1
Fifth stage
Pediatric
Lec. 2
.د
اروى
29/3/2017
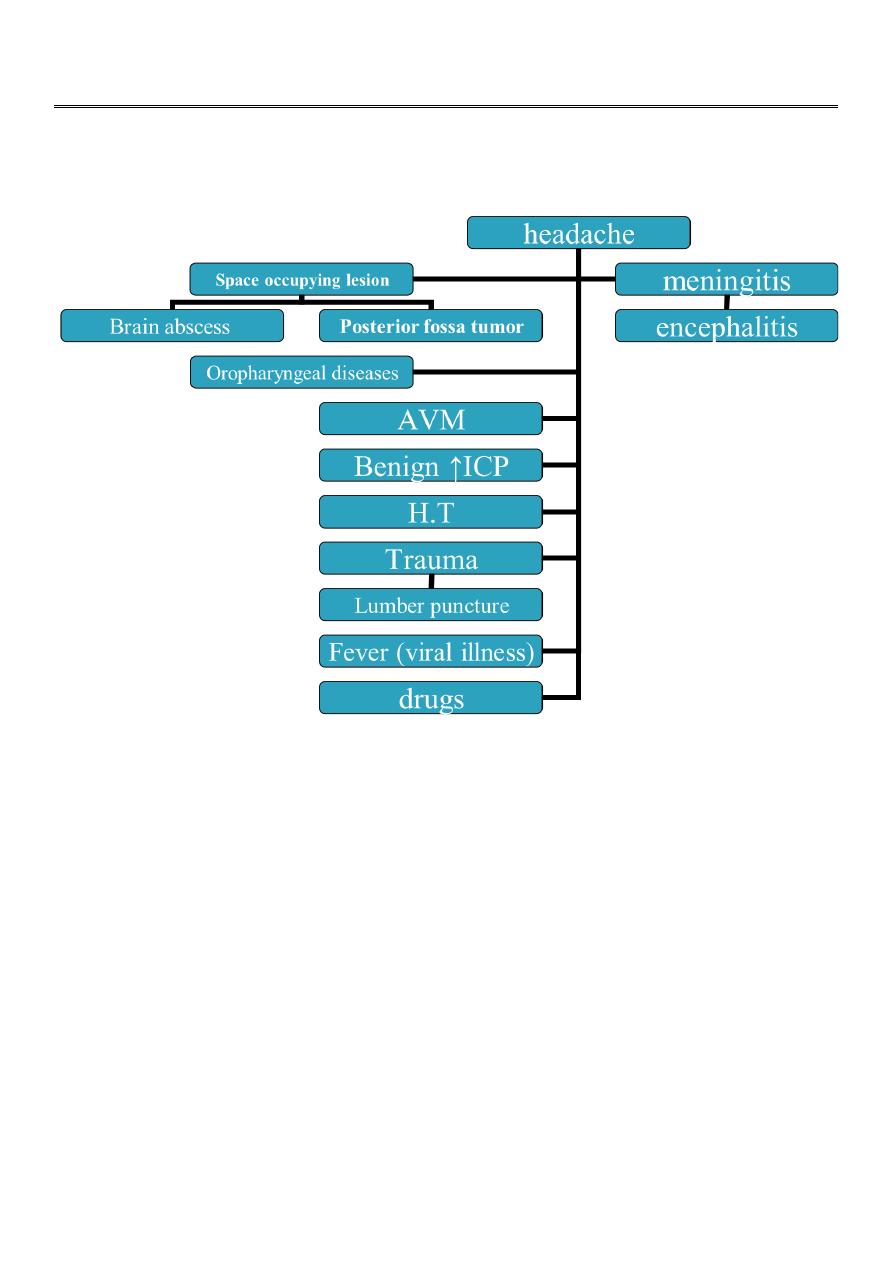
Headache and migraine
Worrisome headache
1-most sever on awakening.
2-that awaken the patient in the middle of night.
3-severly exacerbated on coughing or bending.
4-acute without previous history.
5-present daily &getting progressively more sever.
6-associated with vomiting.
