Fifth stage
RadiologyLec-2
د.هديل
13/3/2017
مكتب الجامعه للطباعه والاستنساخعدد الارواق :7
السعر :500
Radiology of G.I.T
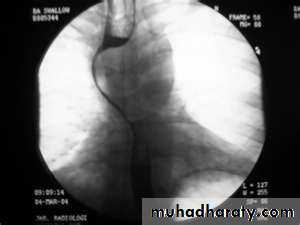
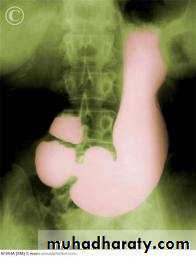
A chalasiaCardiaPresentation:
Equal M:F incidence, most common in middle-age
Slow progression of dysphasia to start with to solid material then to solid & water
Increased incidence of carcinoma
Etiology:
Unknown ??? absent or reduced esophageal ganglion cells at their distal lower sphincter
Incomplete or absent relaxation of LES with swallowing
Absent primary peristaltic waves
A : Absence
Chalasia : Relaxation
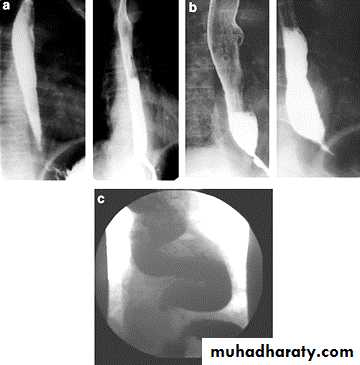
Narrowing :
the narrowing is Constant Short length (confined to cardia).
Regular and smooth.
No shouldering sign.
Tapering (Tip of pencil , cigar shape) Under left dome of diaphragm.
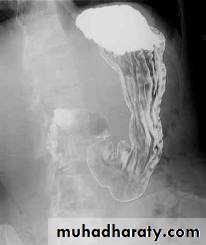
DILATATION (Sac like in proximal part )
Undulating or spiky out line due to sluggish peristalsis.
Non- homogeneity of Barium due to food particles.
Air Barium level.
CXR shows widening of mediastinum.
Absence of fundal gas shadow.
Basal fibrosis in lungs due to repeated aspiration pneumonia .


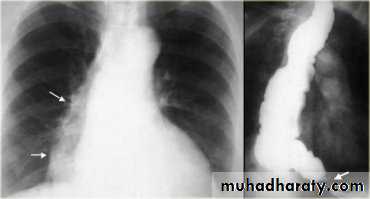
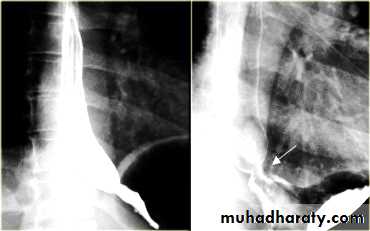
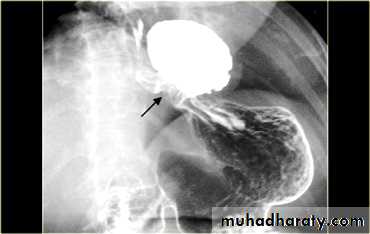
LEFT: Dilated esophagus (arrows) appears as long, well-defined structure paralleling heart RIGHT: Dilated esophagus usually deviates to right. Narrowing (arrow) at hiatus.
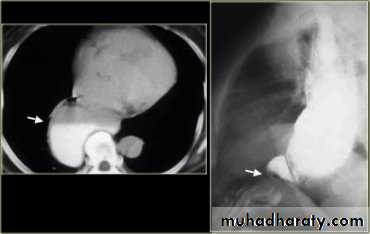
LEFT: CT shows dilated esophagus (arrow) that led to esophagram.RIGHT: Esophagram shows narrowing (arrow) at level of hiatus.

PULSION DIVERTICULUM
Due to:raised intra-luminal tension
Chocking after meal .
In cervical portion at level of C5
Posteriorly (Killience dehiscent)
Lateral view show increased pre-vertebral space with air fluid level.

Confirmed by Ba. Swallow.


