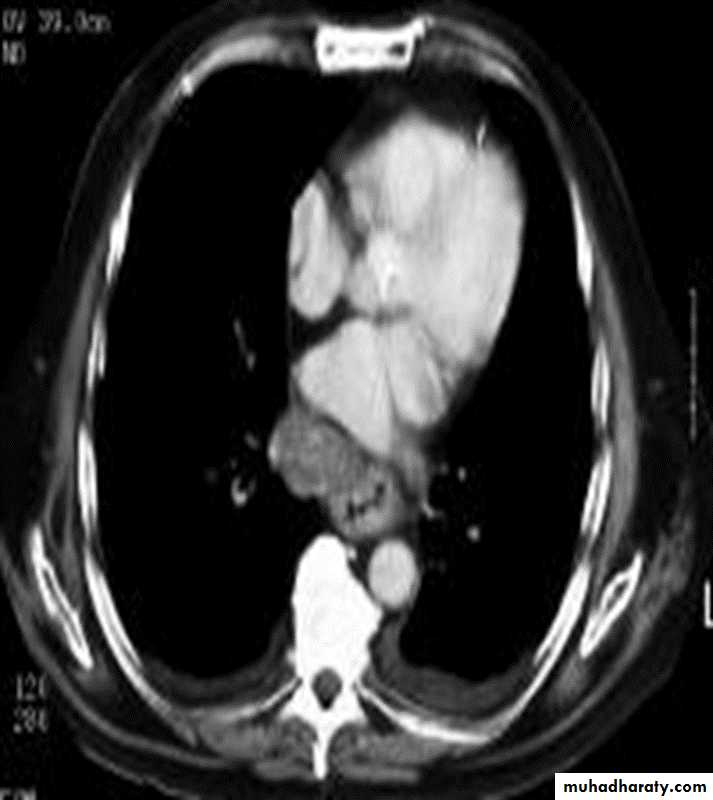
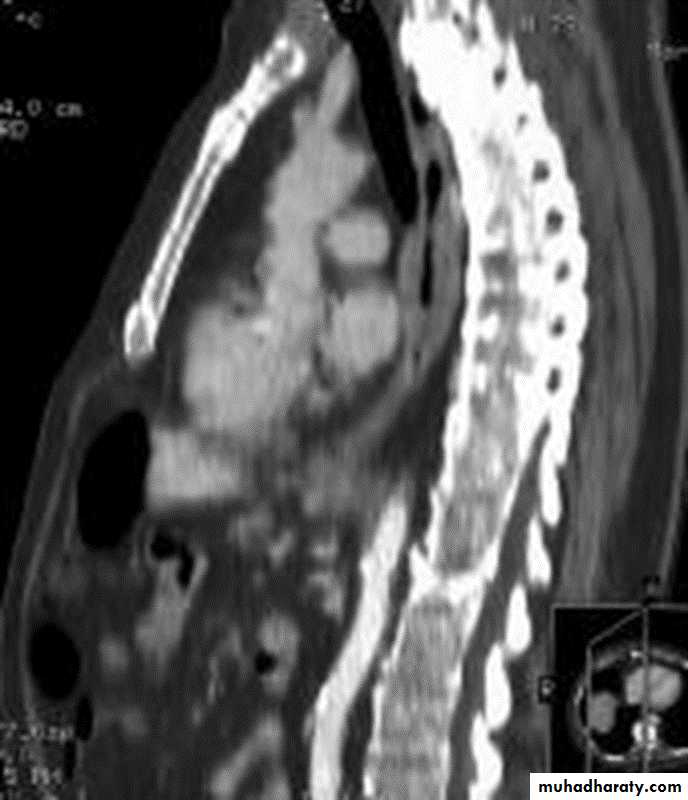
Computed Tomography
Contrast-enhanced CT plays an important role in the1.staging of esophageal carcinoma.