2
Cyclic vomiting
1- mainly occur in infant and young children.
2- recurrent vomiting (dehydration with electrolyte disturbance).
3- fever , abdominal pain , diarrhea.
3- pallor, fright follow by deep sleep→ releave symptoms.
4- family history of migraine.
5- typical migraine headache in future.
Treatment:
1- fluid replacement.
2- rectal antiemetic (ondansetron)
D.Dx:(intestinal obstruction, peptic ulcer, IBD ,inborn error of metabolism ,CNS lesion).
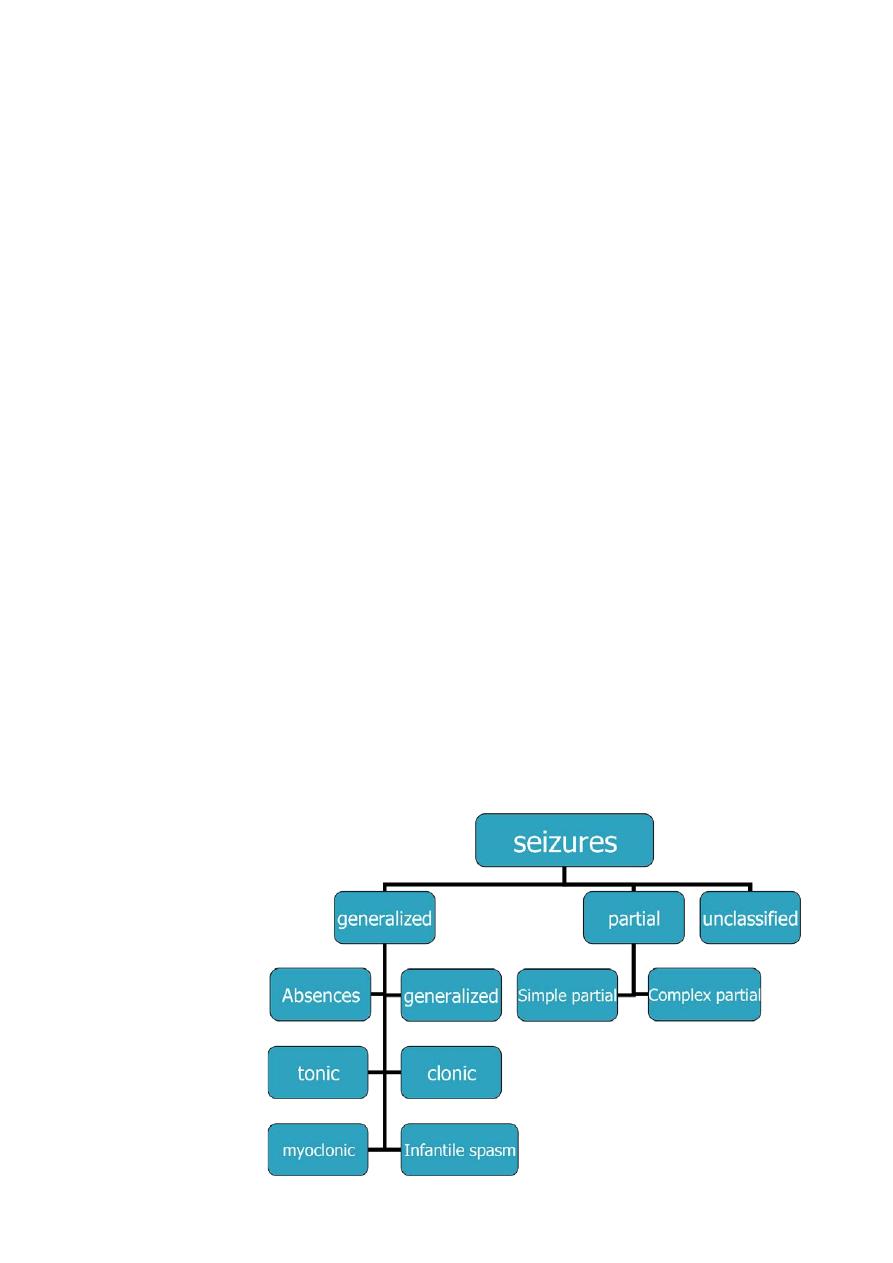
Seizures in childhood
Seizures (convulsion):
Define as is a transient occurrence of signs and/or symptoms resulting from abnormal
excessive neuronal activity in the brain.