TRACTION DIVERTICULUM

Out pouching of lumen laterally due to fibrosis & adhesions ( post-Tb.)
In the middle third at level of hilum
Up ward direction of diverticulum
Irregular base
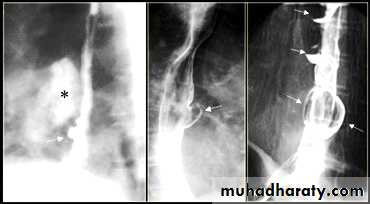
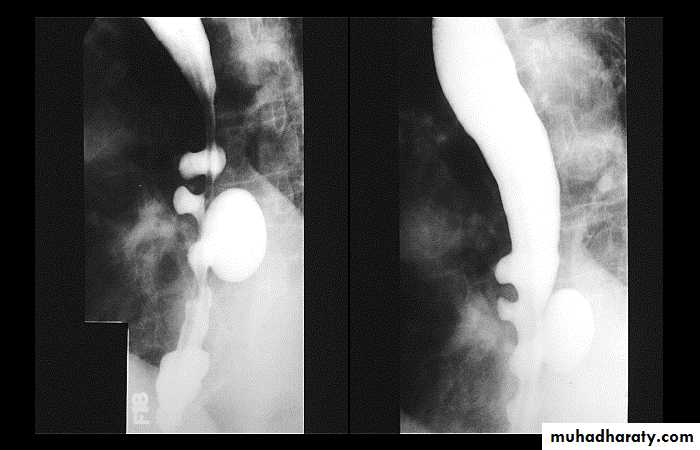
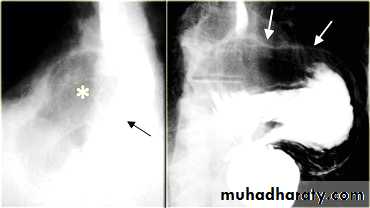
On the far left a traction diverticulum (arrow) due to hilar granulomatous disease. Calcified adenopathy (asterisk).
In the middle a pulsion diverticulum (arrow) due to high intra luminal pressure.
On the right multiple pulsion diverticula (arrows)
CONGENITAL DIVERTICULUM
Asymtomatic unless complicated.
At lower part of esophagus above the diaphragm (Epi-phrenic)
Lateral or posterior in position.
Sliding herniaOn the left initially, GE junction is below the esophageal hiatus. Later, stomach protrudes through hiatus
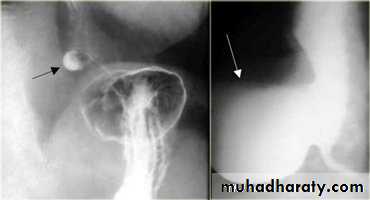
Para esophageal hernia
On the far left gas filled gastric funds (asterisk) protrudes through hiatus but GE junction (arrow) is below diaphragm
ESOPHAGEAL WEB
Thin mucosal fold (membrane)Arise from anterior wall and extend Posteriorly .>>>MCQ
Lateral view Ba. Swallow show self like filling defect with proximal dilatation.
Single or multiple

.
10% incidence at autopsy
Can be congenital or acquiredMost in hypopharynx and proximal esophagus
Majority protrude from anterior esophageal wall
Symptoms if lumen > 50% compromised
Sideropenic dysphagia (Plummer-Vinson syndrome) which is :
Iron deficiency anemia
Esophageal web with dysphagia
Increased incidence of carcinoma

Validity of syndrome debatable
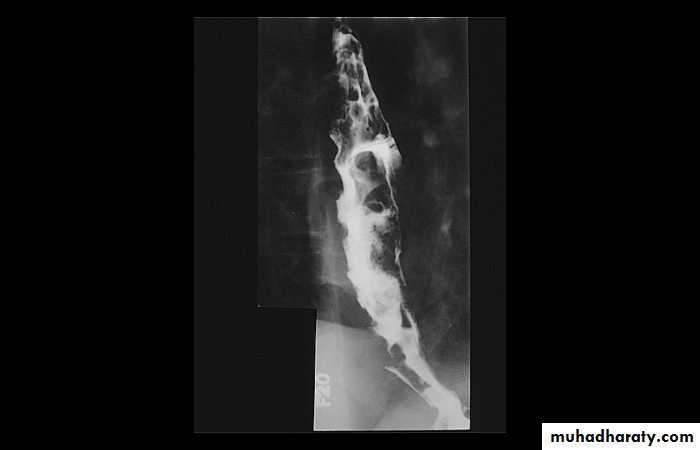
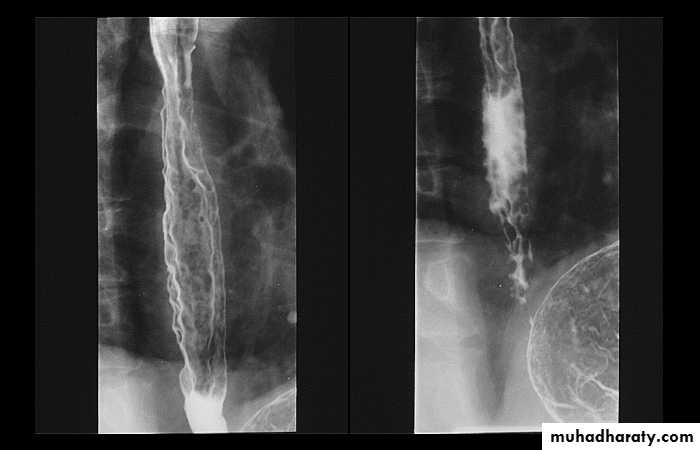
Esophageal Varieces
Dilatation of venous plexus in the wall of the esophagus due to increased pressure ( portal H.T.).Important cause of Hematemesis .
Early changes seen in the mucosa (D.C.) loss of parallelism with thick and tortuous folds.
Later multiple small filling defects (fine cobble stone).
In advanced stage large filling defects ( coarse cobble stone ) .
7More advanced stage elongated and worm like filling defect .

