بسم الله الرحمن الرحيم
Pleural effusion
The accumulation of serous fluid within the pleural
space is termed pleural effusion. The accumulation of
frank pus is termed empyema , that of blood is
haemothorax, and that of chyle is a chylothorax. In
general, pleural fluid accumulates as a result of either
increased hydrostatic pressure or decreased osmotic
pressure (‘transudative’ effusion, as seen in cardiac, liver
or renal failure), or from increased microvascular pressure due to disease of the pleura or injury in the adjacent
lung (‘exudative’ effusion).


Clinical assessment
Symptoms (pain on inspiration and coughing) and signs of pleurisy (a pleural rub) often precede the development of an effusion, especially in patients with under-lying pneumonia, pulmonary infarction or connective tissue disease. However, when breathlessness is the only symptom, depending on the size and rate of accumulation, the onset may be insidious.Investigations
Radiological investigationsThe classical appearance of pleural fluid on the erect PA chest film is of a curved shadow at the lung base, blunting the costophrenic angle and ascending towards the axilla . Fluid appears to track up the lateral chest wall. In fact, fluid surrounds the whole lung at this level, but casts a radiological shadow only where the X-ray beam passes tangentially across the fluid against the lateral chest wall. Around 200 mL of fluid is required in order for it to be detectable on a PA chest X-ray. Previous scarring or adhesions in the pleural space can cause localised effusions. Pleural fluid localised below the lower lobe (‘subpulmonary effusion’) simulates an elevated hemidiaphragm. Pleural fluid localised within an oblique fissure may produce a rounded opacity that may be mistaken for a tumour.
Ultrasound is more accurate than plain chest X-ray for determining the presence of fluid. A clear hypo-echoic space is consistent with a transudate and the presence of moving floating densities suggests an exudate. The presence of septation suggests an evolving empyema or resolving haemothorax. CT scanning is indicated where malignant disease is suspected.
Pleural aspiration and biopsy
In some conditions (e.g. left ventricular failure), it should not be necessary to sample fluid unless atypical features are present; appropriate treatment should be adminis-tered and the effusion re-evaluated. However, in most other circumstances, diagnostic sampling is required. Simple aspiration provides information on the colour and texture of fluid and these alone may immediately suggest an empyema or chylothorax. The presence of blood is consistent with pulmonary infarction or malignancy, but may result from a traumatic tap. Biochemical analysis allows classification into transudate and exudates and Gram stain may suggest para-pneumonic effusion. The predominant cell type provides useful information and cytological examination is essential. A low pH suggests infection but may also be seen in rheumatoid arthritis, ruptured oesophagus or advanced malignancy.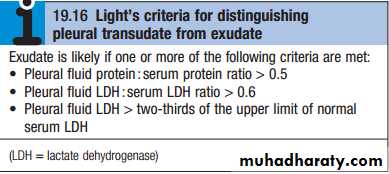
Ultrasound- or CT-guided pleural biopsy provides tissue for pathological and microbiological analysis. Where necessary, video-assisted thoracoscopy allows
visualisaton of the pleura and direct guidance of a biopsy.
Management
Therapeutic aspiration may be required to palliate
breathlessness but removing more than 1.5 L at a time
is associated with a small risk of re-expansion pulmonary oedema. An effusion should never be drained to
dryness before establishing a diagnosis, as biopsy may
be precluded until further fluid accumulates. Treatment
of the underlying cause – for example, heart failure,
pneumonia, pulmonary embolism or subphrenic abscess
– will often be followed by resolution of the effusion.