2.determining the extent of the local tumor
3.invasion of mediastinal structures
4.involvement of supra clavicular, mediastinal, or upper abdominal lymph nodes
5. Assessment of the distant metastases
examination should extend from the thoracic inlet through the liver
Routine oral contrast material such as (gastrographine) or a negative intra luminal
contrast medium, such as water.
+/ - IV contrast injection
CT essential in the Dx & staging of the CA
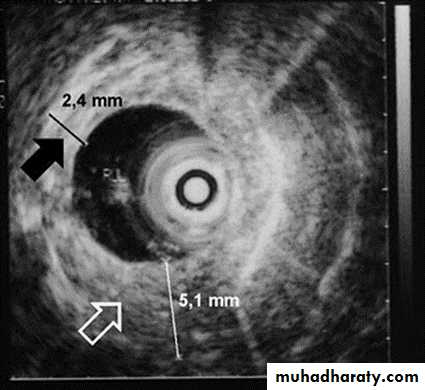
CT finding of esophageal malignancy
1.Eccentric or circumferential wall thickening is greater than 5 mm.
2.Peri-esophageal soft tissue and fat stranding may be demonstrated.
3.A dilated fluid- and debris-filled esophageal lumen is proximal to an obstructing lesion.
4.Aortic invasion .
5.Osophageal CA is often metastatic at the time of presentation ( look for the LN & distal metastasis ) .

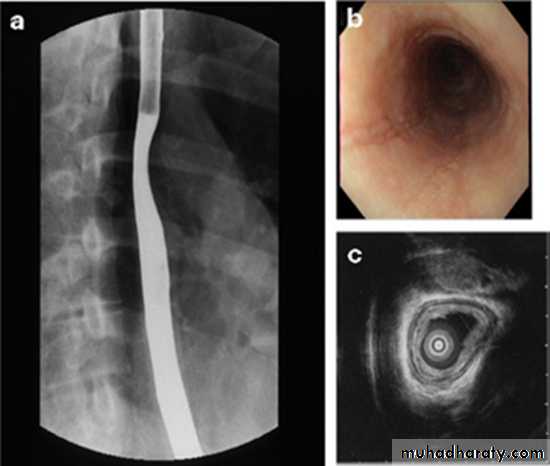
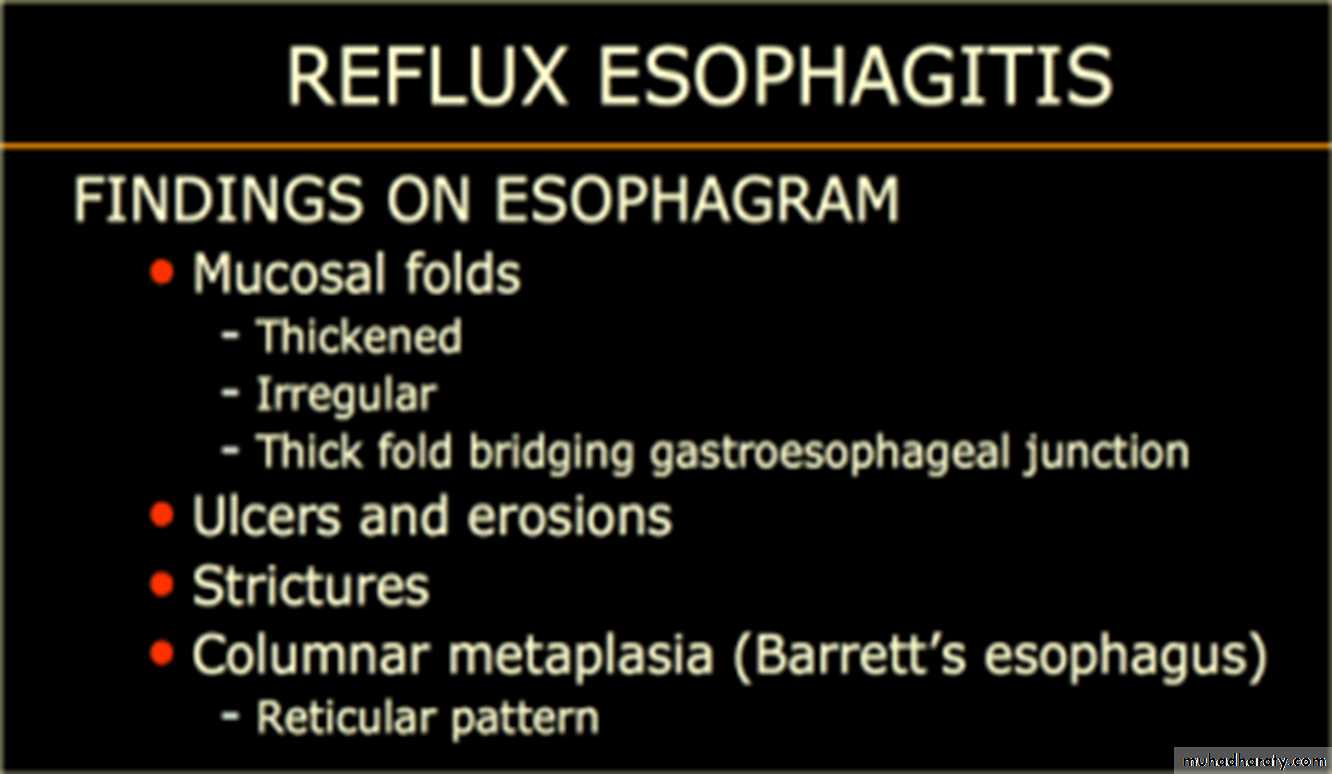
Barrett's esophagus
is a metaplastic disorder in which specialized columnar epithelium replaces healthy squamous epithelium.Barrett's metaplasia is the most common cause or precursor