The changes are seen at lower third and gastric fundus.



Stomach & duodenum
Barium mealBarium meal is radiological study of esophagus,stomach&duodenum.
Done by oral administration of contrast media”BariumSulphate”
Indications:-
Gastric or duodenal obstruction.
Malignancies of gastroesophagealjunction,stomach&duodenum.
Upper Abdominal mass.
Motility disorders.
Systemic disease like Tb.
GIT hemorrhage.

Barium meal Fluoroscopy + spot films Preparation

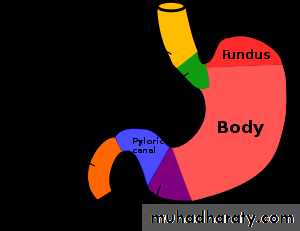
The Normal Anatomy of Stomach

1- Shape.2-Size.3-Site.4-Anatomical parts.5-Mucosal pattern.
Normal Anatomy of DuodenumA.Duodenal cap.
B.Duodenal loop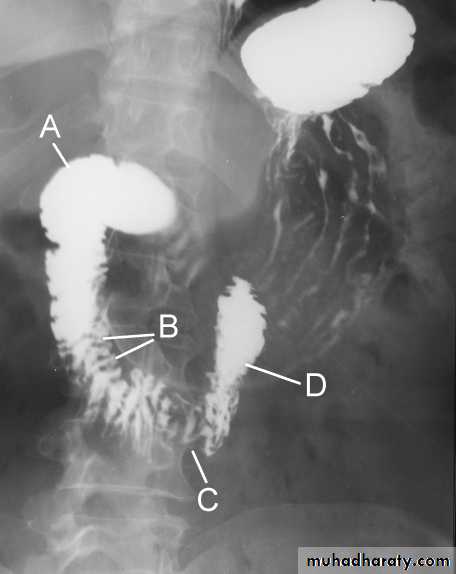
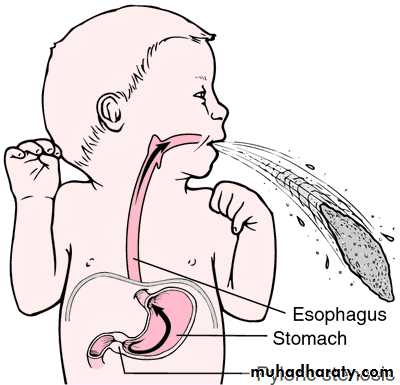
Hypertrophic pyloric stenosisCause:A. Congenital typeB. Adult type
Epidemiology:-Pyloric stenosis is relatively common and has a male predilection (M:F ~ 4:1), and is more commonly seen in Caucasians 4.
It typically occurs between the 4-8 weeks of life. There may be a positive family history.
Incidence of hypertrophic pyloric stenosis is approximately 2-5 per 1,000 births per year in most white populations.

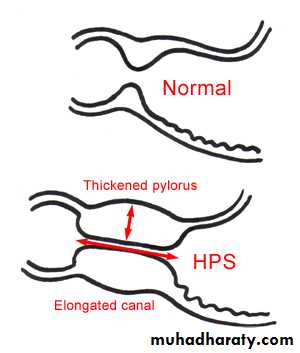
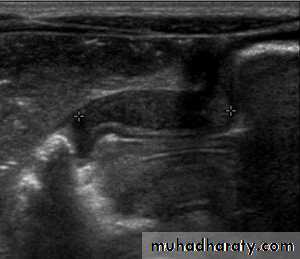
In a normal situation, the pyloric muscle thickness (diameter of a single muscular wall on a transverse image) should normally be less than 3 mm (most accurate 3) and the length (longitudinal measurement) should not exceed 15 mm.