Epilepsy:
is a disorder of the brain characterized by an enduring predisposition to generate seizures,
it is considered to be present when two or more unprovoked seizures occur at an interval
greater than 24 hr apart

3
Absence seizures
1- 6-8%
2-age 5-8 yr
3-brief loss of environmental awareness.
4-automatism(eye fluttering, head bobbing, lip smacking)
5-neurological exam. &brain imaging are normal.
6-characteristic EEG patterns
(synchronous 3-Hz spike-and-wave)
activity with frontal accentuation.
7-seizure provoke by hyperventilation for 3-5 min.
8-last few seconds.
8-patient have hundreds of seizures /day
9-
Treatment :Ethosuximide. alternatives are valproate or lamotrigine.
Febrile seizures
Definition :
Genetic predisposition to seizures in infancy that precipitate by rapid rise in body
temperature.
*Occur in 2-5% of children .
* age 6 months-60 months (50% occur between 1-2 yrs) with a temperature ≥ 38ċ that is
not due to CNS infection or metabolic disturbance, and in the absence of history of prior
afebrile seizures..
Types :
1-
simple febrile convulsion: generalized, last<15 minutes ,occur once in 24 hr , it does not
carry a risk of epilepsy or mortality.
2-
complex febrile convulsion focal ,>15 ms, >once/24 hr
3-
febrile status epilepticus : when febrile convulsion last > 30 min.

4
Risk factors that can predict recurrence of FC:
*Major criteria: age <1 yr, fever 38-39c and fever duration <24hr.
*Minor criteria:family history of FC or epilepsy, complex FC,male, day care &hyponatremia.
Risk factors for subsequent epilepsy including:
Simple FC :1%
complexFC: 6%
Focal complex:29%
Neurodevelepmental abnormalities :33%
Approach to patient with FC:
*assess the cause of fever by proper history, general exam.& investigations e.g. CBP , blood
glucose , serum electrolytes , CSF exam. By LP should be done in any infant <18 mon. with
FC because seizure may be the only manifestation of meningitis, especially if patient had
received antibiotics which mask the other features of meningitis.
*assess the risk factors of recurrence.
*assess the risk factors for later epilepsy.
Treatment:
*in case of febrile status epilepticus, iv benzodiazepines, phenobarbital, phenytoin,or
valproate.
*in general , antiepileptic therapy is not recommended for children with simple FC, but if
patient has risk factors for recurrences, parents should be educated about how to handle
the seizure if recur& last >5 min. by rectal diazepam or buccal/intranasal midazolam.
*management of underlying illness also important part in general RX of FC. Antipyretic can
reduce discomfort of child, but not reduce the risk of having recurrent FC.
*iron deficiency has been associated with increase the risk of FC, and thus screening &Rx
for it.
*prevention: if the parents are very anxious about their child`s seizure, intermittent oral
diazepam 0.33mg/kg or rectal suppository 0.5 mg/kg every 8 hr. can be given during febrile
illness to prevent recurrence of FC.