of esophageal carcinoma. The rate of esophageal adenocarcinoma is increasing in the Western world, and it is associated with a poor prognosis, mainly because individuals present with late-stage disease..
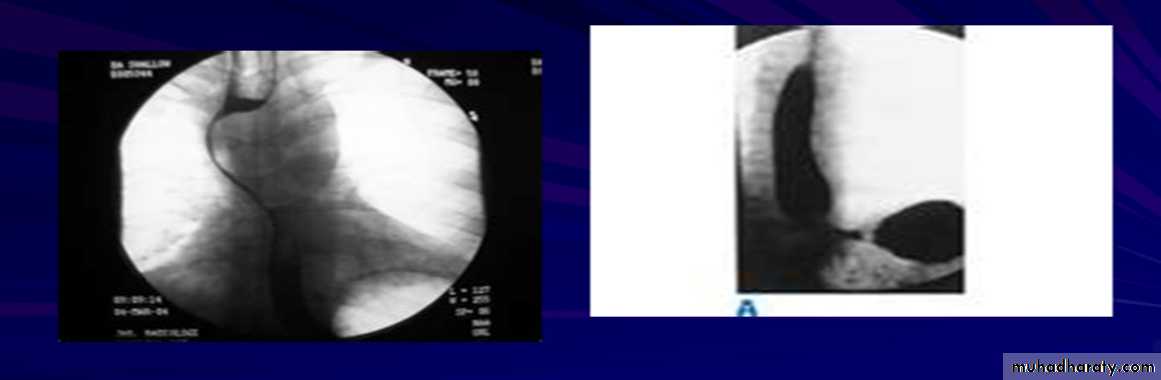
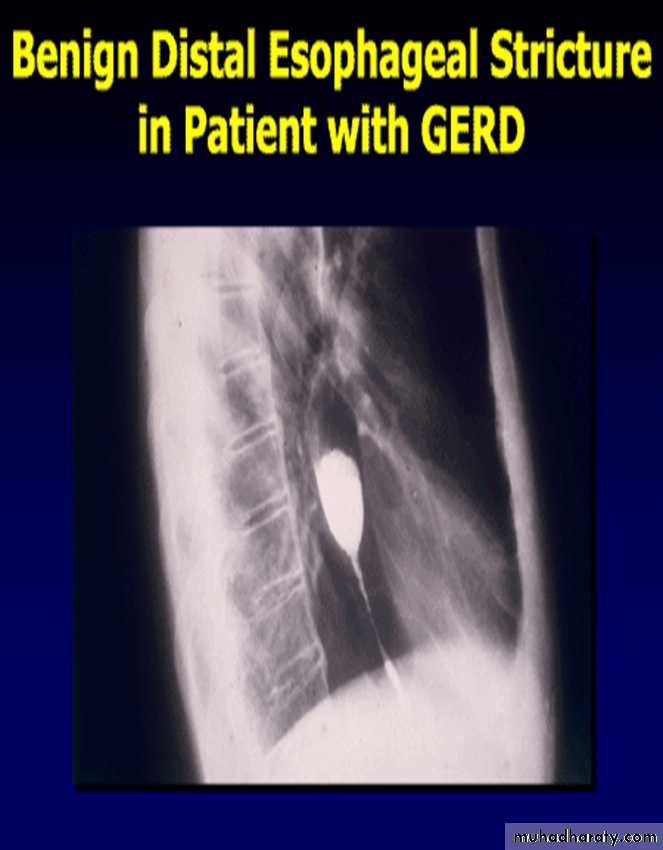
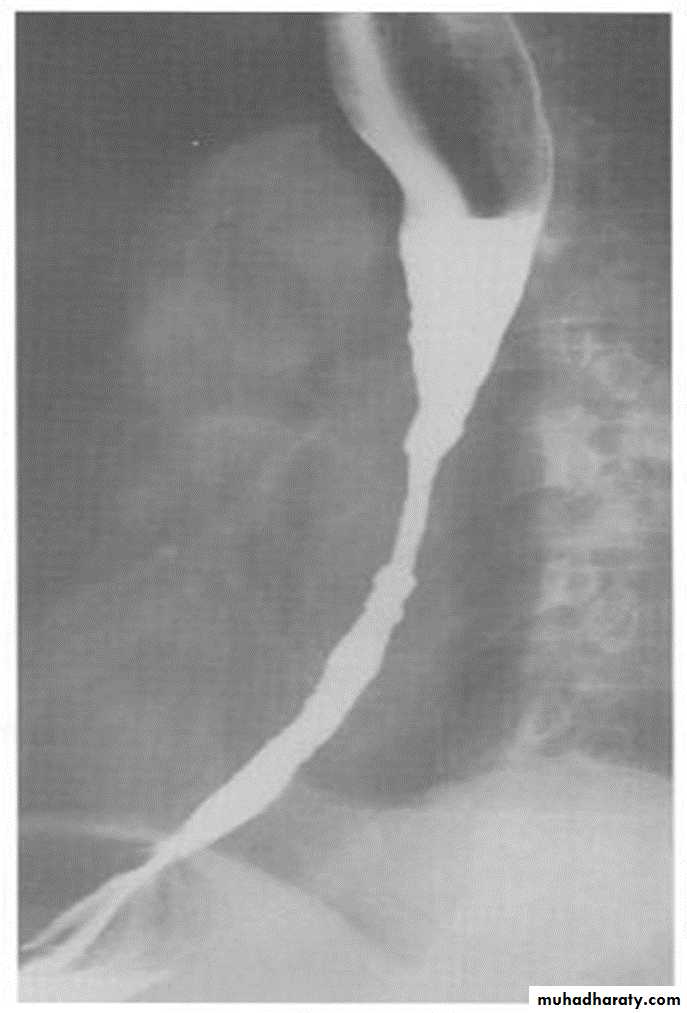
Benign Stricture
Causes :
1-Peptic esophagitis
2-Corrosive
3-Traumatic
Ba. swallow :
1-Constant narrowing.
2- Long length (lower third).
3-Smooth and regular.
4-Mild proximal dilatation.
5-No shouldering sign.
6-Smooth tapering
( funnel shape).
Inflammation and Infection
Gastroesophageal reflux (GERD) is the most common cause of esophagitis.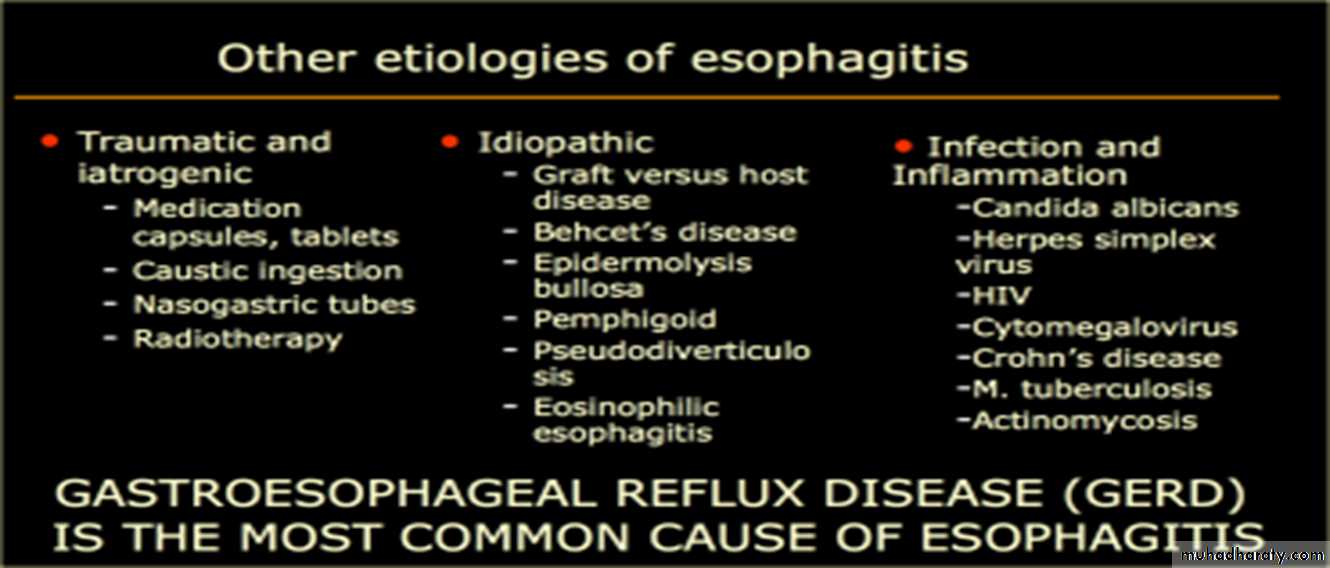
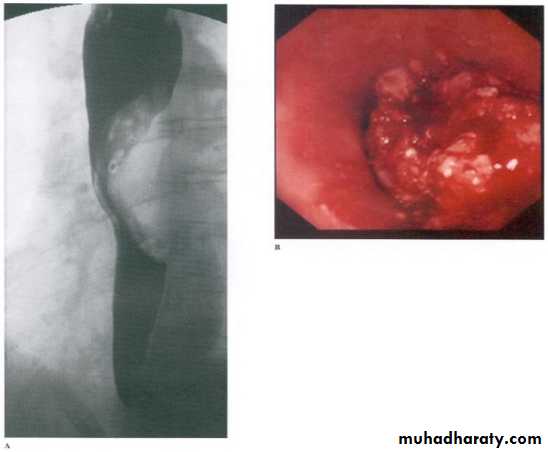
Infectious esophagitis
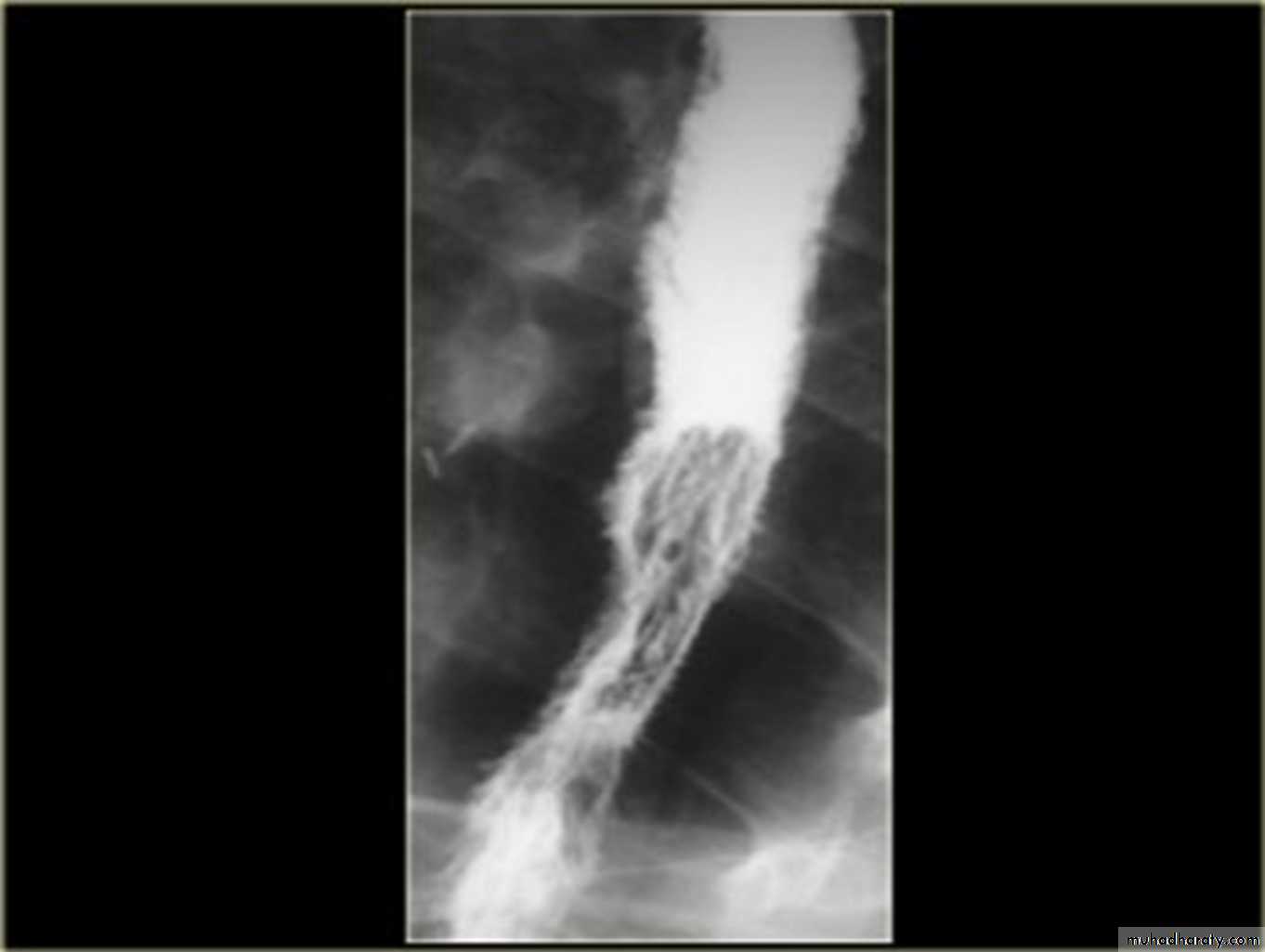
Candida esophagitis:in patient with an infectious esophagitis due to candida , the barium shows numerous fine erosions & plaques causing shaggy outline of the osophagus due to Candida albicans in immunocompromised patient.
middle year old female with a past medical history significant for HIV/AIDS comes in with complaint of loosing their weight over the past 2 weeks with pain & difficulty on swallowing …. Also feels like food is getting stuck in her throat
What is your diagnosis ??????????