5
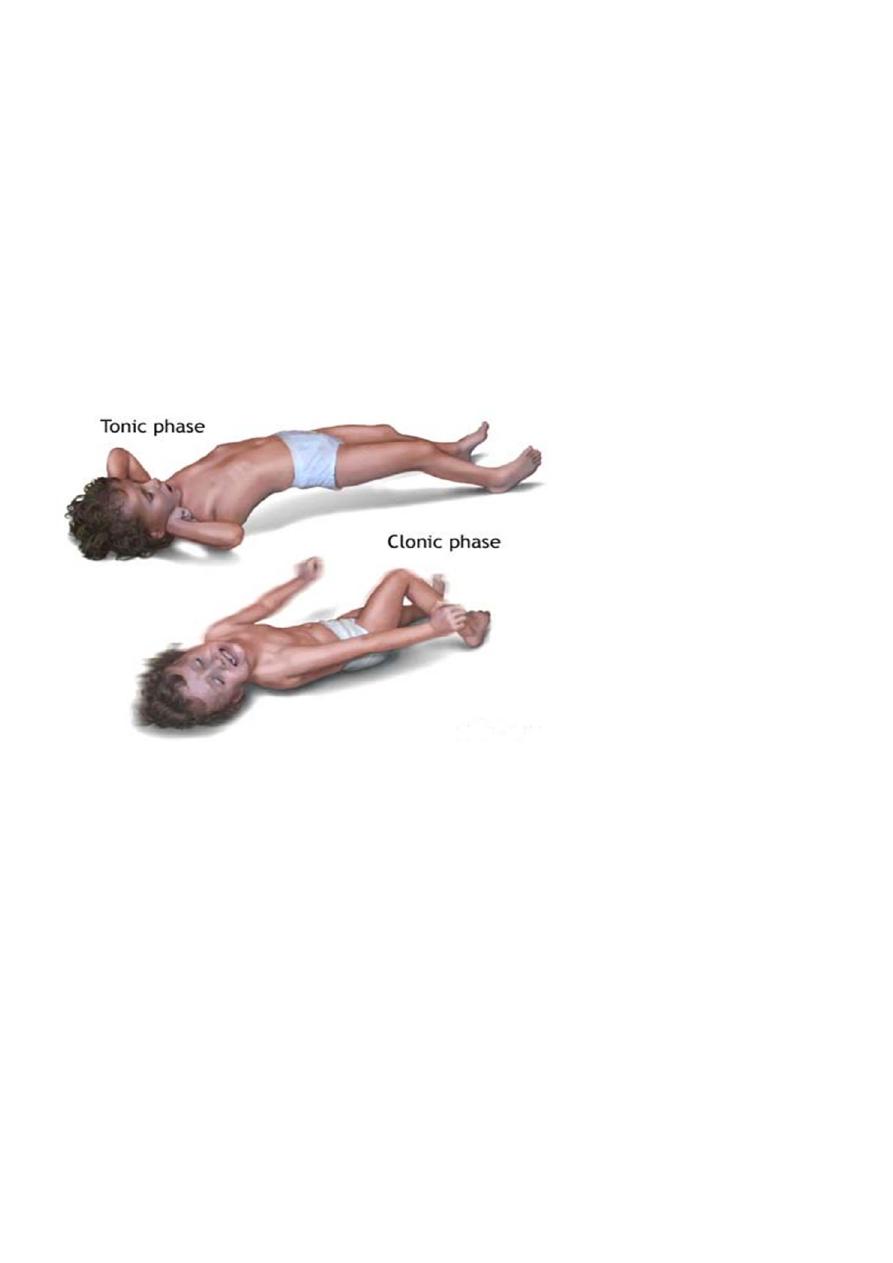
Generalized tonic ,clonic and tonic clonic seizures
May occur alone or with other seizure types.
Loss of posture& consciousness →tonic stiffening & upward deviation of eyes
→pooling of secretion ,pupillary dilation ,diaphoresis ,HT → clonic jerk →briefly tonic
again followed by flaccidity &urinary incontinence.
Treatment:
A B C
Medication :diazepam(0.2-0.4 mg)I.V+phenobarbiton10-20 mg I.V
History & physical exam.
Infantile spasms(west syndrome)
Begin between the age of 2-12 mo.
Consists of a triad of : infantile spasms( usually occure in clusters especially in
drowsiness or upon arousal) , developmental regression, and typical EEG picture
called (hypsarrhythmia).
Of 3 types: 1-flexsters spasm 2- extensor spasm 3- mixed .
Mixed spasm is the most common type.
A cry may precede or follow the spasm, (that confuse with colic).
The clusters of seizures may persist for minutes.
Prognosis is poor.
Recognizing of west syndrome, is a medical emergency because if diagnosis delayed ≥
3 wk. , it can affect the long-term prognosis.

6
Cryptogenic group(40%)good response to therapy without clear etiology.
Symptomatic type (60%)poor response to therapy with clear etiology (e.g. metabolic
like PKU ,congenital malformation of the brain , tuberous sclerosis, congenital
infection…etc.
Treatment
ACTH
Vegabatrine
Valproic acid
Benzodiazepine
Laboratory evaluation of seizures
CBC
Blood chemistry: glucose, Ca, Na, Cl,HCO3, Mg, Ph. .
Urea & creatinine.
Blood & urine for toxicology screen.
In neonates blood for ammonia & inborn error of metabolism.
CSF analysis.
EEG & brain imaging.
Viral study specially for enterovirus.
Principles of seizure therapy
No need for long term treatment of benign febrile convulsion.
Therapy indicated for absence & atypical absence seizures , infantile spasm.
Single , cheap , less toxic drug is the goal that lead to better compliance.
Duration of therapy:
generalized tonic clonic ,tonic, clonic , absence &partial seizures not> than 2-4 yrs.
Myoclonic seizures , atypical absence treatment for life.

7
Risk for recurrence of seizures after discontinuation of therapy
Those children who are neurologically abnormal.
Those having seizures that were initially difficult to control.
Those having persistent epileptiform EEGs.
Status epilepticus
Is defined as continuous seizure activity or recurrent seizure activity without regaining
consciousness lasting for > 30 min.
Impending status epilepticus : is referred to seizure that last between 5 to 30 min.
Etiology:
1-febrile status epilepticus.
2-new-onset epilepsy
3-drug withdrawal in patient on antiepileptic.
4-drug intoxication
5-hypoglycemia
6-electrolytes imbalance (hypocalcemia, hyponatremia , hypomagnesemia).
7- acute head trauma
8-encephalitis & meningitis.
9-postinfectious encephalitis.
10-ischemic stroke
11-intracranial hemorrhage
12- inborne error of metabolism.
13-brain tumor.
Investigation :
-Laboratory studies: serum glucose, sodium, calcium , blood and spinal fluid cultures, toxic
screen and tests for inborn error of metabolism. Antiepileptic drug levels if patient is
already on an antiepileptic.
-EEG: is helpful in identifying the types of status epilepticus.
-neuroimaging: needs to be considered after the child has been stabilized.

8
Treatment :
*Status epilepticus is a medical emergency that better managed in the ICU because it
requires initial and continuous attention to securing airway , breathing, and circulation with
continuous monitoring of vital sign with attention to the systemic complication because
some develop multiorgan failure , as well as management of underlying etiology.
*Medication :
1-benzodiazepines: lorazepam iv 0.05-0.1 mg/kg or diazepam iv 0.2-0.5 mg/kg , if iv access
is not available; use intranasal lorazepam , rectal diazepam , or intranasal / buccal
midazolam.
2- phenytoin( phosphenytoin): iv , loading dose 15-20 mg/kg in a rate not > 0.5-1
mg/kg/min. . Maintenance dose is 5-10 mg /kg/24hr in 2 divided dose.
3-phenobarbital : iv loading dose in neonate 20 mg/kg, but in infant & children 10 mg/kg
4-valproate: iv loading 25mg/kg, maintenance 30-60 mg/kg/24hr.
5-For Refractory , IV bolus of midazolam, propofol, phenobarbital , or thiopental are used
with maintenance of corresponding continuous iv drip.
Acute ataxia
Abnormality of coordination resulting in impairment of direction , rate strength of
voluntary movement.
Usual symptoms are broad-based unsteady gait& tremor , that worsen by intentional
movement of limbs (dysmetria).
Defect in cerebellum and cerebellar pathways.
Etiology:
Post infectious :(chickenpox , infectious mononucleosis ,URTI)
Drug intoxication :(sedative-hypnotic associated with lethargy , carbamazepine &
phenytoin lead to only ataxia).
Tumors of posterior fossa: medulloblastoma , ependymoma.
Hydrocephalus.
Inborn error of metabolism: urea cycle defect , maple syrup urine.
Labyrinthine dysfunction.
Guillain-barré syndrome.